

Abstract
Elbow arthroscopy is an increasingly common procedure performed in orthopaedic surgery. However, because of the presence of several major neurovascular structures in close proximity to the operative portals, it can have potentially devastating complications. The largest series of elbow arthroscopies to date described a 2.5% rate of postoperative neurological injury. All of these injuries were transient nerve injuries resolved without intervention. A recent report of major nerve injuries after elbow arthroscopy demonstrated that these injuries are likely under-reported in literature. Because of the surrounding neurovascular structures, familiarity with normal elbow anatomy and portals will decrease the risk of damaging important structures. The purpose of this Technical Note is to review important steps in performing elbow arthroscopy with an emphasis on avoiding neurovascular injury. With a sound understanding of the important bony anatomic landmarks, sensory nerves, and neurovascular structures, elbow arthroscopy can provide both diagnostic and therapeutic intervention with little morbidity.
Elbow arthroscopy is a technically demanding procedure that requires extensive hands-on training and supervised experience to acquire proficiency. When performed with appropriate judgment and technique, elbow arthroscopy is an excellent tool for the correction of many lesions of the elbow joint with minimal risk.1 However, it poses greater technical challenges and neurological risks than knee or shoulder arthroscopy. Arthroscopy of the elbow joint is perhaps the most hazardous due to the potential for causing injury to important nearby nerves and vessels. The reason for this relates to the complex relation of these structures to the joint (Fig 1).2 Because of the surrounding neurovascular structures, familiarity with the normal elbow anatomy and portals will decrease the risk of damage to important neurovascular structures.3 With a sound understanding of the important bony anatomic landmarks, sensory nerves, and neurovascular structures, elbow arthroscopy can serve as an opportunity for both diagnostic and therapeutic intervention with little morbidity.
Fig 1.

Lateral view of the right elbow viewing medial to lateral showing the antecubital fossa with important neurovascular structures including the ulnar nerve medially, the radial nerve posteriorly, and the median nerve anteriorly.
Because of the proximity of several neurovascular structures to the established portals, the risk of neurological injury during elbow arthroscopy is higher as compared with other joints.4 In addition, the complications after elbow arthroscopy have been reported to be 10%, compared with a rate of approximately 3% after knee arthroscopy.5 Multiple anatomical studies have documented the relation and location of the nerves crossing the elbow to the commonly used arthroscopic portals.6, 7, 8, 9, 10, 11 Not surprisingly, injuries to every nerve about the elbow have been reported after arthroscopy.12, 13, 14, 15, 16, 17 Despite these concerns, the 3 largest consecutive series of elbow arthroscopy to date have reported a low incidence of neurological complications.5, 18, 19 The first large series of consecutive elbow arthroscopies reported one laceration of the ulnar nerve in 187 consecutive cases (0.5%).19 The largest series reported a 2.5% rate of neurological injury after elbow arthroscopy in 473 consecutive cases, with ulnar nerve dysfunction being the most common.5 All of the reported injuries in this series resolved spontaneously without intervention.
In the most recent series, a 1.7% rate of neurological injury was reported in 417 consecutive elbow arthroscopies.18 As with the previous series, all of the reported injuries were transient in nature. From these studies, it can be inferred that a permanent neurological deficit is an extremely rare occurrence, despite the risks highlighted in the anatomical studies. However, a recent online survey of members of the American Society for Surgery of the Hand reported a much higher incidence of major nerve injuries after elbow arthroscopy indicating that this is not a rare occurrence.20 In this Technical Note and in Video 1, we will provide a step-by-step process for performing elbow arthroscopy to minimize the risk to neurovascular structures.
History and Physical Examination
Before proceeding with elbow arthroscopy, a comprehensive history should be taken including the occupation of the patients, whether they are right or left handed, the location of their pain, and the duration of their symptoms. It is also important to determine the details of whether their symptoms started with a single traumatic event or from repetitive activities. Symptoms in the lateral region of the elbow may be indicative of radiocapitellar chondromalacia, osteochondral loose bodies, radial head fracture, osteochondritis dissecans lesions, and most commonly lateral epicondylitis. Symptoms in the medial region of the elbow most commonly present as medial epicondylitis, but medial collateral ligament sprains, ulnar neuritis, ulnar nerve subluxation, or even a medial epicondyle avulsion fracture should also be considered.
