

Abstract
Objective
This study examined the moderating and mediating effects of perceived social support on the association between pre-college sexual assault (SA) and college-onset SA.
Participants
A representative sample of 6,132 undergraduates.
Methods
The PLUM procedure in SPSS was used to test the moderation model, with individual regressions conducted in a hierarchical fashion. A weighted least squared mean and variance adjusted (WLSMV) mediation model was used to examine the mediating effect of social support.
Results
Pre-college SA significantly predicted college-onset SA. Social support significantly mediated the relation between pre-college SA and college-onset SA. Social support was not a significant moderator of this relationship.
Conclusions
Given the high prevalence of SA among college populations, as well as the high rates of SA revictimization, identification of factors that may be related to repeated SA (e.g., low social support) within this population are essential and may inform intervention, policy, and university student services.
Keywords: sexual assault, revictimization, social support, trauma, resilience
Upwards of 25% of women and 7% of men experience a sexual assault (SA) while enrolled in college1,2, making SA the most common form of violence on US college campuses3. Large-scale surveys of college students suggest that approximately one in five female undergraduates have experienced attempted or completed SA following college enrollment2,4, with up to 7.3% reporting SA in the previous 12 months5. Notably, rates of SA are higher among college-aged women than any other age groups6. Furthermore, in a nationally representative sample of college women, only 11.2% of rapes were reported7 and another study found that university reports of sexual assault increase by approximately 44% during audit periods and return to pre-audit levels once the audit period is over8. While focusing on primary prevention targeted at potential perpetrators is essential, the alarmingly high and consistent rates of SA on college campuses elucidate the need to also identify risk factors for victimization to inform intervention, policy, and student services.
One significant risk factor for SA is prior history of SA; in fact, a prior history of SA is associated with a threefold increased risk for future SA9. This association has been demonstrated in both retrospective and prospective research designs10 and has been found among college11,12, clinical13,14, and community-based samples15,16. Moreover, strong associations between repeated SA and psychopathology have been demonstrated. Survivors of repeated SAs are at increased risk for psychiatric conditions, including posttraumatic stress disorder (PTSD) and depression, and are at greater risk of experiencing co-occurring disorders17–21. Considering exposure to childhood sexual abuse doubles, sometimes triples, the likelihood of SA after the age of 1614, it is possible that a large proportion of college-onset victims of SA are not experiencing their first assault, but instead a repeated assault. Pervasive rates of SA and SA revictimization among college populations underscore the need to identify potential risk and protective factors that may influence the likelihood of revictimization. Previous research has demonstrated factors that not only impact differential responses to SA, but also influence the likelihood of repeated SA. Non-male gender (i.e., transgender22 and female gender23), ethnic10 and sexual24,25 minority status, and age14 have been linked to increased risk for SA revictimization.
Although examination of demographic factors associated with SA outcomes and risk of repeated SA may aid in targeting of prevention programming, identification of potentially modifiable variables is critical. To that end, social support has been associated with SA and SA revictimization26,27, as well as with risk for psychopathology post-trauma28–30. For instance, poor social support following SA has been associated with increased self-blame31, lack of interpersonal assertiveness32,33, and use of substances to cope34, which may in turn increase the likelihood of experiencing a repeated assault33,35. Although associations between correlates of social support (e.g., self-blame, lack of assertiveness) and SA revictimization have been identified (e.g.,31,33,36), these studies were cross-sectional and mediation cannot be inferred. Meta-analytic reviews of PTSD have consistently shown that social support is the strongest protective factor against PTSD29,37, suggesting that social support may serve as an important marker for resilience.
The targeting of modifiable factors (e.g., social support) that may buffer the relationship between prior history of SA and college-onset SA is gaining increasing federal support, as SA on college campuses receives growing public attention. As dictated by the Campus Sexual Violence Elimination Act (SaVE), a provision of the Violence Against Women Act (VAWA), all higher education institutions that receive federal funding are required to provide rape prevention programs that include a focus on primary prevention, bystander intervention, and risk reduction (Violence Against Women Reauthorization Act of 2013). Bystander intervention training aims to equip community members with the responsibility and skills to provide social support by responding to rape before, during, or after an assault occurs38. The bystander-intervention model is endorsed by policy makers and sexual assault advocates alike; however, research on best practices utilizing this approach is in its infancy39.
Although previous research exists demonstrating the mediating and moderating effects of social support on the relation between SA and mental and physical health40–42, no studies to our knowledge have investigated the mediating or the moderating effects of social support on the relation between prior history of SA and college-onset SA. Examination of these putative pathways could inform valuable prevention and intervention strategies, including federally mandated programs emphasizing prosocial behavior, that could decrease rates of SA revictimization within college populations. Thus, the first aim of the present study was to explore whether the previously identified relationship between pre-college SA and college-onset SA within this sample (as described in Conley et al.43) was moderated by perceived social support. It was hypothesized that social support would moderate the relationship between pre-college SA and college-onset victimization, such that higher levels of social support would weaken the relationship between pre-college SA and college-onset SA. The second aim of the study was to determine if perceived social support mediated the relationship between pre-college SA and college-onset SA, given that SA has been shown to affect social support through mechanisms such as increased blame and decreased assertiveness, which may, in turn, increase the likelihood for revictimization. It was hypothesized that social support would partially mediate the relationship between pre-college SA and college-onset SA.
