

CASE PRESENTATION
We present a 31-year-old male who sustained an isolated stellate corneal laceration associated with an open globe injury. The patient presented with mild, right eye pain one hour after glass was sustained to the face during a motor vehicle collision. Visual acuity was 20/100 (baseline 20/20), but no obvious facial or ocular trauma was noted. Extraocular movements were intact. Slit lamp examination revealed a central stellate corneal laceration, peaked 4mm non-reactive pupil, flat anterior chamber, and a falsely negative Seidel sign (Image 1). Intraocular pressure was not measured given the nature of the injury. Computed tomography (CT) orbits revealed a flat anterior chamber (Image 2). The patient was placed in an eye shield, treated for nausea/pain, initiated on antibiotics with levofloxacin, and updated on tetanus; ophthalmology then completed a surgical repair.
Image 1.
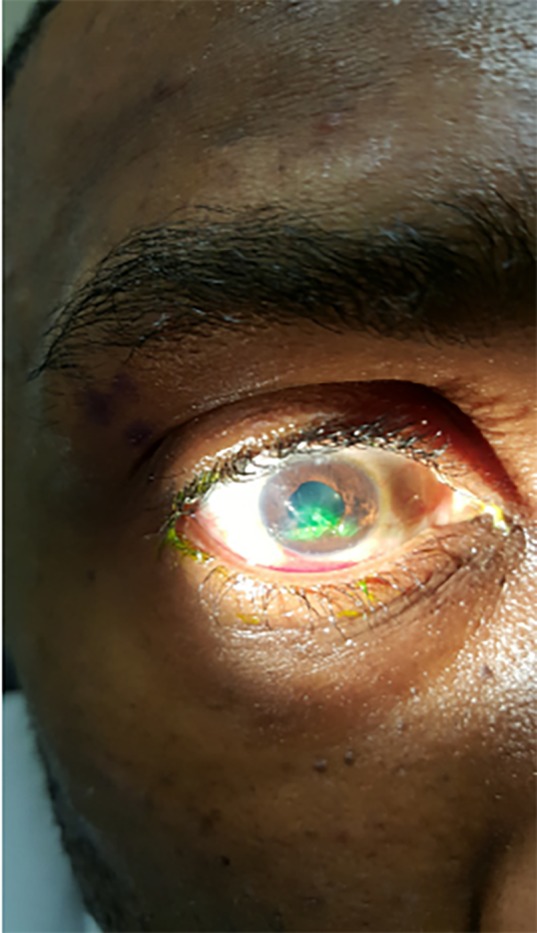
Stellate corneal laceration with negative Seidel Sign.
Image 2.

Computed tomography of the orbits, axial view, revealing right flat anterior chamber (yellow arrow) with iris abutting the cornea.
DISCUSSION
Ocular trauma accounts for roughly 3% of emergency department visits and is a major cause of unilateral visual impairment and permanent visual loss in young individuals.1,2 Open globe injuries occur more commonly in males and should be in the differential diagnosis with any injury involving high-velocity metal or glass.1,3 Penetrating mechanisms tend to be more common in the young, while a blunt mechanism is more common in the elderly.1,3 Exam findings can be subtle. Classic teaching revolves around Seidel’s sign; it is not sensitive, but it is specific.4 A globe rupture with false negative Seidel sign is a rare but known occurrence when ocular contents “plug” the opening, as seen in this patient, preventing aqueous outflow and causing a falsely negative Seidel sign. Other suggestive exam findings include a peaked pupil, poorly reactive pupil, flat anterior chamber, and visual acuity changes.4 Despite poor sensitivity, CT is very specific and can be helpful when identifying open globe injuries.
Documented patient informed consent and/or Institutional Review Board approval has been obtained and filed for publication of this case report.
CPC-EM Capsule.
What do we already know about this clinical entity?
Open globe rupture is an ophthalmologic emergency. Speedy recognition by the emergency department provider and ophthalmologic intervention are essential to restoring functional outcome.
What is the major impact of the image(s)?
A globe rupture with false negative Seidel sign is a rare but known occurrence when ocular contents “plug” the opening, as seen in this patient image.
How might this improve emergency medicine practice?
The case highlights the importance of good clinical exam after ocular trauma. Providers should consider further workup with computed tomography imaging with any injury involving high-velocity metal or glass.
Footnotes
Section Editor: Rick A. McPheeters, DO
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of MAMC, WBAMC, Kimbrough Ambulatory Care Center, the Department of the Army or the DOD.
REFERENCES
- 1.Cheung CA, Rogers-Martel M, Golas L, et al. Hospital-based ocular emergencies: epidemiology, treatment, and visual outcomes. Am J Emerg Med. 2014;32(3):221–4. doi: 10.1016/j.ajem.2013.11.015. [DOI] [PubMed] [Google Scholar]
- 2.Lin KY, Ngai P, Echegoyen JC, et al. Imaging in orbital trauma. Saudi J Ophthalmol. 2012;26(4):427–32. doi: 10.1016/j.sjopt.2012.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Armstrong GW, Kim JG, Linakis JG, et al. Pediatric eye injuries presenting to United States emergency departments: 2001–2007. Graefes Arch Clin Exp Ophthalmol. 2013;251(3):629–36. doi: 10.1007/s00417-011-1917-0. [DOI] [PubMed] [Google Scholar]
- 4.Ritson JE, Welch J. The management of open globe eye injuries: a discussion of the classification, diagnosis and management of open globe eye injuries. J R Nav Med Serv. 2013;99(3):127–30. [PubMed] [Google Scholar]
- 5.Duke-Elder S, MacFaul PA. System of Ophthalmology. CV Mosby; St. Louis: 1972. Injuries: Part 1 Mechanical Injuries; p. 14. [Google Scholar]