The differential diagnosis for symptoms of the anterior elbow includes distal biceps tendon rupture that can be partial or complete, an anterior capsular strain, and a brachioradialis muscle strain.21 Symptoms in the posterior compartment can reflect valgus extension overload syndrome, posterior impingement, osteochondral loose bodies, triceps tendonitis, triceps tendon avulsion, or olecranon bursitis.22 A careful neurovascular history is also important as ulnar nerve paraesthesias can be the result of cubital tunnel syndrome, a subluxing ulnar nerve, or a traction injury from valgus instability.23 A careful physical examination of all 3 compartments of the elbow is critical to determine the correct diagnosis. Each compartment should be examined individually to fully evaluate the elbow.
Diagnostic Imaging
Routine diagnostic radiographs include an anterior posterior view with the elbow in full extension and a lateral view with the joint in 90° of flexion. An axial view can also be obtained to outline the olecranon and its medial and lateral articulations. When there is a history of trauma, an oblique view should also be done to rule out occult fractures.
A magnetic resonance imaging is useful for evaluating osteochondral lesions in the radiocapitellar joint24, 25 and for demonstrating early vascular changes that are not yet apparent on plain radiographs and can be used to assess the extent of the lesion and displacement of fragments.23 Magnetic resonance imaging is also helpful for evaluating the soft tissue structures of the elbow including the tendinous insertions of the flexor and extensor musculature to help in diagnosing medial and lateral epicondylitis, the triceps insertion, and associated musculature to evaluate for triceps tendonitis, and the medial and lateral collateral ligaments for possible tears. Magnetic resonance arthrography with saline contrast or gadolinium can increase the sensitivity for detecting undersurface tears of the ulnar collateral ligament and has now become the test of choice to detect these tears.26
Surgical Technique
Patient Positioning
We typically perform this procedure under general endotracheal anesthesia in the prone position. This procedure can also be performed with the patient in the lateral decubitus position,27 but the prone position is our preference. We prefer the prone position because it allows easy access to both the anterior and posterior compartments of the elbow joint. Similar access can be achieved in the lateral decubitus position, but we prefer the prone position because we find it easier to gain access into both compartments. We strongly advise against the supine position because access to the posterior compartment is difficult and can lead to unintentional neurovascular injury.
Operating Room Setup and Anesthesia Considerations
We prefer general anesthesia because it allows proper positioning of the patient, which is key to avoiding neurological and vascular injuries although a regional block is possible. After an appropriate level of anesthesia (general endotracheal or axillary block) has been achieved, the patient is placed in the prone position, using 2 large chest rolls under the torso to raise the patient's torso up from the operating table. These are made of operating room blankets rolled up and taped together. These chest rolls are very important and must be firm so that it elevates the chest wall off of the operating room table. We advise against the premade devices used by spine surgeons for prone positioning because they do not elevate the patient high enough off of the operating room table.
In the prone position, an arm board is placed on the operative side of the table and parallel to it. A sandbag, block, or firm bump of towels is placed under the shoulder to further elevate the arm away from the table and increase the mobility of the upper extremity. If the chest rolls are not high enough or firm enough, the chest will not be elevated far enough away from the operating room table and the shoulder will be placed in hyperabduction, which can place unnecessary stress or strain on the shoulder capsule or surrounding structures. The forearm is then allowed to hang in a dependent position over the arm board at 90° (Fig 2). A sterile tourniquet may be placed around the proximal aspect of the arm to help to control bleeding during the procedure, but it is not always necessary to inflate when using a mechanical irrigation system.1 The forearm is prepared from the proximal arm to the tip of the fingers, and then the extremity is wrapped with an elastic bandage from the fingers to just below the elbow to minimize fluid extravasation into the forearm.28 After the extremity is prepped and draped, a large sterile “bump” is placed under the arm proximal to the elbow to keep the shoulder abducted to 90° and the elbow at approximately 90° of flexion (Fig 3). Finally, we recommend using a Smith and Nephew/Dyonics 30° 4.5-mm arthroscope and a Smith and Nephew/Dyonics 4.0-mm full-radius shaver.
Fig 2.

The patient in the prone position with the right elbow resting over an arm board that is parallel to the operating room table. A nonsterile U-drape is placed proximally. A sterile bump is placed under the arm for support after the extremity is prepped. Anesthesia is at the head of the table.
Fig 3.

A left elbow is shown in the prone position with the head of the patient to the left and the feet to the right. Anesthesia is at the head (left) of the patient and all equipment is on the opposite side of the table. Note the sterile bump under the arm, which helps stabilize the elbow during the procedure. This rests on the arm board, which has been placed parallel to the table.