METHODS
Participants
The present study utilizes data from the Spit for Science study (S4S), an ongoing university-wide research project, which longitudinally assesses genetic and environmental influences on substance use and psychiatric disorders in a representative majority of college students throughout their enrollment at a large urban university. Data was analyzed from the first three cohorts of S4S. Between 2011–2013, all incoming freshman age 18 or older were invited to participate in a university-wide research study on college behavioral health. First, summer mailings were sent to incoming freshmen, including a study overview of the survey and DNA collection components of the study. Mailings also included general information about alcohol-related programming at VCU. Second, at the start of the Fall semester, incoming freshmen were contacted via e-mail to invite them to participate by completing the online survey. Additional e-mail invitations were sent in the spring to freshmen that did not participate the previous fall, thereby providing another opportunity to complete the survey. In this case, participants were asked to retrospectively report on the items from the fall survey. Follow-up surveys were administered each spring following enrollment. Once enrolled in the S4S study, participants became part of the S4S registry, wherein they were de-identified using established study procedures. Participants in the S4S registry have all provided informed consent allowing for their data to be collected, shared and used for research purposes.
Invitations were sent to 11,328 individuals, with a 67% response rate. Notably, pre-college social support was not assessed retrospectively during the initial time point for individuals enrolling in the study during the spring semester. Therefore, only individuals enrolled during the fall semester were included in the present analyses (N=6,132). Given that previous research using S4S data (e.g., Conley et al.44) has demonstrated high rates (around 20%) of SA, as well as a positive association between pre-college SA and college-onset SA, we sought to extend these findings to include potential factors that may explain this previously identified association. Additionally, the sample was representative of the broader university student population in terms of both gender and race/ethnicity. The university’s Institutional Review Board approved all study procedures and informed consent was obtained from all study participants. Study data were collected and managed using REDCap (Research Electronic Data Capture), a secure web-based application designed exclusively to support data capture for research studies45. Participants received $10 and a t-shirt for their involvement in the study. Additional detailed information concerning recruitment can be found in Dick et al.46
Measures
Pre-College SA (Baseline Assessment)
SA exposure was assessed via an abbreviated version of the Life Events Checklist47. Two items were used to form the dichotomous pre-college ‘broad SA’ variable: “sexual assault (rape, attempted rape, made to perform any type of sexual act through force or threat of harm)” and “other unwanted or uncomfortable sexual experience”. Participants completing the survey in the fall or retrospectively in the spring of their first year were given the response options of “yes” or “no” regarding whether SA occurred “before the past 12 months”, “during the past 12 months”, “before starting college”, or “never happened to me”.
College-onset SA (Follow-up Assessments)
Students completing follow-up assessments were given the same response options as those offered during baseline assessment (“yes” or “no”) but were asked to respond to whether SA had occurred “since starting college” in the follow-up survey conducted spring of their first year and “in the past 12 months” in follow-up surveys completed each subsequent spring. Total number of SAs and total number of other unwanted or uncomfortable sexual experiences since college enrollment were computed and then totaled to create a ‘college-onset broad SA’ variable.
Social Support (Baseline Assessment)
Social support was evaluated via three items from the modified version of the Medical Outcomes Study module48. Items asked about the past 12 months and included “How often was someone available to give good advice about a crisis?”, “How often was someone available to get together with you for relaxation?”, and “How often was someone available to confide in or talk about your problems?”. Responses were made on a Likert-type scale of 1 (none of the time) to 4 (all of the time), with higher scores representing greater perceived social support. The current study utilized a sum score of the three items (Cronbach’s alpha=.84).
Data Analytic Plan
To address Aim 1, the PLUM procedure in SPSS was used to evaluate the hypothesized moderating effect of perceived social support on the relation between pre-college SA and college-onset victimization. The PLUM procedure was used because college-onset victimization was treated as an ordinal outcome variable, coded as 0–3 (0 = no SAs, 1= 1 SA, 2= 2 SAs, 3 = 3+ SAs. Pre-college SA was a dichotomous variable indicating presence or absence of pre-college SA. Prior to the analyses, the independent and moderator variables were centered and a product term was created from the centered variables49 to facilitate interpretation of the moderation results. Because there is no hierarchical function for the PLUM procedure, individual regressions were conducted in a hierarchical fashion. Gender and race were entered in the first regression predicting college-onset victimization. Pre-college SA and the centered social support variable were entered in the second regression. Lastly, the interaction term was added in the final regression. Models were compared by taking the difference between their −2 log likelihoods (−2LLs) and using this as the test statistic in a Chi square test with 1 df.
A weighted least squared mean and variance adjusted (WLSMV) mediation model (see Figure 1 for a theoretical path diagram of the model) was also tested, using Mplus, Version 6.1250. This model examined the effect of pre-college SA on college-onset victimization, both directly and indirectly through social support. Covariates consisted of gender and race and were included at the level of the full regression model (pre-college SA and social support predicting college-onset victimization). Mplus uses the product of coefficients strategy to calculate indirect effects51,52. In the simple case, partial mediation by a single variable (i.e., a partial indirect effect) is evaluated in relation to the Z-distribution.
Figure 1.
