

Abstract
Patient: Male, 53
Final Diagnosis: Gastric cancer
Symptoms: Abdominal and/or epigastric pain • vomiting • weigh loss
Medication: —
Clinical Procedure: Gastrectomy
Specialty: Surgery
Objective:
Unusual setting of medical care
Background:
Hypothyroidism is the second most common endocrine disorder following diabetes. Appropriate hormone replacement therapy is the cornerstone of its management and is typically in the form of oral preparations of levothyroxine. Intravenous replacement is a well-known alternative in patients who are unable to take medication orally for long periods. However, effective and safe alternatives to oral preparations of levothyroxine should be sought in the absence of the parenteral alternative. The aim of this report is to describe an alternative route for levothyroxine supplementation when the oral and parenteral routes are not available.
Case Report:
This study reports a hypothyroid patient with symptomatic malignant gastric outlet obstruction requiring surgery. However, the patient’s surgical condition precluded oral administration of levothyroxine and the parenteral alternative was unavailable. Hormone replacement therapy was administered rectally in the form of enemas in preparing the patient for surgery.
Conclusions:
Rectal administration of levothyroxine using enemas can be a safe and effective alternative for patients in whom administration via the oral route is not feasible, especially when parenteral formulas are unavailable.
MeSH Keywords: Enema, Hypothyroidism, Thyroxine
Background
Hypothyroidism is the most common thyroid disorder in adults. Its prevalence depends on sex, age, ethnicity, and environmental factors such as iodine intake status [1]. Its management is considered straightforward, as it is based on hormone replacement therapy. Synthetic levothyroxine (LT4) is currently the preferred drug for replacement therapy and is rapidly and consistently effective when administered orally [2]. Injectable preparations and rectal suppositories represent alternatives in conditions that preclude oral administration for long periods. Nevertheless, the treatment of hypothyroidism could be challenging, particularly in surgical patients when well recognized alternatives to oral LT4 are unavailable. To the best of our knowledge, this is the first case reported in the literature regarding the use of LT4 rectal enemas in an adult patient as an alternative to the oral preparations.
Case Report
Our patient was a 53-year-old man who has been on oral LT4 for hypothyroidism for the past 10 years. He presented to the outpatient clinic of an academic tertiary referral center in Northern Jordan with a history suggestive of long-term and progressive gastric outlet obstruction. He sought medical help for upper-abdominal pain and recurrent vomiting that became persistent in the past few days before admission. The patient was dehydrated, cachexic, and weak. He was admitted to the surgical ward for rehydration, nourishment, and a thorough work-up. Upper-endoscopy revealed a large ulcerating mass completely obstructing the pylorus and preventing further advancement of the scope. A biopsy was obtained and demonstrated a gastric adenocarcinoma. Staging computed tomography (CT) confirmed oncologic resectability. Nevertheless, of major concern in this patient was his hypothyroid status, which put him at significantly increased risk of cardiac and hemodynamic compromise at the time of major surgery. His thyroid function test on admission showed the following values: free T3: 1.25 pmol/L, free T4: 3.85 pmol/L, and TSH: 73.63 mIU/L. The laboratory reference intervals were 2.8–6.8 pmol/L, 12–22 pmol/L, and 0.270–4.640 mIU/L, respectively.
Due to the lack of parenteral preparations of LT4 in Jordan, these had to be ordered from abroad and required a minimum of 2 weeks to arrive. Rectal suppositories were also unavailable. Meanwhile, doubling and tripling the patient’s usual oral dose of 100 µg/day was attempted in the first week of his admission. However, it failed to provide any favorable response and his TSH level continued to rise. To prove malabsorption, a levothyroxine absorption test was performed. After an overnight fast, an oral dose of 1000 µg LT4 was given to the patient, who was monitored by a physician throughout the test. Blood samples were obtained prior to and at 2, 4, and 6 h following the bolus ingestion to investigate fT4 serum levels. However, there was no change in the fT4 level, indicating no absorption.
