

Abstract
Background:
The success of root canal therapy requires a good knowledge of root canal morphology. Literature review shows variations in a number of roots and canal morphology in studies done across the globe.
Aim:
The purpose of this study was to evaluate the root canal morphology in maxillary first premolars using the clearing technique in a South Indian population.
Methodology:
Two hundred and twenty-five extracted noncarious, nonfractured, sound maxillary first premolars were collected, cleaned, and were injected with India ink to stain the root canals. Teeth were then decalcified and cleared using methyl salicylate. Teeth were then viewed under a stereomicroscope to evaluate the number of roots, root canal morphology based on the Vertucci's classification, variations, and additional features such as accessory root canals, lateral canals, furcation canals, isthmus, and apical delta.
Results:
Nearly 52.88% of maxillary first premolars were single rooted, 44.88% had two roots, and 2.22% had three roots. Vertucci's Type IV root canal configuration was the most common type in maxillary first premolars and was seen in 66.51% of cases followed by Type II in 13.4%. Type I was seen in 9.76%, Type VI in 6.51%, Type VIII in 2.32%, Type III in 0.46%, Type V in 0.46%, and Type VII in 0% of teeth.
Conclusion:
The majority of the maxillary first premolars included in our study were single rooted and Vertucci's Type IV was the most common type of root canal configuration.
Keywords: Clearing, first premolar, maxillary, methyl salicylate, root canal
Introduction
A successful endodontic therapy requires the complete debridement and obturation of the root canals and hence the knowledge of the root canal morphology and its variations is of utmost importance to clinicians. The morphology of roots is highly variable and complex,[1] thus necessitating the need for studies to understand the anatomy better so that clinicians can apply this knowledge clinically.
Human dentition shows a wide range of anatomical variations in each tooth type as reported in terms of the number and shape of roots and root canals.[2,3,4,5,6] Studies done on root canal morphology across the globe have clearly demonstrated that root and canal morphology vary greatly between populations and even within populations.[2,6,7]
The maxillary first premolars are difficult to be treated endodontically due to the variation in a number of roots, canal configuration, direction and longitudinal depressions of the roots, and pulp cavity configurations.[8] Different methods have been used by researchers to study tooth morphology including decalcification of teeth and dye injection, sectioning of the teeth and radiographic studies in vitro, alternative radiographic techniques and radiographic assessment enhanced with contrast media.[9,10,11]
The present study was thus aimed at studying the roots and canal morphology of maxillary first premolars in a South Indian population as the literature shows no studies on maxillary first premolars exclusively in this population. The clearing technique was adopted for the study as it provides a three-dimensional view of the entire root canal system and the technique is relatively simple and acceptable.
Methodology
Teeth were collected from the department of oral surgery, private dental clinics, dental camps, and rural satellite centers of our University. All teeth were collected in separate bottles containing 10% formalin.
Inclusion criteria
Freshly extracted sound permanent maxillary first premolar.
Exclusion criteria
Teeth with caries and restorations
Fractured teeth
Teeth with open apex/immature teeth.
Extracted teeth were collected and cleaned with hydrogen peroxide. Access cavity was prepared occlusally using a dental micromotor and 5.25% sodium hypochlorite solution was injected into the canal and was kept in the same solution for a day to remove organic debris. Teeth were flushed thoroughly with distilled water to remove the solution from the canal system and to ensure patency of apical openings. Nail paint was applied onto the teeth and the teeth were allowed to dry. India ink was injected into the access cavity. The entry into all canals was enhanced with the use of an apical suction. The teeth were then sealed with a glass ionomer cement. Nail paint was removed with acetone and the teeth were allowed to dry. Teeth were then immersed in 8% nitric acid for few days until decalcification and washed under running tap water for the removal of acid. Teeth were dehydrated in different grades of alcohol for half an hour each and then placed in methyl salicylate for clearing until they became transparent. Teeth were then viewed under a stereomicroscope.