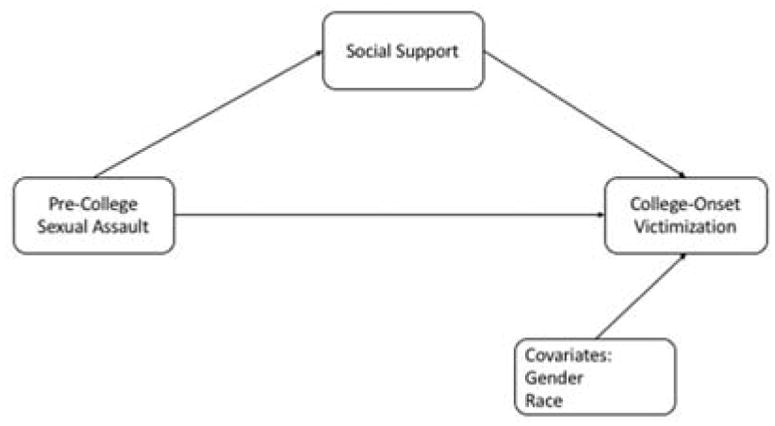
Mediation model
RESULTS
Sample characteristics
6132 participants from the first three Fall cohorts were included in the present analyses (Mage=18.42, SD=.47; 61.6% female). Race/ethnicity was dummy coded and separated into three categories with White (51.5%) set as the reference group. 19% of participants were African American, 16% were Asian, and 13.5% were grouped into the ‘Other’ category which included American Indian/Native Alaskan, Hispanic/Latino, Native Hawaiian/Other Pacific Islander, more than one race, and unknown.
Pre-college SA (i.e., experiencing at least one SA and/or other unwanted or uncomfortable sexual experience prior to college enrollment) was reported by 23.4% of the sample with females endorsing significantly higher rates compared to males (30.4% of females vs. 12.0% of males, X2=259.26, p<.001). 20.8% of the sample endorsed college-onset SA (14.4% endorsed one SA, 4.9% endorsed two SAs, and 1.5% endorsed 3 SAs). Of those who endorsed college-onset SA, 52.3% reported first time assaults, while 47.7% reported revictimization.
Perceived social support was highest across the total sample (M=9.56, SD=2.24), lower for individuals endorsing any “other unwanted or uncomfortable sexual experience” (M=9.17, SD=2.31), and lowest for individuals endorsing sexual assault (M=9.03, SD=2.37).
Moderation models
Results of the hierarchical ordinal logistic regressions conducted to evaluate the hypothesized influence of social support on the relation between pre-college SA and college-onset victimization are shown in Table 1. In the first model (Model 1; demographics only, see row 2 of the table), gender and Asian race significantly predicted college-onset victimization (ps <0.05), such that Asian race was associated with decreased risk of college-onset SA and female sex was associated with increased risk of college-onset SA. The predictive effect of African American race on college-onset victimization was marginally significant (p=.056), with a trend suggesting that African American race was associated with decreased risk of college-onset SA. “Other” race was not a significant predictor (p>.05). The same pattern was seen for these demographic parameters across all subsequent models, with African American race becoming significantly predictive in Models 2 and 3 (p<.05). The protective effects associated with Asian and African American race are likely related to the decreased rates of heavy drinking that have been seen in these groups compared to White individuals within the S4S sample53. In Model 2 (see row 3 of Table 1), pre-college SA significantly predicted increased risk of college-onset victimization (p<.001). Social support was also significantly associated with lower risk for college-onset SA (p<.001). Model 2’s fit was significantly better than Model 1’s (Δ−2LL = 819.21, p<.001), which, along with the greater pseudo R2 in Model 2 (14% vs. 4.3%), suggests that Model 2 has more explanatory power. In the final model (Model 3; includes the interaction term, see Row 4 of Table 1) testing moderation, the joint effect of pre-college SA and social support was not significant (p=0.187), suggesting that social support does not moderate the relationship between pre-college SA and college-onset victimization.
Table 1.
Results of hierarchical logistic regressions to examine the moderating effect of pre-college sexual assault and social support on college-onset victimization.
| Variable | Estimate (B) | 95% CI | Pseudo R2 | −2LL | Δ−2LL | p |
|---|---|---|---|---|---|---|
|
| ||||||
| Model 1 | .043 | 133.97 | ||||
| Gender | .898 | (.727, 1.070) | ||||
| Race | ||||||
| AA | −.184 | (−.372, .004) | ||||
| Asian | −.586 | (−.815, −.357) | ||||
| Other | −.204 | (−.428, .020) | ||||
|
| ||||||
| Model 2 | .140 | 953.18 | 819.21 | .000 | ||
| Gender | .637 | (.446, .828) | ||||
| Race | ||||||
| AA | −.223 | (−.443, −.020) | ||||
| Asian | −.473 | (−.723, −.223) | ||||
| Other | −.235 | (−.480, .009) | ||||
| Pre-College SA | 1.375 | (1.207, 1.544) | ||||
| Social Support | −.118 | (−.153, −.082) | ||||
|
| ||||||
| Model 3 | .141 | 951.45 | 1.73 | .188 | ||
| Gender | .638 | (.448, .829) | ||||
| Race | ||||||
| AA | −.238 | (−.450, −.026) | ||||
| Asian | −.472 | (−.722, −.222) | ||||
| Other | −.242 | (−.487, .003) | ||||
| Pre-College SA | 1.357 | (1.186, 1.528) | ||||
| Social Support | −.099 | (−.144, −.053) | ||||
| Pre-College SA*Social Support | −.048 | (−.120, .023) | ||||
NOTE: African American is notated as AA and sexual assault is notated as SA.