Portal Placement and Diagnostic Arthroscopy
Anterior Compartment
Anatomic Landmark Identification
After prepping and draping the extremity, all bony landmarks are then outlined including the olecranon, the medial and lateral epicondyles, the radiocapitellar joint, and the course of the ulnar nerve (Fig 4). The proximal anteromedial portal is located approximately 2 cm proximal to the medial epicondyle and just anterior to the intermuscular septum (Fig 5) and is established first. If close attention is paid to anatomic landmarks, joint insufflation is not necessary. Before establishing this portal, the location and the stability of the ulnar nerve should be assessed. If there is any history of a previous ulnar transposition or a question of a subluxing ulnar nerve, this portal incision should be extended to the ulnar nerve dissected out and identified before portal placement (Table 1).
Fig 4.

A close-up view of the left elbow in the prone position with the head of the patient to the left and the feet to the right. Anatomic landmarks are identified of the left elbow in the prone position including the medial epicondyle (right), the lateral epicondyle (left), the radial head, the olecranon, and the ulnar nerve (dark blue line on right). The intermuscular septum is also identified on the medial aspect of the elbow, just anterior to the medial epicondyle.
Fig 5.

A close-up view of the left elbow in the prone position with the head of the patient to the left and the feet to the right. The proximal anteromedial portal is the first to be established; it is located just anterior to the intermuscular septum and 2 cm proximal to the medial epicondyle.
Table 1.
Pearls and Pitfalls of Elbow Arthroscopy
| Pearls | Pitfalls |
|---|---|
| 1. The prone or the lateral decubitus position is the preferred patient positioning for elbow arthroscopy. Both positions allow easy access to the both the anterior and posterior compartments | 1. The anterolateral portal located 3 cm distal and 2 cm anterior to the lateral epicondyle places the radial nerve at significant risk and should be avoided |
| 2. It is important to identify and mark landmarks of the elbow joint. This includes the tip of the olecranon, the medial and lateral epicondyle, the radial head, the soft spot of the elbow, the medial intermuscular septum, and the ulnar nerve | 2. A subluxing ulnar nerve or a previous ulnar nerve transposition places the ulnar nerve at risk with proximal anteromedial portal placement |
Neurovascular Considerations
If the course of the ulnar nerve is not in question, then blunt dissection is carried through the proximal anterior medial portal with a straight Kelly instrument until the anterior aspect of the humerus is palpated. This is the key step. If the portal is placed too anterior, then the neurovascular structures in the antecubital fossa are at risk. If the portal is posterior to the humerus and posterior to the intermuscular septum, the ulnar nerve can be damaged. We have seen iatrogenic ulnar nerve damage from improper portal placement and so meticulous attention to detail is important to avoid this complication.
Anteromedial Portal Placement
The arthroscopic cannula and sheath is then inserted anterior to the intermuscular septum while maintaining contact with the anterior aspect of the humerus and directing the trocar toward the radial head. The use of the anterior surface of the humerus as a constant guide helps to prevent injury to the median nerve and the brachial artery, which are anterior to the capsule. The ulnar nerve is located approximately 3 to 4 mm from this portal, posterior to the intermuscular septum (Fig 6). Palpating the septum and making sure that the portal is established anterior to the intermuscular septum minimizes the risk of injury to the nerve while providing excellent visualization of the radiocapitellar joint, the humeroulnar joints, the coronoid fossa, and the superior joint capsule.1, 23 We prefer establishing the proximal anterior medial portal first as there is less fluid extravasation when starting medially because this portal traverses predominantly tendinous tissue and a tough portion of the forearm flexor muscles.29, 30 The thicker tissues minimize fluid extravasation more effectively than the softer, thinner, radial capsule laterally.29, 30 Finally, most elbow disorders are located in the lateral compartment, which is best visualized from the proximal anteromedial portal,23 including the lateral capsule, the radiocapitellar joint, and the distal aspect of the humerus (Fig 7).
Fig 6.

The elbow is in the prone position with the head to the left and the fingers and hand hanging down. Viewing from medial to lateral, the ulnar nerve is posterior to the intermuscular septum. The arthroscope is inserted 2 cm proximal to the medial epicondyle and just anterior to the intermuscular septum on the medial aspect of the arm. In the prone position, the brachial artery and median nerve fall away from the joint capsule allowing for safe portal placement.
Fig 7.
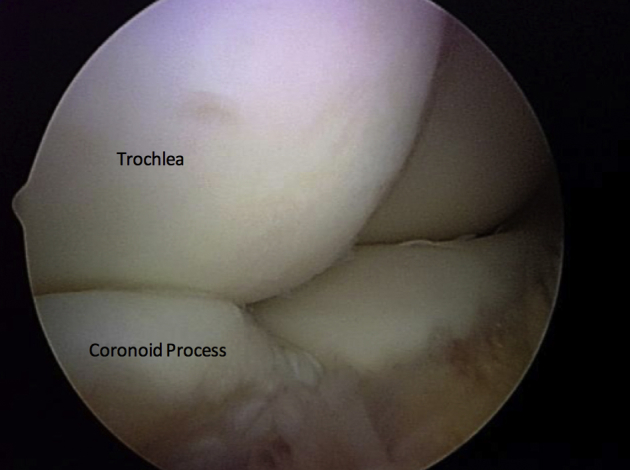
With the patient in the prone position, viewing from the proximal anterior medial portal of a left elbow, the trochlea (top left) and the coronoid process (lower left) can be seen from the proximal anteromedial portal.
