

Abstract
Objective:
To determine whether older workers who follow different work ability (WA) trajectories tend to follow different retirement pathways.
Methods:
Nationally representative data on Americans born between 1943 and 1948. Latent class growth modeling to estimate trajectories of work ability between ages 53–54 and 65–66. Multinomial log-linear models to assess the association between WA trajectories and retirement pathways.
Results:
Three WA trajectories were identified: high (74%), declining (17%), and low (9%). Low WA leads more often to an early-gradual retirement. Declining WA leads to both early-gradual and early-crisp retirements.
Conclusions:
Workers with low and declining WA are more at risk of unemployment, disability, and inactivity prior to retirement; workers with declining WA are also likely to make a direct transition to early retirement. Future changes to social security should consider inter-individual variation over time in WA.
Keywords: health and retirement study, latent growth class analysis, latent work ability trajectories, longitudinal, retirement, retirement pathways, retirement process, social security, United States, work ability, work ability index
Older workers with poorer health are at a greater risk of withdrawing from the labor force. As previous studies showed, workers with chronic conditions, poor self-assessed health, poor mental health, and musculoskeletal complaints are more likely to make a transition from work to disability pension, and to a lesser degree to unemployment or early retirement.1–6 In these studies, health was most often measured at one point in time and modeled as a dichotomous or multinomial outcome. Each respondent is followed until a transition from work into any non-work activity is observed and any subsequent events are disregarded. Thus, most papers that studied the impact of health on transitions out of the labor force at older ages have been implicitly assuming that (1) health is a black and white concept (good vs not good), that (2) poor health develops suddenly, and that (3) withdrawal from the labor force is instantaneous and permanent. This is at odds with the current theory. Indeed, health is better viewed as a continuum and as the result of some slowly changing process.7 Retirement, on the other hand, is a complex process that can stretch out over several years and that can take different forms.8,9
Researchers who study the impact of poor health on transitions out of the labor force have started to underline the need for more refined research strategies that take into account the dynamic and longitudinal aspects of health and retirement.10 The work ability (WA) index was developed in the 1980s and 1990s to better identify workers at risk of withdrawing from work due to health complaints.11 It is measured on a continuous scale and takes multiple dimensions of health in relation to work into account. Studies showed that, at the aggregate level, WA declines gradually with age, passing from good or excellent in young ages to moderate from age 60 onwards.12,13 There exists however a fair amount of variation between individuals at any point in time but also in individual trajectories over time. Variation in individual change in WA over time has been modeled according to latent trajectories where a finite number of trajectories are used to represent inter-individual heterogeneity. Studies found that managers with below optimal trajectories of WA tend to retire earlier14 while construction workers who manage to maintain high WA throughout their career are less at risk of reporting mental and physical strain in relation to their work at older age.15 Other studies that measured WA at one point in time found lower WA to predict subsequent sickness absences16,17 and disability pension.18–20 Results concerning early retirement and unemployment are mixed.18,19 One study examined change in WA between two points in time and found both baseline WA and a decrease in WA to predict transitions from work to disability pension.21 However, studies that considered both WA and retirement as longitudinal processes are still lacking.
The present paper describes the dynamic relationship between longitudinal trajectories of WA and retirement pathways. A nationally representative cohort of American older workers born between 1943 and 1948 is followed between ages 53–54 and 65–66. The analytic strategy reflects the continuous nature of health and allows to keep track of individual change in health over time. The retirement pathways are specified in a way that reflects the complexity and heterogeneity of the present American retirement landscape. Following the 1983 social security amendments,22 people born in 1943 are the first cohort to be eligible to full retirement benefits from age 66 onwards only. It is also the first cohort to have seen its early retirement benefits at age 62 being reduced to 75% of the full retirement benefits. Starting in 2020, other increases in the full retirement age and other decreases in the level of early retirement benefits at age 62 will be phased in, and further changes to social security are being discussed.23 In this context, it is thus important to understand how older workers who follow different WA trajectories make use of the different retirement options available. Although older workers with less than optimal WA trajectories can be predicted to retire earlier, it is still not clear whether older workers with different rates of decline in WA make use of different retirement options.
