

Abstract
Hip muscle strengthening and knee extensor strengthening are common training exercises for patellofemoral pain syndrome (PFPS). PFPS engendered by insufficient hip abductor and external rotator muscle strength has been of interest, but these exercise movements may increase the lateral vector force of the patella warrants clarification. So, the purpose of this study was to assess muscular activations of vastus lateralis (VL), vastus medialis oblique (VMO), and gluteus medius muscles in electromyographic analysis during hip abduction and external rotator movements and open and closed kinetic chain knee extension movements.
The gluteus medius, VMO, and VL muscles, in addition to the ratio of the VL and VMO muscles, were assessed through surface electromyography in 4 movements. Each muscle's amplitude expressed as a percent of maximum voluntary contraction (MVC). The differences on MVC at the terminal joint angle and during the movements were compared.
Thirty female patients with PFPS were recruited. During hip abduction and external rotation movements, the MVC of the gluteus medius muscle increased, and those of the VMO and VL muscles increased in the open and closed kinetic chain knee extension movements. The MVCs of VL in the hip abduction and external rotation movements were significantly higher than those of the VMO muscle (P < .05). The ratios of the VL and VMO muscles in the open and closed kinetic chain knee extension movements approached 1, and they were significantly higher than those in the hip abduction and external rotation movements (P < .05). The highest MVC of the VMO muscle was observed at the terminal joint angle in the closed kinetic chain knee extension movement.
Selective gluteus medius muscle activation was induced during the hip abduction and external rotation movements, accompanied by an increase in VL muscle activation. In open and closed kinetic chain knee movements, the ratios of the VL and VMO muscles approached 1. More selective VMO muscle activation was induced during the closed kinetic chain knee movements.
Keywords: electromyography, maximum voluntary contraction, patellofemoral pain syndrome
1. Introduction
Patellofemoral pain syndrome (PFPS) is a common musculoskeletal disease. A previous study reported that the incidence of PFPS was almost 25%, and the proportion of females to males with PFPS was 2:1.[1] Presently, the causes of PFPS are unclear, and the abnormal biomechanics of patellar malalignment and muscle imbalance may be factors of the occurrence of PFPS.[2] When the knee moves to extension, the vastus medialis oblique (VMO) and vastus lateralis (VL) muscles control the patellar tracking in the trochlear groove. The imbalance in VMO and VL muscle activities caused patellar malalignment, resulting in an increasing lateral vector force and intra-articular pressure on the patella.[3] The patellar cartilage was worn continuously through abnormal patellar tracking, producing patellar pain, instability, and dysfunction.[4] Rehabilitation treatment for PFPS had focused on VMO muscle strengthening to correct patellar malalignment.[5] A previous study reported that specific exercise activities focusing on VMO muscle training were effective in pain reduction and functional ability improvement in patients with PFPS.[6] Increasing the medial vector force of the patella, particularly through VMO muscle training, and improving VMO and VL muscle balance and patellar stability are a common strategy of physical therapy for PFPS.[5]
In recent years, PFPS engendered by insufficient hip abductor and external rotator muscle strength has been of interest to fitness trainers and athletic trainers.[7] The importance of strength training in maintaining the hip abductor and external rotator muscle strength was highlighted by a previous study.[8] Compared with healthy control group, a 21% to 29% decrease in hip abductor and external rotator muscle strength was observed in patients with PFPS.[9] A systematic review provided an evidence-based result, which indicated that hip abductor and external rotator muscle training for the treatment of PFPS demonstrated considerable pain amelioration.[10] Hip abductor and external rotator muscle weakness could result in excessive internal rotation of the lower extremity. A reversed femoral position predisposed the patella to contact with the lateral trochlear groove, causing PFPS.[11] Fukuda et al[12] demonstrated that a 4-week hip abductor and external rotator muscle exercises were effective in pain, function, and functional strength improvement in patients with PFPS. Almeida et al[13] explored the association of dynamic knee valgus with hip abductor strength, pain, and function in PFPS. They observed that dynamic knee valgus (Q angle of knee) had no correlations with hip abductor muscle strength, pain, or function in women with PFPS. However, this study was insufficient to prove that strengthening of hip abductor and external rotator muscles has positive effects on patellar malalignment correction.
