

Abstract
Critical illness insurance to reduce the incidence of catastrophic health expenditure was implemented in China in 2012. The aim of this study is to explore the implementation status and medical guarantee effect of critical illness insurance in various cities.
We extracted insurance reimbursement data for 2014 from the critical illness insurance information systems of 4 cities. Characteristics of the critical illness insurance system were used to describe the implementation status. The share of medical expenses reimbursed by insurance and the percentage of individuals suffering catastrophic health expenditures were calculated to evaluate the effect of critical illness insurance.
The share of medical expenses reimbursed by insurance was 58.93%, 47.29%, 62.05%, and 61.75% in Beijing, Siping, Yichang, and Zhaoqing, respectively; those shares increased by 5.29 percentage points, 7.72 percentage points, 13.30 percentage points, and 22.63 percentage points, respectively, after the introduction of critical illness insurance. The percentage of individuals suffering catastrophic health expenditures was unchanged in Beijing, but decreased by 7.04 percentage points in Siping, 11.22 percentage points in Yichang, and 2.19 percentage points in Zhaoqing.
China's critical illness insurance increases the level of medical guarantee to some extent, but its effect on reducing the incidence of catastrophic health expenditure is somewhat limited.
Keywords: China, critical illness insurance, health insurance
1. Introduction
Impressive achievements in health care reform, especially health insurance, have been made in China in the past decade. Health insurance coverage expanded from 49.6% in urban areas and 12.6% in rural areas in 2003 to >95% in both urban and rural areas in 2013.[1,2] China has achieved nearly universal basic health insurance coverage. The major purpose of basic health insurance is to improve access to health care, increase equity in utilization of health care services, and reduce the incidence of catastrophic health expenditure (CHE)[3,4] However, plenty of evidence indicates that out-of-pocket health expenditures in China still are very high despite the expansion of health insurance coverage to >95% of the population.[5,6] The average share of inpatient costs reimbursed by insurance was 44.87% in 2011,[7] meaning that more than half of such medical costs were out-of-pocket payments. In addition, data from National Health Service surveys show that little change in the percent of households experiencing CHEs occurred in the past decade. That percentage in urban areas was 9.0% in 2003, 11.3% in 2008, and 10.9% in 2011 and in rural areas was 13.6% in 2003, 15.1% in 2008, and 13.8% in 2011.[5]
On August 30, 2012, to relieve people's economic burden of disease, China's National Development and Reform Commission, Ministry of Health and 4 other ministries and commissions issued “Guidance about implementation of residents’ critical illness insurance system.” The guidance points out that critical illness insurance (CII), similar to basic health insurance, is an institutional arrangement aimed at providing reimbursement of high medical expenses associated with critical illness. The initial intent of CII is to solve the problems of illness-caused poverty and reduce CHE. Nonetheless, China's central government proposes only general principles and a framework for implementing CII and requires the local governments to explore appropriate modes consistent with their social economic development and medical spending. For example, the central government suggests that patients who have critical illnesses are those whose annual medical costs exceed per capita annual disposable income. However, the local governments set their own deductibles for CII. In some cities, the deductible is less than the local per capita annual disposable income, but in other cities, the deductible exceeds or equals the local per capita annual disposable income. As of February 2014, 25 provinces had established CII systems.[8] The implementation status of CII in various regions and its effect on reducing the incidence of CHE must be evaluated.
However, the existing literature regarding CII systems in various regions of China has focused mainly on describing, comparing, and analyzing their design and development.[9,10] Few studies have quantitatively assessed their performance relative to the goal of offering financial protection against CHE. In this study, we analyze the implementation status of CII in 4 cities of China and evaluate their performance based on reimbursement rate and CHE incidence reduction.
2. Method
2.1. Data source
As of February 2014, 25 provinces of China had established CII systems. For this study, we focused on 4 cities (Beijing, Siping in Jilin Province, Yichang in Hubei Province, and Zhaoqing in Guangdong Province), which provided us with access to their CII information systems. This study was approved by the Research Ethics Committee of Huazhong University of Science and Technology, Wuhan, China. The study participants are patients who were reimbursed by CII in 2014 in the 4 selected cities. The patient information gathered from the information systems included sex, age, total medical expenses, medical expenses within the payment scope of basic medical insurance, insurance benefits provided by basic medical insurance, and insurance benefits provided by CII. In addition, information about the cities’ CII systems, including insurance premiums, deductibles, caps, and standard reimbursement amounts based on medical expenses within the payment scope of basic medical insurance, was gathered.