The following parameters were analyzed on the plastinated teeth:
Morphology of the root canal and type (based on Vertucci's classification of root canal morphology)
Additional findings such as accessory root canals, lateral canals, furcation canals, isthmus, and apical delta.
Photomicrography was captured and analyzed using the 5MP CMOS Camera (Lawrence & Mayo, India Pvt Ltd, Bengaluru).
Results
Two hundred and twenty-five maxillary first premolars were collected. Majority (52.88%) of the maxillary first premolars were single rooted, 44.88% had two roots, and 2.22% had three roots. Ten teeth could not be assessed for root canal morphology as the canals were completely calcified and did not allow penetration of the dye during the procedure. Two hundred and fifteen teeth were evaluated for root canal morphology.
Morphology of the root canal and type (based on Vertucci's classification of root canal morphology: 1984)
Type IV root canal configuration was the most common type in maxillary first premolars and was seen in 66.51% of cases followed by Type II in 13.4%. Type I was seen in 9.76%, Type VI in 6.51%, Type VIII in 2.32%, Type III in 0.46%, Type V in 0.46%, and Type VII in 0% of teeth [Figures 1, 2 and Table 1].
Figure 1.

(a) Type I root canal morphology. (b) Type II root canal morphology. (c) Type III root canal morphology. (d) Type IV root canal morphology
Figure 2.

(a) Type V root canal morphology. (b) Type VI root canal morphology. (c) Type VIII root canal morphology
Table 1.
Root canal morphology of maxillary first premolars based on Vertucci's classification
![]()
One tooth was categorized as Gulabivala's Type 2–3 root morphology.[12]
Lateral canals, isthmus, furcation canals, accessory canals, and apical delta
Lateral canals were seen in 13.95%, isthmus in 20.93%, furcation canals in 4.65%, accessory canals in 16.27%, and apical delta in 0.93% of maxillary first premolars [Figure 3].
Figure 3.
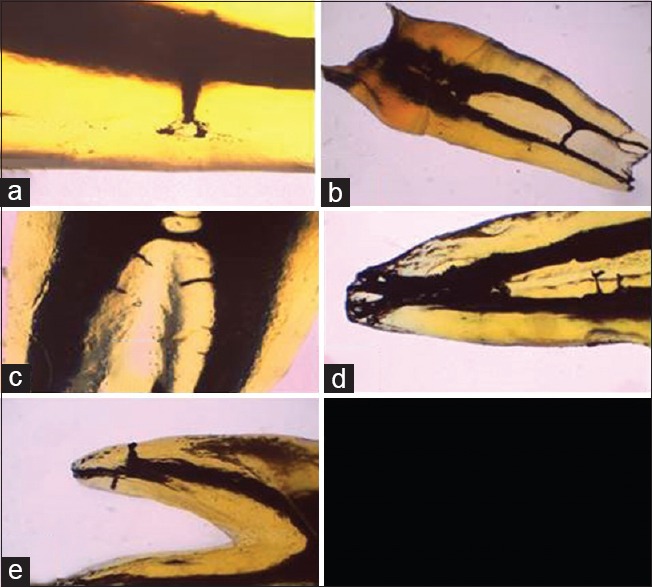
(a) Lateral canals. (b) Isthmus. (c) Furcation canals. (d) Apical delta. (e) Accessory canals
Discussion
Root canal morphology varies significantly among various populations and hence there is a difference in the study results across the globe. The transparent tooth model technique provides the greatest information of the original form and anatomy of the root canals and was, thus, used in this study. Gupta et al. stated that the combination of nitric acid and methyl salicylate for the transparent tooth model provided the best results.[13]
Maxillary premolars account for 15.8%–21.5% of all endodontically treated teeth.[14] Maxillary premolars are believed to be difficult to treat endodontically owing to their variations. Literature review showed that there were no studies on maxillary premolars in the South Indian population.
The aim of the study was to evaluate the root canal morphology of maxillary first premolars using the clearing technique in the South Indian population. A stereomicroscope was used to analyze the teeth.
