

Abstract
Introduction
Anxiety and depression are often comorbid conditions, but there is uncertainty as to how this comorbidity develops. Thus, in three studies, we attempted to discern whether anhedonia may be a key linking factor between anxiety and depression.
Methods
Three studies asked participants about their symptoms of anxiety and depression: in Study 1, 109 participants completed measures of anxiety, depression, activity avoidance, and perceived enjoyability and importance of avoided activities; in Study 2, 747 participants completed measures of anhedonia, anxiety, depression, and defensiveness; in Study 3, 216 participants completed measures assessing the same constructs as in Study 2 at four time-points (ranging 11 months in span).
Results
In Study 1, symptoms of anxiety and depression were only positively related in individuals who relinquished potential enjoyment due to their anxiety-related avoidance; in Study 2, the indirect effect of anhedonia helped explained how anxiety symptoms imparted risk onto depressive symptoms; and in Study 3, anxiety led to anhedonia and then depression over time and anhedonia led to anxiety and then depression at both 5 and 11 months.
Limitations
The manuscript is limited by the use of a student sample in study 2, cross-sectional methods in studies 1 and 2, and reliance on self-ratings in studies 2 and 3.
Conclusions
Anxiety may devolve into depression through anhedonia, such that anxious individuals begin to lose pleasure in anxiety-provoking activities, which results in the development of other depressive symptoms.
Keywords: depressive, anxious, loss of interest, loss of pleasure, longitudinal, comorbidity
Symptoms of anxiety can predate symptoms of depression (Batterham et al., 2013; Belzer and Schneider, 2004; Frewen et al., 2012; Mineka et al., 1998). For example, in a recent longitudinal study in a youth population (Price et al., 2016), anxiety symptoms such as threat avoidance were predictive of depression scores two years later. Evidence also suggests that anxiety is a stronger predictor of depression among participants who perceive anxiety as having a causal effect on depression (Frewen et al., 2013). However, the mechanisms by which symptoms of anxiety transition to symptoms of depression are still unknown.
One candidate variable that may link anxiety and depression is anhedonia (Cramer et al., 2010). Anhedonia may be considered a stable personality trait or a change that indicates increased psychopathology (Loas, 2014; Thomsen, 2015; Winer et al., 2014b). Increases in anhedonia may be uniquely associated with other symptoms of depression, as they have been found to predict suicidality and severe depressive symptoms (Winer et al., 2016c; Winer et al., 2014a). Moreover, anhedonia could indicate the start of a process of reward devaluation (Winer and Salem, 2016); that is, a downward pattern of avoiding positivity associated with other depressogenic biases and poor outcomes (Bartoszek and Winer, 2015; Carvalho and Hopko, 2011; Winer et al., 2011).
Thus, there is need to further understand how and when anhedonia unfolds in anxious individuals and whether that results in other symptoms of depression. In three studies, we evaluated (1) whether specific types of anxiety-related avoidance associated with anhedonia covaried with symptoms of depression; (2) whether specific patterns of anxiety were associated with depression indirectly through anhedonia; and (3) whether anxiety was predictive of depression through anhedonia over approximately 5 months and 11 months. Our main hypotheses were that anxiety, and anhedonia resulting from anxiety-related avoidance, would be predictive of symptoms of depression (Jacobson and Newman, 2014), and that anhedonia would mediate this unfolding relationship.
Study 1
Initially, we examined how anhedonia resulting from anxiety-driven avoidant behavior links anxiety and depression. Functional analysis predicts that avoidance may result in loss of positive reinforcement (Ferster, 1973). However, not all avoidant behavior results in lost enjoyability. Thus, we examined whether the degree of enjoyability relinquishment resulting from avoidance affected the strength of the relationship between anxiety and depression.
We hypothesized that among anxious individuals with high enjoyability relinquishment due to avoidance, anxiety levels would be strongly predictive of depression, whereas among anxious individuals with low enjoyability relinquishment due to avoidance, anxiety would not be associated with depression. We wished to test whether relinquishment of enjoyability would be a discriminant moderator of anxiety and depression by comparing it to other aspects of avoided activities.
Method
Participants
Participants (N = 109) with Beck Anxiety Inventory (BAI) scores of 16 or above were recruited via Amazon’s Mechanical Turk (MTurk) website (each had at least 80% approval rates). Five participants (4.5%) who provided nonsensical responses to open-ended questions were removed. The sample consisted of 65 women and 39 men between 19 and 60 years old (M = 31.54; SD = 9.47). This study was reviewed by the University of Illinois at Chicago Institutional Review Board and all participants provided informed consent.
Materials and Measures
Depression and anxiety symptoms were assessed using the Beck Anxiety Inventory (BAI) and the Beck Depression Inventory II (BDI-II). Both the BDI-II and BAI have acceptable psychometric properties (Beck and Steer, 1990; Beck et al., 1996) and consist of 21 items each answered on a 4-point Likert scale.
Four questions (representing potential moderators) inquired about avoidance-driven relinquishment of enjoyable/interesting or important activities. Specifically, the questions assessed the percentage of (enjoyable or important) activities avoided and the enjoyability or importance of these activities and were rated on a 5-point Likert scale ranging from very slightly to extremely.
Procedure
The study was programmed on Qualtrics software and distributed on MTurk, which produces reliable responses on clinical measures (Chandler and Shapiro, 2016; Shapiro et al., 2013). Participants were pre-screened via the BAI and paid $0.05. Those with BAI scores above 15 were offered participation in the main study for an additional $0.60. Subsequently, participants answered questions related to avoidance-driven lack of enjoyability. They then completed the BDI among other questionnaires included for future analyses, provided basic demographic information, and were debriefed.
Statistical Analyses
The moderation and mediation hypotheses were tested using PROCESS models 1 and 4, respectively (Hayes, 2013). PROCESS constructed 1,000 bootstrapped samples yielding 95% confidence intervals estimating the size of each model’s effects; anxiety was entered as the predictor, depression as the outcome, and moderators or mediators were entered as described below. Participants’ responses about the overall frequency of engagement in enjoyable activities and enjoyability of these activities were covariates in all analyses.
