

Abstract
Choroid metastasis from esophageal carcinoma is rare; reports addressing the effectiveness of treatment strategies are limited. We report a case of a 51-year-old man with metastatic esophageal carcinoma who had a 1-month history of blurred vision in his left eye. An ophthalmologic examination revealed a choroidal mass in his left eye. Adjuvant chemotherapy with cisplatin and 5-fluorouracil was initiated; however, visual acuity did not improve. External beam radiotherapy (EBRT) was initiated, resulting in near complete regression of the mass. EBRT is an effective therapeutic modality and should be considered in patients with choroidal metastasis of esophageal carcinoma.
Keywords: Choroidal metastasis, esophageal carcinoma, radiotherapy
Malignant choroidal tumors are rare, and most of them are metastatic tumors from distant organs. Esophageal carcinoma metastasis to the orbit and eyeball has been reported; however, choroidal metastasis from esophageal carcinoma is extremely rare. An English literature search revealed only seven cases that have been reported so far.[1,2,3,4,5,6,7] To our knowledge, this is the first reported case of esophageal squamous cell carcinoma with choroidal metastasis that was treated with external beam radiotherapy (EBRT) successfully.
Case Report
A 51-year-old Asian man with alcoholic liver cirrhosis presented to our emergency department initially with upper gastrointestinal bleeding. Esophagogastroduodenoscopy revealed a mass lesion over the upper middle segment of his esophagus [Fig. 1]. An esophageal biopsy specimen revealed esophageal squamous cell carcinoma, poorly differentiated type (cT2N2M1; PD-L1:10%). Contrast-enhanced computed tomography of the chest revealed mediastinal lymph node metastases and lung metastasis. The patient also had hematuria, and cystoscopy revealed a tumor over the posterior wall of the bladder; biopsy results were consistent with the esophageal biopsy results. Skeletal scintigraphy showed the presence of multiple bone metastases. Due to the patient's underlying condition of decompensated liver cirrhosis, he was treated initially with palliative radiation therapy to the esophageal cancer primary site only.
Figure 1.

Esophagogastroduodenoscopy showed a mass lesion over the upper middle segment of esophagus
One month later, he presented with blurred vision in his left eye. Ophthalmologic examination revealed visual acuity of 20/320 in the left eye and 20/25 in the right eye. Intraocular pressure was 10 mmHg in the left eye and 8 mmHg in the right eye. Fundus examination of the left eye revealed a submacular large yellowish-white mass. Ultrasonography of the left eye demonstrated a huge choroidal mass with moderate-to-high internal reflectivity at the superior temporal area [Fig. 2a]. Optical coherence tomography (OCT) examination of the left eye showed a large elevated choroidal mass with shallow subretinal fluid [Fig. 2b]. Fluorescein angiography (FA) displayed hyperfluorescence in the late venous phase with dye staining in the left eye [Fig. 2c].
Figure 2.
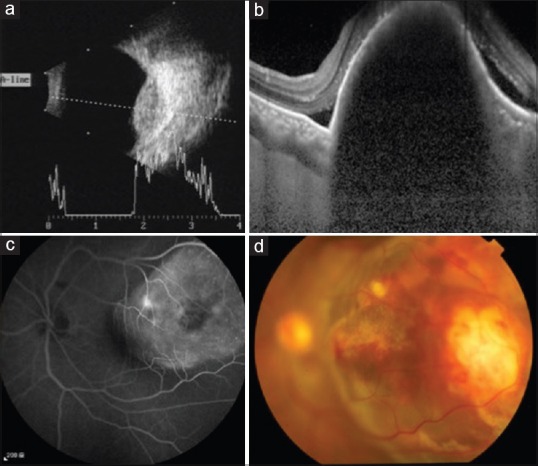
(a) Fundus color photography of the left eye revealed a submacular large yellowish-white mass with hemorrhage (b) Fluorescein angiography displayed hyperfluorescence in late venous phase with dye staining in the left eye mass. (c) Optical coherence tomography of the left eye showed a large elevated choroidal mass with shallow subretinal fluid. (d) B-scan ultrasonography showed a huge mass found at the superior temporal area. A scan shows a 100% spike along with moderate-to-high internal acoustic reflectivity of the choroidal mass
Our impression was that the esophageal squamous cell carcinoma metastasized the choroid. Due to multiple metastases, we administered two cycles of chemotherapy with cisplatin and 5-fluorouracil as adjuvant chemotherapy. However, his disease still progressed and his vision did not improve. A fundus examination of the left eye revealed an increase in size of the choroidal mass with inferior retinal detachment [Fig. 2d]. The patient then received external beam irradiation with 60 Gy over 30 fractions to the left eye for visual restoration. After 6 weeks of treatment, his visual acuity improved from 20/320 to 20/100 in the left eye. Fundus examination revealed marked regression of the tumor when compared with the images taken before initiating treatment [Fig. 3].