2.2. Definitions of indicators
For the purpose of this study, total medical expenses are defined as the total direct costs of seeking health care services in a single policy year. These include costs of drugs, examinations, consultations, treatments, inpatient hospital beds stays, and other direct health care services. Indirect costs, such as the costs of transportation and special diets and wages lost due to illness, are not considered in this study.
The share of medical expenses reimbursed by insurance represents the medical guarantee. Because Chinese health insurance policy categorizes total medical expenses into 2 components—expenses within and beyond the payment scope of basic medical insurance—2 indicators are calculated. S1 represents the medical guarantee stipulated in the current policy, and S2 represents the actual medical guarantee provided.
S1 = aggregate insurance benefit received in a single policy year/medical expenses within the payment scope of basic medical insurance × 100%
S2 = aggregate insurance benefit received in a single policy year/total medical expenses × 100%
CHE is defined as health expenditure that threatens a household's capacity to maintain a basic standard of living. In China, many researchers have suggested that CHE occurs when an individual's aggregate annual out-of-pocket health care expenditure exceeds the per capita annual disposable income of people in the city in which the individual lives.[11–13] The percentage of individuals suffering CHEs is calculated based on this threshold.
2.3. Statistical analysis
Statistical analysis was performed by use of SAS 9.4 for Windows. In the descriptive analysis, 3 indicators were used to evaluate the effect of CII: increase in the medical guarantee stipulated in the current policy; increase in the actual medical guarantee provided; and decline in the percentage of individuals suffering CHEs. Given the remarkable variation in the cities’ socioeconomic status and the cities’ development status of their CII systems, we analyze the 4 cities separately.
3. Results
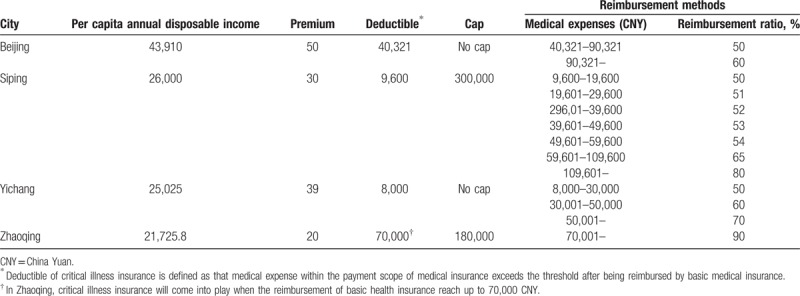
Table 1 summarizes the characteristics of the 4 recruited cities’ CII systems. There is much diversity in insurance premium, deductible, cap, and standard reimbursement amount by city. The payment amount is segmented calculated for all cities except Zhaoqing. In general, higher medical expenses mean a higher compensation ratio.
Table 1.
Characteristics of critical illness insurance in the 4 sampled cities in China.
In 2014, in Beijing, Siping, Yichang, and Zhaoqing, respectively, 1875, 597, 1978, and 729 residents were reimbursed by CII. The share of medical expenses reimbursed by insurance was 58.93% in Beijing, 47.29% in Siping, 62.05% in Yichang, and 61.75% in Zhaoqing. The percentage of individuals suffering CHEs in those cities was 100%, 60.13%, 12.54%, and 97.12%, respectively. After the implementation of CII, the share of medical expenses reimbursed by insurance increased by 5.29 percentage points in Beijing, 7.72 percentage points in Siping, 13.30 percentage points in Yichang, and 22.63 percentage points in Zhaoqing (Table 2). The percent of individuals suffering CHEs was unchanged in Beijing but decreased by 7.04 percentage points in Siping, 11.22 percentage points in Yichang, and 2.19 percentage points in Zhaoqing (Table 3).
Table 2.
Reimbursement of basic health insurance and critical illness insurance.

Table 3.
Catastrophic health expenditure.

4. Discussion
In this study, we have evaluated the effect of the CII systems of 4 cities in China based on the share of medical expenses reimbursed and the incidence of CHE before and after the implementation of the CII system. The results suggest that there is much diversity in the medical guarantee provided by the CII systems of the various cities. In general, however, the medical guarantee provided by CII is somewhat limited.
