

Abstract
Type 2 diabetes is the most common cause of hyperglycemia. It has different prevalence in various populations. It has been found out that type 2 diabetes is a genetic disorder; however, its inheritance and its type have not been well defined. In studying the genes involved in the development of diabetes, several genes have been introduced as candidates; however, the gene or genes involved in diabetes cannot be identified yet. As family diabetes has not been studied in Iran so far, this study was conducted on a population aged over 20 years in east of Tehran. In a population of 14,687 people living in east of Tehran, 180 families with type 2 diabetes were identified. In this research, 802 subjects were female and 792 were male. After oral glucose tolerance test, 40.7% of females and 32.3% of males had diabetes. The incidence of diabetes in females was significantly higher than that in males (P < 0.001). It was found that 656 diabetic patients had age over 20 years, which most of them had age between 41 and 70 years. The highest number of diabetic patients was in the age group of 51–60 years. The percentage of offspring and siblings involvement in this sample was 44% and 53%, respectively. The highest level of involvement among the first-degree family members belonged to sister-brother, followed by father-daughter. This study shows the relationship between family diabetes in Iranian families in a demographic study. By recognizing the family relations, effective measures can be taken to prevent this disease. In the case of type 2 diabetes development in one member of family, the incidence of diabetes in other family members would increase by up to 50%. Thus, screening is suggested for all type 2 diabetic family members continuously so that the disease to be immediately diagnosed and treated to prevent major complications of diabetes.
Keywords: Epidemiology, familial diabetes, type 2 diabetes
INTRODUCTION
Hyperglycemia is the most common metabolic disorder and type 2 diabetes is the most common cause of hyperglycemia. The prevalence of type 2 diabetes is different in various populations. Its prevalence is <6% in most communities; however, it has been reported more than 50% in Pima Indians.[1] The prevalence of type 2 diabetes is increasing, and this is a warning sign for communities. It is believed that both environmental and genetic factors are involved in this disease. It has been recognized that MODY is a dominant autosomal disease and specific mutations have been found in the mitochondrial genome in maternal family diabetes associated with caries; however, these cases account for a small percentage of the causes of diabetes and the causes of diabetes have mainly remained unknown.[2]
Family is more involved in type 2 diabetes than type 1 diabetes; however, it is not clear that how this disease is transmitted.[3] Several genes are involved in type 2 diabetes, and a single gen is not involved in this disease. In fact, it is a polygenic disease and the genetic affects it strongly.[4] The study of identical twins confirms very strong role of genetic in this disease. If one of the twins is affected by type 2 diabetes, other twin would be also affected by it.[4] However, the incidence of diabetes in twins might not be simultaneous, so that it was found in one study that the prevalence of diabetes in other twin is 58%; however, it increased to 100% after 10 years of diabetes in other twins.[4] Genetic factors play an important role in the development of type 2 diabetes. Although many genes, which are involved in this disease, have not been identified yet, it is clear that this disease is polygenic and multifactorial disease. Various genetic leukosis is involved in susceptibility to this disease, and environmental factors such as nutrition and physical activity are also effective in its phenotypic development.[4] Children of people, which one of their parents has type 2 diabetes, are at increased risk of diabetes, and if the parents of one person have type 2 diabetes, the risk of development of disease in the offspring would be 40%.
Insulin resistance, manifested as a reduced consumption of glucose in skeletal muscle, is found in many first-degree nondiabetic relatives of type 2 diabetic patients.[5] However, it is difficult to define the genetic abnormality of type 2 diabetes since genetic defect in the secretion or function of insulin may not be revealed until an environmental factor or other genetic defect such as obesity is added to it.[5] However, studies have shown that >50% of the first-degree relatives of type 2 diabetic people will develop diabetes until the age of 80.[6]. The unclear issue in this regard is the increased prevalence of type 1 diabetes in offspring of diabetic patients. It has not yet been found that whether association of type 1 diabetes in a family is due to a single inheritance trait (that is, type 2 diabetes is the type 1 diabetes) or there is two common genetic predisposition incidentally in one family which each of them probably affects each other's manifestations. Studies have reported that there is an autoantibody against β-cell in 10%–38% of type 2 diabetic patients and it suggests that there is a sub-autoimmunity state of type 2 diabetes.[7,8]
In addition, in a family, two diabetic people may not be affected by diabetes through the single gene; however, two genes might be involved in the diabetes.[8,9,10] No study has been conducted yet on family diabetes and genes affecting type 2 diabetes in Iran. Although little information has been reported on the genetic transmission process in some studies, a certain family tree of these families is not available. Obtaining such information is very important to predict the diabetes status in their families and the marriage of diabetics with each other and with nondiabetic subjects and to find the dominant genes involved in type 2 diabetes in Iran. Thus, this study was conducted in the east of Tehran to evaluate the prevalence of family diabetes.