The hip abductor and external rotator muscles (i.e., tensor fascia lata and gluteus medius muscles) attach to the pelvis to extend the lateral patella through the iliotibial band. Whether hip abductor and external rotator muscle exercises increase the lateral vector force of the patella warrants clarification. These exercises could incorporate hip abductor and external rotator muscle training activities and also induce VL muscle activity through muscular cocontraction. Moreover, they may increase the intra-articular pressure on the patella, leading to an increased risk of PFPS. According to a review of the relevant literatures, no study had compared the gluteus medius, VL, and VMO muscle activation mechanisms during the movements of hip abductor and hip external rotator muscle exercises, and open and closed kinetic chain knee extension exercises. Therefore, the purpose of this study was to assess muscular activations of VL, VMO, and gluteus medius muscles in electromyographic analysis. Specifically, we wanted to determine the muscular activations in 4 exercise movements.
2. Methods
2.1. Participants
The participants were female patients with PFPS, who were recruited from China Medical University Hospital. The patients were assessed by a physician, and inclusion criteria were as follows: positive patellar compression test or tenderness around the patella; persistent anterior knee pain for at least 6 months; and pain during at least any 2 of the following: kneeling, prolonged sitting, squatting, and ascending and descending stairs. Exclusion criteria were a history of patellar dislocation, subluxation or any surgery on the lower extremity, and feel painful to perform the next exercise movements testing. These movements were pain-free exercises for PFPS, which did not affect on firing the motor unit of muscles.[14] The volunteers were informed about the study aim and experimental procedure before participation, and written informed consent was obtained. The study was approved by the Institutional Review Board of China Medical University Hospital (No. CRREC-104-093).
The sample size was estimated using G∗Power software (G∗Power 3.1.9.2, Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). The variables of muscular activations were assessed through electromyography by referring to the study results of Chang et al.[4] They detected a medium effect size on VMO and VL muscle activations of PFPS patients during sling-based exercises at a P = .05 and power = 80%, and estimated sample size was at least 15 patients. So, in the present study, the sample size was set at 30 patients.
2.2. Electromyographic activity
A surface electromyograph (MyoTrace TM 400, Noraxon Inc., Scottsdale, AZ) was used and synchronized with an electronic goniometer (NorAngle Electrogoniometer System, Noraxon Inc.). Muscle activation and joint motion signals were recorded synchronously. Electrodes (Medi-Trace 200, Kendall, FL) were attached to 3 belly muscles (i.e., the gluteus medius, VMO, and VL muscles). The interelectrode distance was 2 cm. The electrode for VL was positioned on the line from the anterior superior iliac spine to the superolateral border of the patella and attached at 10 cm from the superolateral border of the patella. The electrode for VMO was positioned at 4 cm from the superomedial border of the patella at 50° vertically. The electrode for gluteus medius was positioned on the line between the greater trochanter and top of the iliac crest, and placed at 34% of the distance from the greater trochanter (Fig. 1). These standardized electrode positions were adopted from a previous study.[15] Before the electrodes were attached to the muscles, the skin was wiped with alcohol swabs to reduce the electrical impedance.
Figure 1.

Electrodes for VMO, VL (A), and gluteus medius muscles (B). VL = vastus lateralis, VMO = vastus medialis oblique.
2.3. Maximum voluntary contraction test
Before the initiation of the test procedure, demographic data of patients with PFPS, such as age, height, weight, and body mass index, were collected. First, an electronic dynamometer (Hoggan Micro-Fet3, Utah, USA) was used to measure the maximum isometric knee extension strength during knee extension, hip abduction, and hip external rotation movements. Each movement was tested 3 times, and the rest interval was 10 seconds. The electronic dynamometer had moderate to excellent test–retest reliability (intraclass correlation coefficient [ICC] 0.56–0.92) and was valid for measuring the maximum voluntary isometric contraction of hip and knee muscles.[16] Subsequently, the muscle activities during maximum voluntary contraction (MVC) of knee extension and hip abduction were recorded through surface electromyography. Surface electromyography, which had acceptable reliability (ICC > 0.7) in gluteus medius, VMO, and VL muscles, can be collected in PFPS patients.[17] Electromyographic patches were placed over the VL, VMO, and gluteus medius muscles. For the knee extension MVC test, the patient was seated on an N-K table (N-K Products Co, Inc., Soquel, CA) with the hip flexed at 90° and knee flexed at 60° from extension. The movement arm of the N-K table was rotated to 60° of knee flexion for maximal isometric knee extension trials.[18] For MVC tests in hip abduction, the patient was positioned in a side-lying position, with the testing leg placed at 30° of hip abduction above the other leg. A belt was applied on the testing leg for maximal isometric hip abduction trials.[19] Both positions were standardized for the patients and were installed by the same physical therapist. The patients performed each trial for 5 seconds with a 2-minute rest interval between 3 repetitions. A 10-minute rest interval between trials was provided to prevent muscular exhaustion. Verbal encouragement was provided for maximum isometric muscle contraction. The electromyographic signals of the VMO, VL, and gluteus medius muscles were recorded during each test.