Figure 3.
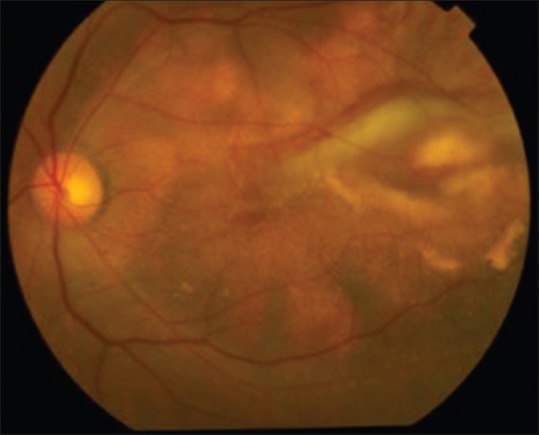
Fundus examination of the left eye after 6 weeks of external beam irradiation showed marked regression of tumor
Although the choroidal metastatic tumor showed signs of regression, his disease progressed, and metastasis to his whole body including the brain, lung, liver, skin, lymph nodes, bladder, bone, and peritoneum was revealed. He is now being treated with nivolumab and is still alive since his initial diagnosis 13 months ago.
Discussion
In a large analysis of 520 eyes with metastatic disease, cancers of the gastrointestinal tract were the primary source of metastasis in 19 (4%) eyes.[8] The most common site of metastasis in the eye is the choroid. The reason that the eye is a metastatic target is uncertain, though it has been proposed that the rich vascularity of the choroid may be a possible etiology for choroid metastasis. The symptoms of choroid metastasis are blurred vision (70%–81%), flashes and floaters (5%–12%), and pain (5%–14%).[9]
The diagnosis of choroid metastasis requires imaging studies, such as ultrasonography, OCT, FA, and orbital CT. Magnetic resonance imaging often shows a well-demarcated choroidal mass that appears isointense on T1-weighted images and hypointense on T2-weighted images. The differential diagnosis of choroidal metastases includes choroidal melanoma, hemangioma, granuloma, osteoma, and choroidal neovascularization.[9]
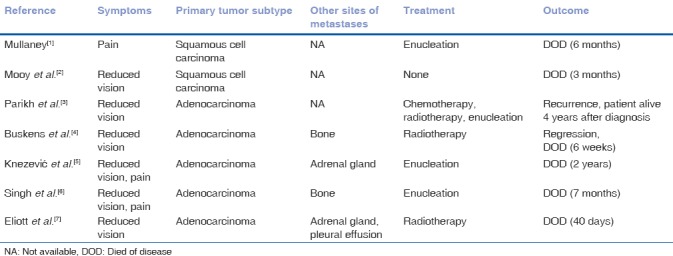
Patients with choroid metastasis have a mean expected life span of 9 months. The prognosis is very poor for patients with choroid metastasis despite multiple treatment modalities.[10] Between 1970 and 2017, a total of seven case reports regarding choroidal metastasis of esophageal carcinoma have been reported.[1,2,3,4,5,6,7] The range of duration between diagnosis of choroidal metastasis and death was 40 days to 2 years; only one patient was reported to be alive after 4 years [Table 1].
Table 1.