METHODS
Sample
The RAND HRS data file was used to run the analyses.24 The RAND HRS data file is an easy to use longitudinal data set based on data from the Health and Retirement Study (HRS).25 The HRS is a longitudinal survey representative of the American population age 50 and older. It is sponsored by the National Institute on Aging and is conducted by the University of Michigan. The HRS started in 1992 and participants were re-interviewed every second year thereafter. More respondents were added to the original sample in 1998, 2004, and 2010, resulting in four distinct survey cohorts. Interview response rates varied for each cohort between 66.2% and 81.6% in the first wave and between 85.4% and 92.3% in the subsequent waves.26
Respondents were selected for analyses based on a certain number of criteria. First, all respondents born between 1943 and 1948 who started participating to the HRS before reaching age 55 were selected (n = 2582). Second, respondents who died or permanently dropped out of the HRS before reaching ages 65 to 66 were excluded (n = 588; attrition rates varied between 3.5% and 5.6% at each wave). Third, respondents who were never observed working (n = 538) and respondents with missing health information at more than 5 waves (n = 39) were dropped, bringing the effective sample down to 1417 respondents.
Respondents who stopped participating to the HRS at one or many waves but who participated again at a later wave (temporary attrition) were kept in the sample. This approach was shown to limit significantly the effect of attrition on the representativity of the sample.27 A backlash of keeping respondents with temporary attrition is the unavailability of information on the labor force and health statuses at some waves. Labor force information was assumed to be missing at random. This may result in a somewhat distorted picture concerning the retirement pathways (presented below). However, the effect is likely small since the proportion of respondents with missing labor force information is very low at each wave as shown in Table 1. The effect on the construction of the work ability trajectories (again presented below) is assumed to be null as the method employed accommodates missing information at one or different points in time. The proportion of respondents with missing labor force and health information is depicted for each wave in Table 1.
TABLE 1.
Number of Respondents With Missing Labor Force and Health Information, by Wave (Percentages in Parenthesis, n = 1,417)
| Wave | |||||||
| Type of Information | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Labor force | 42 (3.0) | 68 (4.8) | 53 (3.7) | 63 (4.4) | 64 (4.5) | 59 (4.2) | 42 (3.0) |
| Health | 105 (7.4) | 172 (12.1) | 194 (13.7) | 204 (14.4) | 143 (10.1) | 131 (9.2) | 136 (9.6) |
Retirement Pathways
A retirement typology was developed to account for inter-individual heterogeneity in retirement processes. The typology was inspired by previous theories and empirical research.28–30 Two dimensions were retained as being particularly relevant for describing the retirement process: timing and mode of entry. Although more dimensions could have been considered, this solution was retained to facilitate the interpretation of the results. In this research, timing referred to the notion of early versus late retirement, while mode of entry opposed crisp to gradual retirement. These two dimensions provided the four retirement pathways 1. Early-Crisp, 2. Early-Gradual, 3. Late-Crisp, and 4. Late-Gradual.
Respondents were assigned to one of these four retirement pathways based on their sequence of labor statuses over the seven waves. Labor status was assessed using the RAND HRS variable lbrf.31 The original version of this variable contained seven categories. Some categories were merged to facilitate the construction of the pathways, resulting in the following four categories: 1. Works full time; 2. Works part-time/partly retired; 3. Retired; 4. Other (containing unemployed/disabled/not in the labor force). Respondents were considered to have retired early if they were observed in state 3. (retired) at two waves or more, as having retired late otherwise. Respondents were considered to have gone through a crisp retirement if they were observed in either state 2. (works part-time/partly retired) or 4. (unemployed/disabled/not in the labor force) at one wave or less for the late retirees and two waves or less for the early retirees; the rest was correspondingly considered to have gone through a gradual retirement. The cutoffs were set arbitrarily while aiming at having groups with balanced numbers of respondents.
Work Ability
WA was defined based on the WA index11 to which some changes were brought due to the limited information contained in the RAND HRS data set. In its standard form, the WA index is based on a seven items questionnaire. The following refers to items 1 to 7 of the WA index’ questionnaire as described in de Zwart et al.32 Items 1 and 6 refer to the respondent's self-reported work ability in the past and over 2 years, respectively. Since the trajectories already capture change over time, these items were excluded. Item 2 was replaced by self-rated health, as the data did not contain information on the respondents’ self-assessed WA in relation to his or her work demands. Self-rated health was measured on a five categories scale ranging from 5. “Excellent” to 1. “Poor”. Item 3 measures the number of diseases at the time of the interview. The diseases that were taken into account here were: high blood pressure, diabetes, any form of cancer, lung disease, heart disease, stroke, and arthritis. Item 4 asks the respondent whether he or she has any work impairment due to a disease. It was measured here based on the question: “Do you have any impairment or health problem that limits the kind or amount of paid work you can do?”. Item 5 (sick leave in the past year) was replaced by whether the respondent had any hospital overnight stay over the last 2 years. Item 7 concerns the mental resources of the respondent and was here based on the score obtained on the Center for Epidemiological Studies Depression 8 scale.33 Each item used here was given a similar score as in the original index. This five item index implies that individual scores vary between 5 and 32 (rather than between 7 and 49 in the original version), a score of 32 meaning optimal WA. It should be stressed that compared with the original index, the index used here is constructed on fewer questions that specifically refer to someone's work or work ability. The index used here might therefore reflect less a person's work ability and more a person's general health status instead.