We then asked one of the gastroenterologists to try to pass a feeding tube into the duodenum under vision using the gastroscope, but that also failed. Therefore, rectal administration of LT4 via enemas was attempted after obtaining the patient’s informed consent. Initially (day 7 of admission), 300 µg of LT4 was ground and dissolved in 500 mL of normal saline and administered as a rectal enema at 6 A.M. fT4 levels were measured at 10 A.M. on the same day, but no response was noted. This amount of saline was used for convenience, as the 500-ml bottle of saline was readily available and the patient tolerated the enema very well. The following day, the dose was increased to 500 µg, but also with no effect. A dose of 1000 µg was given on days 9 through 12 of admission. This only resulted in a slight increase in the level of T4. Therefore, a double dose (2000 µg) was administered on days 13, 14, 15, 16, 17, and 18 and the patient responded appropriately. On day 18, free T3, free T4, and TSH levels were 2.76 pmol/L, 16.72 pmol/L, and 4.24 mIU/L, respectively. Figure 1 demonstrates the patient’s response to various doses of oral and rectal LT during the first 21 days of his admission.
Figure 1.
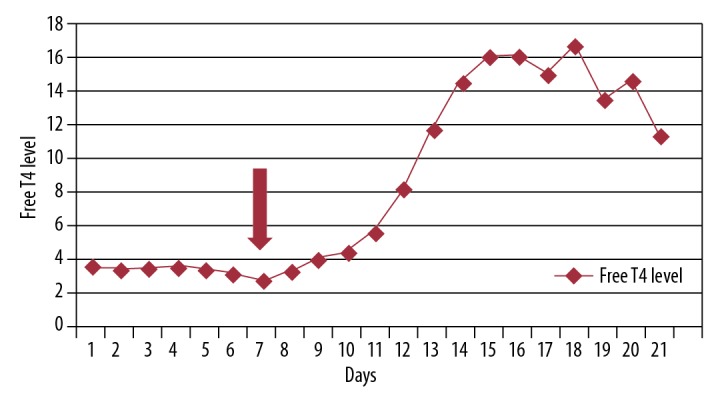
The chart represents the detailed patient response (T4 level) to various preparations and doses of levothyroxine (LT4). The arrow indicates commencement of rectal administration. Days 1–3: oral LT4 100 µg/day. Days 4 and 5: oral LT 200 µg/day. Days 6: oral LT 300 µg. Day 7: rectal LT 300 µg. Day 8: rectal LT 500 µg. Days 9–12: rectal LT 1000 µg/day. Days 13–18: rectal LT 2000 µg/day. Day 19 is the day of surgery.
On day 19, the patient underwent subtotal gastrectomy with Roux-en-Y gastrojejunostomy and tier 2 lymphadenectomy. By this time, the intravenous LT, ordered earlier, was received and was administered to the patient in the immediate postoperative period. The patient received 50 µg of IV thyroxine and his T4 was 14.72 and 11.33 pmol/L on postoperative days 1and 2, respectively. Unfortunately, the TSH was not available in our lab during that specific postoperative period, but we obtained a normal TSH level before surgery, as mentioned before.