Results
See Table 1 for descriptive and correlational statistics. The relationship between anxiety and depression was not moderated by the mere percentage of enjoyable/interesting activities that were avoided, ΔR2 = .004, F(1, 98) = 0.44, p = .51. However, as expected, the relation of depression and anxiety was moderated by the prospective enjoyability of avoided activities (i.e., enjoyability relinquished as a result of avoidance), ΔR2 = .033, F(1, 98) = 4.48, p = .04 (Figure 1). Anxiety was strongly associated with depression when avoided activities were considered to be highly enjoyable, b = .60, 95% CI [0.26, 0.95], t = 3.45, p = .001, but anxiety and depression were not associated when avoided activities were not enjoyable, b = .05, 95% CI [−0.31, 0.42], t = 0.30, p = .77.
Table 1.
Descriptive Statistics and Zero-Order Correlations among Predictor (BAI), Outcome (BDI), and the Four Moderator Variables
| M | SD | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|
| 1. BAI | 27.85 | 9.20 | |||||
| 2. BDI | 29.02 | 12.32 | .26** | ||||
| 3. %ENJavoid | 51.11 | 25.45 | .29** | .21* | |||
| 4. Enjoyability Relinquished | 3.90 | 0.89 | .11 | .21* | .29** | ||
| 5. %IMPavoid | 52.66 | 25.51 | .26** | .14 | .63*** | .24* | |
| 6. Importance Relinquished | 3.97 | 0.95 | −.05 | .10 | .19† | .50*** | .27** |
Note. BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; %ENJavoid = Percentage of Enjoyable Activities Avoided; %IMPavoid = Percentage of Important Activities Avoided.
p < .10.
p < .05.
p < .01.
p < .001.
Figure 1.
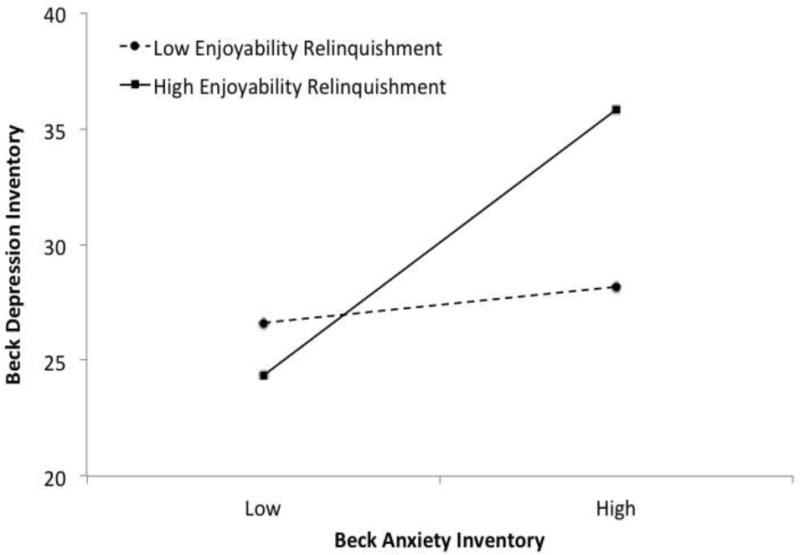
Simple slopes between symptoms of depression and anxiety at low and high levels of enjoyability of avoided activities (i.e., enjoyability relinquishment).
Conversely, the avoided activities that were considered important did not moderate the relationship between anxiety and depression whether the percentage of important activities avoided, ΔR2 = .002, F(1, 98) = 0.20, p = .65, or the magnitude of importance of these activities, ΔR2 = .002, F(1, 98) = 0.27, p = .61, was taken into account. We also conducted a comparison mediation analysis consistent with previous findings that general avoidant behavior mediates the relationship between anxiety and depression (Jacobson and Newman, 2014; Moitra et al., 2008). We found that the enjoyability of avoided activities did not mediate the relationship between anxiety and depression. Examination of correlations between the variables showed that although enjoyability of avoided activities correlated with the outcome variable (BDI-II scores: r = 21, p < .05), they did not correlate with the predictor (BAI scores: r = 11, ns). Thus, the lack of mediation may have been primarily due to the negligible relationship between enjoyability of avoided activities and anxiety.
Discussion
Level of prospective enjoyment relinquished due to anxiety-driven avoidance moderated the relationship between anxiety and depression. Specifically, highly anxious individuals who experienced a high level of relinquished enjoyment due to their behavioral avoidance also evidenced an increase in depressive symptoms. However, it should be noted that the effect size of this relationship was small (3.3% of the total variance). The percentage of enjoyable activities avoided, and the importance of the avoided activities, did not moderate the relationship between anxiety and depression. Thus, it is only when avoided activities are considered highly enjoyable (i.e., relinquished enjoyability is high) that anxiety becomes linked with depression.
Study 2
Consistent with Study 1, we wanted to examine what particular aspects of anxiety were associated with anhedonia and depression, and whether we might begin to identify a mediational model (anxiety ➔ anhedonia ➔ depression) for future longitudinal investigation. One candidate variable is defensiveness, which is supported by a wide range of previous findings as a moderator of anxiety (Myers et al., 2008; Weinberger, 1990). Individuals with elevated anxiety but non-elevated defensiveness display patterns of responding more intuitively associated with anxious response styles than do individuals with both elevated anxiety and elevated defensiveness (Brosschot et al., 1999; Myers et al., 2008; Winer et al., 2011). Given that the findings of Study 1 indicate that only anxiety related to relinquishment of pleasure was associated with depression, we hypothesized that only anxiety not associated with defensive response styles would be cross-sectionally associated with depression indirectly through anhedonia in a moderated mediation model. Most importantly, we also hypothesized that the relationship between anxiety and depression would be indirectly explained by anhedonia.
Method
Participants and Procedure
Participants (N = 747) completed measures online as part of a larger study (Nadorff et al., 2014; Winer et al., 2016a; Winer et al., 2016c) in exchange for course credit. Participants who completed all questionnaires (N=652) were included, and the sample consisted of 43% males and 57% females, ages 18–22 (M = 18.9, SD = 1.43). This study was reviewed by the Mississippi State University Institutional Review Board and all participants provided informed consent.