Socio-Demographic Variables
Socio-demographic variables included sex, year of birth (2 years groups), education (reconverted into less than high school degree, high school degree only, and at least some college degree), and race (non-Hispanic white race or ethnicity vs any other race or ethnicity).
Analyses
WA trajectories were identified using the R package lcmm.34 This package allows to perform latent class growth analysis (LCGA), a method that is based on maximum likelihood.35 LCGA allows to model individual change over time in a continuous or discrete outcome while allowing for different unobserved subpopulations to follow different trajectories. Each individual in the data set was assigned to the latent class that fitted best his or her own change over time in WA. The chosen model includes three latent classes and change over time in the value of the WA index was modeled using a linear link function. Although some other models based on a different number of latent classes and different link functions provided better fits (as based on the Bayesian information criterion), this three-classes model was preferred for its greater parsimony, better balance between group sizes, and better ease of interpretation of the change over time in the predicted values of the WA index. The function lcmm was used to fit the model and the post-estimation command predictY was used to obtain the predicted values.
The associations between the latent classes of the WA trajectories and the different retirement pathways were assessed using a multinomial log linear model with the retirement pathways as dependent variable. The results are presented as the predicted marginal mean inside of each latent WA trajectory with the 95% confidence bounds. Only the model including the socio-demographic confounders is presented as the introduction of these variables did not affect the significance of the associations between the WA trajectories and the retirement pathways.
RESULTS
Descriptive Analysis
Figure 1 presents the proportion of respondents that correspond to each labor force status by year of age, for each retirement pathway. The sequences of labor force statuses that correspond to the respondents who were observed retiring early are pictured in the top, while the ones of those who were observed retiring late are pictured in the bottom. Furthermore, the sequences of labor force statuses that correspond to the respondents who were observed going through a crisp retirement are pictured on the left-hand side, while the ones of those who were observed going through a gradual retirement are pictured on the right-hand side. The Early-Crisp and Early-Gradual pathways (top) contain at older ages a much bigger proportion of respondents with labor status “Retired” than the Late-Crisp and Late-Gradual patterns (bottom). In the meanwhile, the Early-Crisp and Late-Crisp pathways (left) contain almost exclusively respondents that are either working full time or retired, while the Early-Gradual and Late-Gradual patterns (right) contain at each age the largest shares of participants with the labor statuses “Other” and “Partly retired.” As indicated in the graph titles, a bit more than one fifth of the respondents were assigned to the Early-Crisp pathway and just over one out of six to the Early-Gradual pathway. In the meanwhile, a little more than one fourth was assigned to the Late-Crisp pathway and about one out of three was assigned to the Late-Gradual pathway.
FIGURE 1.