Mediation model
Similar to the moderation model, gender and Asian race significantly predicted college-onset victimization (ps <0.05). African American and “other” race did not significantly predict college-onset victimization (ps>.05). A mediation analysis determined that there was a small but significant indirect effect of pre-college SA on college-onset victimization through social support, β=.048, p<.001. This accounted for 5.8% of the total effect, with the remainder of the effect (~94%) resulting from pre-college SA’s direct association with college-onset victimization (p<.001).
COMMENT
The aims of the present study were to examine the mediating and moderating effects of perceived social support on the association between pre-college SA and college-onset SA. Consistent with previous research using the S4S sample (Conley et al.43), pre-college SA significantly predicted college-onset SA. This finding is consistent with a preponderance of literature suggesting that prior history of sexual assault is a strong predictor of subsequent sexual assaults9, particularly among college samples11,12. Indeed, approximately half of individuals who reported college-onset SA also reported prior SA. Social support was found to be a significant mediator, but not moderator, of the relationship between pre-college SA and college-onset SA; each result is discussed in turn.
In line with our hypothesis, social support accounted for a small, but meaningful amount of the total effect of pre-college SA on college-onset SA. Thus, social support may serve as a mechanism through which pre-college SA predicts college-onset victimization. There are numerous possible pathways by which this relationship may develop posited here that may warrant empirical attention. For example, because social support was inversely associated with college-onset SA, one way in which social support might serve as a mechanism through which pre-college SA predicts college-onset SA is explained by the social support deterioration theory, whereby stressful life events curtail actual or perceived social support54. SA often results in survivors feeling isolated and/or neglected socially, which may result in increases of behaviors that may put someone at increased risk for SA (e.g., substance use55, loneliness, displaced blame56). For instance, individuals having experienced SA prior to college may be less likely to seek out and establish adequate social support systems upon entering college. Such individuals, therefore, may be more prone to isolation and engagement in risky behaviors (e.g., substance use), a combination that may put them at significantly increased risk for SA (e.g., being intoxicated without the buffer of a “buddy system” to ensure that they are safe). The social support deterioration theory adds to the growing traction that social support has been getting as a marker of resilience, such that individuals with higher levels of social support may be less likely to be exposed to repeated traumas that, in turn, put them at even greater risk for PTSD and post-trauma difficulties20.
Another theory which may help explain the mediating role of social support on the relation between pre-college and college-onset SA is the tension-reduction theory, which suggests that SA survivors may use risky sexual behavior (RSB) as a means of regulating negative affect57,58. Without adequate social support systems in place post-SA, individuals may be more likely to likely to engage in risky tension-reducing behaviors, such that they are without more adaptive tension-reducing strategies (e.g., engagement in social support) and unmonitored by friends. RSB could then, in turn, increase the risk of another assault. Although previous research has demonstrated associations between correlates of social support (e.g., self-blame, lack of assertiveness, substance use) and repeated SA33,35,36,59, this is the first study to our knowledge to demonstrate a mediating effect of social support on the relation between pre-college and college-onset SA. These findings implicate an essential role of social support in the occurrence of college-onset SA, particularly among individuals at increased risk (i.e., those with a history of SA prior to starting college).
Future directions for this line of research include investigation into which specific components of social support are most influential in predicting college-onset SA among individuals with a prior history of SA. For example, determining whether emotional versus instrumental social support is more beneficial for reducing the likelihood of college-onset SA would allow for tailored intervention and prevention strategies on college campuses. Additionally, studies examining college social support may inform interventions that bolster social support systems already in place among many college students. For instance, research has demonstrated that how a support provider responds to SA disclosure has important implications for the process of recovery60–62. Therefore, education provision across campuses for how to respond when a friend discloses SA could help decrease blaming reactions and increase emotionally supportive reactions, which could not only have a positive effect on post-SA adjustment, but could also serve to potentially decrease the likelihood of repeated SA.
Another potential aspect of social support to target is prosocial bystander behavior, defined by Darley and Latane63 as a process whereby a prosocial bystander notices what is happening and labels it as a problem where help is needed, decides what actions to take, and feels they have the skills to take action safely. SA prevention programs focused on prosocial bystander behavior are becoming more prevalent [e.g. Bringing in the Bystander64, The Men’s Program65, and Mentors in Violence Prevention (MVP)66]. Although evaluations of these programs are promising67, more research is needed to better understand efficacy and applicability across various collegiate populations and settings. For example, while Hanson & Gidycz68 found their program decreased SA among women with no history of SA, it was not effective for those who had already been victimized. However, the findings were not replicated in subsequent studies69,70. Research on a pro-social bystander approach to SA prevention typically focuses on evaluating the short and long-term impact of such programs on bystander attitudes and behaviors39,71. Future research should examine the impact that increased pro-social bystander capacity has on perceived social support. As campus communities continue to be educated and trained in bystander prevention programs, if survivors of SA experience heighted support perhaps such programs will aid in the prevention of revictimization of this vulnerable group.