Although the medical guarantee increased after the implementation of the CII system, out-of-pocket payments, which account for almost 40% of total medical expenses, still are very high. In addition, for the purposes of this study, medical expenses are defined as direct costs of seeking health care services, and therefore exclude indirect costs such as the costs of transportation and special diets and wages lost due to illness. Because health care resources allocation is seriously uneven in China,[14,15] previous evidence indicates that the indirect costs of seeking health care services are considerable.[16] A large number of seriously ill patients cannot obtain effective treatment in local hospitals and instead must seek high-quality health care services in cities far from their homes.[17] Doing so may further aggravate their economic burden and cause them incur CHE. Unfortunately, indirect medical costs are not covered by China's health insurance systems. The health insurance system must be improved to reduce the potential risks of CHE.
The main purpose of CII is to provide protection against CHE. In this study, we have shown that the current CII system has limited effect on reducing the incidence of CHE but that its effect varies by city. We had expected high deductibles to serve as the main barrier to effectiveness of CII systems. Excessively high deductibles make CHE inevitable among some patients with high medical expenses, even if the patients obtain some reimbursement from CII; this is the situation in Beijing. Excessively high deductibles also limit the number of beneficiaries who receive reimbursement. In addition, some researchers believe that setting uniform deductibles for various income groups is unfair. In fact, CHE is caused not only by high-cost medical procedures or interventions. A relatively small payment can mean financial catastrophe to a poor individual or a poor household, forcing them to reduce other basic living expenses, such as food, shelter, or education.[18–20] Therefore, a scientific approach to determining fair deductibles for various income groups should be considered by the CII systems’ management.
Since the early 1980s, the Chinese health care system has encountered great challenges, which resulted both from economic reform and the decentralization and privatization of the health system. The main challenge, though, was an increasing inequality in health care. Expanding health insurance coverage was one of the 5 key components of the latest round of health care reforms initiated in 2009 to supply affordable and equitable health care for all in China. Although China has made impressive progress in expansion of insurance coverage and established CII systems, the present study showed that the reimbursement rate of health insurance is still low, which may impede the delivery of accessible health care that is both equitable and affordable for all Chinese citizens. Therefore, there is an urgent need for Chinese government to improve health care insurance system, including keeping trying to extend health care insurance fund investment channel and increasing the reimbursement ratio. In addition, health care insurance is just one of the factors that influence accessibility and inequality in health care. More efforts are needed to strengthen primary health care and build an integrated primary care-based delivery system. Meanwhile, any decision to promote the decentralization and privatization of the health system should not be made without objective assessment of its effect on China's health care system.
The limitation of our study must be noted. Because data about participants’ household income were not available, the proportion of individuals suffering CHEs could not be calculated according to the method recommended by the World Health Organization.[21] Although the threshold of per capita annual disposable income is commonly used in defining CHE in China, some studies have suggested that this threshold is higher than the one recommended by the World Health Organization and therefore may underestimate the incidence of CHE.[22,23]
5. Conclusion
The implementation of CII systems in China has increased the medical guarantee provided, to some extent, but patients’ economic burdens still are very high. The effect of CII on reducing the incidence of CHE is limited and varies dramatically by city, mainly due to variation in deductible. CII systems’ management should actively explore scientific methods to determining fair deductibles based on patients’ income.
Author contributions
Conceptualization: Pengqian Fang, Xiaoxv Yin.
Data curation: Xiaoyan Zhang, Xue Bai.
Formal analysis: Xiaoyan Zhang, Xue Bai, Yanhong Gong.
Funding acquisition: Pengqian Fang.
Investigation: Zhengqiong Pan, Xiaoyan Zhang, Xue Bai.
Methodology: Yanhong Gong.
Project administration: Xiaoxv Yin.
Resources: Xiaoxv Yin.
Software: Zhengqiong Pan, Xue Bai, Yanhong Gong.
Supervision: Xiaoxv Yin.
Validation: Xiaoxv Yin.
Visualization: Xiaoxv Yin.
Writing – original draft: Pengqian Fang.
Writing – review and editing: Pengqian Fang, Xiaoxv Yin.
Footnotes
Abbreviations: CHE = catastrophic health expenditure, CII = critical illness insurance.
Availability of data and materials statement: The datasets supporting the conclusions of this article are available upon requests from the corresponding author (email: yxx@hust.edu.cn).
This project was funded by the National Natural Science Foundation of China (key program) (No. 71333005); Major Program of National Fund of Philosophy and Social Science (No. 15ZDC037).
The authors have no conflicts of interest to disclose.