2.4. Exercise movement testing procedure
On the following day, the patients with PFPS practiced 4 exercise movements (Fig. 2), namely hip abductor exercise, hip external rotator exercise, and open and closed kinetic chain knee extension exercises, and the activities of the VMO, VL, and gluteus medius muscles were recorded simultaneously. Prior to the exercise movements, a warm-up exercise was performed on a stationary bike for 10 minutes at a submaximal speed. Four sets of exercise movements were practiced under a randomly arranged test sequence. Before the exercise movements were tested, detailed verbal descriptions were provided. Electromyographic patches were positioned over the VL, VMO, and gluteus medius muscles, and skin debris was removed using alcohol cotton pads.
Figure 2.
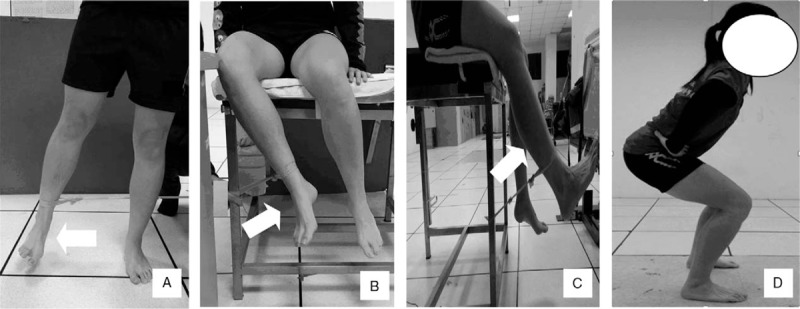
Specific exercise movements, including hip abductor exercise (A), hip external rotator exercise (B), and open and closed kinetic chain knee extension (C, D) exercises.
During the measurement of the angle of motion in hip abduction movement by using the electronic goniometer, the lever arms were fixed by tape and placed on the front of the thigh and the line between the anterior superior iliac spine of the pelvis. The axis was located in the anterior superior iliac spine of the measured side. During the measurement of the angle of motion in hip external rotation movement, the axis of the electronic goniometer was aligned with the midpoint of the patella. One lever arm was fixed with tape to the anterior tibia, and the other lever arm was placed perpendicular to the ground. Moreover, during the measurement of the angle of motion in knee extension movement, the lever arms of the electronic goniometer were fixed with tape to the lateral thigh and leg, and the axis was located at the knee joint. Prior practice ensured that the electromyographic signals and joint angles were synchronized for recording before the exercise movement tests.
For measuring the performance of hip abduction movement, each patient was instructed to stand on the nontested limb, and the tested leg was fixed with a yellow elastic band (Thera-Band, Hygenic Corp., Akron, OH). The patient was then asked to perform hip abduction to an extent of 30° for 2 seconds and then return to the initial position. For measuring the performance of hip external rotation movement, the patient was instructed to sit straight, and the tested leg was fixed with a yellow elastic band. The patient was then instructed to perform hip external rotation to 30° for 2 seconds and then return to the initial position. For measuring the performance of open kinetic chain knee extension movement, the patient position was the same as that of the hip external rotation movement, and the tested leg was fixed with a yellow elastic band. The patient was then asked to perform knee extension to 60° for 2 seconds and then return to the initial position. For measuring the performance of closed kinetic chain knee extension movement, the patient was instructed to perform a semisquat and flex the knee to 60° for 2 seconds and then return to the knee extension position. The exercise movements were practiced at least 5 times for familiarization. Moreover, the exercise movements were tested 3 times to collect the electromyographic signals of the VL, VMO, and gluteus medius muscles. A 1-minute rest interval between the tests and a 20-minute rest interval between the exercise movements were provided to prevent muscle fatigue.
2.5. Data analysis
The original electromyographic signals of the VL, VMO, and gluteus medius muscles were collected and analyzed. The sampling rate was set to 1000 Hz, and a band-pass filter of 40 to 400 Hz was used to remove extrinsic noise. Subsequently, the signals were processed through full-wave rectification, and the root mean squares were calculated for amplitude normalization at 100 milliseconds. For standardization, the MVC test results for the VL, VMO, and gluteus medius muscles were converted to percentages of the MVCs, which were recorded during the movements and represented the muscle activities. Finally, the simultaneous analysis of the MVC percentages and joint angle represented the muscle activities during the movements. The MVCs of the VL, VMO, and gluteus medius muscles were calculated for each 10° of the joint angle. The percentage of the MVCs at the terminal angle and ratio of VL and VMO were compared.