METHODOLOGY
The subjects studied in this study were selected from Tehran Lipid and Glucose Study (TLGS). In the TLGS study, 14,687 people were examined. As the objective of the study was to evaluate type 2 diabetes in subjects aged over 20 years, people over the age of 20 years (10,136 people) were tested for fasting blood glucose and 2-h glucose after consuming 75 g of glucose. In this study, subjects with type 1 diabetes and normal people were excluded from the study. Finally, 1291 type 2 diabetic people were identified [Algorithm 1].
Algorithm 1.
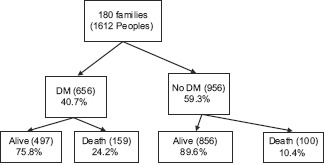
Screening of 180 families (1612 people)
To diagnose the type 2 family diabetes, questionnaires were completed by qualified questioners, and accordingly, 565 Type 2 diabetic people were identified. These people had at least one type 2 first-degree family member (father, mother, brothers, sisters, and children). Out of them, 407 diabetic families were available, which 44% (180 families) were willing to cooperate in the study. A total of 180 alive families, aged over 20 years (1335 people), underwent fasting blood glucose test, and oral glucose tolerance test. Finally, the family tree of each family was mapped, and the relationship between the sisters-brothers (siblings) and children with the parents was determined. Chi-square and t-test were used to compare the results.
RESULTS
Out of 180 families (1594), 259 died, which 159 of them had previously known diabetes, which accurate information was not on diabetes or nondiabetic status of 100 of them. Thus, they were considered as “probably nondiabetic” people. Among those who were alive (1335 people), 479 had diabetes [Algorithm 1]. Table 1 shows the distribution of diabetic people and the distribution of total alive members of studied families in different age groups.
Table 1.
Calcification of diabetic patients by age groups

Based on Table 1, 78.8% of diabetics were 41–70 years of old, and the highest percentage belonged to age group of 51–60 years, which included about one-third of the total diabetic population. The lowest percentages belonged to age group of 20–30 years, which only 1.2% of the diabetics were in this age group. Table 1 shows that the age group of 71–80 years includes 9.25% of the total diabetic population, while 48.42% in this age group are diabetic and those in the age group of over 81 years include 2.41% of this population and 29.2% of them are diabetic. In this study, the number of females and males was almost equal (802 females and 792 males), whereas diabetes was seen more in females than that in males (286 female diabetes versus 211 male diabetes) (P < 0.001).
Twenty-five family marriages were observed in 180 families; however, no difference was seen between their offspring and other families regarding the incidence of diabetes. The percentage of offspring (children) and siblings (sisters and brothers) involvement was 44% and 53%, respectively, and the most diabetes involvement belonged to siblings (52.7%) [Table 2].
Table 2.
Prevalence of diabetic patients in offspring

In this study, in 57 families, only mothers had diabetes. The total number of children in this group was 253, which 144 of them (57%) were diabetic [Table 2]. In addition, in 57 families, only fathers had diabetes, and the total number of children in this group was 274 people, which 136 (49.6%) of them were diabetes.
In this study, both parents were diabetic in 42 families. This group had 184 children, which 98 (53.3%) of them had diabetes. In 23 families, none of the parents had diabetes, and 57.9% of their children had diabetes. In this study, three families had no diabetic parents, while all their children had diabetes.