References
- [1].Center for Health Statistics and Information of Ministry of Health of People's Republic of China. Reports of the Third Nation Health Service Survey. 2004. Available at: http://www.nhfpc.gov.cn/cmsresources/mohwsbwstjxxzx/cmsrsdocument/doc9908.pdf. Accessed November 10, 2016. [Google Scholar]
- [2].Center for Health Statistics and Information of Ministry of Health of People's Republic of China. Reports of the Fifth Nation Health Service Survey, vol. 2016. Beijing: Pecking Union Medical College Press; 2013. [Google Scholar]
- [3].World Health Organization. Strategy on health care financing for countries of the Western Pacific and South-East Asia Regions (2006–2010). 2005. Available at: http://www2.wpro.who.int/NR/rdonlyres/97291867-000D-4AFD-B3E1-ABD954D57722/0/RC56_R06.pdf. Accessed November 15, 2016. [Google Scholar]
- [4].World Health Organization. Advancing and sustaining universal coverage. The World Health Report 2008—Primary Health Care (Now More Than Ever). 2008. Available at: http://www.who.int/whr/2008/08_chap2_en.pdf?ua=1. Accessed November 10, 2016. [Google Scholar]
- [5].Meng Q, Xu L, Zhang YG, et al. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. Lancet 2012;379:805–14. [DOI] [PubMed] [Google Scholar]
- [6].Li YQ. Study on real security level of China's Urban Residents’ Health Insurance System: an empirical analysis based on typical cities of Guangdong Province. Popul Dev 2013;19:55–62. [Google Scholar]
- [7].The National Audit Office of the People's Republic of China. Report of the audit result of the national social security fund. 2012. Available at: http://www.gov.cn/zwgk/2012-08/02/content_2196871.htm. Accessed November 15, 2016. [Google Scholar]
- [8].Wang W. Discussion on financing mechanism and reimbursing policy of critical illness insurance: based on the comparison of pilot schemes from 25 provinces of China. J Huazhong Normal Univ (Hum Soc Sci) 2014;53:16–22. [Google Scholar]
- [9].Liu PC, Jiang LW, Li CY, et al. How to deal with burden of critical illness: a comparison of strategies in different areas of China. Pak J Med Sci 2014;30:659–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Ma R, Huang L, Zhao D, et al. China critical illness insurance policy—the recent developments and prospects. Value Health 2014;17:A795. [DOI] [PubMed] [Google Scholar]
- [11].Song ZJ. The Evaluation on the operation of the supplementary major medical insurance for urban and rural residents. Insurance Stud 2014;98–107. [Google Scholar]
- [12].Sun ZG. Implementing critical illness insurance is the key to relieve people's economic burden of disease. Admin Reform 2012;54–7. [Google Scholar]
- [13].Xu SC. Critical illness insurance: a key point for the health care system. Macroecon Manag 2013;31–2. [Google Scholar]
- [14].He MH, Wang L, He J, et al. Studying on the status and equity of health services resources allocation in China. Chin Health Serv Manag 2013;197–9. [Google Scholar]
- [15].Zhang N, Sun XJ, Li C, et al. Analyzing the equity of health resources allocation in China based on Theil Index. Chin Health Serv Manag 2014;88–91. [Google Scholar]
- [16].Ma Y, Yu XL, Zhang J. The empirical research on the effectiveness of critical illness insurance for urban residents. China Health Insurance 2015;8:29–32. [Google Scholar]
- [17].Guo MT, Wu QH, Li Y, et al. Analysis of the changing tendency of inpatient reimbursement, copayment rate and impoverishment from medical expenses of the patient with medical insurance. Chin Hosp Manag 2014;34:74–6. [Google Scholar]
- [18].Xu K, Evans DB, Carrin G, et al. Protecting households from catastrophic health spending. Health Aff 2007;26:972–83. [DOI] [PubMed] [Google Scholar]
- [19].Kawabata K, Xu K, Carrin G. Preventing impoverishment through protection against catastrophic health expenditure. Bull World Health Organ 2002;80:612. [PMC free article] [PubMed] [Google Scholar]
- [20].Su TT, Kouyate B, Flessa S. Catastrophic household expenditure for health care in a low-income society: a study from Nouna District, Burkina Faso. Bull World Health Organ 2006;84:21–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Xu K. Distribution of health payments and catastrophic expenditures Methodology. 2004. Available at: http://apps.who.int/iris/bitstream/10665/69030/1/EIP_HSF_DP_05.2.pdf. Accessed Novmber 15, 2016. [Google Scholar]
- [22].Zhu ML, Song ZJ. The effect of catastrophic medical insurance on the risk diversification of the household catastrophic health expenditure. Chin J Health Pol 2012;5:4–7. [Google Scholar]
- [23].Zhou L. Critical illness insurance and household catastrophic health expenditure. China Economist 2015;52–3. [Google Scholar]