

Introduction
Eventration of the diaphragm is a rare condition where the diaphragm is permanently elevated, but retains its continuity and attachments to the costal margins.1 This condition affects less than 0.05% of general population and is more common in males.2 Rupture of eventration of diaphragm, which is extremely rare in a child, can be either traumatic or spontaneous.3, 4, 5, 6, 7, 8, 9 As there is paucity of literature of spontaneous rupture of eventration of diaphragm in children, we report a child with non-traumatic rupture of eventration of diaphragm.
Case report
A 5 year old male patient presented to the pediatric emergency with history of diffuse pain abdomen, repeated vomiting, and constipation since 4 days and fever since 1 day. There was no history of cough, chest in drawings or fast breathing. In the past, there was no significant history of respiratory illnesses. Clinically the child was having mild dehydration with low grade fever, however there was no features of hemodynamic instability or respiratory distress. The abdomen was tender at the left hypochondrium, but there was no significant distension or guarding. Auscultation of the chest revealed bowel sounds associated with decreased breath sounds in left lower hemithorax. Radiograph chest and abdomen showed dilated bowel loops in the abdomen extending into the left lower chest causing mediastinal shift toward right (Fig. 1A). Contrast enhanced CT scan of the thorax confirmed the chest X-ray findings (Fig. 1B). All hematological and metabolic parameters including the blood gas were normal.
Fig. 1.

(A and B) Raised left hemidiaphragm with abdominal contents inside left hemithorax with mediastinal shift to right (radiograph and Computed Tomography (CT) respectively of chest and abdomen).
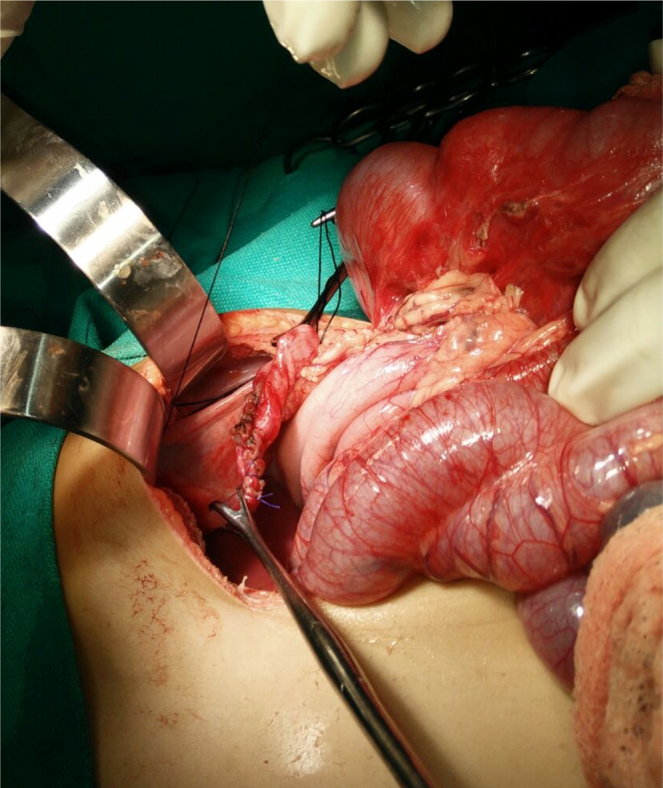
Surgery was undertaken with a probable diagnosis of left sided diaphragmatic hernia. Laparotomy was done through the left subcostal incision, which revealed a grossly thinned out diaphragm with a rent of 2 cm at its apex (Fig. 2A). Through the rent, part of the transverse colon and the omentum was herniating causing proximal colonic dilatation. The contents were reduced and the obstruction got relieved. The bowel seemed to be viable and the gangrenous omentum was excised (Fig. 2B). The rent was closed with vicryl and thinned out diaphragm was plicated with nonabsorbable sutures (Fig. 3).
Fig. 2.

(A and B) Rent (after widening) and gangrenous omentum as seen intra op.
Fig. 3.
Closure of rent in diaphragm.
Post operatively the child recovered well, and the feeds were resumed on postop day 3 and were discharged at the end of a week. The child was asymptomatic during the follow up and the radiograph chest showed well-expanded lungs and near normal contour of the diaphragm (Fig. 4).
Fig. 4.

