

Abstract
Objectives
Researchers continue to seek easier ways to evaluate the quality of bone and screen for osteoporosis and osteopenia. Until recently, radiographic images of various parts of the body, except the distal femur, have been reappraised in the light of dual-energy X-ray absorptiometry (DXA) findings. The incidence of osteoporotic fractures around the knee joint in the elderly continues to increase. The aim of this study was to propose two new radiographic parameters of the distal femur for the assessment of bone quality.
Methods
Anteroposterior radiographs of the knee and bone mineral density (BMD) and T-scores from DXA scans of 361 healthy patients were prospectively analyzed. The mean cortical bone thickness (CBTavg) and the distal femoral cortex index (DFCI) were the two parameters that were proposed and measured. Intra- and interobserver reliabilities were assessed. Correlations between the BMD and T-score and these parameters were investigated and their value in the diagnosis of osteoporosis and osteopenia was evaluated.
Results
The DFCI, as a ratio, had higher reliability than the CBTavg. Both showed significant correlation with BMD and T-score. When compared with DFCI, CBTavg showed better correlation and was better for predicting osteoporosis and osteopenia.
Conclusion
The CBTavg and DFCI are simple and reliable screening tools for the prediction of osteoporosis and osteopenia. The CBTavg is more accurate but the DFCI is easier to use in clinical practice.
Cite this article: Q-F. He, H. Sun, L-Y. Shu, Y. Zhu, X-T. Xie, Y. Zhan, C-F. Luo. Radiographic predictors for bone mineral loss: Cortical thickness and index of the distal femur. Bone Joint Res 2018;7:468–475. DOI: 10.1302/2046-3758.77.BJR-2017-0332.R1.
Keywords: Osteoporosis, Knee joint, Radiography, Dual-energy X-ray absorptiometry, Prospective study
Article focus
Radiographic images of various parts of the body have been reappraised in light of dual-energy X-ray absorptiometry (DXA) findings.
No parameter from the distal femur has been proposed and verified to predict changes in bone quality.
We propose two radiographic parameters of the distal femur that may be used in the diagnosis of osteoporosis and osteopenia.
Key messages
The mean cortical bone thickness of the distal femur (CBTavg) and the distal femoral cortex index (DFCI) were the two parameters that were assessed in this study.
Excellent reliability agreements were achieved using both CBTavg and DFCI.
Both parameters are valuable predictors of change in bone quality.
Strengths and limitations
This is the first time that new radiographic parameters have been proposed to focus on the distal femur, where the fragility fracture has a high morbidity. They have been compared with the bone mineral density (BMD) measured by DXA.
The local BMD around the knee using DXA or a specific peripheral quantitative CT was not obtained as a control.
Introduction
Osteoporosis, which is characterized by low bone mass, microarchitectural deterioration of bone, and an increased risk of fracture, is a major threat to health. The incidence of fragility fractures resulting from osteoporosis is expected to increase during the next few decades.1-3 The costs of diagnosing and treating osteoporosis in both developed and developing countries are very high.4,5 Currently, the diagnosis of primary osteoporosis without fragility fracture is based on bone mineral density (BMD), which can be measured conveniently and non-invasively by dual-energy X-ray absorptiometry (DXA). Not all physicians, however, have access to this equipment. The cost of DXA and a lack of instruments may limit its widespread use in some communities, and complementary approaches are required in order to develop screening tools to identify patients who are at risk of osteoporosis.
Despite improvements in treatment, osteoporotic fractures remain difficult to treat.5,6 They may take a long time to heal7 and are associated with high complication rates and adverse outcomes.8,9 The surgical treatment of fractures around the knee in elderly patients and those with osteoporosis remains problematic. However, the diagnosis of osteoporosis can be overlooked, as DXA studies may not be routinely undertaken in patients who suffer trauma.10 Various radiographic parameters have focused on the frequently fractured metaphyseal regions, such as the proximal humerus,11-15 proximal femur,16,17 femoral shaft,18 proximal tibia,19,20 and the distal tibia,21 in an attempt to predict osteoporosis. The validity of all of these parameters has been verified, except for those at the distal femur. The purpose of this study, therefore, was to propose and validate two easily available parameters around the knee joint in order to simplify the evaluation of bone quality.