Discussion
In an ironic twist, our patient, who had a condition whose treatment is typically straightforward (hypothyroidism), posed a great therapeutic challenge in the absence of well-recognized alternatives to oral LT4. Initially, higher oral doses were administered, similar to the trend followed in certain conditions [2,3]. However, this failed to achieve any response, most likely because the patient had a complete obstruction preventing the drug from reaching its site of absorption. The lack of injectable preparations led us to consider the rectal route. Most studies regarding rectal administration (typically in the form of suppositories) are from Japan, where injectable preparations of the drug are yet to be approved. The first reported reference on the use of rectal LT4 replacement therapy dates back to 1990 [4], in which the authors used rectal suppositories in an animal model and demonstrated that high doses, ranging between 31.25 µg/Kg and 62.5 µg/Kg, were required for an adequate response. A study evaluating the efficacy and pharmacokinetics of LT4 in human subjects with hypothyroidism demonstrated that LT4 suppositories had lower bioavailability and efficacy compared to oral LT4, even though T4 levels can be maintained in patients with hypothyroidism by administering LT4 suppositories at approximately twice the oral dose [5]. The lower bioavailability of rectal LT4 compared to its oral counterpart has been attributed to the low level of release LT4 in the rectum [6]. The rectal route seemed appealing, but LT4 suppositories were also not available. Rectal enemas were administered instead, as the effectiveness and safety of this preparation has been reported in an infant with short bowel syndrome [7]. Furthermore, the comparability of the therapeutic effectiveness of antithyroid drugs as enemas to suppositories, with a higher bioavailability in favor of enemas, was encouraging [8]. Initially, we administered rectal enemas within the range of twice the oral dose. However, the lack of an adequate response eventually led us to use the dose range used in the animal study mentioned earlier. A dose of 40 µg/Kg (2000 µg) administered on days 13 through 18 achieved a biochemically and clinically adequate response (Figure 1). The high dose required to achieve euthyroid status in our patient may have been caused by the limited time for which the patient could hold the enema before needing to defecate. This alternative route and method of administration, despite being potentially inconvenient to patients, was safe and effective. Furthermore, it was less costly when compared to the injectable preparation and required no aseptic handling or specialized preparation methods.
Conclusions
In conclusion, rectal enemas of LT4 at high doses can be a useful, safe, and effective alternative to oral LT4 in conditions precluding oral administration, particularly when well-recognized alternatives to oral preparations are not available. This report provides an alternative for the parenteral levothyroxine supplementation when the oral route is not possible, especially in less developed countries. It may also advocate for increased availability of rectal levothyroxine preparations worldwide.
Abbreviations:
- LT4
levothyroxine;
- TSH
thyroid stimulating hormone;
- T3
Triiodothyronine;
- T4
thyroxine
Footnotes
Conflicts of interest
None.
References:
- 1.Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39–51. doi: 10.1093/bmb/ldr030. [DOI] [PubMed] [Google Scholar]
- 2.Wiersinga WM. Thyroid hormone replacement therapy. Horm Res. 2001;56(Suppl. 1):74–81. doi: 10.1159/000048140. [DOI] [PubMed] [Google Scholar]
- 3.Formenti AM, Daffini L, Pirola I, et al. Liquid levothyroxine and its potential use. Hormones (Athens) 2015;14:183–89. doi: 10.14310/horm.2002.1579. [DOI] [PubMed] [Google Scholar]
- 4.Yamamoto M, Yonezawa K, Mizugaki M, et al. Replacement of L-T4 suppository in MMI treated rabbits. Endocrinol Jpn. 1990;37:355–59. doi: 10.1507/endocrj1954.37.355. [DOI] [PubMed] [Google Scholar]
- 5.Kashiwagura Y, Uchida S, Tanaka S, et al. Clinical efficacy and pharmacokinetics of levothyroxine suppository in patients with hypothyroidism. Biol Pharm Bull. 2014;37:666–70. doi: 10.1248/bpb.b13-00998. [DOI] [PubMed] [Google Scholar]
- 6.Hamada Y, Masuda Pharmaceutical studies of levothyroxine sodium hydrate suppository provided as a hospital preparation. Biol Pharm Bull. 2015;38:625–28. doi: 10.1248/bpb.b14-00721. [DOI] [PubMed] [Google Scholar]
- 7.Ybarra M, Pinheiro C, Setian N, et al. Rectal diluted levothyroxine for the treatment of neonatal hypothyroidism: An alternative route of administration. ESPE Abstracts. 2015 84 P-31211. [Google Scholar]
- 8.Jongjaroenprasert W, Akarawut W, Chantasart D, et al. Rectal administration of propylthiouracil in hyperthyroid patients: Comparison of suspension enema and suppository form. Thyroid. 2002;12:627–31. doi: 10.1089/105072502320288500. [DOI] [PubMed] [Google Scholar]