Anterolateral Portal Placement
After creating the proximal anteromedial portal, we establish the proximal anterolateral portal using an outside-in technique localizing the position with a spinal needle. This portal is created 2 cm proximal and 1 cm anterior to the lateral epicondyle, as described by Field et al.31 If this portal is created too far distally near the radiocapitellar joint or even further distally near the radial neck, it places the posterior interosseous nerve at significant risk. Nonfenestrated cannulas are used to prevent extravasation of the fluid into the subcutaneous tissues.
Visualizing from the proximal anteromedial portal, one can visualize the lateral capsule and palpate the skin to localize the exact location of the spinal needle for accurate portal placement (Fig 8). It is important to direct the cannula toward the humerus while penetrating the capsule so that the portal placement is not too far anterior and medial.3 The proximal anterolateral portal is often a working portal and is ideal for arthroscopic lateral epicondyle release and debridement of the radiocapitellar joint. Viewing from this portal permits visualization of the anterior compartment, and is particularly good in evaluating medial structures, such as the trochlea, coronoid tip, and the medial capsule (Fig 9).
Fig 8.

With the patient in the prone position, viewing from the proximal anterior medial portal of a left elbow, the lateral capsule is seen from the proximal anteromedial portal. This is the location where a spinal needle is introduced for the proximal anterolateral portal.
Fig 9.

With the patient in the prone position, viewing from the proximal anterolateral portal of a left elbow, the trochlea and the coronoid process can also be seen.
Posterior Compartment
Posterior Portal Placement
For evaluating the posterior compartment, the straight posterior portal is usually created first and is located 3 cm proximal to the tip of the olecranon and can be used as a viewing portal or as a working portal. When it is the first portal created, a cannula with a blunt trocar is inserted. The cannula pierces the triceps muscle just above the musculotendinous junction and is bluntly maneuvered in a circular motion manipulating the soft tissues from the olecranon fossa for better visualization. When used as a working portal, it is helpful for removal of impinging olecranon osteophytes and loose bodies from the posterior elbow joint (Table 2).32 The straight posterior portal passes within 25 mm of the ulnar nerve and within 23 mm of the posterior antebrachial cutaneous nerve.29
Table 2.
Advantages and Disadvantages of Elbow Arthroscopy
| Advantages | Disadvantages |
|---|---|
| 1. Elbow arthroscopy can be an effective and less invasive tool to enter into the elbow joint to confirm the diagnosis of an infection, irrigate the joint, debride infected tissue, remove loose bodies and osteophytes, and treat lateral epicondylitis | 1. Significant distortions of normal bony or soft tissue anatomy, previous ulnar nerve transposition, or severe ankylosis may place important neurovascular structures at risk and preclude safe entry of the arthroscope into the joint |
| 2. Elbow arthroscopy permits a more complete visualization of the articular surface of the elbow, rapid rehabilitation, and an earlier return to work or sports | 2. Iatrogenic damage to the radial nerve, posterior interosseous nerve, and ulnar nerve can occur but can be minimized with careful attention to detail. Careful portal placement is necessary to avoid damage to neurovascular structures along with the careful and judicious use of the arthroscopic shaver in the elbow joint |
|
Posterolateral Portal Placement
The posterolateral portal is located 2 to 3 cm proximal to the tip of olecranon at the lateral border of the triceps tendon. This is created while visualizing from the straight posterior portal using a spinal needle directed toward the olecranon fossa (Fig 10). Initial visualization of the posterior compartment can be impeded by synovitis, scar tissue, and fat pad hypertrophy. A trocar is directed toward the olecranon fossa, passing through the triceps muscle to reach the capsule. A shaver is then introduced to improve visualization of the posterior compartment. This portal permits visualization of the olecranon tip, olecranon fossa, and posterior trochlea. It may also be used as a working portal to remove osteophytes and loose bodies from the posterior compartment (Fig 11). The medial and posterior antebrachial cutaneous nerves are the 2 neurovascular structures at most risk, residing an average of 25 mm from this portal.33 The ulnar nerve is also at significant risk near the medial epicondyle and the medial gutter. Careful direct visualization of the arthroscopic shaver is important when in this area, and the judicious use of the suction of the shaver can prevent iatrogenic injury to the ulnar nerve. At no time should the arthroscopic shaver be used “blind” in this area because the ulnar nerve can be inadvertently sucked into the shaver tip and cause significant and possible irreversible damage to the nerve.
