

Abstract
The use of digital tools offers a new perspective to daily clinical activities. The digital information serves as a starting point for a wax-up and intraoral mock-up, which is widely reported in literature as an objective and efficient communication tool among dentist, patient, and technician. This case report of a maxillary anterior rehabilitation demonstrates esthetic planning with the digital smile design (DSD) system and a direct mock-up technique. After preoperative photographs were obtained, digital planning was created using DSD. However, due to differences in virtual simulation, a direct mock-up with composite resin was performed. Porcelain laminate veneers using feldspathic ceramics were used to restore the anterior teeth. Many times, the DSD simulation is not enough for the patient to understand and observe the changes that will be performed on the anterior teeth. This combination of techniques can offer predictability to results as well increasing the patient expectation satisfaction.
Keywords: Ceramic, digital smile design, esthetics, mock-up, veneer
INTRODUCTION
A beautiful smile and harmonic facial esthetics are attributes that contribute to the well-being of any patient. Smile esthetics are related to the form, texture, color, and alignment of the anterior teeth as well as to intraoral soft tissues, lips, and facial esthetics.[1] An important objective of an esthetic treatment is that the final result should be as close as possible to the patient's expectations, improving his/her facial esthetics and smile.[1,2,3]
The digital smile design (DSD) is a digital planning tool for esthetic dentistry, in which the evaluation of the esthetic relationship among the teeth, gingiva, smile, and face is obtained through lines and digital drawings that are inserted on the facial and intraoral photographs of the patient. The use of digital tools offers dentists and technicians a new perspective for diagnosis and treatment plan, facilitating and improving the communication among dentist, technician, and patient.[1,2,4,5]
While DSD presents many advantages over more traditional treatment planning methods, the mock-up technique is still regarded as an objective and efficient tool in treatment planning communication[3,6] and used to confirm the treatment plan before the final preparations and evaluate final restorations within the limitations of biological and functional considerations.[6] The mock-up can also be a clinical confirmation of the digital tool. Based on the above considerations, the objective of this report is to demonstrate a clinical case where the anterior teeth were rehabilitated using DSD and the direct mock-up technique for esthetic and functional treatment planning.
CASE REPORT
A 38-year-old male patient who was unhappy with his smile presented with lateral incisors out of proportion with the central incisors. His main wish was to improve the esthetic appearance of his maxillary incisors.
During the clinical examination, the facial aspects, the smile harmony, the gingival contour, and the dental characteristics were evaluated. Two lines were placed in the center of the initial page of the DSD program, making a cross, and the facial photograph was placed behind the lines [Figure 1a]. The interpupillary line was used as an initial reference to establish the horizontal plane. Next, the midfacial line was projected based on the facial characteristics such as glabella, nose, and chin. The purpose of this initial tracing was to find the best facial position relative to the horizon while determining the midfacial line with no interference from the dental position, angle, or midline. For clinical smile design, the overall proportion of the patient's face was assessed, and then, the length of the upper lip at rest and in a smile was checked to determine the gingival display. It was established that crown lengthening was not necessary. After this preliminary facial analysis, the condition of teeth, parafunctional habits, oral hygiene, occlusal plane, interocclusal distance, and incisal edge were checked. The initial tracing (the cross) was transferred to the smile region, allowing the positioning of the smile [Figure 1b]. This overlapping allows a comparative analysis of the teeth and face. The relative proportions between teeth are important for smile esthetics and depend on the relationship between their length and width, as well on how teeth are arranged in the arch and the smile configuration. A commonly cited method to establish dental proportions is the golden proportions.[7] Based on these proportion rules, it was possible to prepare simulations to improve the positioning of the teeth and their proportion for the ideal smile. The dental contour was defined according to the lower lip proportions and the anteroposterior curvature of the teeth. After finishing the drawings [Figure 1c], it was observed that it would not be possible to obtain smile harmony following exactly the anteroposterior reference line of the teeth. To find an adequate proportion, the length of the incisal edges was decreased [Figure 1d]. At the initial planning, an increase of 1.8–1.9 mm of the incisal third length was proposed. However, this much incisal lengthening was judged to be excessive and incompatible with the width-to-height ratio of 0.75–0.78 for the maxillary anterior teeth.[8] Therefore, it was decided to reposition the incisal border of the central incisors to the same level as the maxillary canines, resulting in an incisal length of 1 mm for the maxillary central incisors. Due to the differences in the virtual simulation (DSD), a mock-up was proposed with composite resin to improve the communication between the clinician and the technician and to facilitate the visualization of the final result by the patient. Many times, the DSD simulation is not enough for the patient to understand and observe the changes that will be performed on the anterior teeth.