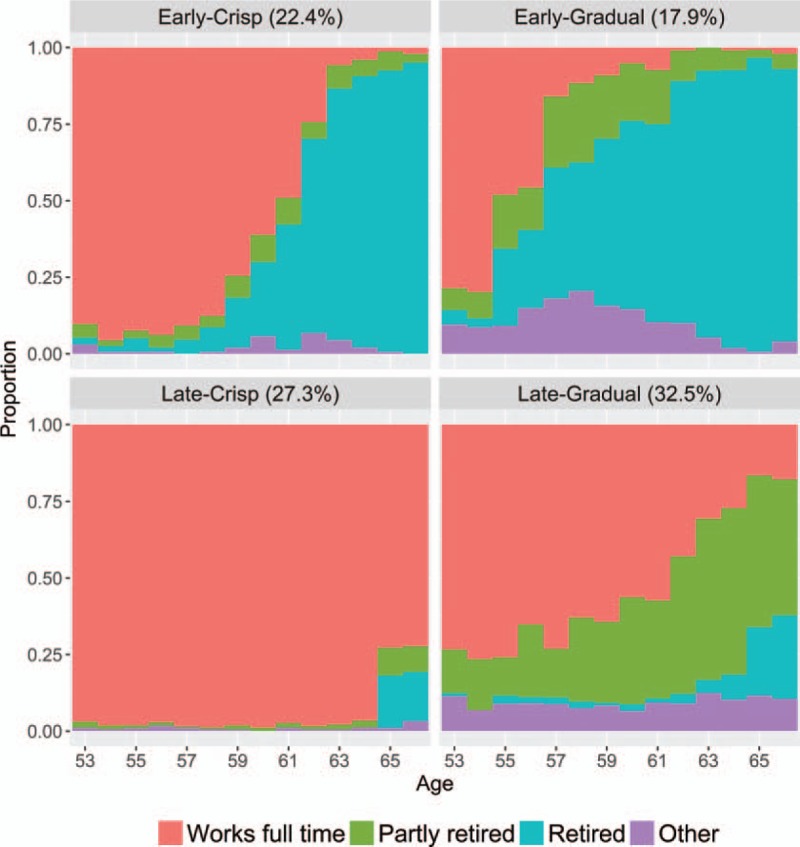
Cross-sectional overview of labor force status by year of age and retirement pathway (with proportion in sample). The areas give the proportion of respondents that correspond to each labor force status as shown in the legend.
Figure 2 shows the variation according to age in the predicted values on the WA index, by latent class. The classes were labeled “High,” “Declining,” and “Low.” The model assigned about three fourth of the sample to the high trajectory, about one sixth to the declining trajectory, and a little less than one tenth to the low trajectory.
FIGURE 2.
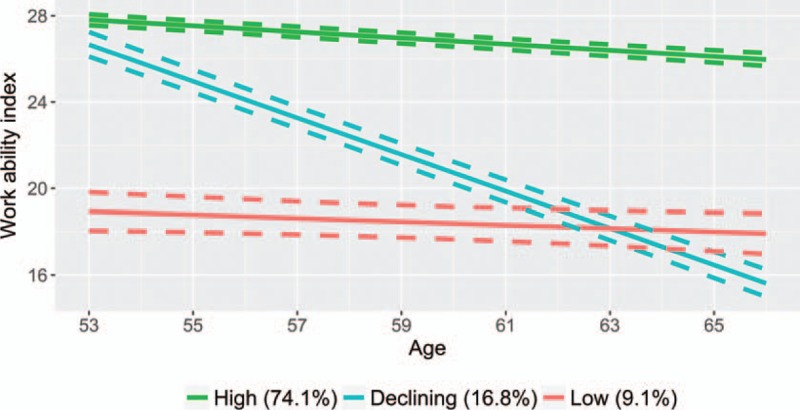
Trajectories of work ability as measured based on an adaptation of the work ability index (the dashes represent the 95% confidence bounds).
Table 2 shows that in the sample used, more than half of the respondents were women. About a third of the sample was born in 1943 to 1944. The figures are slightly higher for the cohort born in 1945 to 1946 and slightly lower for the cohort born in 1947 to 1948. Only a minority of respondents had no high school degree, while about half of the sample had a high school degree only, and one third had a college degree or more. More than three quarters of the sample was of non-Hispanic white race or ethnicity.
TABLE 2.
Socio-Demographic Variables, Count and Proportion in Sample
| Variable/Modality | Count | Proportion |
| Female gender | 842 | 59.4 |
| Cohort | ||
| 1943–1944 | 479 | 33.8 |
| 1945–1946 | 546 | 38.5 |
| 1947–1948 | 392 | 27.7 |
| Education | ||
| No high school | 211 | 14.9 |
| High school only | 737 | 52.0 |
| At least some college | 469 | 33.1 |
| Non-hispanic white race or ethnicity | 1084 | 76.5 |
| Total | 1,417 | 100.0 |
Multivariate Analysis
Figure 3 shows the results of the multinomial model. The predicted marginal means are grouped by retirement pathway. Respondents who were assigned to the high WA trajectory were more likely than respondents assigned to the two other trajectories to have gone through a late and crisp retirement pathway. Furthermore, respondents who followed the high WA trajectory were more likely than the respondents assigned to the declining WA trajectory to experience a late and gradual retirement. The respondents who were assigned to the declining WA trajectory were more likely to go through an early and crisp retirement pathway in comparison to the respondents that were assigned to the two other trajectories. Finally, both the respondents who were assigned to the declining and to the low WA trajectory were more susceptible than respondents who were assigned to the high WA trajectory to experience an early and gradual retirement.