Fig 10.

With the patient in the prone position, the arthroscope is introduced into the posterior compartment of a left elbow using a straight posterior portal, 3 cm proximal from the tip of the olecranon. A spinal needle is introduced lateral to the triceps tendon toward the olecranon fossa for the posterolateral portal.
Fig 11.

Viewing the left elbow from above, the arthroscope is in the posterior compartment and the posterior lateral portal is used as a working portal to remove osteophytes and loose bodies from the posterior compartment.
Lateral Portal Placement
The direct lateral portal is located at the “soft spot” that is the triangle formed by the radial head, lateral epicondyle, and olecranon. It is developed under direct visualization using a spinal needle and may be used as either a viewing portal for the posterior compartment and radiocapitellar joint or a working portal for radial head resection.34 This is the only portal that provides easy access to the posterior capitellum and radioulnar joint and can be useful for lesions of the radiocapitellar joint.22 Altering the portal position along the line between the posterolateral portal and lateral soft spot changes the orientation of the portal relative to the joint.28 These portals are particularly useful for gaining access to the posterolateral recess.
Discussion
The several published consecutive series of elbow arthroscopies performed demonstrated extremely low rates of neurological complications. Taken in the aggregate, these studies demonstrated one permanent nerve palsy out of over a thousand elbow arthroscopies. The vast majority of the nerve palsies reported in these series were transient, sensory deficits.
However, a recent survey of members of the American Society for Surgery of the Hand received 322 responses and a total of 222 nerve injuries were reported. There were 107 major nerve injuries that were defined as those requiring surgical intervention. The most common nerve involved was the ulnar nerve (38%), followed by the radial nerve (22%) and the posterior interosseous nerve (PIN) (19%). It is obvious from this report that the risk of neurological complications after elbow arthroscopy has likely been under-reported in the literature.20
At our institutions where we have been referred patients with neurovascular complications after elbow arthroscopy, we have found that the PIN palsy is the most common injury after elbow arthroscopy followed by ulnar nerve palsy. Many of these complications could have been avoided with proper portal placement. In particular, each of the patients with PIN palsies or lacerations had lateral portal placements either at the level of the radiocapitellar joint or distal to it. Staying at least 2 cm proximal to the lateral epicondyle will minimize or even eliminate this risk. This is important when performing an anterior capsule release or a radial head resection.
For the anterior-medial portal, it is very important to stay anterior to the intermuscular septum, which protects the ulnar nerve. Palpation of the intermuscular septum is key and the inability to locate it can cause inadvertent placement of the arthroscopic cannula and trocar posteriorly and damage the ulnar nerve. Blunt dissection anterior to the intermuscular septum and anteriorly to the anterior aspect of the humerus is critical. The use of the anterior surface of the humerus as a constant guide helps to prevent injury to the median nerve and the brachial artery, which are anterior to the capsule. It also prevents posterior placement of the portal posterior to the humerus, which can place the ulnar nerve at risk. As mentioned previously, if there is a question of a subluxing ulnar nerve or if there is a history of a previous ulnar nerve transposition, the portal incision should be enlarged both proximally and distally and the ulnar nerve should be dissected out and identified before portal placement.
In the posterior compartment, the ulnar is also at greatest risk and can be injured with the use of the arthroscopic shaver in the medial gutter, so careful attention must be used when the shaver is used in this region. It is paramount that there is direct visualization of the shaver tip at all times and that there is never “blind” shaving in the medial gutter.