Measures
The Specific Loss of Interest and Pleasure Scale (SLIPS) measured recent changes in anhedonia. The SLIPS is a 23-item self-report measure with established psychometric properties (Winer et al., 2014b) measured on a four-point scale, with the highest choice of “3” indicating a trait level response. Responses of “3” (e.g., “I have never enjoyed going out with anyone”) are recoded as “0” to limit endorsement of trait responses and emphasize anhedonia associated with a potential emotional downturn, resulting in a range of 0–46.
Depression was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), a validated measure of depression. The CES-D is a 20-item self-report measure assessed along a four-point scale. To eliminate tautological overlap with anhedonia, items related to positive affect and happiness were removed.
Trait anxiety was assessed using the short form of the Taylor Manifest Anxiety Scale (MAS; Bendig, 1956). The MAS is a 20-item true/false measure of trait anxiety used commonly in research examining the interaction of anxiety and defensiveness (e.g., Winer et al., 2011).
Defensiveness was assessed with the 20-item shortened version of the Marlowe-Crowne Social Desirability Scale (MC; Strahan and Gerbasi, 1972). The MC is a commonly used validated true/false measure of defensive response style. An example item is “I’ve never intensely disliked anyone,” for which a response of “true” would indicate defensiveness.
Statistical Analyses
Cross-sectional moderated mediation was tested using PROCESS model 7 (Hayes, 2013). Anxiety was entered as predictor, defensiveness as moderator, anhedonia as mediator, and depression as the outcome. All variables were within acceptable limits of skewness and kurtosis (Kline, 2005).
Results
The overall model was significant, F(2, 649) = 417.03, p < .001, accounting for 56.25% of the total variance (Figure 2). Defensiveness moderated the relationship between anxiety and anhedonia, b = −.03, t = 2.00, p < .05. Furthermore, the index of moderated mediation was significant, b = −.0141, 95% CI [−.0312, −.0010], indicating that the indirect effect of anxiety on depression through anhedonia differed at varying levels of defensiveness.
Figure 2.
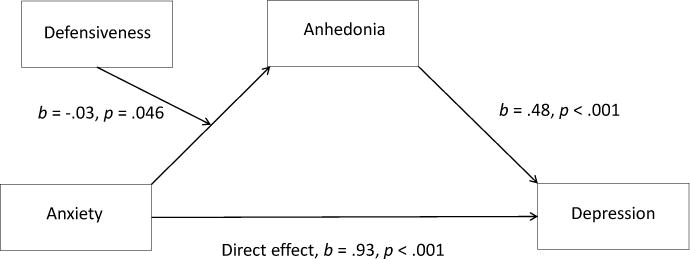
Study 2 moderated mediation model with anxiety as the independent variable, defensiveness as the moderator, anhedonia as the mediator, and depression as the outcome.
Probing the relationship between anxiety, anhedonia, and depression at different levels of defensiveness indicated that the cross-sectional mediational relationship between anxiety, anhedonia, and depression was strongest at low levels of defensiveness, b = .37, 95% CI [.27, .51] and weakest at high levels of defensiveness, b = .27, 95% CI [.19, .37]. However, the confidence intervals of each simple indirect effect overlapped, qualifying the moderation.
Discussion
Anxiety was associated with depression through the indirect effect of anhedonia. This relationship was strongest when defensiveness was low, although it remained significant when defensiveness was high. Taking Studies 1 and 2 together, anxiety was related to anhedonia or relinquishment of enjoyability, which was cross-sectionally related to depression. Two main questions remain unanswered regarding the direction of these relations, however.
First, because the cross-sectional mediation in Study 2 remained significant at high levels of defensiveness despite the significant index of moderated mediation, it is difficult to interpret the extent to which defensiveness is a robust moderator of anxiety in relation to anhedonia and depression. Defensive response styles may be valid indicators of unrealistic self-assessment of anxiety, or they could merely indicate participants who have not paid close attention, which would weaken the indirect effect in a non-psychologically-meaningful way.
Second, and most important, the preliminary mediational pattern established in Study 2 is one resting on atemporal associations (Winer et al., 2016a). That is, despite the intuitive possibility that symptoms of anxiety can lead to anhedonia, which can subsequently lead to symptoms of depression, assessing this possibility cross-sectionally does not inform whether this assumption is true over time (Judd et al., 2001).
Thus, it is necessary to examine (1) a different way to evaluate defensive or valid response styles to assess the veridicality of defensiveness as a moderator and, most importantly, (2) the temporal associations of anxiety, anhedonia, and depression.
Study 3
Study 3 examined the relationship between anxiety, anhedonia, and depression over time and included an additional check for valid responding. We hypothesized that we would again find that anxiety leads to anhedonia and subsequently depression. We evaluated two different temporal models, each incorporating three time-points, to include a built-in longitudinal replication. In Model 1, anxiety and defensiveness were assessed at time 1, anhedonia was assessed at time 2 (1–2 months after time 1), and depression was assessed at time 3 (1–3 months after time 2). Model 2 assessed the predictors and mediator at the same time-points, but examined depression at time 4 (6–9 months after time 3).
Method
Participants
Participants were at least 18 years of age and lived in the United States to be considered for participation. Only participants validly completing each questionnaire at each assessment were entered into analyses. Participants were paid between $1.00 and $3.00 per each wave, consistent with prior studies (Horton and Chilton, 2010; Shapiro et al., 2013). Valid-responding participants consenting to be re-contacted completed wave 1 (N=706), wave 2 (N=384), wave 3 (N=294), and wave 4 (N=216), resulting in data from 196 participants (138 female; Mage=41.54, range 18–75) for Model 1 and 165 participants (120 female; Mage=42.39, range 20–75) for Model 2. This study was reviewed by the Mississippi State University Institutional Review Board and all participants provided informed consent.
Procedure
The online data collection was collected using MTurk and Qualtrics as in Study 1 (with the exception of the methods described below). Data was collected as part of a large longitudinal study (Jordan, in press). Participants were re-contacted via their de-identified MTurk ID first using Python, then using R software, and the MTurkR package to ensure confidentiality (Leeper, 2014; Mueller and Chandler, 2012) and at least two researchers verified all longitudinal responses.