2.6. Statistical analysis
The SPSS 15 software package (SPSS Inc., Chicago, IL) was used to analyze all patient data. Kolmogorov–Smirnov test was applied to determine whether the data were normally distributed. Descriptive statistics for continuous variables are expressed as means and standard deviations. Independent t tests were conducted to compare the group differences in the percentage of the MVCs at the terminal angle and ratio of the VL and VMO muscles. The electromyographic activities of the VL, VMO, and gluteus medius muscles during the 4 movement tests were compared, and multivariate analysis of variance was used to determine the differences between the MVCs of the 3 muscles at each 10° interval of the joint angle. A post hoc test was also used to determine significant differences of pair-wise comparisons. A 2-tailed test was used, and the level of significance was set at α < 0.05.
3. Results
Thirty female patients with PFPS (age = 24.93 ± 4.91 years; weight = 58.62 ± 11.69 kg; height = 159.73 ± 28.91 cm; and leg length = 46.93 ± 8.29 cm) participated in the study. Their right legs were the dominant legs. For the hip abduction movement during the abduction and adduction phases, the MVC of the gluteus medius muscle was significantly higher than those of the VL and VMO muscles (P = .02–.001, Fig. 3A). In addition, the MVC of the gluteus medius muscle was significantly high in the external rotation and internal rotation phases during the hip external rotation movement (P = .04–.001, Fig. 3B). The MVCs of the VL muscle were higher than those of the VMO muscle at the abduction phase of the hip abduction movement (P = .02–.04) and external rotation phase of the hip external rotation movement (P = .03–.04). Regarding the open and closed kinetic chain knee extension movements during the extension and flexion phases, the MVCs of the gluteus medius muscle were significantly lower than those of the VL and VMO muscles (P = .01–.001, Fig. 3C and D). No significant differences in MVC were observed between the VL and VMO muscles during the open and closed kinetic chain knee extension movements (P > .05).
Figure 3.
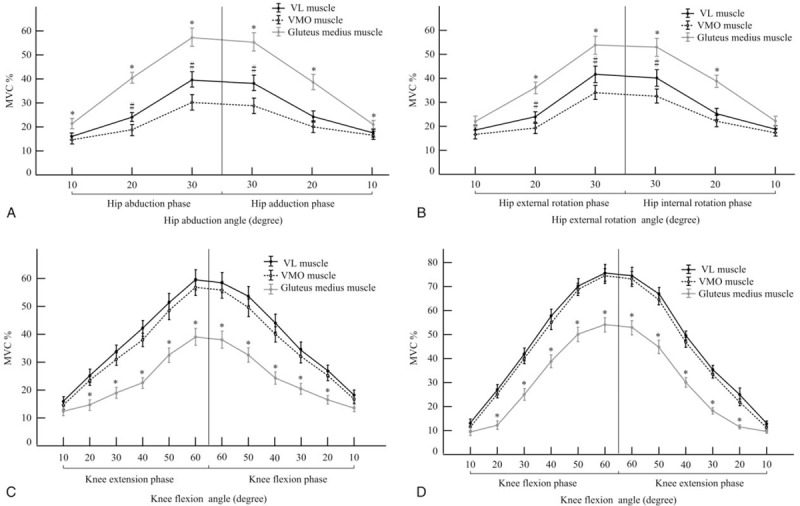
(A) The muscle activities during hip abduction movement (mean ± standard error; ∗Gluteus medius vs VL and VMO muscles, P < .05; #VL vs VMO muscle, P < .05). (B) The muscle activities during hip external rotation movement (mean ± standard error; ∗Gluteus medius vs VL and VMO muscles, P < .05; #VL vs VMO muscle, P < .05). (C) The muscle activities during open kinetic chain knee extension movement (mean ± standard error; ∗Gluteus medius vs VL and VMO muscles, P < .05). (D) The muscle activities during closed kinetic chain knee extension movement (mean ± standard error; ∗Gluteus medius vs VL and VMO muscles, P < .05). VL = vastus lateralis, VMO = vastus medialis oblique.
In the concentric phase, which is the first phase of the hip abduction, hip external rotation, and open kinetic chain knee extension movements, the muscle could sufficiently extend the elastic band and shorten it as it contracts (Fig. 4A). The second phase of the movements was the eccentric phase. The closed kinetic chain knee extension movement entailed adopting a squatting position, and the muscle contracted from the eccentric to concentric phases. The ratio of the VL and VMO muscles decreased in the concentric phase of the hip abduction and external rotation movements and then increased to restore the eccentric phase. In the concentric and eccentric phases of the open kinetic chain knee extension movement, the ratio of the VL and VMO muscles decreased to 0.91 at 40° of the knee joint and recovered to 0.96 at 10° of the knee joint (Fig. 4B). During the closed kinetic chain knee extension movement, the ratio of the VL and VMO muscles increased in the concentric phase and then decreased in the eccentric phase.