In the present study, the majority (52.88%) of the maxillary first premolars were single rooted, 44.88% had two roots, and 2.22% had three roots. This was in accordance with other studies done on the Asian population as follows: Gupta et al. in the Indian population, Dashrath et al. in the Nepalese population, Tian et al., Cheng and Weng, and Walker in the Chinese population, and Peiris et al. in the Sri Lankan population of Japan.[15,16,17,18,19,20]
In contrast, Neelakantan et al. in a similar study in India found that 11.7% of maxillary first premolars had one root, 86% had two roots, and 2.3% had three roots.[21]
However, an extensive database review of all similar studies on maxillary first premolar across the globe shows the predominance of double-rooted teeth.[14]
The differences between the results of these studies could be the result of different examination methods, classification systems, sample sizes, and ethnic background of the population.[15]
Three-rooted premolars are also called radiculous premolars, small molars, minimolars, or miniature three-canalled molars and have an incidence of 1.7% (0.4%–9.2%).[14] Our study showed 5 (2.22%) out of 225 teeth with three roots.
In the present study, Type IV root canal configuration was the most common type and was seen in 66.51% cases followed by Type II in 13.4%. Type I was seen in 9.76%, Type VI in 6.51%, Type VIII in 2.32%, Type III in 0.46%, Type V in 0.46%, and Type VII in 0% of teeth.
Type IV root canal configuration was the most common type in maxillary first premolar in all similar studies reviewed. When other types are compared, our results were similar to the study done by Vertucci et al. who found Type IV root canal configuration in 62% cases followed by Type II in 18%. Type I was seen in 8%, Type V in 7%, Type VIII in 5%, Type III in 0%, Type VI in 0%, and Type VII in 0% of teeth.[12]
Type IV root canal morphology was the most common type seen in all studies on maxillary first premolars but vary to some extent in frequency and percentage of individual canal types in studies done by other authors in the Indian population. Gupta et al. in a similar study of maxillary premolars in the Indian population found Type IV root canal configuration in 33.2% cases followed by Type I in 23.2%. Type II was seen in 14.8%, Type III in 13.6%, Type V in 6.8%, Type VII in 4%, Type VI in 2%, and Type VIII in 0.4% of teeth.[17] Sharma and Mathur in a computed tomographic study of canal variations in maxillary first premolars in Jaipur (Indian) population found Type IV root canal configuration in 45% of cases followed by Type II in 25%. Type V was seen in 11.67%, Type III in 8.33%, Type I in 5%, Type VI in 3.33%, Type VII in 1.67%, and Type VIII in 0% of teeth.[22]
Since factors such as ethnicity contribute immensely to root canal morphology and their variations, there is a considerable variation in the study results by various authors from different countries.
Lateral canals are communication channels between the main root canal and the periodontal ligament space. They are seen anywhere along its length, at right angles to the main canal. The term accessory canal is usually reserved for small canals found in the apical few millimeters. Lateral and accessory canals develop due to breaks in the Hertwig's epithelial root sheath or the sheath grows around existing blood vessels during development.[23] These canals act as avenues for the transit of irritants from the pulp to the periodontium.[2]
Our study showed lateral canals and accessory canals in 13.95% and 16.27% of teeth, respectively. Gupta et al. in a similar study demonstrated the presence of lateral canals in 34.8%, Rwenyonyi et al. in 19.3% and Rwenyonyi et al. in 28.2%, of maxillary first premolars.[15,24,25] A complete literature review of all studies on maxillary first premolars noted that lateral canals on average are seen in 37% of teeth.[14] Our study showed less percentage of lateral canals as the accessory canals were examined separately in contrast to the other studies which have included accessory canals as lateral canals.