Validity Item
Participants received a validity question at the end of the battery of questionnaires consisting of the following instructions within a larger description of an emotion question: “So, in order to demonstrate that you have read the instructions, choose the ‘Other’ category and write ‘I’ve read the instructions’ in the text field. That is, ignore the question and emotion choices below.” Participants then had to select the answer choice “Other” then manually input “I’ve read the instructions” to respond validly.
Measures
All measures were the same as Study 2, with the exception of the measure of depression, which was assessed using the Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR). The QIDS-SR is a 16-item questionnaire assessing the nine main symptoms of depression along a four-point scale with established internal consistency and validity (Rush et al., 2006; Rush et al., 2003). Scores range from 0 to 27; as in Study 2, to eliminate tautological overlap with anhedonia, the ‘general interest’ item was removed from analyses.
Results
Analysis at 5 months
Moderated mediation was tested using PROCESS model 7 (Hayes, 2013) with the same parameters as in Study 2. The moderation model with anhedonia as the outcome variable was significant, F(3, 192) = 42.12, p < .001, accounting for 39.69% of the total variance (Figure 3). Also, the mediation model with depression as the outcome variable was significant, F(2, 193) = 126.31, p < .001, accounting for 56.69% of the total variance. Unlike in Study 2, however, defensiveness did not moderate the relationship between anxiety and anhedonia, b = −.02, t < 1, p = .40. Furthermore, the index of moderated mediation was not significant, b = −.004, 95% CI [−.0130, .0036], indicating that the indirect effect of anxiety on depression through anhedonia did not differ significantly at varying levels of defensiveness.
Figure 3.
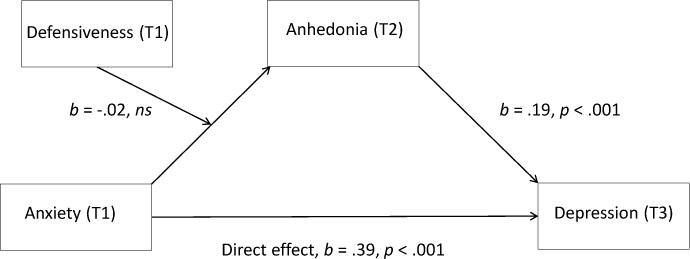
Study 3 moderated mediation model with anxiety as the independent variable (T1), defensiveness as the moderator (T1), anhedonia as the mediator (T2), and depression as the outcome (T3).
Because the moderated mediation model was not significant, we conducted a simple mediation model – model 4 of PROCESS – to examine the mediational relationship of anxiety and depression via anhedonia without the prospective moderator of defensiveness included in the model. Both the direct effect of anxiety at time 1, b = .39, t = 7.47, p < .001, and anhedonia at time 2, b = .19, t = 6.27, p <.001, significantly predicted depression at time 3 (Figure 4). Moreover, the indirect effect of anxiety on depression through anhedonia was significant, b = .21, 95% CI [.1247, .2876], indicating longitudinal mediation that partially explains this relationship.
Figure 4.
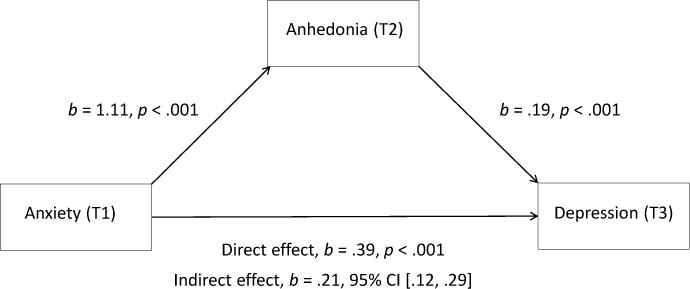
Study 3 mediation model with anxiety as the independent variable (T1), anhedonia as the mediator (T2), and depression as the outcome (T3).
We also ran a mediation model examining an alternative temporal path with anhedonia at time 1 and anxiety at time 2 (see figure 7). As with the initial model, the direct effect of anhedonia at time 1 on depression at time 3 was significant, b = .15, t = 5.73, p < .001, as well as the indirect effect, b = .16, 95% CI [.1192, .2086], suggesting that longitudinal mediation partially explains this relationship as well.
Figure 7.
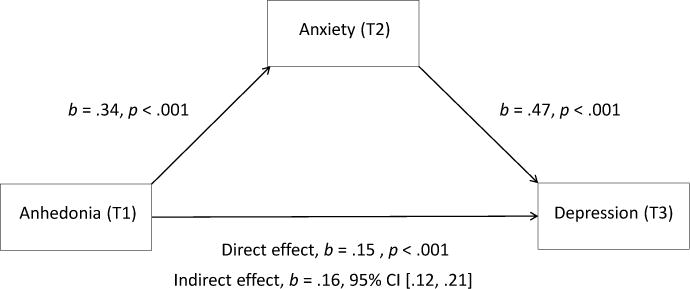
Study 3 alternative mediation model with anhedonia as the independent variable (T1), anxiety as the mediator (T2), and depression (T3) as the outcome.
Analysis at 11 months
Moderated mediation was again tested using PROCESS model 7, but with anxiety and defensiveness assessed at time 1, anhedonia assessed at time 2, and depression assessed at time 4 (collected approximately 11 months after time 1). The overall moderation model with anhedonia as the outcome variable was significant, F(3, 161) = 37.91, p < .001, accounting for 41.40% of the total variance (Figure 5). The overall mediation model was also significant, F(2, 162) = 74.95, p < .001, accounting for 48.06% of the total variance. As with Model 1, defensiveness did not moderate the relationship, b = −.03, t = −1.24, p = .22, and moderated mediation was not significant, b = −.004, 95% CI [−.0114, .0012].
Figure 5.