DISCUSSION
This study is the first study conducted in Iran to evaluate the prevalence of family diabetes in an Iranian population. In TLGS, the prevalence of type 2 diabetes in subjects aged over 20 years was 11.4% based on 2-h blood glucose after consuming 75 g of glucose equal to or >200 mg/dl. In most communities, its prevalence has been reported 5%–6%. The prevalence of diabetes increases with aging so that it reaches more than 9% in people aged over 65 years.[1] Family studies on the incidence of diabetes in families are important since type 2 diabetes is a genetic and family disease. One person with type 2 diabetes in a family increases the likelihood of diabetes in other first-degree members of the family so that the percentage of offspring and siblings involvement reaches 33%.[11,12]
In this study, the percentage of offspring and siblings involvement was 44% and 53%, respectively, which this figure is slightly higher than previously reported figures. Increasing incidence of diabetes in Iran could be due to the prevalence of diabetes in this study or systematic screening for the diagnosis of type 2 diabetes in the current study. Sampling method might be another reason in this regard. Selective sampling was used in this study and subjects included in this study had type 2 diabetes and at least one of their first-degree family members was diabetic. Another reason is the increasing industrialization of Iran and nutritional issues, so more studies are required to be conducted to find the cause this increasing trend. Lack of knowledge on the genetic nature and inheritance of type 2 diabetes has caused that today's science to be unable in predicting the incidence of diabetes in diabetic first-degree individuals.[13] Genetic examination cannot predict diabetes in the children of these people, except in specific mutations and MODY in the maternally transmitted mitochondrial genome. MODY is major genetic achievement in diabetes and it includes 2%–2.5% of diabetes; however, 10%–15% of the diabetic people population are MODY in France.[13]
Many studies have reported that the prevalence of diabetes is slightly higher in females than that in males. In the study conducted by Yavari, the ratio of diabetic females to diabetic males was 4:1, while the ratio of normal males to females was equal in that population.[2] In the research conducted by Ramchandran, no significant difference was seen in diabetic males and females (301 versus 307) (P < 0.62).[14] In this study, the prevalence of diabetes was significantly higher in females than that in males (40.6% versus 32.3%) (P < 0.001). In 42 families, both parents had diabetes, which 53.3% of their children were diabetic, and 23 families were found in which none of the parents had diabetes; however, 57.9% of their children had diabetes. Based on other studies, when both parents had type 2 diabetes, the risk of diabetes in children would be higher. Most of the studies revealed that disease transmission in cases where the mother is involved is more than when the father is involved.
In the study conducted by Vassy on 2310 diabetic patients, it was found that the incidence of diabetes is higher when the mother is involved;[15] however, in the study conducted by Ridderstrale, this increase was not observed.[16] In the conducted study, the percentage of children involvement is more when they have diabetic mothers. In 57 families, in which only father is diabetic, the percentage of diabetic children was 52% on average, and in 57 families, in which only mother had diabetes, the percentage of diabetic children was 59% on average, indicating that mothers’ involvement in diabetes plays more important role in children involvement of children. This should be sought in genetic transmission of mothers, which maternal mitochondrial mutation with maternal transmission is one of these cases.[17,18]
A study conducted by Ridderstrale, 3243 people were examined and it was found that type 2 diabetes and its mother carrier. A study found that 60% of type 2 diabetic patients along with caries had this mutation.[16] In a study, it was found that the mothers of MODY people were more likely diabetic than fathers (fathers 9.1% vs. mothers 18.2%).[13] Morris found that the frequency of diabetes is 2.5 times more when the father is involved in diabetes.[19] Another study conducted on pregnancy diabetes found that 3% of mothers of these people were diabetic and 8.8% of their fathers were diabetic.[20] Another issue making the genetic examination more difficult is the presence of diabetes in children whose parents are not diabetic.
In this study, three families were found in which all children had diabetes; however, their parents were not diabetic. There were also 23 families in the study, in which parents had no diabetes, while 57.9% of their children were diabetic. No specific justification can be provided for these families. Another issue is the relationship between type 2 diabetes and type 1 diabetes. Epidemiologic studies suggest that if the parents have type 2 diabetes, the chance of development of type 1 diabetes in children would be higher.[21] It indicates the genetic association between type 2 diabetes and type 1 diabetes. There are 856 healthy people in these families; however, it should be noted that the risk of diabetes in these subjects is not rejected, and with increasing the age, there is a risk of diabetes involvement in these people since the incidence of diabetes increases with increasing the age.