Patients and Methods
After obtaining ethical approval for this study, patients who simultaneously underwent DXA scans and radiographs of the knee were enrolled. Before DXA scans, pelvic and lumbar radiographs were undertaken in order to exclude any problem that might influence the BMD results. The inclusion criteria were: the ability to undertake normal activities; a full range of movement of the lower limbs with no deformity or dysplasia; no pathological change such as periosteal hyperplasia, hyperostosis, or osteolysis of the distal femur; no severe osteoarthritis (OA) of the knee according to the Kellgren–Lawrence grading score,22 (grade 0 to 2); and no history of trauma or surgery involving the knee. Exclusion criteria included: skeletal immaturity (age ⩽ 16 years); a history or evidence of metabolic bone disease such as diabetes, hyper- or hypoparathyroidism, Paget’s disease, osteomalacia, renal osteodystrophy or osteogenesis imperfecta, or other systemic disease such as rheumatoid arthritis, renal failure, and an immune disease; taking a relative’s medications; a neoplasia with known metastasis to bone; and a history or the presence of a hip fracture, vertebral fracture or disease, or other osteoporotic fractures and associated surgery including fixation or arthroplasty. After collection of the medical history, examination, DXA scans, and radiographs of the knee, every patient who satisfied the inclusion criteria was randomly enrolled by tossing a coin. In order to avoid the outcome of the coin toss being manipulated by the examiner, it was tossed by the patient. All the screening processes were handled one patient at a time, rather than taking place simultaneously. All patients gave written consent before having DXA scans and radiographs.
Radiological measurement
All patients had weight-bearing anteroposterior (AP) radiographs of the knee, in an extended position, using a standard technique. Which knee was radiographed was also decided by the toss of a coin by the patients. All radiographs were taken on the same X-ray machine (Philips Corp., New York, New York). The exposure was from mid-thigh (25 cm proximal to the joint line) to proximal tibia (5 cm distal to the joint line). The radiation dose was estimated to be 0.01 mSv.
A musculoskeletal radiologist (WWY) and orthopaedic surgeon (C-FL), each with > 20 years of experience, independently screened the radiographs and assigned Kellgren–Lawrence grades.22 They agreed on a grade by consensus if there was disagreement. There are five grades: 0, normal; 1, doubtful OA; 2, minimal OA; 3, moderate OA; and 4, severe OA.
The images were obtained using picture archiving and communication system workstations, and the measurements were performed using Kingstar Winning TV view software (Shanghai Kingstar Winning Medical Information Technology Co. Ltd., Shanghai, China), which has precision of within 0.01 mm.
Two parameters were measured from the distal femoral cortex: the mean cortical bone thickness (CBTavg) and the distal femoral cortical index (DFCI). The method for calculating the CBTavg of the medial and lateral distal femur was adapted from the methods used for the proximal humerus described by Bloom and Laws23 and Tingart et al.11 The anatomical axes of the femur (line P) were initially defined, as described by Luo.24 The CBTavg and DFCI were measured at two levels in which the lines were perpendicular to the line P. Level 1 was the most distal level of the femoral diaphysis where the tangent line of endosteal borders of the lateral diaphyseal cortices was separated from the diaphysis. Level 2 was 20 mm proximal and parallel to level 1. The distances between levels 1 and 2 were chosen in an effort to capture the transition zone from the diaphyseal to the metaphyseal bone. It has been suggested that this area would be sensitive to bone mineral loss.25 At these two levels, the points of intersection of the two lines and the edges of the distal femoral cortex (inner and outer edges) could be confirmed. The width of the entire bone could be measured at these levels from the outer medial cortex of the distal femur to the outer lateral cortex (E1 and E2). At the same level, a measurement of the width of the intramedullary canal was obtained (I1 and I2). The CBTavg was defined as the mean cortical thickness of levels 1 and 2; therefore, it could be calculated by [(E1-I1) + (E2-I2)]/2 for each patient and adjusted automatically for the magnification factor by the software. The measurement of DFCI was similar to the deltoid tuberosity index in the proximal humerus as described by Spross et al.12 The DFCI was measured at level 1, where the cortical change in the transitional area between the diaphysis and the metaphysis is most obvious. The ratio between the outer cortical (E1) and the inner endosteal diameter (I1) is calculated (E1/I1) as DFCI (Fig. 1).