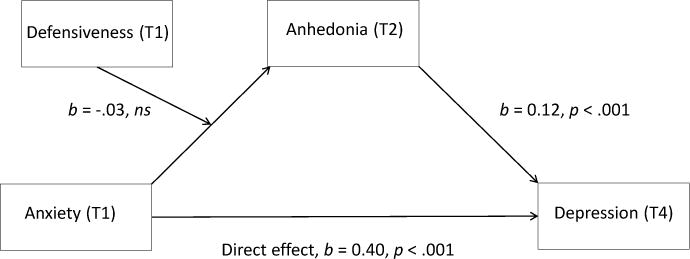
Study 3 moderated mediation model with anxiety as the independent variable (T1), defensiveness as the moderator (T1), anhedonia as the mediator (T2), and depression (T4) as the outcome.
In the simple mediation model, the direct effect of anxiety at time 1, b = .4022, t = 6.75, p < .001, and anhedonia at time 2, b = .1159, t = 3.55, p <.001, significantly predicted depression (Figure 6). Moreover, the indirect effect of anxiety on depression through anhedonia was significant, b = .1350, 95% CI [.0519, .2341], indicating longitudinal mediation partially explaining this relationship.
Figure 6.
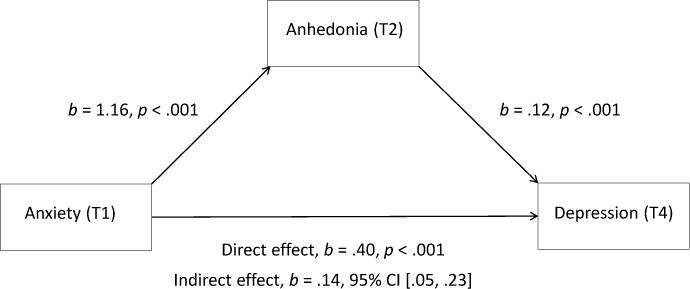
Study 3 mediation model with anxiety as the independent variable (T1), anhedonia as the mediator (T2), and depression (T4) as the outcome.
We also ran a mediation model examining the alternative temporal path with anhedonia at time 1 and anxiety at time 2 (see figure 8), with depression at time 4 as the outcome. Again, the direct effect of anhedonia at time 1 on depression at time 4 was significant, b = .09, t = 3.01, p < .01, as well as the indirect effect, b = .15, 95% CI [.1030, .2072], suggesting again that longitudinal mediation partially explains this relationship.
Figure 8.
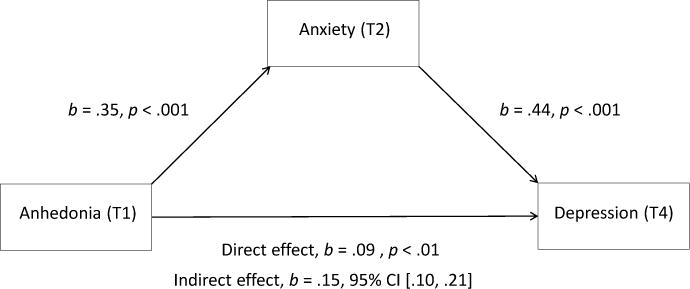
Study 3 alternative mediation model with anhedonia as the independent variable (T1), anxiety as the mediator (T2), and depression (T4) as the outcome.
Discussion
The mediational findings from Study 2 received further longitudinal support in Study 3. Anxiety, as measured at time 1, predicted anhedonia at time 2, which predicted depression over five and eleven total months. This provides further evidence of the connection between anxiety, anhedonia, and depression, and suggests how this relationship unfolds over time. Anhedonia did not explain all variance associated with this relationship, and thus there are of course other mechanisms that explain this connection (Batterham et al., 2013). We also found that a similar mediational pattern emerged such that anhedonia led to anxiety, which in turn led to depression. This suggests that this pathway to symptoms of depression also emerges in some individuals.
Unlike Studies 1 and 2, we did not find a moderator of anxiety. This could be for two reasons. First, Study 3 included an advance in our procedure ensuring valid response styles that may have precluded the need to assess for moderators such as defensive responding. Alternatively, it may merely be the case that defensiveness is not a robust moderator of the relationship between anxious and depressive symptoms. Future research can further parse these explanations.
General Discussion
In three studies, we found that anhedonia and enjoyment-relinquishment behaviors related to anxiety were also related to depression. In Study 1, relinquishment of enjoyment related to anxiety was uniquely associated with depression cross-sectionally. In Study 2, anxiety was indirectly related to depression through anhedonia in a cross-sectional sample. In Study 3, anhedonia again mediated the relationship between anxiety and depression, with this mediation emerging in two longitudinal analyses with different time-points to measure depression symptom outcomes, using validly-responding participants. In addition, we found that an alternative path showing that anhedonia at time 1 was associated with anxiety at time 2 and depression at time 3 and 4. Taken together, the findings provide evidence that for some individuals anxiety leads to anhedonia, which in turn leads to depression.
The manner in which anhedonia was operationalized may have been particularly important to contextualizing the current findings. The heightened relationship between anhedonia and depression (and, to a lesser extent, anxiety) was elevated in part because we were assessing recent changes in anhedonia, which have previously been found to be associated with other virulent depressive symptoms (Joiner et al., 2003; Winer et al., 2016b; Winer et al., 2014a; Winer et al., 2014b). Increase in anhedonia is thus distinguishable from trait physical anhedonia (Shankman et al., 2010), and is likely more associated with anticipatory than consummatory disturbance (Thomsen, 2015; Winer et al., 2014b). Thus, the relationships described herein are particular to increased social anhedonia, and would not necessarily emerge from trait-level, physical, or consummatory anhedonia based investigations.
These findings can also be considered alongside Clark and Watson’s (Clark and Watson, 1991; Mineka et al., 1998; Watson and Tellegen, 1985) tripartite model. This model posits that decreased positive affect (associated with extraversion or anhedonia) may be a unique contributing factor to depression. This model has received mixed evidence (Shankman and Klein, 2003), likely in part because of the trait-level conceptualization of positivity, as well as personality-based psychopathology in general (Borsboom, 2006; Clark, 2006). The current findings consider instead how one might move from anxious to depressed (or vice versa) outside of trait-level conceptualizations.