Relative distribution of the age group in all living subjects in this study showed that the highest rate of it belonged to age group of 41–44 years (26.5%) and the lowest rate of it belonged to those aged over 81 years (% 3). In addition, the percentage of diabetic people is the highest in the age group of 51–60 years (55.3%), followed by the age group of 71–80 years (48.42%). Moreover, as the percentage of living people older than 81 years was 3%, it is seen that the percentage of diabetic people in this age group was 29.3%. These findings suggest this fact that the incidence of diabetes increases with increasing the age, and if the first-degree members of family are living adequately, they would probably be affected by diabetes. One reason for the difference in the prevalence of type 2 diabetes and diabetes in children and siblings are age and average life expectancy in the community. Based on Table 1, 78.8% of diabetic people were in the age group of 41–70 years and the highest percentage of them was in the age group of 51–60 years (32.3%). Current studies suggest that the maximum incidence of diabetes is in the age group of 51–60 years, and then, this trend decreases and reaches 2.4% in subjects older than 81 years. Reduced prevalence of diabetes in people aged over 60 is due to an increase in the mortality rate of diabetics in this age group, and another reason is lower average life expectancy in Iran compared to that in other countries.
Thus, the population at risk of diabetes is in the age range of 41–60 years, so screening programs in this age group should be applied so that almost one-third of the diabetic people in the community are not aware of their diabetes.[22] Investigating the percentage of diabetic people in each family showed that the highest percentage was related to the presence of 3 diabetics in one family (35%) and the lowest was related to seven diabetics in one family. This might be due to the large number of low-population families compared to high-population families. In this study, 25 families of diabetic people had family marriage, while significant change was not found in the development of diabetes in their children. It seems that family marriage has no significant impact on development of family type 2 diabetes. In other studies, the increased prevalence of diabetes in children in family marriage has not been reported.
With regard to relations of diabetic first-degree family members, the highest percentage is related to the sister-brother, and the relations of mother-daughter, father-daughter, and sister-sister are almost the same. This study identified important points with regard to inherited the transmission of diabetes in the urban community and could be used in genetic investigation of family diabetes in the country. Gene testing is required in patients with family history of type 2 diabetes, because genetic transmission is very common in these people.
Financial support and sponsorship
This study was financially supported by Tehran University of Medical sciences.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi: 10.1016/j.diabres.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 2.Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378:31–40. doi: 10.1016/S0140-6736(11)60679-X. [DOI] [PubMed] [Google Scholar]
- 3.Yavari A, Najafipoor F, Aliasgarzadeh A, Niafar M, Mobasseri M. Effect of aerobic exercise, resistance training or combined training on glycaemic control and cardiovascular risk factors in patients with type 2 diabetes. Biol Sport. 2012;29:135. [Google Scholar]
- 4.Qureshi N, Kai J. Informing patients of familial diabetes mellitus risk: How do they respond?. A cross-sectional survey. BMC Health Serv Res. 2008;8:37. doi: 10.1186/1472-6963-8-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Najafipour F, Mobasseri M, Yavari A, Nadrian H, Aliasgarzadeh A, Mashinchi Abbasi N, et al. Effect of regular exercise training on changes in HbA1c, BMI and VO2max among patients with type 2 diabetes mellitus: An 8-year trial. BMJ Open Diabetes Res Care. 2017;5:e000414. doi: 10.1136/bmjdrc-2017-000414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ayyobi AF, Brunzell JD. Lipoprotein distribution in the metabolic syndrome, type 2 diabetes mellitus, and familial combined hyperlipidemia. Am J Cardiol. 2003;92:27J–33J. doi: 10.1016/s0002-9149(03)00613-1. [DOI] [PubMed] [Google Scholar]