Elbow arthroscopy is a technically demanding procedure. Attention to detail, including careful portal placement (Table 1), is necessary to avoid iatrogenic injury to neurovascular structures around the elbow joint. In every clinical case, the bony anatomy should be drawn on the patient's elbow and an 18-gauge spinal needle should be used to confirm the correct portal location before introducing larger arthroscopic instruments.20 As with any operative procedure, careful preoperative planning, including a detailed history and physical examination, along with proper imaging studies, and sound clinical judgment, is necessary to ensure a successful procedure.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
The patient is positioned in the prone position on the operating table, optimizing access to the anterior and posterior compartments of the left elbow. Bony landmarks are then outlined including the olecranon, the medial and lateral epicondyles, the radiocapitellar joint, and the course of the ulnar nerve. First, a skin incision is made to establish the anteromedial portal, which is located approximately 2 cm proximal to the medial epicondyle and just anterior to the intermuscular septum. Blunt dissection of the soft tissues through the proximal anteromedial portal is performed with a straight Kelly instrument until the anterior aspect of the humerus is palpated. Careful attention is paid to stay anterior to the intermuscular septum to avoid damage to the ulnar nerve, which lies posteriorly. Using the anterior surface of the humerus as a guide to avoid injury to the median nerve and the brachial artery, an arthroscopic cannula and sheath are inserted anterior to the intermuscular septum. The capitellum, radial head, lateral capsule, medial gutter, and coronoid process are visualized with the arthroscope. The anteromedial portal allows excellent visualization of the lateral compartment where most elbow pathology occurs. Next, the proximal anterolateral portal is established using an outside-in technique with a spinal needle, which helps establish safe portal placement. Careful attention is paid to stay proximal to the radiocapitellar joint to avoid damage to the posterior interosseous nerve, a branch of the radial nerve. The proximal anterolateral portal is often a working portal that is ideal for addressing pathology such as lateral epicondylitis and loose bodies. A switching stick technique is then used to change portals. The arthroscope is placed in the anterolateral portal, whereas the working cannula is placed in the anteromedial portal to allow for further visualization of the anterior compartment of the elbow including the coronoid process, distal aspect of the humerus, radiocapitellar joint, and a different vantage point of the radial head. Using the switching stick technique helps prevent iatrogenic nerve damage. For evaluating the posterior compartment, the direct posterior portal is established by using a spinal needle directed toward the olecranon fossa. The arthroscope is placed 2 fingerbreadths proximal to the tip of the olecranon. Careful attention is paid to the course of the radial nerve. A spinal needle and arthroscopic shaver are then introduced to improve visualization of the posterior compartment through debridement. This portal permits visualization of the olecranon tip, olecranon fossa, and posterior trochlea. It may also be used as a working portal to remove osteophytes and loose bodies from the posterior compartment. The ulnar nerve is also at significant risk near the medial epicondyle and the medial gutter. Direct visualization of the arthroscopic shaver is important when in this area, and judicious use of the suction of the shaver can prevent iatrogenic injury to the ulnar nerve. In summary, while performing elbow arthroscopy, it is important to use anatomical landmarks for exact portal placement to prevent neurovascular injury.
References
- 1.Strothers D., Day B., Regan W.R. Arthroscopy of the elbow: Anatomy, portal sites, and description of the proximal lateral portal. Arthroscopy. 1995;11:449–457. doi: 10.1016/0749-8063(95)90200-7. [DOI] [PubMed] [Google Scholar]
- 2.Poehling G.G., Ekman E.F. Arthroscopy of the elbow. Instr Course Lect. 1995;44:217–223. [PubMed] [Google Scholar]
- 3.Moskal M.J. Canada; Vancouver: May 2005. Advanced arthroscopic management of common elbow disorders. Arthroscopy Association of North America 24th Annual Meeting. [Google Scholar]
- 4.Adams J.E., Steinmann S.P. Nerve injuries about the elbow. J Hand Surg Am. 2006;31:303–313. doi: 10.1016/j.jhsa.2005.12.006. [DOI] [PubMed] [Google Scholar]