The prospective causal relationship that results in an anxious person developing depressive symptoms is intuitive. The individual develops anxious symptoms (“I frequently find myself worrying about something”) that begin to result in the loss of interest in previously rewarding experiences (“I have lost most interest in my favorite activities”) that results in other depressive symptoms (“I feel sad nearly all of the time”). The reverse pattern is feasible, as well. Losing interest in previously pleasurable social experiences may result in increased anxiety regarding that loss, which in turn manifests itself in ultimate sadness.
Compare the above path with the symptom negative mood. How might negative mood lead from composite anxious symptoms to depressive symptoms in a mediational model over time? In other words, how would negative mood be a mediating process between anxiety and depression? In our opinion it is merely a symptom that both anxious and depressed individuals endorse. So, were we to include it as a “control,” it would be to see if it reduced the association of anxiety and depression; but we already know that it likely would, because the vast majority of individuals experiencing depression or anxiety “has” general negative mood. In other words, does anxiety or depression commonly present without negative mood? If the answer is that one expects to see negative mood in both at any time point, then it is a poor candidate variable to predict changes from primarily anxious to primarily depressed symptoms over time.
One potential weakness of our analyses is that anhedonia is by definition a symptom of depression, which might prospectively explain this relationship. However, in both of our analyses, we removed items related to anhedonia from our measure of depression, thus accounting for this explanation. Instead, it is likely that the prospective causal pattern we have presented here is predictive of a particular path to depressive symptoms for some people. This may sound underwhelming, especially when considering the uniquely positive aspects of the constellation of methods and evidence we report here, which includes three separate studies, a replication of a mediation model in two studies, and a multiple time-point design unfolding over approximately one year and containing a built-in replication. But not all persons, of course, will demonstrate a pattern that emerges from even significant longitudinal mediational models (Winer et al., 2016a).
Indeed, these findings are an important step toward understanding causal relations between anxiety and depression that unfold over time. The current investigations were limited in our relatively small number of subjects and limited scope of our investigation, which focused primarily on determining if the pattern uncovered in Studies 1 and 2 extended over time. Because of these limitations we did not account for earlier time-points in our meditational analyses of Study 3 (e.g., depression at T1), a technique that is needed to confidently infer causal changes. However, we also chose not to overly penalize our longitudinal study on this account, given that a cross-sectional investigation, which has no ability to hold non-existent time-points constant (i.e., there is only one time-point to begin with), would not be vitiated by this limitation. However, the next step is to extend these findings by examining a fully cross-lagged panel model with a notably larger number of subjects over many years to further illuminate causal processes that turn anxious symptoms into depressed ones. Indeed, we found evidence for multiple prospective causal pathways to depressive symptoms, both of which might otherwise merely look like associations when examined cross-sectionally. The next step is to examine the dynamical interaction of anhedonia and other symptoms of depression over time to get more focused personalized pictures of the development of psychopathology.
Additionally, the studies presented here also are limited in that they are reliant on self-report measures of anxiety, anhedonia, and depression. Structured clinical interviewing would be beneficial in future investigations to determine the clinical significance of reported anxiety and depression symptoms. Furthermore, future work should examine the relationship between anxiety, anhedonia, and depression using experimental measures to further investigate the nature of this relationship.
Table 2.
Descriptive Statistics of Predictor, Outcome, and Mediator Variables for Studies 2 and 3
| M | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Study 2 | ||||
| 1. Anxiety | 8.68 | 4.81 | 0 | 20 |
| 2. Defensiveness | 10.14 | 3.52 | 0 | 19 |
| 3. Anhedonia | 5.30 | 7.67 | 0 | 39 |
| 4. Depression | 12.75 | 9.28 | 0 | 48 |
| Study 3, Mediation 1 | ||||
| 1. Anxiety (T1) | 8.66 | 6.01 | 0 | 20 |
| 2. Defensiveness (T1) | 10.17 | 4.49 | 0 | 20 |
| 3. Anhedonia (T2) | 9.84 | 10.65 | 0 | 40 |
| 4. Depression (T3) | 6.44 | 5.20 | 0 | 22 |
| Study 3, Mediation 2 | ||||
| 1. Anxiety (T1) | 8.56 | 5.97 | 0 | 20 |
| 2. Defensiveness (T1) | 10.25 | 4.64 | 0 | 20 |
| 3. Anhedonia (T2) | 10.33 | 10.89 | 0 | 40 |
| 4. Depression (T4) | 5.86 | 4.84 | 0 | 20 |
Highlights.
Three studies examined the relationships between anxiety, anhedonia, and depression
Anxiety and depression were positively associated in individuals who relinquished enjoyment due to anxiety-related avoidance.
Anhedonia also mediated the relationship between anxiety and depression cross-sectionally and over time.
Individuals thus begin to avoid potentially pleasurable activities because of anxiety, which may result in loss of pleasure and other depressive symptoms.
This is the first study to assess anxiety, anhedonia, and depression over time with both behavioral and the novel specific interest and pleasure scale.
Acknowledgments
None
Role of Funding: Research reported in this publication was partially supported by the National Institute of Mental Health of the National Institutes of Health [Grant Number: R15MH101573] awarded to ESW and a Research Fellowship from the Mississippi State University Shackhouls Honors College to JK. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix
Items administered between the Beck Anxiety Inventory and the Beck Depression Inventory.
— Page 1, Questions 1 —
-
1) How often do you engage in activities that you find enjoyable/interesting and that you are looking forward to?
Never or Rarely
Occasionally
Sometimes
Often
Very Often
— Page 2, Question 2 —
-
2) How enjoyable/interesting do you find these activities to be?
Very slightly
A little
Moderately
Quite a bit
Extremely
— Page 3 —
People sometimes give up certain enjoyable or interesting activities because these activities are also anxiety provoking.
Take a moment to think of enjoyable/interesting activities you may be giving up because they are anxiety provoking. Please list some or all of them below:
[Responses provided in a textbox]
— Page 4, Questions 3 and 4 —
1) Currently, what percentage of enjoyable/interesting activities do you avoid because they may trigger anxiety?
[Answers provided on a sliding scale from 0 to 100%]
-
2) How enjoyable/interesting would you find these activities to be (if you could do them without experiencing any anxiety)?