Furcation canals result due to the entrapment of periodontal vessels during merging of the diaphragm which becomes the roof of the pulp chamber.[26] Furcation canals were present in 4.65% of teeth in the present study. Vertucci and Anthony noted that mandibular teeth show a higher incidence of furcation canals than maxillary teeth.[27]
Apical delta is a root canal morphology where the main canal divides into multiple accessory canals at or near the apex.[28] Only 0.93% of teeth showed the presence of apical delta in the present study. Apical delta were seen in 3.2% of maxillary first premolars in a similar study by Vertucci (1984) and in 4.3% by Awawdeh et al.[2,24]
An isthmus is a ribbon-shaped, narrow connection between the two root canals.[29] The present study showed isthmus in 20.93% of the study sample as compared to the other studies which found an average of 16%. Isthmus was seen in 16% and 21% of teeth in studies done by Gupta et al. and Kartal et al.[15,30]
The main canals/additional canals are left untreated or inadequately cleaned/obturated mainly because the dentist fails to recognize its presence. Bacteria persist in root canals because areas such as isthmuses, lateral canals, accessory canals, and ramifications may evade disinfectants. Maxillary premolars show a considerable degree of endodontic failures owing to their variations in a number of roots and root canal types. Every practitioner must treat teeth assuming that complicated root canal anatomy occurs enough to be considered normal.
Conclusion
Although numerous studies have been done previously on maxillary premolars, there are very few studies among the Indian population, especially the South Indian population. This study contributes toward gathering data regarding the root canal morphology in the South Indian population which can be utilized by endodontists and for further population-based studies by researchers. Dentists need to be aware of the complex root canal anatomy and specifically of a particular population for better treatment planning.
Financial support and sponsorship
This study was funded by the Grant-in-aid scheme of the Department of Health Research, Indian Council of Medical Research, New Delhi, India.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to acknowledge the Indian Council of Medical Research, New Delhi, India, for funding this project under the Grant-in-aid scheme of the Department of Health Research.
References
- 1.Ahmed HM, Dummer PM. A new system for classifying tooth, root and canal anomalies. Int Endod J. 2018;51:389–404. doi: 10.1111/iej.12867. [DOI] [PubMed] [Google Scholar]
- 2.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Top. 2005;10:3–29. [Google Scholar]
- 3.Ahmed HM. Anatomical challenges, electronic working length determination and current developments in root canal preparation of primary molar teeth. Int Endod J. 2013;46:1011–22. doi: 10.1111/iej.12134. [DOI] [PubMed] [Google Scholar]
- 4.Ahmed HM, Hashem AA. Accessory roots and root canals in human anterior teeth: A review and clinical considerations. Int Endod J. 2016;49:724–36. doi: 10.1111/iej.12508. [DOI] [PubMed] [Google Scholar]
- 5.Versiani MA, Pécora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: A micro-computed tomography study. J Endod. 2012;38:977–82. doi: 10.1016/j.joen.2012.03.026. [DOI] [PubMed] [Google Scholar]
- 6.Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch Oral Biol. 2016;61:130–7. doi: 10.1016/j.archoralbio.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 7.Ahmed HM. A paradigm evolution shift in the endodontic map. Eur J Gen Dent. 2015;4:98. [Google Scholar]
- 8.Pécora JD, Saquy PC, Sousa Neto MD, Woelfel JB. Root form and canal anatomy of maxillary first premolars. Braz Dent J. 1991;2:87–94. [PubMed] [Google Scholar]
- 9.Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33:101–10. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 10.Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int Endod J. 2009;42:447–62. doi: 10.1111/j.1365-2591.2008.01530.x. [DOI] [PubMed] [Google Scholar]