Figure 4.

(A) The ratio of the VL and VMO muscles among hip joint angle (mean ± 95% CI). (B) The ratio of the VL and VMO muscles among knee joint angle (mean ± 95% CI). CI = confidence interval, VL = vastus lateralis, VMO = vastus medialis oblique.
As shown in Table 1, compared with the MVCs at the terminal joint angle, the MVC of the gluteus medius muscle was significantly higher than those of the VL and VMO muscles in the hip abduction and external rotation movements, whereas it was significantly lower than those of the VL and VMO muscles in the open and closed kinetic chain knee extension movements (P < .05). The MVCs of the VL and VMO muscles in the open and closed kinetic chain knee extension movements were significant higher than those in the hip abduction and external rotation movements (P < .05). The MVCs of VL in the hip abduction and external rotation movements were significantly higher than that of the VMO muscle (P < .05); however, no significant differences were observed in the open and closed kinetic chain knee extension movements (P > .05). The ratios of the VL and VMO muscles in the open and closed kinetic chain knee extension movements approached 1, and they were significantly higher than those in the hip abduction and external rotation movements (P < .05). The highest MVC of the VMO muscle was observed at the terminal joint angle of the closed kinetic chain knee extension movement.
Table 1.
The maximum voluntary contraction at the terminal angle in 4 exercise movements.

4. Discussion
Hip abduction and external rotation movements induced the activation of the gluteus medius muscle as well as the VMO and VL muscles. Moreover, open and closed kinetic chain knee extension movements engendered the activation of the VMO and VL muscles, in addition to the gluteus medius muscle. Muscle cocontraction helps to stabilize the motion practice to enable agonist muscle to resist resistance, resulting in the movement. Notably, VL muscle activation was induced during hip abduction and external rotation movements. At the terminal joint angle of the 2 movements, the MVC percentages of the VL muscle were 40.13% and 42.08%, which were higher than those of the VMO muscle activation. Felício et al[20] indicated that hip abduction movement stimulated the gluteus medius muscle activation and also caused increased VL muscle activation. Escamilla et al[21] considered that movements with high VL activation should not be advocated in exercise training programs for PFPS, because such movements can cause patellar lateralization.
In a previous study, knee extensor strengthening training focused on the correct alignment of the patella, depending on the dynamic balance of the VMO and VL muscle strength.[22] Physiotherapists have expressed particular concern for the weakness of the VMO muscle, which may lead to abnormal patellar tracking. Morrish and Woledge[23] indicated that knee extensor strengthening training should focus on the VMO muscle activity in patients with PFPS. Open and closed kinetic knee exercises are recommended for strengthening the VMO muscle. Open kinetic knee exercise is a single joint movement in a nonweight-bearing position, and closed kinetic exercise is a functional multijoint movement in a weight bearing position.[24]
In a comparison between 2 knee extension movements, O'Sullivan et al[25] found that closed kinetic chain knee extension movement demonstrated maximum VMO muscle activation. Irish et al[26] also applied electromyography analysis to compare the activity of the VMO and VL muscles during open and closed kinetic chain movements. They suggested that the double-leg squat, which is a closed kinetic chain movement, could be a selective movement for strengthening the VMO muscle and facilitating the correction of patellar tracking. In the present study, the closed kinetic chain knee movement resulted in a 76.22% MVC of the VMO muscle in patients with PFPS and thus demonstrated higher VMO muscle activity than the open kinetic chain extension movement did. This result evidences that the closed kinetic chain knee movement can be used for VMO muscle strength training in patients with PFPS.
In recent years, hip muscle strength training has been recommended for patients with PFPS, and the training focuses on strengthening the hip abductor and external rotator muscles. The strengthening training effect could increase the muscle tension and reduce excessive hip internal rotation. Therefore, a study results revealed that this training was helpful in reducing the excessive intra-articular stress on the patellofemoral joint.[27] Some studies have reported that hip abductor and external rotator muscle strengthening reduced PFPS pain and improved functional ability and hip muscle strength.[7,28] However, the present study determined that the VL muscle activity increased, and that the MVC of the VL muscle was significantly higher than that of the VMO muscle during hip abduction and external rotation movements. Irrespective of whether it occurred during the movement or at the terminal joint angle, this phenomenon may be attributed to the synergistic contraction of the VL muscle.