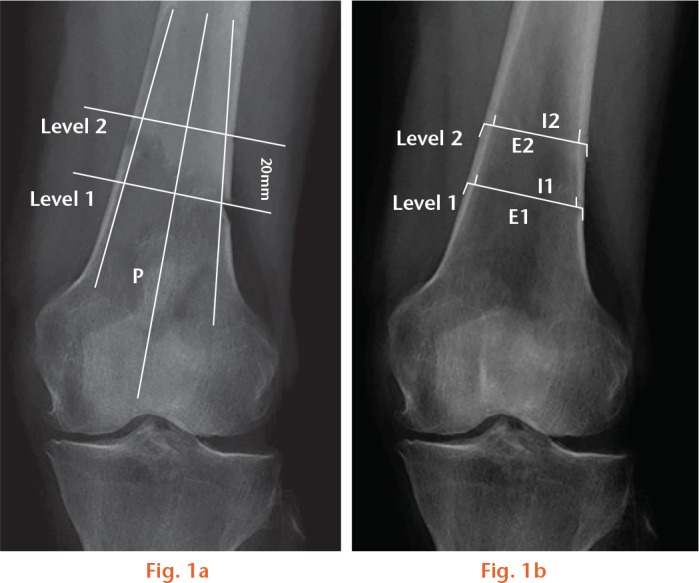
Schematic diagrams of the radiographic parameters on the anteroposterior view of the knee joint: a) the location of the two levels; b) the width of the entire bone and intramedullary canal; the cortical thickness of the medial and lateral side of the distal femur at these levels.
The mean of three consecutive measurements performed by one investigator was calculated for each patient. All measurements were performed twice, on two different days at four-week intervals by two independent investigators, a trauma surgeon (HS) and a resident doctor (YZ), to determine the intra- and interobserver variability.
BMD measurement
The BMD (g/cm2) of the lumbar spine (L1-4), and the left femoral neck and hip were measured using a Lunar Prodigy DXA densitometer (Lunar Corp., Madison, Wisconsin) and the data were analyzed using Prodigy Encore software (Ver. 6.70, Lunar Corp., standard array mode). The scanner was set on fan-beam mode and calibrated daily. The coefficient of variation (CV) was obtained from three repeated measurements on 15 patients. The CV for the BMD at L1-4, the left femoral neck, trochanter, and hip were 1.39%, 2.22%, 1.41%, and 0.70%, respectively.26 The T-score, based on comparisons with the maximum mean BMD found in healthy young adults of the same ethnicity and gender, was automatically calculated by the processor of the Lunar device. The bone quality was defined as: normal if the T-score was > -1.0; osteopenic if it was between -1.0 and -2.5; and osteoporotic if it was < -2.5.27 All scans were conducted by the same team with well-trained surveyors (team leader: YW) who were blinded to the study.
For the subset of patients in this analysis, BMD at the left hip including the femoral neck, greater trochanter and proximal femur, was strongly correlated with the value for the spine (L1-4) (Pearson’s r = 0.065, p = 0.0003). Patients who had osteophytes and/or disc space narrowing were excluded because these values were technically unsuitable for analysis. Thus, analyses with values for the hip are reported, while results were similar to those for the other site.
Statistical analysis
This was performed using Statistical Package for the Social Sciences, version 19.0 software (IBM Corp., Armonk, New York). All parameters were tested for normal distribution. Univariate analysis was performed using the chi-squared test or Fisher’s exact test for comparison of proportions between two categorical data. The Mann–Whitney U test was used to compare the non-parametric data between two independent samples. The level of statistical significance was defined as p ⩽ 0.05.
Intra- and interobserver reliabilities of the CBTavg and DFCI were assessed by calculating the intraclass correlation coefficients (ICC).28 The strength of agreement was assessed as described by Landis and Koch29: values of 0.81 to 1.00 indicating excellent agreement; 0.61 to 0.80, good agreement; 0.41 to 0.60, moderate agreement; 0.21 to 0.40, fair agreement; and 0 to 0.20, slight agreement. In order to evaluate differences between single ICC values, 95% confidence intervals (CI) were calculated. Differences between single ICC values were considered significant when upper and lower boundaries of the 95% CI did not overlap.30
Pearson’s correlation coefficient (r) was used to test the relationship between age, BMD, T-score, CBTavg, and DFCI, using the grading suggested by Evans31: r with 0.81 to 1.0, very strong correlation; 0.60 to 0.79, strong correlation; 0.40 to 0.59, moderate correlation; 0.20 to 0.39, weak correlation; and 0 to 0.19, very weak correlation.