- 11.Scarfe WC, Fana CR, Jr, Farman AG. Radiographic detection of accessory/lateral canals: Use of radioVisioGraphy and Hypaque. J Endod. 1995;21:185–90. doi: 10.1016/S0099-2399(06)80563-7. [DOI] [PubMed] [Google Scholar]
- 12.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34:359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 13.Gupta B, Tiwari B, Raj V, Kashyap B, Chandra S, Dwivedi N. Transparent tooth model: A study of root canal morphology using different reagents. Eur J Gen Dent. 2014;3:66–70. [Google Scholar]
- 14.Ahmad IA, Alenezi MA. Root and root canal morphology of maxillary first premolars: A Literature review and clinical considerations. J Endod. 2016;42:861–72. doi: 10.1016/j.joen.2016.02.017. [DOI] [PubMed] [Google Scholar]
- 15.Gupta S, Sinha DJ, Gowhar O, Tyagi SP, Singh NN, Gupta S, et al. Root and canal morphology of maxillary first premolar teeth in North Indian population using clearing technique: An in vitro study. J Conserv Dent. 2015;18:232–6. doi: 10.4103/0972-0707.157260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dashrath K, Nisha A, Subodh S. Root morphology and tooth length of maxillary first premolar in Nepalese population. Dentistry. 2015;5:324. [Google Scholar]
- 17.Tian YY, Guo B, Zhang R, Yu X, Wang H, Hu T, et al. Root and canal morphology of maxillary first premolars in a Chinese subpopulation evaluated using cone-beam computed tomography. Int Endod J. 2012;45:996–1003. doi: 10.1111/j.1365-2591.2012.02059.x. [DOI] [PubMed] [Google Scholar]
- 18.Cheng XL, Weng YL. Observation of the roots and root canals of 442 maxillary first premolars. Shanghai Kou Qiang Yi Xue. 2008;17:525–8. [PubMed] [Google Scholar]
- 19.Walker RT. Root form and canal anatomy of maxillary first premolars in a Southern Chinese population. Endod Dent Traumatol. 1987;3:130–4. doi: 10.1111/j.1600-9657.1987.tb00614.x. [DOI] [PubMed] [Google Scholar]
- 20.Peiris R. Root and canal morphology of human permanent teeth in a Srilankan and Japanese population. Anthropol Sci. 2008;116:123–33. [Google Scholar]
- 21.Neelakantan P, Subbarao C, Ahuja R, Subbarao CV. Root and canal morphology of Indian maxillary premolars by a modified root canal staining technique. Odontology. 2011;99:18–21. doi: 10.1007/s10266-010-0137-0. [DOI] [PubMed] [Google Scholar]
- 22.Sharma D, Mathur M. A computed tomographic study of canal variations in maxillary and mandibular first premolar teeth in Jaipur population: An in vitro study. People J Sci Res. 2011;4:1–5. [Google Scholar]
- 23.Carrotte P. Endodontics: Part 4. Morphology of the root canal system. Br Dent J. 2004;197:379–83. doi: 10.1038/sj.bdj.4811711. [DOI] [PubMed] [Google Scholar]
- 24.Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of Jordanian maxillary first premolars. J Endod. 2008;34:956–61. doi: 10.1016/j.joen.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 25.Rwenyonyi CM, Kutesa A, Muwazi L, Buwembo W. Root and canal morphology of maxillary first premolar teeth in a Ugandan population. Open J Stomatol. 2011;1:7–11. [Google Scholar]
- 26.Cutright DE, Bhaskar SN. Pulpal vasculature as demonstrated by a new method. Oral Surg Oral Med Oral Pathol. 1969;27:678–83. doi: 10.1016/0030-4220(69)90104-2. [DOI] [PubMed] [Google Scholar]
- 27.Vertucci FJ, Anthony RL. A scanning electron microscopic investigation of accessory foramina in the furcation and pulp chamber floor of molar teeth. Oral Surg Oral Med Oral Pathol. 1986;62:319–26. doi: 10.1016/0030-4220(86)90015-0. [DOI] [PubMed] [Google Scholar]
- 28.Glossary of Endodontic Terms. 9th ed. Chicago: American Association of endodontists; 2015. American Association of endodontists; p. 6. [Google Scholar]
- 29.Weine FS. The enigma of the lateral canal. Dent Clin North Am. 1984;28:833–52. [PubMed] [Google Scholar]
- 30.Kartal N, Ozçelik B, Cimilli H. Root canal morphology of maxillary premolars. J Endod. 1998;24:417–9. doi: 10.1016/S0099-2399(98)80024-1. [DOI] [PubMed] [Google Scholar]