Limitations
Although the present study sample is robust and representative of the larger university population, several methodological limitations should be considered. Although significant, the mediating effect of social support on college-onset SA was small. Additionally, the assessment measures used were not tailored to these specific study aims (e.g., social support was assessed using only three items; although these three items demonstrated good internal reliability [α=.84]). Moreover, there are timing issues that ought to be considered when interpreting the results of the present study. For instance, given the longitudinal nature of data collection for the parent study, there is potential overlap in the fall administration between the responses “in the past twelve months” and “before starting college.” Therefore, it is possible that a participant who experienced SA during their initial days of college was erroneously coded as pre-college onset rather than college-onset SA. Similarly, social support was queried only at baseline for “past 12 months”; thus, the timing of pre-college SA in relation to social support assessment is unknown.
Additionally, psychiatric symptoms were not included in the present analyses. Thus, the potential confounding effects of PTSD, depression, anxiety, and substance use were not accounted for in the present analyses and, notably, may contribute to the mediating effect of social support on future revictimization. Moreover, although longitudinal assessment provides an approximate idea as to timing of trauma, exact timing of assaults was not specifically assessed and time elapsed since trauma and between traumas is not accounted for. Notably, whereas the extensive use of college students in psychological research is typically a concern with regards to generalizability of findings to the general population, the use of college students in the proposed study is a strength, as college undergraduates embody the general population of interest for the research questions of interest (i.e., young adults are at greater risk for SA and related outcomes). Moreover, seeing as the present study sample has been recruited from a large, urban university setting, participants are likely representative of the general college population in terms of both gender and race/ethnicity. However, by using a collegiate sample, the representativeness of other variables, such as socioeconomic status and education will be less applicable to non-college populations. Additionally, given that transgender individuals are at increased risk for SA revictimization22, future studies would benefit from targeted recruitment of gender nonconforming individuals. Findings should be considered in light of these limitations.
Conclusions
Despite these limitations, results from the present study further contribute to the existing literature, which suggests that social support influences SA revictimization (e.g., 36,72). This sample provides an apt picture of SA within a college population; one which is particularly relevant to study with regards to SA, as it is composed of the age group (i.e., 16–25 year-olds) demonstrated to be at highest risk for interpersonal (e.g., sexual/physical assault) trauma exposure73,74 and SA victimization and revictimization74,75. The present findings have important theoretical and practical applications. The strong predictive nature of SA exposure on future revictimization, coupled with the strongly evidenced relationship between SA revictimization and psychopathology10, supports the need for interventions for individuals who have experienced sexually assaultive violence. Additionally, high rates of pre-college and college-onset SA impels the need for colleges to adopt a trauma-informed approach to curricula, campus initiatives, social life, etc. Implementing intervention strategies that target known mediators of this relationship could reduce rates of revictimization and, in turn, subsequent mental health issues. Interventions that increase levels of social support, particularly in the context of prosocial bystander behavior, following an SA could reduce the predictive likelihood that revictimization would occur.
Footnotes
Author Contributions
Spit for Science: The Student Survey has been supported by P20 AA107828, R37AA011408, K02AA018755, K02 AA023239, and P50 AA022537 from the National Institute on Alcohol Abuse and Alcoholism, and UL1RR031990 from the National Center for Research Resources and National Institutes of Health Roadmap for Medical Research. We would like to thank the Spit for Science students for making this study a success, as well as the many faculty, students, and staff who contributed to the design and implementation of the project. All authors approved the final version of the manuscript for submission.
References
- 1.New J. Justice Department: 1 in 5 women sexually assaulted in college. 2016 https://www.insidehighered.com/quicktakes/2016/01/21/justice-department-1-5-women-sexually-assaulted-college.
- 2.Krebs CP, Lindquist CH, Warner TD, Fisher BS, Martin SL. College women’s experiences with physically forced, alcohol-or other drug-enabled, and drug-facilitated sexual assault before and since entering college. J Am Coll Health. 2009;57(6):639–649. doi: 10.3200/JACH.57.6.639-649. [DOI] [PubMed] [Google Scholar]
- 3.Cantalupo NC. Campus violence: Understanding the extraordinary through the ordinary. 2009. [Google Scholar]