Post-operative radiograph chest showing well expanded lungs and near normal contour of diaphragm.
Discussion
Eventration of diaphragm often remains asymptomatic for long and may present with recurrent respiratory tract infections and sometimes as gastric volvulus. Though congenital diaphragmatic hernias (CDH) are known to present with bowel herniation and obstruction but eventration of diaphragm without rupture are seldom known to cause this situation. Eventration of diaphragm presenting with rupture in a child is extremely rare. So far only 6 cases of children with non-traumatic rupture have been reported in literature, to our knowledge.4, 5, 6, 7, 8, 9 In adults, on the other hand, the rupture of eventrated diaphragm reported so far, have been mostly post-traumatic and sometimes after a precedential straining in the form of severe coughing or labor.10
Diaphragmatic rupture in the background of eventration is more common on left side, most possibly because the liver protects the right hemi diaphragm. The reasons of rupture other than blunt trauma,3 are varied in nature. The rupture of eventratic diaphragm has been attributed to spontaneous without any cause,4, 5, 6 violent cough due to pertussis,7, 8 and physical exertion.9 In our case there was no preceding history of cough, trauma or any heavy physical exertion and thus the reason of rupture was thought to be spontaneous.
Thus spontaneous rupture should be considered as a possible complication of diaphragmatic eventration, albeit reported rarely. The closest differential diagnosis is a CDH. The factor that differentiates itself from CDH being the ragged edges of the rent on a thinned out diaphragm compared to well-defined rim of defect in CDH. These ruptures are especially prone to strangulation of contents and require prompt exploration. The possibility of absence of respiratory symptoms and features of intestinal obstruction can be misleading. However the routine use of radiograph, which is likely to show bowel gas in thorax can clinch the diagnosis and guide the clinician to a suitable appropriate laparotomy access through a subcostal incision. Thoracotomy is generally preferred for diaphragmatic ruptures on the right side due to presence of liver, whereas laparotomy is preferred for the left sided ruptures.5 Thoracoscopic and laparoscopic approaches are also equally effective but usually not resorted to in acute presentation especially with associated intestinal obstruction. The procedure should involve reduction of the contents, closure of the rent and addressing the redundant thinned out diaphragm by plication or partial excision. Mesh cover may be required in case of large defect. However, in our patient, simple closure of defect with placation of native diaphragm yielded good outcome.
To conclude, we have presented a spontaneous non-traumatic rupture of eventration of diaphragm on left side of a child. The aim of reporting this case is to sensitize the readers of a rare unexpected finding in a child with diffuse abdominal pain, closely mimicking congenital diaphragmatic hernia on the left side.
Conflicts of interest
The authors have none to declare.
References
- 1.Cordeiro J.A., Almeida A.K., Junior S.A.O. Diaphragmatic eventration: review of current knowledge, diagnostic, and management options. Int J Med Res Health Sci. 2016;5(3):62–65. [Google Scholar]
- 2.Miyano G., Yamoto M., Kaneshiro M. Diaphragmatic eventration in children: laparoscopy versus thoracoscopic plication. J Laparoendosc Adv Surg Tech A. 2015;25(April (4)):331–334. doi: 10.1089/lap.2014.0237. [DOI] [PubMed] [Google Scholar]
- 3.Lone R.A., Sharma M.L., Wani M. Traumatic diaphragmatic rupture, a diagnostic dilemma in the presence of eventration: a case report. Cases J. 2009;2:6615. doi: 10.4076/1757-1626-2-6615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gun F., Gunendi T., Erginel B. Rupture of a congenital diaphragmatic eventration in a child: report of a case. Surg Today. 2011;41:1630–1632. doi: 10.1007/s00595-010-4475-x. [DOI] [PubMed] [Google Scholar]
- 5.Saha S., Bal H.S., Sen S. Spontaneous rupture of a congenital diaphragmatic eventration in an infant. BMJ Case Rep. 2015 doi: 10.1136/bcr-2014-208634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Akbar A., Dakshesh H.P., Alton H., Clarke J., Weller P., Green S. Spontaneous rupture of the diaphragm. Arch Dis Child. 1999;81:341–342. doi: 10.1136/adc.81.4.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dutta T. Spontaneous rupture of the diaphragm due to pertussis. J Pediatr Surg. 1975;10:147–148. doi: 10.1016/s0022-3468(75)80027-3. [DOI] [PubMed] [Google Scholar]
- 8.Heuckmann L., Kuster P., Schleef J., Uekotter J. Diaphragmatic rupture in pertussis. Monatsschr Kinderheilkd. 1996;144:259–262. [Google Scholar]
- 9.Srpčič M., Bitenc M. Subacute presentation of spontaneous diaphragmal rupture: a case report. Eur Surg. 2005;37(6):340–342. [Google Scholar]
- 10.Ali Shah S.Z., Khan S.A., Bilal A. Eventration of diaphragm in adults: eleven years’ experience. J Ayub Med Coll Abbottabad. 2014;26(October–December (4)):459–462. [PubMed] [Google Scholar]