FIGURE 3.
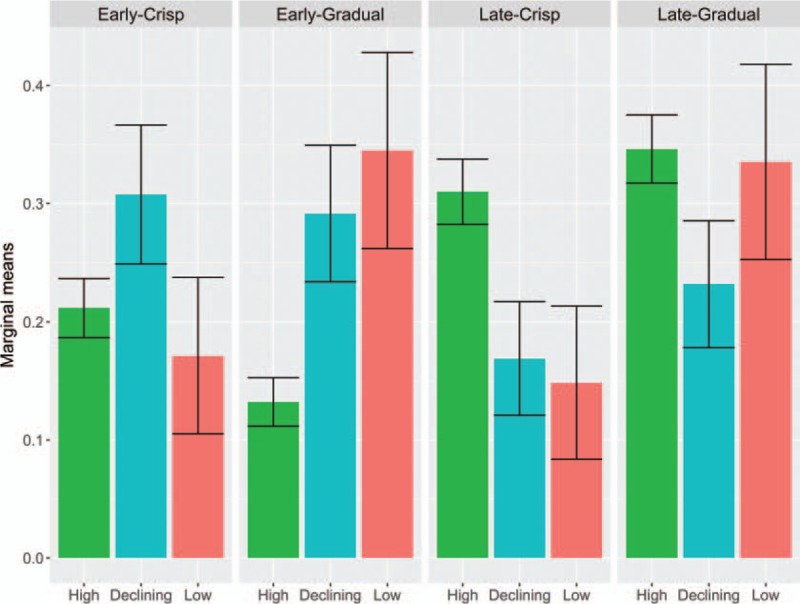
Predicted marginal means by class of work ability trajectory, for each category of the retirement pathways, with 95% confidence bounds.
DISCUSSION
Summary of Results
This study unraveled the dynamic associations between WA trajectories and retirement pathways among a cohort of American workers followed from ages 53–54 to ages 65–66. Each retirement pathway represented different labor force behaviors in the years preceding the official retirement age of 66 years old. These different behaviors are largely influenced by the available retirement options offered by social security in the United States.36 The early-crisp retirement pathway probably represented mostly people who benefited from early retirement benefits because many of them were observed making a direct transition from work to complete retirement around the age of 62 years old. The early-gradual pathway contained many respondents corresponding to the labor status “Other,” especially prior to age 62. This labor status was made up of survey participants who identified themselves as unemployed, disabled, or out of the labor force. Therefore, the respondents who followed an early-gradual retirement pathway probably benefited from unemployment and disability benefits prior to benefiting from early retirement benefits. The late-crisp pathway represented people who chose to retire at the full retirement age only, or who even delayed their retirement beyond the age of 66 years old thus benefiting from delayed retirement credits. Respondents who were part of the late-gradual pathway probably profited of part time or partial retirements arrangements with their employer, and may even have benefited from some early retirement benefits while continuing to work.37
In parallel to the retirement pathways, respondents were assigned to one of three latent classes that best described their individual change over time in values of the WA index. These WA trajectories were specified using LCGA.34 The model containing as trajectories high WA, declining WA, and low WA was retained, though other possibilities could have been chosen. Some trajectories were found to be more strongly linked with specific retirement pathways. According to the expectation formulated in the introduction, respondents who maintained a high WA throughout the observation kept more often working until the full retirement age, either full time or on a reduced basis (part time or partly retired). This finding confirms the results of a previous study that found that people who maintain a high WA also tend to retire later.14 The finding that they made more use of partial retirement arrangements than people with declining WA is however novel. It is somewhat surprising too, since it was suggested that gradually reducing the amount of work could help workers with deteriorating work ability to stay longer on the labor market. However, our findings do not find any support for this kind of behavior. Respondents with declining WA tended to retire earlier. They did so by either making a crisp transition from work into retirement from about age 60 or 62 onwards, or by retiring gradually, including stints of unemployment, disability, and inactivity. Respondents with constantly low WA also tended to retire early, but they only did so by retiring gradually and by thereby spending time unemployed, disabled, or out of the labor force. Older workers with different rates of decline in WA thus do differ to some extent in their use of the different retirement options: respondents with declining WA tend to make more use of both the early retirement pathways (crisp and gradual) while respondents with low WA tend to make more use of the early-gradual retirement pathway only.