Receiver operating characteristic (ROC) curve analysis was performed to determine the diagnostic efficiency of the CBTavg and DFCI for osteoporosis and osteopenia.32 The sensitivity, specificity, negative predictive values, and the area under the curve (AUC) were calculated from ROC. The value of the AUC was interpreted according to the following principle: non-predictive (AUC < 0.5); less predictive (0.5 < AUC ⩽ 0.7); moderately predictive (0.7 < AUC ⩽ 0.9); highly predictive (0.9 < AUC < 1.0); and perfect prediction (AUC = 1.0).33 AUC values of > 0.75 are generally considered to represent good performance. The difference between the AUCs under these two dependent ROC curves was tested with the method of DeLong et al.34
Statistical significance was set at p < 0.01.
Results
Between July 2015 and June 2016, a total of 361 eligible patients were enrolled into the study. Their characteristics, including diagnostic categories according to World Health Organization (WHO) criteria,35 are shown in Table I. The correlations between age and BMD of the lumbar spine and hip were very weak (r = -0.306, p < 0.001; r = -0.127, p = 0.004).
Table I.
Summary of descriptive characteristics of the 361 patients in the study
| Characteristic | |
|---|---|
| Mean age, yrs (sd; range) | 61.81 (12.31; 21 to 89) |
| Gender (female/male), n (%) | 294 (81.4)/67 (18.6) |
| Knee side (left/right), n (%) | 212 (58.7)/149 (41.3) |
| Mean BMI, kg/m2 (sd; range) | 24.32 (3.01; 15.39 to 33.87) |
| Mean BMD, g/cm2 (sd; range) | |
| Lumbar spine (L1 to L4) | 1.01 (0.18; 0.56 to 1.91) |
| Hip | 0.88 (0.13; 0.48 to 1.36) |
| Mean T-score (sd; range) | |
| Lumbar spine (L1 to L4) | -0.79 (0.39; -2.72 to 3.10) |
| Hip | -0.65 (1.05; -3.80 to 3.20) |
| Diagnostic categories, n (%)*† | |
| Normal | 228 (63.2) |
| Osteopenia | 99 (27.4) |
| Osteoporosis | 34 (9.4) |
According to the World Health Organization criteria35
Lowest BMD T-score in the lumbar spine or hip was considered
BMI, body mass index; BMD, bone mineral density
The mean CBTavg and DFCI for the whole cohort was 4.55 mm (sd 0.73; 2.38 to 6.90) and 1.10 mm (sd 0.03; 1.04 to 1.19), respectively.
The reliability of CBTavg and DFCI
Based on the plain radiographs, excellent intra- and interobserver reliability agreements could be achieved using the CBTavg and DFCI. The DFCI as a ratio showed higher intra- and interobserver reliability than CBTavg (Table II).
Table II.
Intraclass correlation coefficients (ICC) of mean cortical bone thickness of the distal femur (CBTavg) and the distal femoral cortex index (DFCI)
| Intraobserver (95% CI) | Interobservers (95% CI) | |
|---|---|---|
| ICC, CBTavg | 0.892 (0.867 to 0.912) | 0.890 (0.864 to 0.910) |
| ICC, DFCI | 0.910 (0.889 to 0.927) | 0.908 (0.887 to 0.925) |
| p-value | 0.021* | 0.018* |
Significant difference (p < 0.05)
CI, confidence interval
Correlation between CBTavg, DFCI, BMD, and T-score
There were strong correlations between the CBTavg and BMD of the hip (r = 0.664, p < 0.01), T-score (r = 0.654, p < 0.01) (Fig. 2). Moderate correlations were found between the DFCI and BMD of the hip (r = 0.457, p < 0.01), T-score (r = 0.464, p < 0.01) (Fig. 3).
Fig. 2.

Graph showing the correlation between the mean cortical bone thickness of the distal femur (CBTavg) and bone mineral density (BMD) of the hip and T-score.
Fig. 3.

Graph showing the correlation between the distal femoral cortex index (DFCI) and bone mineral density (BMD) of the hip and T-score.
ROC and AUC
The ROC and AUC showed a moderate accuracy for predicting osteoporosis using the CBTavg and DFCI, whereas CBTavg was better, as the AUC was larger than for DFCI (0.820 vs 0.740, z = 2.432, p = 0.015) (Fig. 4a). The cut-off value for CBTavg for predicting osteoporosis was 4.4 mm, with a sensitivity of 100% and a specificity of 61%. The cut-off value for the DFCI was 1.10, with a sensitivity of 88% and a specificity of 80% (Table III). CBTavg and DFCI were moderately accurate for the diagnosis of osteopenia; the AUC of CBTavg was better than that of DFCI (0.798 vs 0.721, z = 4.929, p = 0.019) (Fig. 4b). Selecting a 4.5 mm threshold value for CBTavg resulted in a sensitivity of 78% and a specificity of 67%, and selecting a 1.08 threshold value for DFCI resulted in a sensitivity of 51.52% and a specificity of 80.35% (Table IV).