Very slightly
A little
Moderately
Quite a bit
Extremely
— Page 5 —
Now consider activities important to your future, your career, your health, your family etc., that you may be giving up because they are anxiety provoking. Please list some or all of them below:
[Responses provided in a textbox]
— Page 6, Questions 5 and 6 —
1) Currently, what percentage of important activities do you avoid because they may trigger anxiety?
[Answers provided on a sliding scale from 0 to 100%]
-
2) How important would you find these activities to be (if you could do them without experiencing any anxiety)?
Very slightly
A little
Moderately
Quite a bit
Extremely
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of interest
None.
Contributors
ESW, JB, GB, and ER conceived of the design and analytic plan and performed statistical analyses. ESW, GB, MN, and JK led data collection. ESW drafted the manuscript along with JB and GB. All authors contributed to and approved the final manuscript.
References
- Bartoszek G, Winer ES. Spider-fearful individuals hesitantly approach threat, whereas depressed individuals do not persistently approach reward. Journal of behavior therapy and experimental psychiatry. 2015;46:1–7. doi: 10.1016/j.jbtep.2014.07.012. [DOI] [PubMed] [Google Scholar]
- Batterham PJ, Christensen H, Calear AL. Anxiety symptoms as precursors of major depression and suicidal ideation. Depression and Anxiety. 2013;30:908–916. doi: 10.1002/da.22066. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA. Manual for the Beck anxiety inventory 1990 [Google Scholar]
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory 1996 [Google Scholar]
- Belzer K, Schneider FR. Comorbidity of Anxiety and Depressive Disorders: Issues in Conceptualization, Assessment, and Treatment. Journal of Psychiatric Practice®. 2004;10:296–306. doi: 10.1097/00131746-200409000-00003. [DOI] [PubMed] [Google Scholar]
- Bendig AW. The development of a short form of the manifest anxiety scale. Journal of consulting psychology. 1956;20:384. doi: 10.1037/h0045580. [DOI] [PubMed] [Google Scholar]
- Borsboom D. Can we bring about a velvet revolution in psychological measurement? A rejoinder to commentaries. Psychometrika. 2006;71:463. doi: 10.1007/s11336-006-1502-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brosschot JF, de Ruiter C, Kindt M. Processing bias in anxious subjects andrepressors, measured by emotional Stroop interferenceandattentional allocation. Personality and Individual Differences. 1999;26:777–793. [Google Scholar]
- Carvalho JP, Hopko DR. Behavioral theory of depression: reinforcement as a mediating variable between avoidance and depression. J Behav Ther Exp Psychiatry. 2011;42:154–162. doi: 10.1016/j.jbtep.2010.10.001. [DOI] [PubMed] [Google Scholar]
- Chandler J, Shapiro D. Conducting Clinical Research Using Crowdsourced Convenience Samples. Annual Review of Clinical Psychology. 2016;12:53–81. doi: 10.1146/annurev-clinpsy-021815-093623. [DOI] [PubMed] [Google Scholar]
- Clark LA. When a psychometric advance falls in the forest. Psychometrika. 2006;71:447. doi: 10.1007/s11336-006-1500-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark LA, Watson D. Journal of Abnormal Psychology. 1991;100:316. doi: 10.1037//0021-843x.100.3.316. [DOI] [PubMed] [Google Scholar]
- Cramer AO, Waldorp LJ, Van Der Maas HL, Borsboom D. Comorbidity: A network perspective. Behavioral and Brain Sciences. 2010;33:137–193. doi: 10.1017/S0140525X09991567. [DOI] [PubMed] [Google Scholar]
- Ferster CB. A functional analysis of depression. American psychologist. 1973;28:857. doi: 10.1037/h0035605. [DOI] [PubMed] [Google Scholar]
- Frewen PA, Allen SL, Lanius RA, Neufeld RWJ. Perceived Causal Relations Novel Methodology for Assessing Client Attributions About Causal Associations Between Variables Including Symptoms and Functional Impairment. Assessment. 2012;19:480–493. doi: 10.1177/1073191111418297. [DOI] [PubMed] [Google Scholar]
- Frewen PA, Schmittmann VD, Bringmann LF, Borsboom D. Perceived causal relations between anxiety, posttraumatic stress and depression: extension to moderation, mediation, and network analysis. European journal of psychotraumatology. 2013;4 doi: 10.3402/ejpt.v4i0.20656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Press; New York: 2013. [Google Scholar]
- Horton JJ, Chilton LB. The labor economics of paid crowdsourcing, Proceedings of the 11th ACM conference on Electronic commerce. ACM. 2010:209–218. [Google Scholar]
- Jacobson NC, Newman MG. Avoidance mediates the relationship between anxiety and depression over a decade later. Journal of Anxiety Disorders. 2014;28:437–445. doi: 10.1016/j.janxdis.2014.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joiner TE, Brown JS, Metalsky GI. A test of the tripartite model’s prediction of anhedonia’s specificity to depression: patients with major depression versus patients with schizophrenia. Psychiatry Research. 2003;119:243–250. doi: 10.1016/s0165-1781(03)00131-8. [DOI] [PubMed] [Google Scholar]
- Jordan DG, Winer ES, Salem T, Kilgore J. Longitudinal evaluation of anhedonia as a mediator of fear of positive evaluation and other depressive symptoms. Cognition & Emotion. doi: 10.1080/02699931.2017.1289895. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Judd CM, Kenny DA, McClelland GH. Estimating and testing mediation and moderation in within-subject designs. Psychol Methods. 2001;6:115–134. doi: 10.1037/1082-989x.6.2.115. [DOI] [PubMed] [Google Scholar]
- Kline RB. Principles and Practice of Structural Equation Modeling. New York, NY: Guilford; 2005. 2005. [Google Scholar]
- Leeper TJ. Introduction to the Simple Wizard (Text Based) 2014 [Google Scholar]