Figure 1.
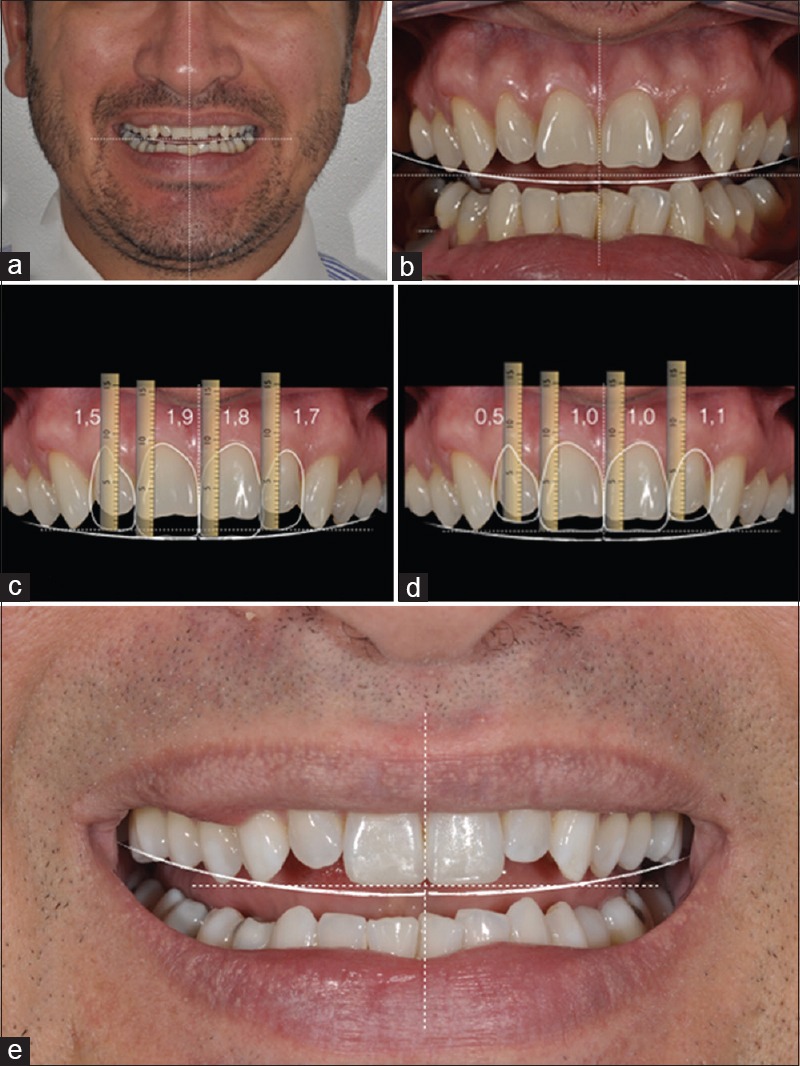
Facial photograph was placed behind crossing lines, for initial digital smile design planning (a) Intraoral photograph showing the positioning of the smile, based on the crossing lines (b) Virtual simulation with digital smile design (c) Alteration of the planning proposed initially by the digital smile design (d) direct mock-up (e)
Using the diagnostic wax-up as a reference [Figure 2a], a silicone guide was prepared (Zetalabor, Zhermack, Badia Polesine [RO], Italy) to make the mock-up with bis-acryl resin (Protemp, 3M ESPE, Seefeld, Germany) [Figure 2b and c]. After the functional evaluation, such as anterior and lateral disclusion and effect on phonetics, esthetic evaluation was also performed (smile, positioning of the lower lip, and harmony of the new teeth design). Then, it was observed that adequate lateral guidance, with canine function occlusion, occurred at the superior and inferior canines. Porcelain veneers requiring minimal tooth preparation were proposed for teeth #s 7, 8, 9, and 10, using refractory porcelain (creation). Initially, horizontal slots in the region of the middle and cervical third with the spherical diamond tips (1014 and 1012, KG Sorensen, Cotia, São Paulo, BR) were performed with a 45°. Following this, the preparation was completed with a cylindrical diamond burr (2135, KG Sorensen, Cotia, São Paulo, BR). The polishing of the preparation was done with sequential disks (Sof-Lex, 3M ESPE, Seefeld, Germany) and polishing rubber points (Exa-Intrapol Edenta AG, Heidelberg, Switzerland).