Receiver operating characteristic curve analysis was performed to determine the diagnostic efficiency of the mean cortical bone thickness of the distal femur (CBTavg) and distal femoral cortex index (DFCI) for a) osteoporosis and b) osteopenia. AUC, area under the curve.
Table III.
Area under the curve (AUC) and the value for osteoporosis
| AUC (95% CI) | Criterion value (95% CI) | |
|---|---|---|
| CBTavg, mm | 0.820 (0.776 to 0.858) | 4.40 (4.365 to 4.4) |
| DFCI, mm | 0.740 (0.692 to 0.785) | 1.10 (1.093 to 1.097) |
| p-value | 0.015* | N/A |
Significant difference (p < 0.05)
CI, confidence interval; CBTavg, mean cortical bone thickness of the distal femur; DFCI, distal femoral cortex index; N/A, not applicable
Table IV.
Area under the curve (AUC) and value for osteopenia
| AUC (95% CI) | Criterion value (95% CI) | |
|---|---|---|
| CBTavg, mm | 0.798 (0.753 to 0.838) | 4.50 (4.315 to 4.935) |
| DFCI, mm | 0.721 (0.672 to 0.767) | 1.08 (1.068 to 1.087) |
| p-value | 0.019* | N/A |
Significant difference (p < 0.05)
CI, confidence interval; CBTavg, mean cortical bone thickness of the distal femur; DFCI, distal femoral cortex index; N/A, not applicable
Discussion
A simple and accurate method of identifying the risk of osteoporosis is essential for the management of orthopaedic patients. Although the BMD from DXA of the lumbar spine, hip, and proximal femur have been the benchmarks to screen for osteoporosis, these methods are not practical for either patients or practitioners, especially in an emergency or outpatient department.19 In the past, the bone quality has been assessed radiographically.23,36-40 However, the relationship between the radiographic parameters and BMD have not been reappraised.11,13,15-21,41 To our knowledge, this is the first study to propose new radiographic parameters focusing on the distal femur, where a fragility fracture has a high morbidity,42 and compare these parameters with the BMD from DXA.
Except for the BMD from conventional sites such as the lumbar spine, hip, and proximal femur as the reference, other studies have used different control groups11,12,17 or compared the radiographic parameters between different groups.14 Tingart et al11 evaluated the correlation between the BMD of the proximal humerus (the humeral head, the surgical neck, and the greater and lesser tuberosity) using DXA and the cortical thickness of the proximal humeral diaphysis. Peripheral quantitative CT (pQCT) may be used to evaluate the local BMD, but has limited availability. Spross et al12 defined and validated the deltoid tuberosity index in an attempt to simplify the measurement of bone quality in patients with a proximal humeral fracture using the BMD of the humeral head by pQCT as a control. Hepp et al14 evaluated the use of the cortical index as a predictor of the risk of failure after locking plate osteosynthesis of displaced proximal humeral fractures by comparing the fracture group with a control group of patients who had fallen on the shoulder without sustaining a fracture. However, it was subjective because the mechanism of injury, including the degree of violence and the condition of the patient, could not be controlled. Thus, the radiographic parameters or indices verified by local BMD or compared by different groups can only reflect local bone quality, and only the parameters or indices verified by the BMD from DXA could be a used when screening the whole body for osteoporosis.
The aims of this study were: 1) to provide a simple way of determining the bone quality of the whole body and a useful screening tool for osteoporosis without using DXA apparatus; 2) to raise awareness of a screening protocol for patients who are at risk of osteoporosis; and 3) to facilitate decision-making in the surgical treatment of patients with fractures or OA of the knee based on radiographic measurements of the uninjured distal femur.