- Loas G. Anhedonia and risk of suicide: an overview, Anhedonia: A Comprehensive Handbook Volume II. Springer; 2014. pp. 247–253. [Google Scholar]
- Mineka S, Watson D, Clark LA. Comorbidity of anxiety and unipolar mood disorders. Annual review of psychology. 1998;49:377–412. doi: 10.1146/annurev.psych.49.1.377. [DOI] [PubMed] [Google Scholar]
- Moitra E, Herbert JD, Forman EM. Behavioral avoidance mediates the relationship between anxiety and depressive symptoms among social anxiety disorder patients. Journal of Anxiety Disorders. 2008;22:1205–1213. doi: 10.1016/j.janxdis.2008.01.002. [DOI] [PubMed] [Google Scholar]
- Mueller P, Chandler J. Emailing workers using Python. 2012 Available at SSRN 2100601. [Google Scholar]
- Myers LB, Burns JW, Derakshan N, Elfant E, Eysenck MW, Phipps S. In: Vingerhoets A, Nyklícek I, Denollet J, editors. Current issues in repressive coping and health; Conference on The (Non)Expression of Emotions in Health and Disease; 2003; Tilburg, Netherlands. New York, NY, US: Springer Science + Business Media; 2008. pp. 69–86. [Google Scholar]
- Nadorff MR, Salem T, Winer ES, Lamis DA, Nazem S, Berman ME. Explaining alcohol use and suicide risk: a moderated mediation model involving insomnia symptoms and gender. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2014;10:1317–1323. doi: 10.5664/jcsm.4288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price RB, Rosen D, Siegle GJ, Ladouceur CD, Tang K, Allen KB, Ryan ND, Dahl RE, Forbes EE, Silk JS. From anxious youth to depressed adolescents: Prospective prediction of 2-year depression symptoms via attentional bias measures. J Abnorm Psychol. 2016;125:267–278. doi: 10.1037/abn0000127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale a self-report depression scale for research in the general population. Applied psychological measurement. 1977;1:385–401. [Google Scholar]
- Rush AJ, Bernstein IH, Trivedi MH, Carmody TJ, Wisniewski S, Mundt JC, Shores-Wilson K, Biggs MM, Woo A, Nierenberg AA, Fava M. An evaluation of the quick inventory of depressive symptomatology and the hamilton rating scale for depression: a sequenced treatment alternatives to relieve depression trial report. Biol Psychiatry. 2006;59:493–501. doi: 10.1016/j.biopsych.2005.08.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, Markowitz JC, Ninan PT, Kornstein S, Manber R, Thase ME, Kocsis JH, Keller MB. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54:573–583. doi: 10.1016/s0006-3223(02)01866-8. [DOI] [PubMed] [Google Scholar]
- Shankman SA, Klein DN. The relation between depression and anxiety: An evaluation of the tripartite, approach-withdrawal and valence-arousal models. Clinical psychology review. 2003;23:605–637. doi: 10.1016/s0272-7358(03)00038-2. [DOI] [PubMed] [Google Scholar]
- Shankman SA, Nelson BD, Harrow M, Faull R. Does physical anhedonia play a role in depression? A 20-year longitudinal study. Journal of affective disorders. 2010;120:170–176. doi: 10.1016/j.jad.2009.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shapiro DN, Chandler J, Mueller PA. Using Mechanical Turk to Study Clinical Populations. Clinical Psychological Science. 2013;1:213–220. [Google Scholar]
- Strahan R, Gerbasi KC. Short, homogeneous versions of the Marlowe-Crowne Social Desirability Scale. Journal of Clinical Psychology. 1972;28:191–193. [Google Scholar]
- Thomsen KR. Measuring anhedonia: impaired ability to pursue, experience, and learn about reward. Frontiers in Psychology. 2015;6:1409. doi: 10.3389/fpsyg.2015.01409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Tellegen A. Toward a consensual structure of mood. Psychological bulletin. 1985;98:219. doi: 10.1037//0033-2909.98.2.219. [DOI] [PubMed] [Google Scholar]
- Weinberger DA. The construct validity of the repressive coping style. Repression and dissociation: Implications for personality theory, psychopathology, and health. 1990:337–386. [Google Scholar]
- Winer ES, Cervone D, Bryant J, McKinney C, Liu RT, Nadorff MR. Distinguishing Mediational Models and Analyses in Clinical Psychology: Atemporal Associations Do Not Imply Causation. J Clin Psychol. 2016a;72:947–955. doi: 10.1002/jclp.22298. [DOI] [PubMed] [Google Scholar]
- Winer ES, Cervone D, Newman LS, Snodgrass M. Subchance perception: Anxious, non-defensive individuals identify subliminally-presented positive words at below-chance levels. Personality and Individual Differences. 2011;51:996–1001. [Google Scholar]
- Winer ES, Drapeau CW, Veilleux JC, Nadorff MR. The Association between Anhedonia, Suicidal Ideation, and Suicide Attempts in a Large Student Sample. Archives of suicide research : official journal of the International Academy for Suicide Research. 2016b;20:265–272. doi: 10.1080/13811118.2015.1025119. [DOI] [PubMed] [Google Scholar]
- Winer ES, Drapeau CW, Veilleux JC, Nadorff MR. The relationship between anhedonia, suicidal ideation, and suicide attempts in a large student sample. Archives of Suicide Research. 2016c;20:265–272. doi: 10.1080/13811118.2015.1025119. [DOI] [PubMed] [Google Scholar]
- Winer ES, Nadorff MR, Ellis TE, Allen JG, Herrera S, Salem T. Anhedonia predicts suicidal ideation in a large psychiatric inpatient sample. Psychiatry Research. 2014a;218:124–128. doi: 10.1016/j.psychres.2014.04.016. [DOI] [PubMed] [Google Scholar]
- Winer ES, Salem T. Reward devaluation: Dot-probe meta-analytic evidence of avoidance of positive information in depressed persons. Psychological Bulletin. 2016;142:18–78. doi: 10.1037/bul0000022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winer ES, Veilleux JC, Ginger EJ. Development and validation of the Specific Loss of Interest and Pleasure Scale (SLIPS) Journal of Affective Disorders. 2014b:152–154. doi: 10.1016/j.jad.2013.09.010. [DOI] [PubMed] [Google Scholar]