- 4.Muehlenhard CL, Peterson ZD, Humphreys TP, Jozkowski KN. Evaluating the One-in-Five Statistic: Women’s Risk of Sexual Assault While in College. The Journal of Sex Research. 2017;54(4–5):549–576. doi: 10.1080/00224499.2017.1295014. [DOI] [PubMed] [Google Scholar]
- 5.Association ACH. National College Health Assessment II: Reference Group Executive Summary. Hanover, MD: American College Health Association; Fall. 2013. [Google Scholar]
- 6.Mirghassemi FL, Scott KA, Lundberg-Love PK, Phelps H, Burke AL. Ramifications of Title IX on Campus Sexual Assault Prevention and Treatment Protocol: Will Recent Changes Work to Protect College Students? Campus Action Against Sexual Assault: Needs, Policies, Procedures, and Training Programs: Needs, Policies, Procedures, and Training Programs. 2016:163. [Google Scholar]
- 7.Wolitzky-Taylor K, Resnick HS, Amstadter AB, McCauley JL, Ruggiero KJ, Kilpatrick DG. Reporting Rape in a National Sample of College Women. The Journal of American College Health. 2011;59(7):582–587. doi: 10.1080/07448481.2010.515634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yung CR. Concealing campus sexual assault: An empirical examination. Psychology, public policy, and law. 2015;21(1):1. [Google Scholar]
- 9.Messman-Moore TL, Long PJ. The role of childhood sexual abuse sequelae in the sexual revictimization of women: An empirical review and theoretical reformulation. Clinical Psychology Review. 2003;23:537–571. doi: 10.1016/s0272-7358(02)00203-9. [DOI] [PubMed] [Google Scholar]
- 10.Classen CC, Palesh OG, Aggarwal R. Sexual revictimization: A review of the empirical literature. Trauma, Violence, & Abuse. 2005;6(2):103–129. doi: 10.1177/1524838005275087. [DOI] [PubMed] [Google Scholar]
- 11.Messman-Moore TL, Ward RM, Zerubavel N. The role of substance use and emotion dysregulation in predicting risk for incapacitated sexual revictimization in women: results of a prospective investigation. Psychology of addictive behaviors. 2013;27(1):125. doi: 10.1037/a0031073. [DOI] [PubMed] [Google Scholar]
- 12.Waldron JC, Wilson LC, Patriquin MA, Scarpa A. Sexual victimization history, depression, and task physiology as predictors of sexual revictimization: Results from a 6-month prospective pilot study. Journal of interpersonal violence. 2015;30(4):622–639. doi: 10.1177/0886260514535258. [DOI] [PubMed] [Google Scholar]
- 13.Cloitre M, Cohen LR, Scarvalone P. Understanding revictimization among Childhood Sexual Abuse survivors: An interpersonal schema approach. 2001. Unpublished manuscript. [Google Scholar]
- 14.Coid J, Petruckevitch A, Feder G, Chung W-S, Richardson J, Moorey S. Relation between childhood sexual and physical abuse and risk of revictimisation in women: a cross-sectional survey. The Lancet. 2001;358(9280):450–454. doi: 10.1016/s0140-6736(01)05622-7. [DOI] [PubMed] [Google Scholar]
- 15.Chu AT, DePrince AP, Mauss IB. Exploring revictimization risk in a community sample of sexual assault survivors. Journal of Trauma & Dissociation. 2014;15(3):319–331. doi: 10.1080/15299732.2013.853723. [DOI] [PubMed] [Google Scholar]
- 16.Ullman SE, Vasquez AL. Mediators of sexual revictimization risk in adult sexual assault victims. Journal of child sexual abuse. 2015;24(3):300–314. doi: 10.1080/10538712.2015.1006748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Arata CM. Child sexual abuse and sexual revictimization. Clinical Psychology: Science and Practice. 2002;9:135–164. [Google Scholar]
- 18.Janssen I, Krabbendam L, Bak M, et al. Childhood abuse as a risk factor for psychotic experiences. Acta Psychiatrica Scandinavica. 2004;109(1):38–45. doi: 10.1046/j.0001-690x.2003.00217.x. [DOI] [PubMed] [Google Scholar]
- 19.Kaltman S, Krupnick J, Stockton P, Hooper L, Green BL. Psychological impact of types of sexual trauma among college women. Journal of Traumatic Stress. 2005;18(5):547–555. doi: 10.1002/jts.20063. [DOI] [PubMed] [Google Scholar]
- 20.Kaysen D, Rosen G, Bowman M, Resick PA. Duration of exposure and the dose-response model of PTSD. Journal of Interpersonal Violence. 2010;25(1):63–74. doi: 10.1177/0886260508329131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shih RA, Schell TL, Hambarsoomian K, Belzberg H, Marshall GN. Prevalence of posttraumatic stress disorder and major depression after trauma center hospitalization. J Trauma. 2010;69(6):1560–1566. doi: 10.1097/TA.0b013e3181e59c05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nemoto T, Bödeker B, Iwamoto M. Social support, exposure to violence and transphobia, and correlates of depression among male-to-female transgender women with a history of sex work. Am J Public Health. 2011;101(10):1980–1988. doi: 10.2105/AJPH.2010.197285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Perrin M, Vandeleur CL, Castelao E, et al. Determinants of the development of post-traumatic stress disorder, in the general population. Social psychiatry and psychiatric epidemiology. 2014;49(3):447–457. doi: 10.1007/s00127-013-0762-3. [DOI] [PubMed] [Google Scholar]
- 24.Balsam KF, Lehavot K, Beadnell B. Sexual revictimization and mental health: A comparison of lesbians, gay men, and heterosexual women. Journal of Interpersonal Violence. 2011;26(9):1798–1814. doi: 10.1177/0886260510372946. [DOI] [PubMed] [Google Scholar]