Approximately half of all periarticular fractures about the knee, including distal femoral, tibial plateau, and patellar fractures, occur in osteoporotic patients, aged > 50 years, as a result of low-energy trauma.43 Unsatisfactory outcomes are common following surgery in elderly patients with osteoporosis due to loss of fixation, post-traumatic arthritis, malunion, and nonunion. Appropriate forms of treatment include conservative management, internal fixation, or arthroplasty and the availability of suitable implants including locking fixation systems, bone grafts, cements, or prostheses are required for managing these fractures.44-46 The use of parameters based on the radiographic appearances of the knee might allow easy evaluation of bone quality before treatment. Two such parameters with different natures were proposed and evaluated in our study, a numerical value (CBTavg) and a ratio (DFCI). Previously, only one type of parameter was used in most studies, either a numerical value or an index.11,13,15-21 We found that the radiographic parameters of the distal femur, CBTavg and DFCI, correlated well with BMD and the T-score. Thus, these parameters could be used for identifying both osteoporosis and osteopenia. Although the CBTavg was more accurate than DFCI in the diagnosis of both, DFCI had better ICCs than CBTavg, as it is a ratio and could be measured using a relatively simple formula regardless of the magnification of radiographic images or the size of the bone.
In addition, radiographs are routinely undertaken in symptomatic patients with arthritis of the knee, which is common in the elderly.47 Different views are not required and the measurements are based only on the AP view of the knee, without the lateral view, which may have varying degrees of rotation.
In order to eliminate the selection bias, the study was designed as a prospective study and the patients were screened to represent the general population without age limitation. DXA scans and radiographs were prospectively collected and examined simultaneously. We found a weak correlation between age and bone quality. Thus, analysis was not stratified according to age.
This study has limitations. It involved healthy Chinese patients, and the results are not generalizable to all races. Furthermore, the local BMD from the knee using DXA or a specific qCT was not obtained as a control, because we thought that these might be influenced by many factors, including the choosing of regions of interest, the measurement scope, and the regional soft tissue.
In conclusion, we propose two new radiographic parameters, the CBTavg and DFCI, from the distal femur, which may be used to predict osteoporosis and osteopenia reliably. They are simple and effective screening tools. The DFCI, which is a ratio, might be more user-friendly in clinical practice because of the simpler calculation with fewer influential factors.
Acknowledgments
We thank W. W. Yao of the radiological department for screening the radiographs and assigned Kellgren-Lawrence grades, and thank Y. Wang of the osteoporosis department for leading her team to conduct the DXA scan.Q-F. He and H. Sun contributed equally to this work.
Footnotes
Author Contributions: Q-F. He: Designing and conducting the study, Collecting and analyzing the data, Drafting the manuscript.
H. Sun: Designing and conducting the study, Collecting and analyzing the data, Drafting the manuscript.
L-Y. Shu: Collecting the data, Drafting the manuscript.
Y. Zhu: Analyzing the data, Drafting the manuscript.
X-T. Xie: Analyzing the data, Drafting the manuscript.
Y. Zhan: Analyzing the data, Drafting the manuscript.
C-F. Luo: Designing and conducting the study, Drafting the manuscript.
Conflict of Interest Statement: No conflicts of interest
Follow us @BoneJointRes
Funding Statement
No funding received.
References
- 1. Benzvi L, Gershon A, Lavi I, Wollstein R. Secondary prevention of osteoporosis following fragility fractures of the distal radius in a large health maintenance organization. Arch Osteoporos 2016;11:20. [DOI] [PubMed] [Google Scholar]
- 2. Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury 2006;37:691-697. [DOI] [PubMed] [Google Scholar]