Comparing hip muscle and knee extensor strength training revealed that both exercise programs could reduce pain and improve function in patients with PFPS. Moreover, hip muscle strength training demonstrated more favorable effects than knee extensor strength training did in the early stage of PFPS,[29] and the improvements were maintained at the 6-month follow-up.[30] In a systematic review, Santos et al[31] found that hip abductor and external rotator muscle strengthening was effective in reducing pain and improving function. However, the meta-analysis results revealed no evidence of the effectiveness of muscle strengthening in increasing hip muscle strength. Santos et al[31] indicated that the specificity of the training caused the difference in study results. The present study supports that the activity of the gluteus medius muscles increased during the hip abduction and external rotation movements. The motor units of the muscle can be recruited and used for hip muscle strengthening.
Souza and Gross[32] recommended that VMO and VL muscle balance could maintain correct patellar tracking in the femoral groove. The exercise movements, which had an ideal ratio of the VL and VMO muscles (VMO/VL = 1), are suitable for patients with PFPS. In the present study, the ratios of the VL and VMO muscles decreased to 0.78 and 0.81, respectively, during the hip abduction and external rotation movements, because of the higher VL muscle activation. VMO and VL muscle imbalance was observed during the movements and at the terminal joint angle. The VL and VMO muscle ratios approached 1 in the open and closed kinetic chain knee movements compared with hip abduction and external rotation movements. During the open kinetic chain knee movement, higher ratios of the VL and VMO muscles were observed at 20° and 60° in the concentric phase and at 10° in the eccentric phase. Doucette and Child[33] indicated that open kinetic chain exercises from 30° to full flexion are safe knee joint ranges for exercises in patients with PFPS. The present study's results supported the contention. However, the mechanism of open kinetic chain movement remains unclear. A presumption in this study was that VMO and VL muscle activations were regulated to tie in the patellar tracking. At the terminal joint angle in the closed kinetic chain knee movement, the ratio of the VL and VMO muscles was 0.99 and the MVC of the VMO muscle was 76.22%, which was the highest among the 4 movements. Souza and Gross[32] analyzed the MVCs of the VMO and VL muscles during a lunge exercise and determined that the ratio of the VL and VMO muscles in a closed kinetic chain knee movement was nearly 1. These results are similar to the findings of the present study. In the present study, the highest ratio of the VL and VMO muscles was produced at 60° of the knee joint. Tang et al[34] compared the ratio of the VL and VMO muscles, as well as the MVC of the VMO muscle, between open and closed kinetic chain knee movements in patients with PFPS. The findings indicated that maximum VMO activation and the highest ratio of the VL and VMO muscles were observed at a 60° knee flexion in the closed kinetic chain knee movement. Moreover, Tang et al[34] indicated that this joint range may exert the lowest stress forces on the patellofemoral joint. In the present study, the MVC of the gluteus medius muscle during the closed kinetic chain knee movement was higher than that during the open kinetic chain knee movement. The MVC of the gluteus medius muscle increased to 55.06% at the terminal joint angle of the closed kinetic chain knee movement. The possible reason is that squatting is a multijoint movement and that the gluteus medius muscle is a synergist that helps in hip stabilization.
There are certain limitations in this study. First, lack of healthy participants as control group were difficult to compare the effects outcomes or effect sizes of the exercise movements in PFPS patients. Second, because the participants were general college students in current study, insufficient records of their exercise habits and specific sports were analyzed. So, it was difficult to explore the differences on electromyographic analysis in female athlete or amateur. Hip muscle movement (i.e., hip abductor and hip external rotator exercises) was caused more VL muscle activation, and more lateral vector of patella. Knee movements (i.e., open and closed kinetic chain exercises) were caused a balance of VMO and VL muscle activation on patella. They were suitable exercises for PFPS patients in clinic training. The therapeutic exercise program for PFPS was suggested to be determined on the basis of patients’ biomechanics problem. A detailed orthopedic assessment is recommended for patients with PFPS. If the selected hip muscle strengthening training is conducted to improve hip stabilization and then correct patellar malalignment, the increase in VL muscle activation should be closely monitored to detect abnormal patellar tracking. If the selected knee extensor strengthening training is conducted to increase VMO activation and obtain ideal ratios of VL and VMO muscles, closed kinetic chain knee movements can be used for patients with PFPS.
5. Conclusion
This study demonstrated that selective gluteus medius muscle activation was induced during hip abduction and external rotation movements, accompanied by an increase in VL muscle activation. The hip muscle movements had more VL muscle activation, resulting in more lateral vector of patella. In open and closed kinetic chain knee movements, the ratios of the VL and VMO muscles approached 1. More selective VMO muscle activation was induced during the closed kinetic chain knee movement. The knee movements were suggested for PFPS patients as clinic training exercises.