Strengths and Limitations
The strengths of this study were its longitudinal and dynamic design that exploited the full potential offered by the data.10 More specifically, both retirement and WA were conceptualized taking the whole period of observation into consideration, a period that covered 12 years. The use of retirement pathways allowed to render better than most studies the variety of retirement patterns that exist in the United States. The finding that there is important heterogeneity in retirement pathways among American older workers is in line with other studies.38–40 The use of LCGA allowed to model health as a continuous, age-dependent latent process which better corresponds to the present theory of health.7 The representativeness of the data at the national level was another strength of this research as the other studies that investigated the link between WA trajectories and retirement focused on specific groups only, that is, managers and construction workers.14,15
This study had to face some limitations. A first set of limitations concern the specification of the retirement pathways. The proportions of people in the American population who follow one of the four retirement pathways may differ from those observed here. First, the pathways were specified based on information available in average 2 years apart. Therefore, the actual number of transitions that are made between labor force statuses at older ages was probably underestimated.29 On the other hand, the assumption that labor force information was missing at random may have resulted in an overestimation of the number of respondents with the statuses “Partly-retired” and “Other,” which were less often observed than the statuses “Working full-time” and “Retired.” This may in turn have contributed to underestimating the amount of crisp transitions into retirement. Also, transitions in and out of retirement were not explicitly taken into account in the specification of the pathways. Although classic retirement theory28 did not consider this dimension either, more recent work showed that many American workers “unretire”, that is, they make transitions from retirement back to work. More research will therefore be needed to unravel the associations between change in health and transitions out of retirement.
A second set of limitations concerns the estimation of the work ability trajectories. The specification of the WA index used in this study differed slightly from the most commonly accepted one.32 Therefore, the comparability of this study with other ones that also used the WA index may not be optimal. The reader should also keep in mind that the cohort followed in this study was made of respondents who survived to at least age 66 and who were observed working at least at one wave. Therefore, the outcome of the LCGA modeling likely underestimated the proportion of people in the population who has declining or poor WA at these ages. Furthermore, the method used does not allow to establish a direction of causality between change over time in work ability and change over time in retirement statuses. It seems however unlikely that change in retirement status had any important impact on the trajectories of ability to work. First, the work ability trajectories are based on a latent construct that take many aspects of health into consideration. Second, individuals are assigned to the trajectory that best describes their own change in work ability over time; therefore, no individual follows exactly the change in work ability that is predicted by the model.41 It is possible that health changes following retirement, at least according to some dimensions.42 However, such changes are not captured by the model as no non-monotonous trajectories were found to satisfactorily describe change in work ability in this sample.
A third set of limitations concerns the control variables used in this analysis. Due to missing information among many respondents, the analyses did not take into account the occupational class or any characteristics of the respondents’ work. Although including such information would probably not have changed dramatically the results, they would probably have mitigated the strength of the associations between the WA trajectories and the retirement pathways.19
Finally, a word on the generalizability of the results to other countries. Unlike in most European countries, there is high heterogeneity in retirement behavior in the United States. The American retirement landscape features more instances of gradual retirement and “unretirement” while retirement in Europe consist more often of single and unidirectional transitions.38,39 However, studies have shown that retirement in Europe increasingly takes diverse forms.43 Therefore, the observations made here may be indicative of the future situation of European countries.
CONCLUSION
Social security in the United States is going through a period of reforms22 and calls for further increasing the ages of admissibility to full and reduced retirement benefits are being heard.23 People with declining and low WA in their fifties and sixties are less likely to reach the full retirement age while still working, either full or part time. Given the current proportions of people who enter the latter part of their career with declining or low WA, increasing the age of admissibility to full benefits will force more people to rely on early retirement benefits for a longer period of time. People with declining WA more often made a direct transition from work to early retirement and more often made a gradual transition to early retirement, including stints of unemployment, disability, and inactivity. People who entered the latter part of their career with an already low WA made more use of the latter option only. Therefore, increasing the age of availability to early retirement benefits might force people to make use of unemployment and disability benefits or to be inactive for a longer period of time. Conversely, helping people to maintain a high level of WA prior to reaching the latter part of their career, and helping them to delay the onset of the decline in WA, might reduce the amount of people who make use of unemployment, disability, and early retirement benefits altogether.
Footnotes
Funding: This work was funded by the Dutch Royal Academy of Sciences (Koninklijke Nederlandse Akademie van Wetenschappen, project DeLaForce https://www.nidi.knaw.nl/en/research/al/270024).
Conflicts of Interest: None declared.