- 3. Harvey NC, Curtis EM, van der Velde R, et al. On epidemiology of fractures and variation with age and ethnicity. Bone 2016;93:230-231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Hopkins RB, Burke N, Von Keyserlingk C, et al. The current economic burden of illness of osteoporosis in Canada. Osteoporos Int 2016;27:3023-3032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Chang CY, Tang CH, Chen KC, Huang KC, Huang KC. The mortality and direct medical costs of osteoporotic fractures among postmenopausal women in Taiwan. Osteoporos Int 2016;27:665-676. [DOI] [PubMed] [Google Scholar]
- 6. Goldhahn J, Suhm N, Goldhahn S, Blauth M, Hanson B. Influence of osteoporosis on fracture fixation—a systematic literature review. Osteoporos Int 2008;19:761-772. [DOI] [PubMed] [Google Scholar]
- 7. Van Lieshout EM, Alt V. Bone graft substitutes and bone morphogenetic proteins for osteoporotic fractures: what is the evidence? Injury 2016;47(Suppl 1):S43-S46. [DOI] [PubMed] [Google Scholar]
- 8. Horwitz DS, Kubiak EN. Surgical treatment of osteoporotic fractures about the knee. Instr Course Lect 2010;59:511-523. [PubMed] [Google Scholar]
- 9. Kammerlander C, Neuerburg C, Verlaan JJ, et al. The use of augmentation techniques in osteoporotic fracture fixation. Injury 2016;47(Suppl 2):S36-S43. [DOI] [PubMed] [Google Scholar]
- 10. Amstrup AK, Jakobsen NF, Moser E, et al. Association between bone indices assessed by DXA, HR-pQCT and QCT scans in post-menopausal women. J Bone Miner Metab 2016;34:638-645. [DOI] [PubMed] [Google Scholar]
- 11. Tingart MJ, Apreleva M, von Stechow D, Zurakowski D, Warner JJ. The cortical thickness of the proximal humeral diaphysis predicts bone mineral density of the proximal humerus. J Bone Joint Surg [Br] 2003;85-B:611-617. [DOI] [PubMed] [Google Scholar]
- 12. Spross C, Kaestle N, Benninger E, et al. Deltoid tuberosity index: a simple radiographic tool to assess local bone quality in proximal humerus fractures. Clin Orthop Relat Res 2015;473:3038-3045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Mather J, MacDermid JC, Faber KJ, Athwal GS. Proximal humerus cortical bone thickness correlates with bone mineral density and can clinically rule out osteoporosis. J Shoulder Elbow Surg 2013;22:732-738. [DOI] [PubMed] [Google Scholar]
- 14. Hepp P, Theopold J, Osterhoff G, et al. Bone quality measured by the radiogrammetric parameter “cortical index” and reoperations after locking plate osteosynthesis in patients sustaining proximal humerus fractures. Arch Orthop Trauma Surg 2009;129:1251-1259. [DOI] [PubMed] [Google Scholar]
- 15. Skedros JG, Mears CS, Burkhead WZ. Ultimate fracture load of cadaver proximal humeri correlates more strongly with mean combined cortical thickness than with areal cortical index, DEXA density, or canal-to-calcar ratio. Bone Joint Res 2017;6:1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sah AP, Thornhill TS, LeBoff MS, Glowacki J. Correlation of plain radiographic indices of the hip with quantitative bone mineral density. Osteoporos Int 2007;18:1119-1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Baumgärtner R, Heeren N, Quast D, Babst R, Brunner A. Is the cortical thickness index a valid parameter to assess bone mineral density in geriatric patients with hip fractures? Arch Orthop Trauma Surg 2015;135:805-810. [DOI] [PubMed] [Google Scholar]
- 18. Feola M, Rao C, Tempesta V, Gasbarra E, Tarantino U. Femoral cortical index: an indicator of poor bone quality in patient with hip fracture. Aging Clin Exp Res 2015;27(Suppl 1):S45-S50. [DOI] [PubMed] [Google Scholar]
- 19. Agarwal S, Das SK, Agarwal GG, Srivastava R, Singh GP. X-ray knee as a screening tool for osteoporosis. J Clin Densitom 2012;15:362-365. [DOI] [PubMed] [Google Scholar]
- 20. Sadat-Ali M, Elshaboury E, Al-Omran AS, et al. Tibial cortical thickness: A dependable tool for assessing osteoporosis in the absence of dual energy X-ray absorptiopmetry. Int J Appl Basic Med Res 2015;5:21-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Patterson J, Rungprai C, Den Hartog T, et al. Cortical bone thickness of the distal part of the tibia predicts bone mineral density. J Bone Joint Surg [Am] 2016;98-A:751-760. [DOI] [PubMed] [Google Scholar]
- 22. Kellgren JH, Lawrence JS. Epidemiology of chronic rheumatism. In: Kellgren JH, ed. Atlas of Standard Radiographs of Arthritis. Philadelphia: FA Davis, 1963:10-11. [Google Scholar]
- 23. Bloom RA, Laws JW. Humeral cortical thickness as an index of osteoporosis in women. Br J Radiol 1970;43:522-527. [DOI] [PubMed] [Google Scholar]