- 5.Kelly E.W., Morrey B.F., O'Driscoll S.W. Complications of elbow arthroscopy. J Bone Joint Surg Am. 2001;83:25–34. doi: 10.2106/00004623-200101000-00004. [DOI] [PubMed] [Google Scholar]
- 6.Lynch G.J., Meyers J.F., Whipple T.L., Caspari R.B. Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy. 1987;2:191–197. doi: 10.1016/s0749-8063(86)80067-6. [DOI] [PubMed] [Google Scholar]
- 7.Marshall P.D., Fairclough J.A., Johnson S.R., Evans E.J. Avoiding nerve damage during elbow arthroscopy. J Bone Joint Surg Br. 1993;75:129–131. doi: 10.1302/0301-620X.75B1.8421009. [DOI] [PubMed] [Google Scholar]
- 8.Miller C.D., Jobe C.M., Wright M.H. Neuroanatomy in elbow arthroscopy. J Shoulder Elbow Surg. 1995;4:168–174. doi: 10.1016/s1058-2746(05)80047-3. [DOI] [PubMed] [Google Scholar]
- 9.Omid R., Hamid N., Keener J.D., Galatz L.M., Yamaguchi K. Relation of the radial nerve to the anterior capsule of the elbow: Anatomy with correlation to arthroscopy. Arthroscopy. 2012;12:1800–1804. doi: 10.1016/j.arthro.2012.05.890. [DOI] [PubMed] [Google Scholar]
- 10.Unlu M.C., Kesmezacar H., Akgun I., Ogut T., Uzun I. Anatomic relationship between elbow arthroscopy portals and neurovascular structures in different elbow and forearm positions. J Shoulder Elbow Surg. 2006;15:457–462. doi: 10.1016/j.jse.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 11.Verhaar J., van Mameren H., Brandsma A. Risks of neurovascular injury in elbow arthroscopy: Starting anteromedially or anterolaterally? Arthroscopy. 1991;7:287–290. doi: 10.1016/0749-8063(91)90129-l. [DOI] [PubMed] [Google Scholar]
- 12.Dumonski M.L., Arciero R.A., Mazzocca A.D. Ulnar nerve palsy after elbow arthroscopy. Arthroscopy. 2006;22:577.E1–577.E3. doi: 10.1016/j.arthro.2005.12.049. [DOI] [PubMed] [Google Scholar]
- 13.Haapaniemi T., Berggren M., Adolfsson L. Complete transection of the median and radial nerves during arthroscopic release of post-traumatic elbow contracture. Arthroscopy. 1999;15:784–787. doi: 10.1016/s0749-8063(99)70015-0. [DOI] [PubMed] [Google Scholar]
- 14.Gupta A., Sunil T.M. Complete division of the posterior interosseous nerve after elbow arthroscopy: A case report. J Shoulder Elbow Surg. 2004;13:566–567. doi: 10.1016/j.jse.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 15.Papilion J.D., Neff R.S., Shall L.M. Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy. 1988;4:284–286. doi: 10.1016/s0749-8063(88)80046-x. [DOI] [PubMed] [Google Scholar]
- 16.Ruch D.S., Poehling G.G. Anterior interosseous nerve injury following elbow arthroscopy. Arthroscopy. 1997;13:756–758. doi: 10.1016/s0749-8063(97)90014-1. [DOI] [PubMed] [Google Scholar]
- 17.Thomas M.A., Fast A., Shapiro D. Radial nerve damage as a complication of elbow arthroscopy. Clin Orthop Relat Res. 1987;215:130–131. [PubMed] [Google Scholar]
- 18.Nelson G.N., Wu T., Galatz L.M., Yamaguchi K., Keener J.D. Elbow arthroscopy: Early complications and associated risk factors. J Shoulder Elbow Surg. 2014;2:273–278. doi: 10.1016/j.jse.2013.09.026. [DOI] [PubMed] [Google Scholar]
- 19.Reddy A.S., Kvitne R.S., Yocum L.A., Elattrache N.S., Glousman R.E., Jobe F.W. Arthroscopy of the elbow: A long-term clinical review. Arthroscopy. 2000;6:588–594. doi: 10.1053/jars.2000.8953. [DOI] [PubMed] [Google Scholar]
- 20.Desai M.J., Suhail K.M., Lodha S.L., Richard M.J., Leversedge F.J., Ruch D.S. Major peripheral nerve injuries after elbow arthroscopy. Arthroscopy. 2016;32:999–1002. doi: 10.1016/j.arthro.2015.11.023. [DOI] [PubMed] [Google Scholar]
- 21.Dodson C.C., Nho S.J., Williams R.J., Altchek D.W. Elbow arthroscopy. J Am Acad Orthop Surg. 2008;16:574–585. doi: 10.5435/00124635-200810000-00003. [DOI] [PubMed] [Google Scholar]
- 22.Yadao M.A., Field L.D., Savoie F.H., III Osteochondritis dissecans of the elbow. Instr Course Lect. 2004;53:599–606. [PubMed] [Google Scholar]
- 23.Baker C.L., Grant L.J. Arthroscopy of the elbow. Am J Sports Med. 1999;27:251–264. doi: 10.1177/03635465990270022401. [DOI] [PubMed] [Google Scholar]
- 24.Jaraw P.M., Hessen U., Hirsch G. Osteochondral lesion in the radiocapitellar joint in the skeletally immature: Radiographic MRI and arthroscopic findings in 13 conservative cases. J Pediatr Orthop. 1997;17:311–314. [PubMed] [Google Scholar]
- 25.Takahara M., Shundo M., Kondo M. Early detection of osteochondritis dissecans of the capitellum in young baseball players: Report of three cases. J Bone Joint Surg Am. 1998;80:892–897. doi: 10.2106/00004623-199806000-00014. [DOI] [PubMed] [Google Scholar]
- 26.Timmerman L.A., Schwartz M.L., Andrews J.R. Preoperative evaluation of the ulnar ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22:26–32. doi: 10.1177/036354659402200105. [DOI] [PubMed] [Google Scholar]