REFERENCES
- 1.van Rijn RM, Robroek SJ, Brouwer S, Burdorf A. Influence of poor health on exit from paid employment: a systematic review. Occup Environ Med 2014; 71:295–301. [DOI] [PubMed] [Google Scholar]
- 2.Leijten FR, de Wind A, van den Heuvel SG, et al. The influence of chronic health problems and work-related factors on loss of paid employment among older workers. J Epidemiol Community Health 2015; 69:1058–1065. [DOI] [PubMed] [Google Scholar]
- 3.Robroek SJ, Rongen A, Arts CH, Otten FW, Burdorf A, Schuring M. Educational inequalities in exit from paid employment among Dutch workers: the influence of health, lifestyle and work. PLoS One 2015; 10:e0134867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Palmer KT, Goodson N. Ageing, musculoskeletal health and work. Best Pract Res Clin Rheumatol 2015; 29:391–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kouwenhoven-Pasmooij TA, Burdorf A, Roos-Hesselink JW, Hunink MG, Robroek SJ. Cardiovascular disease, diabetes and early exit from paid employment in Europe; the impact of work-related factors. Int J Cardiol 2016; 215:332–337. [DOI] [PubMed] [Google Scholar]
- 6.Leinonen T, Laaksonen M, Chandola T, Martikainen P. Health as a predictor of early retirement before and after introduction of a flexible statutory pension age in Finland. Soc Sci Med 2016; 158:149–157. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland:World Health Organization; 2001. [Google Scholar]
- 8.Beehr TA. To retire or not to retire: that is not the question. J Organ Behav 2014; 35:1093–1108. [Google Scholar]
- 9.Wang M, Shultz KS. Employee retirement: a review and recommendations for future investigation. J Manag 2010; 36:172–206. [Google Scholar]
- 10.Burdorf A. The need for novel strategies to analyze the dynamic pattern of worker's health over time and the consequences for sustained employability. Scand J Work Environ Health 2012; 38:485–488. [DOI] [PubMed] [Google Scholar]
- 11.Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A. Work ability index. Helsinki:Institute of Occupational Health; 1994. [Google Scholar]
- 12.Ilmarinen J, Tuomi K, Klockars M. Changes in the work ability of active employees over an 11-year period. Scand J Work Environ Health 1997; 23 suppl:49–57. [PubMed] [Google Scholar]
- 13.Ilmarinen J, Ilmarinen V. Finkelstein LM, Truxillo DM, Fraccaroli F, Kanfer R. Work ability and aging. Facing the Challenges of a Multi-Age Workforce: A Use-Inspired Approach. London, UK:Routledge; 2015. 134–156. [Google Scholar]
- 14.Feldt T, Hyvönen K, Mäkikangas A, Kinnunen U, Kokko K. Development trajectories of Finnish managers’ work ability over a 10-year follow-up period. Scand J Work Environ Health 2009; 35:37–47. [DOI] [PubMed] [Google Scholar]
- 15.von Bonsdorff ME, Kokko K, Seitsamo J, et al. Work strain in midlife and 28-year work ability trajectories. Scand J Work Environ Health 2011; 37:455–463. [DOI] [PubMed] [Google Scholar]
- 16.Schouten LS, Bültmann U, Heymans MW, Joling CI, Twisk JW, Roelen CA. Shortened version of the work ability index to identify workers at risk of long-term sickness absence. Eur J Public Health 2016; 26:301–305. [DOI] [PubMed] [Google Scholar]
- 17.Ohta M, Higuchi Y, Kumashiro M, Yamato H, Sugimura H. Decrease in work ability index and sickness absence during the following year: a two-year follow-up study. Int Arch Occup Environ Health 2017; 90:883–894. [DOI] [PubMed] [Google Scholar]
- 18.Lundin A, Kjellberg K, Leijon O, Punnett L, Hemmingsson T. The association between self-assessed future work ability and long-term sickness absence, disability pension and unemployment in a general working population: a 7-year follow-up study. J Occup Rehabil 2016; 26:195–203. [DOI] [PubMed] [Google Scholar]
- 19.Roelen CA, Heymans MW, Twisk JW, van der Klink JJ, Groothoff JW, van Rhenen W. Work Ability Index as tool to identify workers at risk of premature work exit. J Occup Rehabil 2014; 24:747–754. [DOI] [PubMed] [Google Scholar]
- 20.Alavinia SM, De Boer AGEM, Van Duivenbooden JC, Frings-Dresen MHW, Burdorf A. Determinants of work ability and its predictive value for disability. Occup Med (Lond) 2008; 59:32–37. [DOI] [PubMed] [Google Scholar]