- 24. Luo CF. Reference axes for reconstruction of the knee. Knee 2004;11:251-257. [DOI] [PubMed] [Google Scholar]
- 25. Edwards WB, Schnitzer TJ, Troy KL. Bone mineral and stiffness loss at the distal femur and proximal tibia in acute spinal cord injury. Osteo Int 2014;25:1005-1015. [DOI] [PubMed] [Google Scholar]
- 26. Yu JB, Ke YH, He JW, et al. No association between LRP5 gene polymorphisms and bone and obesity phenotypes in Chinese male-offspring nuclear families. Acta Pharmacol Sin 2010;31:1464–1469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Kanis JA, Melton LJ, III, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res 1994;9:1137–1141. [DOI] [PubMed] [Google Scholar]
- 28. McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods 1996;1:30-46. [Google Scholar]
- 29. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159-174. [PubMed] [Google Scholar]
- 30. Doornberg J, Lindenhovius A, Kloen P, et al. Two and three-dimensional computed tomography for the classification and management of distal humeral fractures. Evaluation of reliability and diagnostic accuracy. J Bone Joint Surg [Am] 2006;88-A:1795–1801. [DOI] [PubMed] [Google Scholar]
- 31. Evans JD. Straightforward Statistics for the Behavioral Sciences. Pacific Grove, California: Brooks/Cole Publishing, 1995. [Google Scholar]
- 32. Swets JA. Measuring the accuracy of diagnostic systems. Science 1988;240:1285–1293. [DOI] [PubMed] [Google Scholar]
- 33. Greiner M, Pfeiffer D, Smith RD. Principles and practical application of the receiver-operating characteristic analysis for diagnostic tests. Prev Vet Med 2000;45:23–41. [DOI] [PubMed] [Google Scholar]
- 34. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44:837-845. [PubMed] [Google Scholar]
- 35. Delmas PD. Do we need to change the WHO definition of osteoporosis? Osteoporos Int 2000;11:189-191. [DOI] [PubMed] [Google Scholar]
- 36. Virtama P, Telkka A. Cortical thickness as an estimate of mineral content of human humerous and femur. Br J Radiol 1962;35:632-633. [DOI] [PubMed] [Google Scholar]
- 37. Meema HE, Meema S. Measurable Roentgenologic changes in some peripheral bones in senile osteoporosis. J Am Geriatr Soc 1963;11:1170-1182. [DOI] [PubMed] [Google Scholar]
- 38. Virtama P, Mahonen H. Thickness of the cortical layer as an estimate of mineral content of human finger bones. Br J Radiol 1960;33:60-62. [DOI] [PubMed] [Google Scholar]
- 39. Barnett E, Nordin BE. The radiological diagnosis of osteoporosis: a new approach. Clin Radiol 1960;11:166-174. [DOI] [PubMed] [Google Scholar]
- 40. Bloom RA. A comparative estimation of the combined cortical thickness of various bone sites. Skeletal Radiol 1980;5:167-170. [DOI] [PubMed] [Google Scholar]
- 41. Wahner HW, Dunn WL, Brown ML, Morin RL, Riggs BL. Comparison of dual-energy x-ray absorptiometry and dual photon absorptiometry for bone mineral measurements of the lumbar spine. Mayo Clin Proc 1988;63:1075-1084. [DOI] [PubMed] [Google Scholar]
- 42. Park KC, Lim SJ, Song YS, Hwang KT. Factors affecting peri-implant fracture following locking plate for osteoporotic distal femur fractures. Orthop Traumatol Surg Res 2017;103:1201-1204. [DOI] [PubMed] [Google Scholar]
- 43. Bohm ER, Tufescu TV, Marsh JP. The operative management of osteoporotic fractures of the knee: to fix or replace? J Bone Joint Surg [Br] 2012;94-B:1160-1169. [DOI] [PubMed] [Google Scholar]
- 44. Ries MD. Primary arthroplasty for management of osteoporotic fractures about the knee. Curr Osteoporos Rep 2012;10:322-327. [DOI] [PubMed] [Google Scholar]
- 45. van de, Pol GJ, Iselin LD, Callary SA, et al. Impaction bone grafting has potential as an adjunct to the surgical stabilisation of osteoporotic tibial plateau fractures: early results of a case series. Injury 2015;46:1089-1096. [DOI] [PubMed] [Google Scholar]
- 46. Doht S, Lehnert T, Frey S, et al. Effective combination of bone substitute and screws in the jail technique: a biomechanical study of tibial depression fractures. Int Orthop 2012;36:2121-2125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Tak EC, van Meurs JB, Bierma-Zeinstra SM, Hofman A, Hopman-Rock M. Changes in disability in older adults with generalized radiographic osteoarthritis: A complex relationship with physical activity. Musculoskeletal Care 2017;15:364-372. [DOI] [PubMed] [Google Scholar]