Author contributions
Conceptualization: Shuya Chen, Yi-Chin Fong.
Data curation: Shuya Chen, Wen-Dien Chang, Jhih-Yun Wu, Yi-Chin Fong.
Formal analysis: Wen-Dien Chang.
Investigation: Jhih-Yun Wu, Yi-Chin Fong.
Methodology: Shuya Chen.
Supervision: Wen-Dien Chang.
Writing – original draft: Shuya Chen, Wen-Dien Chang.
Writing – review and editing: Wen-Dien Chang.
Footnotes
Abbreviations: MVC = maximum voluntary contraction, PFPS = patellofemoral pain syndrome, VL = vastus lateralis, VMO = vastus medialis oblique.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Boling M, Padua D, Marshall S, et al. Gender differences in the incidence and prevalence of patellofemoral pain syndrome. Scand J Med Sci Sports 2010;20:725–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Chang WD, Chen FC, Lee CL, et al. Effects of Kinesio taping versus McConnell taping for patellofemoral pain syndrome: a systematic review and meta-analysis. Evid Based Complement Alternat Med 2015;2015:471208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Mohr KJ, Kvitne RS, Pink MM, et al. Electromyography of the quadriceps in patellofemoral pain with patellar subluxation. Clin Orthop Relat Res 2003;415:261–71. [DOI] [PubMed] [Google Scholar]
- [4].Chang WD, Huang WS, Lai PT. Muscle activation of vastus medialis oblique and vastus lateralis in sling-based exercises in patients with patellofemoral pain syndrome: a cross-over study. Evid Based Complement Alternat Med 2015;2015:740315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Chang WD, Huang WS, Lee CL, et al. Effects of open and closed kinetic chains of sling exercise therapy on the muscle activity of the vastus medialis oblique and vastus lateralis. J Phys Ther Sci 2014;26:1363–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Hodges PW, Richardson CA. The influence of isometric hip adduction on quadriceps femoris activity. Scand J Rehabil Med 1993;25:57–62. [PubMed] [Google Scholar]
- [7].Khayambashi K, Mohammadkhani Z, Ghaznavi K, et al. The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain: a randomized controlled trial. J Orthop Sports Phys Ther 2012;42:22–9. [DOI] [PubMed] [Google Scholar]
- [8].Robinson RL, Nee RJ. Analysis of hip strength in females seeking physical therapy treatment for unilateral patellofemoral pain syndrome. J Orthop Sports Phys Ther 2007;37:232–8. [DOI] [PubMed] [Google Scholar]
- [9].Prins MR, van der Wurff P. Females with patellofemoral pain syndrome have weak hip muscles: a systematic review. Aust J Physiother 2009;55:9–15. [DOI] [PubMed] [Google Scholar]
- [10].Bolgla LA, Boling MC. An update for the conservative management of patellofemoral pain syndrome: a systematic review of the literature from 2000 to 2010. Int J Sports Phys Ther 2011;6:112–25. [PMC free article] [PubMed] [Google Scholar]
- [11].Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population: a two-year prospective study. Am J Sports Med 2000;28:480–9. [DOI] [PubMed] [Google Scholar]
- [12].Fukuda TY, Rossetto FM, Magalhães E, et al. Short-term effects of hip abductors and lateral rotators strengthening in females with patellofemoral pain syndrome: a randomized controlled clinical trial. J Orthop Sports Phys Ther 2010;40:736–42. [DOI] [PubMed] [Google Scholar]
- [13].Almeida GP, Silva AP, França FJ, et al. Q-angle in patellofemoral pain: relationship with dynamic knee valgus, hip abductor torque, pain and function. Rev Bras Ortop 2016;51:181–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Sohn MK, Graven-Nielsen T, Arendt-Nielsen L, et al. Inhibition of motor unit firing during experimental muscle pain in humans. Muscle Nerve 2000;23:1219–26. [DOI] [PubMed] [Google Scholar]
- [15].Rainoldi A, Melchiorri G, Caruso I. A method for positioning electrodes during surface EMG recordings in lower limb muscles. J Neurosci Methods 2004;134:37–43. [DOI] [PubMed] [Google Scholar]
- [16].Clarke MN, Ni Mhuircheartaigh DA, Walsh GM, et al. Intra-tester and inter-tester reliability of the MicroFET 3 hand-held dynamometer. Physiother Pract Res 2011;32:13–8. [Google Scholar]