- 25.Han SC, Gallagher MW, Franz MR, Chen MS, Cabral FM, Marx BP. Childhood sexual abuse, alcohol use, and PTSD symptoms as predictors of adult sexual assault among lesbians and gay men. Journal of interpersonal violence. 2013;28(12):2505–2520. doi: 10.1177/0886260513479030. [DOI] [PubMed] [Google Scholar]
- 26.Carter SP, DiMauro J, Renshaw KD, Curby TW, Babson KA, Bonn-Miller MO. Longitudinal associations of friend-based social support and PTSD symptomatology during a cannabis cessation attempt. J Anxiety Disord. 2016;38:62–67. doi: 10.1016/j.janxdis.2016.01.008. [DOI] [PubMed] [Google Scholar]
- 27.Messman-Moore TL, Resick PA. Brief treatment of complicated PTSD and peritraumatic responses in a client with repeated sexual victimization. Cognitive and Behavioral Practice. 2002;9:89–99. [Google Scholar]
- 28.Kaniasty K. Social support and traumatic stress. PTSD research Quarterly. 2005;16(2):1–7. [Google Scholar]
- 29.Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychol Bull. 2003;129(1):52–73. doi: 10.1037/0033-2909.129.1.52. [DOI] [PubMed] [Google Scholar]
- 30.Evans SE, Steel AL, DiLillo D. Child maltreatment severity and adult trauma symptoms: Does perceived social support play a buffering role? Child abuse & neglect. 2013;37(11):934–943. doi: 10.1016/j.chiabu.2013.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Macy RJ, Nurius PS, Norris J. Responding in their best interests: Contextualizing women’s coping with acquaintance sexual aggression. Violence Against Women. 2006;12(5):478–500. doi: 10.1177/1077801206288104. [DOI] [PubMed] [Google Scholar]
- 32.Classen C, Field NP, Koopman C, Nevil-Manning K, Spiegel D. Interpersonal problems and their relationship to sexual revictimization among women sexually abused in childhood. Journal of Interpersonal Violence. 2001;16:495–509. [Google Scholar]
- 33.Livingston JA, Testa M, VanZile-Tamsen C. The reciprocal relationship between sexual victimization and sexual assertiveness. Violence Against Women. 2007;13(3):298–313. doi: 10.1177/1077801206297339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ullman S. Sexual Assault Disclosure, Social Reactions, And Problem Drinking In Women. Alcoholism: Clinical & Experimental Research. 2006;30(6):56A. [Google Scholar]
- 35.Ullman SE, Starzynski LL, Long SM, Mason GE, Long LM. Exploring the relationships of women’s sexual assault disclosure, social reactions, and problem drinking. Journal of interpersonal violence. 2008;23(9):1235–1257. doi: 10.1177/0886260508314298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mason GE, Ullman S, Long SE, Long L, Starzynski L. Social support and risk of sexual assault revictimization. J Community Psychol. 2009;37(1):58–72. [Google Scholar]
- 37.Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology. 2000;68(5):748–766. doi: 10.1037//0022-006x.68.5.748. [DOI] [PubMed] [Google Scholar]
- 38.Banyard VL, Plante EG, Moynihan MM. Bystander education: Bringing a broader community perspective to sexual violence prevention. J Community Psychol. 2004;32(1):61–79. [Google Scholar]
- 39.McMahon S, Postmus JL, Koenick RA. Conceptualizing the engaging bystander approach to sexual violence prevention on college campuses. Journal of College Student Development. 2011;52(1):115–130. [Google Scholar]
- 40.Ullman SE. Social support and recovery from sexual assault: A review. Aggression and violent behavior. 1999;4(3):343–358. [Google Scholar]
- 41.Esposito CL, Clum GA. Social support and problem-solving as moderators of the relationship between childhood abuse and suicidality: Applications to a delinquent population. Journal of Traumatic Stress. 2002;15(2):137–146. doi: 10.1023/A:1014860024980. [DOI] [PubMed] [Google Scholar]
- 42.Hill TD, Kaplan LM, French MT, Johnson RJ. Victimization in early life and mental health in adulthood: An examination of the mediating and moderating influences of psychosocial resources. J Health Soc Behav. 2010;51(1):48–63. doi: 10.1177/0022146509361194. [DOI] [PubMed] [Google Scholar]
- 43.Conley A, Overstreet C, Hawn S, Kendler K, Dick D, Amstadter A. Prevalence and predictors of sexual assault among a college sample. J Am Coll Health. 2017;65(1):41–49. doi: 10.1080/07448481.2016.1235578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Conley AH, Overstreet CM, Hawn SE, Kendler KS, Dick DM, Amstadter AB. Prevalence and predictors of sexual assault among a college sample. J Am Coll Health. 2017;65(1):41–49. doi: 10.1080/07448481.2016.1235578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of biomedical informatics. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Dick DM, Nasim A, Edwards AC, et al. Spit for Science: launching a longitudinal study of genetic and environmental influences on substance use and emotional health at a large US university. Frontiers in genetics. 2014:5. doi: 10.3389/fgene.2014.00047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Gray MJ, Litz BT, Hsu JL, Lombardo TW. Psychometric properties of the life events checklist. Assessment. 2004;11(4):330–341. doi: 10.1177/1073191104269954. [DOI] [PubMed] [Google Scholar]
- 48.Sherbourne CD, Stewart AL. The MOS social support survey. Social Science and Medicine. 1991;32:705–714. doi: 10.1016/0277-9536(91)90150-b. [DOI] [PubMed] [Google Scholar]
- 49.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 50.Muthén L, Muthén B. Mplus statistical modeling software (Version 6.12) Los Angeles: Muthén & Muthén; 2011. [Google Scholar]