- 27.O'Driscoll S.W., Morrey B.F. Arthroscopy of the elbow: Diagnostic and therapeutic benefits and hazards. J Bone Joint Surg Am. 1992;74:84–94. [PubMed] [Google Scholar]
- 28.Abboud J.A., Ricchette E.T., Tjoumakaris F., Ramsey M.L. Elbow arthroscopy: Basic set-up and portal placement. J Am Acad Orthop Surg. 2006;14:312–318. doi: 10.5435/00124635-200605000-00007. [DOI] [PubMed] [Google Scholar]
- 29.Baker C.L., Brooks A.A. Arthroscopy of the elbow. Clin Sports Med. 1996;15:261–281. [PubMed] [Google Scholar]
- 30.Lo I.K.Y., King G.J.W. Arthroscopic radial head excision (case report) Arthroscopy. 1994;10:689–692. doi: 10.1016/s0749-8063(05)80068-4. [DOI] [PubMed] [Google Scholar]
- 31.Field L.D., Altchek D.W., Warren R.F., O'Brian S.J., Skyltar M.J., Wickiewicz T.L. Arthroscopy anatomy of the lateral elbow: A comparison of 3 portals. Arthroscopy. 1994;10:602–607. doi: 10.1016/s0749-8063(05)80055-6. [DOI] [PubMed] [Google Scholar]
- 32.Andrews J.R., St. Pierre R.K., Carson W.G. Arthroscopy of the elbow. Clin Sports Med. 1986;5:653–662. [PubMed] [Google Scholar]
- 33.Lynch G.J., Meyers J.F., Whipple T.L., Caspari R.B. Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy. 1986;2:190–197. doi: 10.1016/s0749-8063(86)80067-6. [DOI] [PubMed] [Google Scholar]
- 34.Savoie F.H., Nunley P.D., Field L.D. Arthroscopic management of the arthritic elbow: Indications, technique and results. J Shoulder Elbow Surg. 1999;8:214–219. doi: 10.1016/s1058-2746(99)90131-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient is positioned in the prone position on the operating table, optimizing access to the anterior and posterior compartments of the left elbow. Bony landmarks are then outlined including the olecranon, the medial and lateral epicondyles, the radiocapitellar joint, and the course of the ulnar nerve. First, a skin incision is made to establish the anteromedial portal, which is located approximately 2 cm proximal to the medial epicondyle and just anterior to the intermuscular septum. Blunt dissection of the soft tissues through the proximal anteromedial portal is performed with a straight Kelly instrument until the anterior aspect of the humerus is palpated. Careful attention is paid to stay anterior to the intermuscular septum to avoid damage to the ulnar nerve, which lies posteriorly. Using the anterior surface of the humerus as a guide to avoid injury to the median nerve and the brachial artery, an arthroscopic cannula and sheath are inserted anterior to the intermuscular septum. The capitellum, radial head, lateral capsule, medial gutter, and coronoid process are visualized with the arthroscope. The anteromedial portal allows excellent visualization of the lateral compartment where most elbow pathology occurs. Next, the proximal anterolateral portal is established using an outside-in technique with a spinal needle, which helps establish safe portal placement. Careful attention is paid to stay proximal to the radiocapitellar joint to avoid damage to the posterior interosseous nerve, a branch of the radial nerve. The proximal anterolateral portal is often a working portal that is ideal for addressing pathology such as lateral epicondylitis and loose bodies. A switching stick technique is then used to change portals. The arthroscope is placed in the anterolateral portal, whereas the working cannula is placed in the anteromedial portal to allow for further visualization of the anterior compartment of the elbow including the coronoid process, distal aspect of the humerus, radiocapitellar joint, and a different vantage point of the radial head. Using the switching stick technique helps prevent iatrogenic nerve damage. For evaluating the posterior compartment, the direct posterior portal is established by using a spinal needle directed toward the olecranon fossa. The arthroscope is placed 2 fingerbreadths proximal to the tip of the olecranon. Careful attention is paid to the course of the radial nerve. A spinal needle and arthroscopic shaver are then introduced to improve visualization of the posterior compartment through debridement. This portal permits visualization of the olecranon tip, olecranon fossa, and posterior trochlea. It may also be used as a working portal to remove osteophytes and loose bodies from the posterior compartment. The ulnar nerve is also at significant risk near the medial epicondyle and the medial gutter. Direct visualization of the arthroscopic shaver is important when in this area, and judicious use of the suction of the shaver can prevent iatrogenic injury to the ulnar nerve. In summary, while performing elbow arthroscopy, it is important to use anatomical landmarks for exact portal placement to prevent neurovascular injury.