Characteristics of patients with choroid metastasis from esophagus cancer in the reported studies
Systemic chemotherapy should be considered as adjuvant therapy for those with multiple metastases as seen in our patient. The choice of drug and its effectiveness of chemotherapy for choroidal metastasis depends on the type of primary cancer. However, choroidal metastasis from esophageal carcinoma seems to be resistant to chemotherapy.[9]
Lemoine and McLeod reported the first successful treatment of eye metastasis with radiotherapy from breast cancer. Almost all patients with choroid metastasis received EBRT. The prescription dose ranged from 30 Gy to 50 Gy. Generally, tumor regression occurs in 85%–93% of patients, and vision improvement or stabilization is found in 56% of eyes.[10] The common complications of EBRT include dry eye, keratitis, cataracts, and radiation retinopathy.[10] Of the seven patients that we reviewed,[1,2,3,4,5,6,7] three patients who were diagnosed with adenocarcinoma had undergone radiotherapy, and only one patient showed regression in choroidal metastasis [Table 1]. After external beam radiation, our patient had no major side effects except for mild eye pain; his visual acuity also improved. Orbital CT revealed almost complete regression of the choroidal mass lesion. The patient showed a relatively good response to radiotherapy.
Conclusion
Radiotherapy is an effective therapy for choroidal metastasis. Effective control of these choroidal lesions may improve the patient's quality of life and help to prevent blindness in the patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mullaney J. Squamous cell carcinoma of the oesophagus with choroidal metastasis. Br J Ophthalmol. 1970;54:281–3. doi: 10.1136/bjo.54.4.281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mooy CM, de Jong PT, Verbeek AM. Choroidal metastasis of oesophageal squamous cell carcinoma. Int Ophthalmol. 1990;14:63–71. doi: 10.1007/BF00154203. [DOI] [PubMed] [Google Scholar]
- 3.Parikh HK, Deshpande RK, Swaroop DV, Desai PB. Choroidal metastasis from primary adenocarcinoma of the esophagus. J Surg Oncol. 1993;52:68–70. doi: 10.1002/jso.2930520118. [DOI] [PubMed] [Google Scholar]
- 4.Buskens CJ, Tan HS, Hulscher JB, de Smet MD, van Lanschot JJ. Adenocarcinoma of the esophagus with choroidal metastasis. Dis Esophagus. 2001;14:70–2. doi: 10.1111/j.1442-2050.2001.00154.x. [DOI] [PubMed] [Google Scholar]
- 5.Knezević J, Radovanović N, Simić A, Bobić Radovanović A, Latković Z, Micev M, et al. Isolated choroidal metastasis from primary adenocarcinoma of the distal esophagus: A case report. Dis Esophagus. 2003;16:41–3. doi: 10.1046/j.1442-2050.2003.00279.x. [DOI] [PubMed] [Google Scholar]
- 6.Singh D, Sharma A, Arora B, Shukla NK, Mohanti BK. Adenocarcinoma esophagus with choroid metastasis. Indian J Gastroenterol. 2004;23:112–3. [PubMed] [Google Scholar]
- 7.Eliott D, Salehi-Had H, Plous OZ. Adenocarcinoma of the esophagus presenting as choroidal metastasis. Dis Esophagus. 2011;24:E16–8. doi: 10.1111/j.1442-2050.2010.01170.x. [DOI] [PubMed] [Google Scholar]
- 8.Arepalli S, Kaliki S, Shields CL. Choroidal metastases: Origin, features, and therapy. Indian J Ophthalmol. 2015;63:122–7. doi: 10.4103/0301-4738.154380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology. 1997;104:1265–76. doi: 10.1016/s0161-6420(97)30148-1. [DOI] [PubMed] [Google Scholar]
- 10.Rudoler SB, Corn BW, Shields CL, De Potter P, Hyslop T, Shields JA, et al. External beam irradiation for choroid metastases: Identification of factors predisposing to long-term sequelae. Int J Radiat Oncol Biol Phys. 1997;38:251–6. doi: 10.1016/s0360-3016(97)00050-3. [DOI] [PubMed] [Google Scholar]