Figure 2.
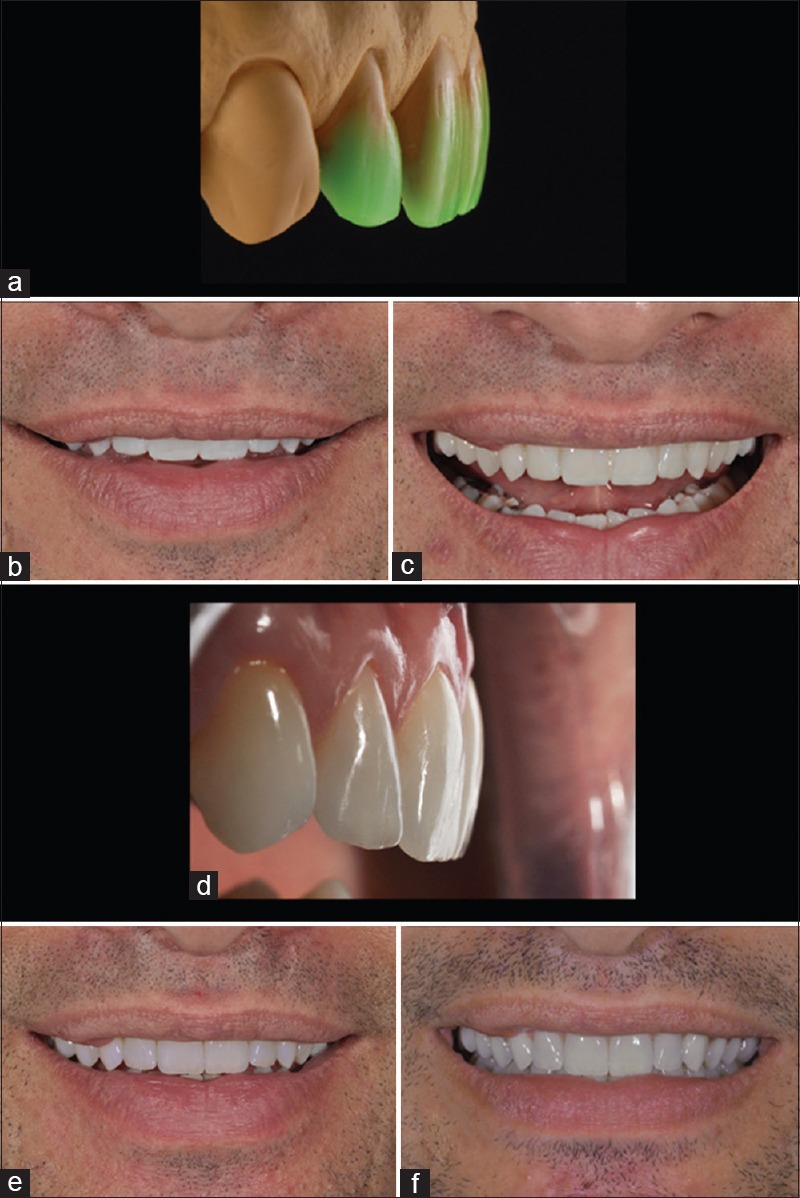
Diagnostic wax-up of teeth #7–10 (a) Front view of the mock-up with bis-acryl resin (b) Front view of the mock-up with bis-acryl resin, patient with forced smile (c) Side view of the feldspathic porcelain veneers in their position (d) Finished case (e) Follow-up after 12 months (f)
A retraction cord was inserted and a silicone addition impression was performed (Futura, Nova DFL, Rio de Janeiro, Brazil) with the double-step technique. The color selection was made with Vita classical shade guide (A2, A1, B1, and B2), followed by digital photographs. After the preparation of the ceramic veneers, they were tried using a try-in paste (Ivoclar Vivadent, AG, Schaan, Liechtenstein). The restorations were conditioned with 10% hydrofluoric acid (Condac Porcelana 10% FGM, Joinville, SC, Brazil) for 90 s, washed with air/water jet, and conditioned with 37% phosphoric acid (Condac 37 FGM, Joinville, SC, Brazil) for 60 s for the removal of the residues resulting from the first acid conditioning and then dried. Silane coupling agent (Monobond Plus, Ivoclar Vivadent AG) was applied for 60 s and dried.