- 7.Anaya JM, Castiblanco J, Tobón GJ, García J, Abad V, Cuervo H, et al. Familial clustering of autoimmune diseases in patients with type 1 diabetes mellitus. J Autoimmun. 2006;26:208–14. doi: 10.1016/j.jaut.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 8.InterAct Consortium, Scott RA, Langenberg C, Sharp SJ, Franks PW, Rolandsson O, et al. The link between family history and risk of type 2 diabetes is not explained by anthropometric, lifestyle or genetic risk factors: The EPIC-interAct study. Diabetologia. 2013;56:60–9. doi: 10.1007/s00125-012-2715-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mobasseri M, Yavari A, Najafipoor F, Aliasgarzadeh A, Niafar M. Effect of a long-term regular physical activity on hypertension and body mass index in type 2 diabetes patients. J Sports Med Phys Fitness. 2015;55:84–90. [PubMed] [Google Scholar]
- 10.Boney CM, Verma A, Tucker R, Vohr BR. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics. 2005;115:e290–6. doi: 10.1542/peds.2004-1808. [DOI] [PubMed] [Google Scholar]
- 11.Carlsson S, Midthjell K, Grill V. Influence of family history of diabetes on incidence and prevalence of latent autoimmune diabetes of the adult: Results from the Nord-Trøndelag Health Study. Diabetes Care. 2007;30:3040–5. doi: 10.2337/dc07-0718. [DOI] [PubMed] [Google Scholar]
- 12.Janssens AC, van Duijn CM. Genome-based prediction of common diseases: Advances and prospects. Hum Mol Genet. 2008;17:R166–73. doi: 10.1093/hmg/ddn250. [DOI] [PubMed] [Google Scholar]
- 13.Vassy JL, Hivert MF, Porneala B, Dauriz M, Florez JC, Dupuis J, et al. Polygenic type 2 diabetes prediction at the limit of common variant detection. Diabetes. 2014;63:2172–82. doi: 10.2337/db13-1663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ramachandran A, Snehalatha C, Sivasankari S, Hitman GA, Vijay V. Parental influence on the spectrum of type 2 diabetes in the offspring among Indians. J Assoc Physicians India. 2007;55:560–2. [PubMed] [Google Scholar]
- 15.Vassy JL, Durant NH, Kabagambe EK, Carnethon MR, Rasmussen-Torvik LJ, Fornage M, et al. A genotype risk score predicts type 2 diabetes from young adulthood: The CARDIA study. Diabetologia. 2012;55:2604–12. doi: 10.1007/s00125-012-2637-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ridderstråle M, Groop L. Genetic dissection of type 2 diabetes. Mol Cell Endocrinol. 2009;297:10–7. doi: 10.1016/j.mce.2008.10.002. [DOI] [PubMed] [Google Scholar]
- 17.Manning AK, Hivert MF, Scott RA, Grimsby JL, Bouatia-Naji N, Chen H, et al. A genome-wide approach accounting for body mass index identifies genetic variants influencing fasting glycemic traits and insulin resistance. Nat Genet. 2012;44:659–69. doi: 10.1038/ng.2274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Prudente S, Jungtrakoon P, Marucci A, Ludovico O, Buranasupkajorn P, Mazza T, et al. Loss-of-function mutations in APPL1 in familial diabetes mellitus. Am J Hum Genet. 2015;97:177–85. doi: 10.1016/j.ajhg.2015.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Morris AP, Voight BF, Teslovich TM, Ferreira T, Segrè AV, Steinthorsdottir V, et al. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet. 2012;44:981–90. doi: 10.1038/ng.2383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Scott RA, Lagou V, Welch RP, Wheeler E, Montasser ME, Luan J, et al. Large-scale association analyses identify new loci influencing glycemic traits and provide insight into the underlying biological pathways. Nat Genet. 2012;44:991–1005. doi: 10.1038/ng.2385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mellin AE, Neumark-Sztainer D, Patterson J, Sockalosky J. Unhealthy weight management behavior among adolescent girls with type 1 diabetes mellitus: The role of familial eating patterns and weight-related concerns. J Adolesc Health. 2004;35:278–89. doi: 10.1016/j.jadohealth.2003.10.006. [DOI] [PubMed] [Google Scholar]
- 22.Hussain A, Claussen B, Ramachandran A, Williams R. Prevention of type 2 diabetes: A review. Diabetes Res Clin Pract. 2007;76:317–26. doi: 10.1016/j.diabres.2006.09.020. [DOI] [PubMed] [Google Scholar]