- 21.Jääskeläinen A, Kausto J, Seitsamo J, et al. Work ability index and perceived work ability as predictors of disability pension: a prospective study among Finnish municipal employees. Scand J Work Environ Health 2016; 42:490–499. [DOI] [PubMed] [Google Scholar]
- 22.Svahn JA, Ross M. Social Security Amendments of 1983: legislative history and summary of provisions. Soc Secur Bull 1983; 46:3–48. [PubMed] [Google Scholar]
- 23.Kingson E, Altman N. The social security retirement age (s) debate: perspectives and consequences. Public Policy Aging Rep 2011; 21:3–9.26755892 [Google Scholar]
- 24.RAND HRS Data, Version P. Produced by the RAND Center for the Study of Aging, with funding from the National Institute on Aging and the Social Security Administration. Santa Monica, CA (August 2016). [Google Scholar]
- 25.Health and Retirement Study, RAND HRS Data Public Use Dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI; 2017. [Google Scholar]
- 26.HRS. Sample size and response rate. Available at: http://hrsonline.isr.umich.edu/sitedocs/sampleresponse.pdf Accessed December 4, 2018. [Google Scholar]
- 27.Michaud PC, Kapteyn A, Smith JP, Van Soest A. Temporary and permanent unit non-response in follow-up interviews of the Health and Retirement Study. Longitudinal Life Course Stud 2011; 2:145–169. [Google Scholar]
- 28.Beehr TA. The process of retirement: a review and recommendations for future investigation. Pers Psychol 1986; 39:31–55. [Google Scholar]
- 29.Mutchler JE, Burr JA, Pienta AM, Massagli MP. Pathways to labor force exit: work transitions and work instability. J Gerontol B Psychol Sci Soc Sci 1997; 52B:S4–S12. [DOI] [PubMed] [Google Scholar]
- 30.Fisher GG, Chaffee DS, Sonnega A. Retirement timing: a review and recommendations for future research. Work Aging Retirement 2016; 22:230–261. [Google Scholar]
- 31.Bugliari D, Campbell N, Chan C, et al. Rand Hrs Data Documentation, Version P. Santa Monica, CA, USA:RAND Center for the Study of Aging; 2016. [Google Scholar]
- 32.De Zwart BC, Frings-Dresen MH, Van Duivenbooden JC. Test–retest reliability of the Work Ability Index questionnaire. Occup Med (Lond) 2002; 52:177–181. [DOI] [PubMed] [Google Scholar]
- 33.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measure 1977; 1:385–401. [Google Scholar]
- 34.Proust-Lima C, Philipps V, Liquet B. Estimation of extended mixed models using latent classes and latent processes: the R package lcmm. arXiv preprint arXiv:1503.00890; 2015 Mar 3. [Google Scholar]
- 35.Muthén B, Muthén LK. Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcohol Clin Exp Res 2000; 24:882–891. [PubMed] [Google Scholar]
- 36.Coile C, Gruber J. The Effect of Social Security on Retirement in the United States. In Social Security Programs and Retirement Around the World: Micro-estimation. 2004; Chicago, IL:University of Chicago Press, 691–730. [Google Scholar]
- 37.Feldman DC. The decision to retire early: A review and conceptualization. Acad Manage Rev 1994; 19:285–311. [Google Scholar]
- 38.Cahill KE, Giandrea MD, Quinn JF. Retirement patterns and the macroeconomy, 1992-2010: the prevalence and determinants of bridge jobs, phased retirement, and reentry among three recent cohorts of older Americans. Gerontologist 2013; 55:384–403. [DOI] [PubMed] [Google Scholar]
- 39.Maestas N. Back to work expectations and realizations of work after retirement. J Hum Resour 2010; 45:718–748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cahill KE, Giandrea MD, Quinn JF. Retirement patterns from career employment. Gerontologist 2006; 46:514–523. [DOI] [PubMed] [Google Scholar]
- 41.Nagin DS, Odgers CL. Group-based trajectory modeling (nearly) two decades later. J Quant Criminol 2010; 26:445–453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Van der Heide I, van Rijn RM, Robroek SJ, Burdorf A, Proper KI. Is retirement good for your health? A systematic review of longitudinal studies. BMC Public Health 2013; 13:1180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kanabar R. Unretirement in England: An Empirical Perspective. Discussion Papers in Economics; 2012. Jul 29 (12/31). [Google Scholar]