Before bonding, the restorations were tried in to determine the correct luting shade with try-in pastes. A modified rubber dam technique was performed for isolation. The teeth were cleaned with pumice and water, etched with 37% phosphoric acid (Condac 37 FGM) for 30 s, washed, and dried. A simplified adhesive system was applied (Excite F DSC, Ivoclar Vivadent AG) without photoactivation. The light-cured resin cement (color 0, Variolink Veneer, Ivoclar Vivadent AG) was applied to each veneer, which was carefully positioned on the preparations. The cement excess was removed with brush and dental floss, followed by photoactivation (Bluephase N, Ivoclar Vivadent AG) for 40 s on each side.
The final result immediately after cementation can be seen in Figure 2d, in which it is possible to observe that the esthetic parameters were established satisfying the expectations of the patient. Afterward, the patient was instructed on oral hygiene and was informed about the probability of stains appearing on the cementation line. The patient was called for periodical control. Figure 2f shows that in the 12-month follow-up, there was no alteration in color, shape, or gingival tissue. At the end of the rehabilitation, the patient was stable without any parafunctional habits and as such did not require an occlusal guard [Figure 2e and 2f].
DISCUSSION
It is important to highlight that spending more time in the diagnosis and planning phase helps to improve treatment predictability and execution efficacy. Improving predictability will support earlier identification of complementary treatments such as orthodontic movement[9] and clinic crown increase.[9,10] Besides, it diminishes clinical errors and frustration by inadequate patient and clinician communication. With the objective of obtaining esthetic and functional rehabilitation, every professional looks for improvement in planning and better predictability support for the clinical treatment.
The use of digital tools such as DSD offers dentists a new perspective when combined with the traditional mock-up technique, showing a bigger success rate in relation to the final results. The combination of DSD and mock-up techniques allows for improved esthetic manipulation, therefore, a better predictable model to support the treatment plan.[11] Digital imaging allows patients to visualize the expected final result, besides facilitating the presentation of the current condition of his oral health.[9,12,13]
DSD is also a powerful marketing tool.[1,2,4] However, correct digital planning requires a precise photography protocol. The photography obtained following this protocol supplies important information for the esthetic planning. Inadequate photography may distort the reference image and may result in an incorrect diagnosis and planning.[10] Despite studies that show a satisfactory clinical result,[1,2,4,10] this tool should be used cautiously due to these limitations in this protocol.[4] Even though DSD is a simple technique with minimum software and equipment requirements, training is necessary which increases time and cost.[1]
In addition, a powerful tool commonly used to support digital treatment planning is the mock-up technique; as it gives the patient and dentist, a tridimensional visualization of the final result of the proposed treatment is one of its big advantages.[2,10,14] While in the diagnostic wax-up, one can only see the desired shape for the teeth, the mock-up allows the visualization of the shape integrated to the gingiva, lips, face, and phonetics,[15] during the evaluation period.[3] As such, the patient may evaluate, provide opinion, and approve the final shape of the new smile before any irreversible procedures are performed such as dental wearing.
The mock-up is considered a fast, easy, and efficient tool for the diagnosis and planning of rehabilitating esthetic treatments. This technique should be used as a routine protocol by the clinician since it permits the professional to work with higher predictability of results and smaller margin of error in more complex cases.[13,15] The mock-up must also be seen as a marketing tool to help the patient accept the proposed treatment, because one technique complements the other,[14] as in the case presented here.
After every technology barrier toward the future is transposed, new technologies appear to human benefit and sometimes can change the common paradigm on clinical protocols and best techniques. Important to mention that vanguard fronts such as this may be scarce in references until more related important work is developed. Combining traditional and new techniques such as mock-up and DSD as presented in this article will collaborate to reduce the number of intraoral adjustments[12] as well as avoid unnecessary tooth wear.[9,13] The unnecessary tooth preparation can lead to undesired factors such as improved tooth sensibility, dentin exposure, and unnecessary enamel wearing that can negatively influence on reducing the short- and long-term clinical success as part of the restoration treatment.