- [17].Bolgla LA, Malone TR, Umberger BR, et al. Reliability of electromyographic methods used for assessing hip and knee neuromuscular activity in females diagnosed with patellofemoral pain syndrome. J Electromyogr Kinesiol 2010;20:142–7. [DOI] [PubMed] [Google Scholar]
- [18].Graham VL, Gehlsen GM, Edwards JA. Electromyographic evaluation of closed and open kinetic chain knee rehabilitation exercises. J Athl Train 1993;28:23–30. [PMC free article] [PubMed] [Google Scholar]
- [19].Bevilaqua-Grossi D, Monteiro-Pedro V, de Vasconcelos RA, et al. The effect of hip abduction on the EMG activity of vastus medialis obliquus, vastus lateralis longus and vastus lateralis obliquus in healthy subjects. J Neuroeng Rehabil 2006;3:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Felício LR, Dias LA, Silva AP, et al. Muscular activity of patella and hip stabilizers of healthy subjects during squat exercises. Rev Bras Fisioter 2011;15:206–11. [PubMed] [Google Scholar]
- [21].Escamilla RF, Zheng N, Macleod TD, et al. Patellofemoral joint force and stress during the wall squat and one-leg squat. Med Sci Sports Exerc 2009;41:879–88. [DOI] [PubMed] [Google Scholar]
- [22].Cowan SM, Bennell KL, Hodges PW, et al. Delayed onset of electromyographic activity of vastus lateralis compared to vastus medialis obliquus in subjects with patellofemoral pain syndrome. Arch Phys Med Rehabil 2001;82:183–9. [DOI] [PubMed] [Google Scholar]
- [23].Morrish GM, Woledge RC. A comparison of the activation of muscles moving the patella in normal subjects and in patients with chronic patellofemoral problems. Scand J Rehabil Med 1997;29:43–8. [PubMed] [Google Scholar]
- [24].Grood ES, Suntay WJ, Noyes FR, et al. Biomechanics of the knee-extension exercise. Effect of cutting the anterior cruciate ligament. J Bone Joint Surg Am 1984;66:725–34. [PubMed] [Google Scholar]
- [25].O'Sullivan SP, Popelas CA. Activation of vastus medialis obliquus among individuals with patellofemoral pain syndrome. J Strength Cond Res 2005;19:302–4. [DOI] [PubMed] [Google Scholar]
- [26].Irish SE, Millward AJ, Wride J, et al. The effect of closed-kinetic chain exercises and open-kinetic chain exercise on the muscle activity of vastus medialis oblique and vastus lateralis. J Strength Cond Res 2010;24:1256–62. [DOI] [PubMed] [Google Scholar]
- [27].Cichanowski HR, Schmitt JS, Johnson RJ, et al. Hip strength in collegiate female athletes with patellofemoral pain. Med Sci Sports Exerc 2007;39:1227–32. [DOI] [PubMed] [Google Scholar]
- [28].Dolak KL, Silkman C, McKeon JM, et al. Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: a randomized clinical trial. J Orthop Sports Phys Ther 2011;41:560–70. [DOI] [PubMed] [Google Scholar]
- [29].Ferber R, Bolgla L, Earl-Boehm JE, et al. Strengthening of the hip and core versus knee muscles for the treatment of patellofemoral pain: a multicenter randomized controlled trial. J Athl Train 2015;50:366–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Khayambashi K, Fallah A, Movahedi A, et al. Posterolateral hip muscle strengthening versus quadriceps strengthening for patellofemoral pain: a comparative control trial. Arch Phys Med Rehabil 2014;95:900–7. [DOI] [PubMed] [Google Scholar]
- [31].Santos TR, Oliveira BA, Ocarino JM, et al. Effectiveness of hip muscle strengthening in patellofemoral pain syndrome patients: a systematic review. Braz J Phys Ther 2015;19:167–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Souza DR, Gross MT. Comparison of vastus medialis obliquus: vastus lateralis muscle integrated electromyographic ratios between healthy subjects and patients with patellofemoral pain. Phys Ther 1991;71:310–6. [DOI] [PubMed] [Google Scholar]
- [33].Doucette SA, Child DP. The effect of open and closed chain exercise and knee joint position on patellar tracking in lateral compression syndrome. J Orthop Sports Phys Ther 1996;23:104–10. [DOI] [PubMed] [Google Scholar]
- [34].Tang SF, Chen CK, Hsu R, et al. Vastus medialis obliquus and vastus lateralis activity in open and closed kinetic chain exercises in patients with patellofemoral pain syndrome: an electromyographic study. Arch Phys Med Rehabil 2001;82:1441–5. [DOI] [PubMed] [Google Scholar]