- 51.MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological methods. 2002;7(1):83. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior research methods, instruments, & computers. 2004;36(4):717–731. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- 53.Kendler KS, Edwards A, Myers J, Cho SB, Adkins A, Dick D. The predictive power of family history measures of alcohol and drug problems and internalizing disorders in a college population. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics. 2015;168(5):337–346. doi: 10.1002/ajmg.b.32320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Barrera M., Jr Distinctions between social support concepts, measures, and models. Am J Community Psychol. 1986;14(4):413–445. [Google Scholar]
- 55.Ullman SE, Relyea M, Peter-Hagene L, Vasquez AL. Trauma histories, substance use coping, PTSD, and problem substance use among sexual assault victims. Addict Behav. 2013;38(6):2219–2223. doi: 10.1016/j.addbeh.2013.01.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Tharp AT, DeGue S, Valle LA, Brookmeyer KA, Massetti GM, Matjasko JL. A systematic qualitative review of risk and protective factors for sexual violence perpetration. Trauma, Violence, & Abuse. 2013;14(2):133–167. doi: 10.1177/1524838012470031. [DOI] [PubMed] [Google Scholar]
- 57.Batten SV, Follette VM, Aban IB. Experiential avoidance and high-risk sexual behavior in survivors of child sexual abuse. Journal of Child Sexual Abuse. 2001;10:101–120. doi: 10.1300/j070v10n02_06. [DOI] [PubMed] [Google Scholar]
- 58.Filipas HH, Ullman SE. Child sexual abuse, coping responses, self-blame, posttraumatic stress disorder, and adult sexual revictimization. Journal of Interpersonal Violence. 2006;21(5):652–672. doi: 10.1177/0886260506286879. [DOI] [PubMed] [Google Scholar]
- 59.Ullman S. Correlates and consequences of adult sexual assault disclosure. Journal of Interpersonal Violence. 1996;11(4):554–571. [Google Scholar]
- 60.Orchowski LM, Untied AS, Gidycz CA. Social reactions to disclosure of sexual victimization and adjustment among survivors of sexual assault. Journal of interpersonal violence. 2013;28(10):2005–2023. doi: 10.1177/0886260512471085. [DOI] [PubMed] [Google Scholar]
- 61.Littleton HL. The impact of social support and negative disclosure reactions on sexual assault victims: A cross-sectional and longitudinal investigation. Journal of Trauma & Dissociation. 2010;11(2):210–227. doi: 10.1080/15299730903502946. [DOI] [PubMed] [Google Scholar]
- 62.Jacques-Tiura AJ, Tkatch R, Abbey A, Wegner R. Disclosure of sexual assault: Characteristics and implications for posttraumatic stress symptoms among African American and Caucasian survivors. Journal of Trauma & Dissociation. 2010;11(2):174–192. doi: 10.1080/15299730903502938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Darley JM, Latane B. Bystander intervention in emergencies: diffusion of responsibility. Journal of personality and social psychology. 1968;8(4p1):377. doi: 10.1037/h0025589. [DOI] [PubMed] [Google Scholar]
- 64.Banyard VL, Moynihan MM, Plante EG. Sexual violence prevention through bystander education: An experimental evaluation. J Community Psychol. 2007;35(4):463–481. [Google Scholar]
- 65.Foubert JD. The men’s program: How to successfully lower men’s likelihood of raping. 2000. [Google Scholar]
- 66.Katz J. Mentors in violence prevention: history and overview. 2007;30:2007. Retrieved November. [Google Scholar]
- 67.Lonsway KA, Banyard VL, Berkowitz AD, et al. Rape prevention and risk reduction: Review of the research literature for practitioners. VAWnet. 2009 [Google Scholar]
- 68.Hanson KA, Gidycz CA. Evaluation of a sexual assault prevention program. Journal of Consulting and Clinical Psychology. 1993;61:1046–1052. doi: 10.1037//0022-006x.61.6.1046. [DOI] [PubMed] [Google Scholar]
- 69.Breitenbecher KH, Gidycz CA. An empirical evaluation of a program designed to reduce the risk of multiple sexual victimization. Journal of Interpersonal Violence. 1998;13(4):472–488. [Google Scholar]
- 70.Breitenbecher KH, Scarce M. A longitudinal evaluation of the effectiveness of a sexual assault education program. Journal of Interpersonal Violence. 1999;14:459–478. [Google Scholar]
- 71.Banyard V, Moynihan M, Cares A, Warner R. How do we know if it works? Defining measurable outcomes in bystander-focused violence prevention. Psychology of Violence. 2013 [Google Scholar]
- 72.Messman-Moore TL, Long PJ. Alcohol and substance use disorders as predictors of child to adult sexual revictimization in a sample of community women. Violence Vict. 2002;17:319–340. doi: 10.1891/vivi.17.3.319.33662. [DOI] [PubMed] [Google Scholar]
- 73.Breslau N, Kessler R, Chilcoat HD, Schultz LR, Davis GC, Andreski P. Trauma and posttraumatic stress disorder in the community: The 1996 Detroit area survey of trauma. Archives of General Psychiatry. 1998;55:626–632. doi: 10.1001/archpsyc.55.7.626. [DOI] [PubMed] [Google Scholar]
- 74.Benjet C, Bromet E, Karam E, et al. The epidemiology of traumatic event exposure worldwide: results from the World Mental Health Survey Consortium. Psychological medicine. 2016;46(2):327–343. doi: 10.1017/S0033291715001981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Brener ND, McMahon PM, Warren CW, Douglas KA. Forced sexual intercourse and associated health-risk behaviors among female college students in the United States. Journal of consulting and clinical psychology. 1999;67(2):252. doi: 10.1037//0022-006x.67.2.252. [DOI] [PubMed] [Google Scholar]