CONCLUSION
DSD utilizes photographic information to create an esthetic treatment protocol, and then, the intraoral mock-up serves as confirmation and demonstration of the final porcelain veneer restorations. The combination of DSD and mock-up for diagnosis and treatment planning has positive results in the esthetic rehabilitation of the anterior teeth. When used in combination, these techniques offer predictable results and highly satisfactory results.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Meereis CT, de Souza GB, Albino LG, Ogliari FA, Piva E, Lima GS, et al. Digital smile design for computer-assisted esthetic rehabilitation: Two-year follow-up. Oper Dent. 2016;41:E13–22. doi: 10.2341/14-350-S. [DOI] [PubMed] [Google Scholar]
- 2.Miranda ME, Olivieri KA, Rigolin FJ, de Vasconcellos AA. Esthetic challenges in rehabilitating the anterior maxilla: A Case report. Oper Dent. 2016;41:2–7. doi: 10.2341/14-269-S. [DOI] [PubMed] [Google Scholar]
- 3.Reshad M, Cascione D, Magne P. Diagnostic mock-ups as an objective tool for predictable outcomes with porcelain laminate veneers in esthetically demanding patients: A clinical report. J Prosthet Dent. 2008;99:333–9. doi: 10.1016/S0022-3913(08)00056-5. [DOI] [PubMed] [Google Scholar]
- 4.Lin WS, Zandinejad A, Metz MJ, Harris BT, Morton D. Predictable restorative work flow for computer-aided design/computer-aided manufacture-fabricated ceramic veneers utilizing a virtual smile design principle. Oper Dent. 2015;40:357–63. doi: 10.2341/13-295-S. [DOI] [PubMed] [Google Scholar]
- 5.Cooper LF, Culp L, Luedin N. A digital approach to improved overdentures for the adolescent oligodontia patient. J Esthet Restor Dent. 2016;28:144–56. doi: 10.1111/jerd.12217. [DOI] [PubMed] [Google Scholar]
- 6.Gürel G. Porcelain laminate veneers: Minimal tooth preparation by design. Dent Clin North Am. 2007;51:419–31, ix. doi: 10.1016/j.cden.2007.03.007. [DOI] [PubMed] [Google Scholar]
- 7.Al Taki A, Hamdan AM, Mustafa Z, Hassan M, Abu-Alhuda S. Smiles esthetics: Impact of variations in the vertical and horizontal dimensions of the maxillary lateral incisors. Eur J Dent. 2017;11:514–20. doi: 10.4103/ejd.ejd_351_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rosenstiel SF, Ward DH, Rashid RG. Dentists' preferences of anterior tooth proportion – A web-based study. J Prosthodont. 2000;9:123–36. [PubMed] [Google Scholar]
- 9.Sancho-Puchades M, Fehmer V, Hämmerle C, Sailer I. Advanced smile diagnostics using CAD/CAM mock-ups. Int J Esthet Dent. 2015;10:374–91. [PubMed] [Google Scholar]
- 10.Zanardi PR, Laia Rocha Zanardi R, Chaib Stegun R, Sesma N, Costa BN, Cruz Laganá D, et al. The use of the digital smile design concept as an auxiliary tool in aesthetic rehabilitation: A Case report. Open Dent J. 2016;10:28–34. doi: 10.2174/1874210601610010028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cattoni F, Mastrangelo F, Gherlone EF, Gastaldi G. A new total digital smile planning technique (3D-DSP) to fabricate CAD-CAM mockups for esthetic crowns and veneers. Int J Dent. 2016;2016:6282587. doi: 10.1155/2016/6282587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Coachman C, Paravina RD. Digitally enhanced esthetic dentistry – From treatment planning to quality control. J Esthet Restor Dent. 2016;28(Suppl 1):S3–4. doi: 10.1111/jerd.12205. [DOI] [PubMed] [Google Scholar]
- 13.Pimentel W, Teixeira ML, Costa PP, Jorge MZ, Tiossi R. Predictable outcomes with porcelain laminate veneers: A Clinical report. J Prosthodont. 2016;25:335–40. doi: 10.1111/jopr.12413. [DOI] [PubMed] [Google Scholar]
- 14.Neto AF, Bandeira AS, de Miranda BF, Sánchez-Ayala A. The use of mock-up in dentistry: Working with predictability. Full Dent Sci. 2015;6:256–60. [Google Scholar]
- 15.Magne P, Magne M. Use of additive waxup and direct intraoral mock-up for enamel preservation with porcelain laminate veneers. Eur J Esthet Dent. 2006;1:10–9. [PubMed] [Google Scholar]