

Abstract
Background
The incidence of melanoma and non‐melanoma skin cancer is continuing to increase worldwide, with sun exposure serving as the primary external aetiologic force in its development. Despite noticeable public health efforts, there continue to be gaps in public awareness and primary and secondary prevention mechanisms. This survey study sought to investigate preventative behaviours regarding sun exposure and skin cancer detection at an international scale.
Methods
A questionnaire was submitted, both online and by telephone, to a representative sample (based on official demographic statistics on gender, age and region) of people aged from 15 to 65 originating from 23 countries. Questions dealt with demographics, sun exposure and protection, risk knowledge, self‐examination, medical advice seeking. Data were then gathered and analysed at different levels.
Results
A total of 19 569 respondents were recruited. Overall, sunscreen and sunglasses were the most used measures for sun protection. There were however difference between countries and geographical areas. Some high‐risk countries in terms of sun exposure (according to their location to Equator) exhibited higher rates of primary preventative behaviours, in particular Australia, Chile and Greece. There were also discrepancies between countries regarding secondary prevention through self‐examination and medical advice seeking. Young people, men, individuals belonging to a lower socio‐economic class or having a lower education level were all least likely to know or follow primary and secondary preventive measures.
Conclusion
We found imperfections and geographical inequality both regarding primary and secondary prevention of skin cancer. Our study provides insights that could help to target populations more effectively through information campaigns embedded into the global needed endeavour aiming to reduce mid‐ and long‐term development of skin cancer.
Introduction
The growing incidence of melanoma is unparalleled to that of other solid tumours. About 232 000 new cases of melanoma are diagnosed worldwide each year, according to the World Health Organization.1 Even though substantial progress has recently been made in the development of targeted therapies,2, 3 the prognosis remains poor in most patients with advanced disease and the annual global mortality has reached the unprecedented number of 55 000 deaths per year.1 Furthermore, each year there are more new cases of skin cancer than the combined incidence of cancers of the breast, prostate, lung and colon and the most recent study estimated that in US in 2012, 5.4 million cases were diagnosed among 3.3 million people.1 Although multiple genetic and phenotypic risk factors have been documented throughout the literature, the main causal factor remains sun exposure, in particular, ultraviolet (UV) radiation. UV radiation has been shown to exert a direct mutagenic effect, highlighting its role in melanoma pathogenesis.4 Individuals with lighter skin type undergoing intense but intermittent sun exposure are particularly vulnerable and at risk of melanoma development.5 Despite the reasonable body of knowledge regarding risk factors and causal mechanisms of cutaneous melanoma, behavioural preventative measures have proven hard to implement in wide populations and evidence is mixed as to whether sun avoidance campaigns have actually reduced risk. Therefore, a greater insight regarding sun exposure and skin cancer prevention is still needed so as to understand any failure in preventative behaviours and to consequently adapt communication to populations with the ultimate goal of reducing delayed development of cutaneous melanoma.
Our research objective was to conduct an international survey to study global sun exposure and prevention behaviours regarding skin cancer.
Methods
An international survey was launched from 3 December 2014 through 8 January 2015. The study encompassed 23 countries and was conducted online except for Russia (face‐to‐face interviews) and Brazil, Mexico and Greece (telephone interviews). The sample of survey included men and women between 15 and 65. Except for age limits, in each country, those surveyed were selected to serve as a representative sample of their national population (quotas based on official demographic statistics on gender, age and region). People invited were selected based on demographic information linked to their identification details as members of Ipsos Interactive Services proprietary online access panel. Their selection also takes into account their recorded likeliness of participation and eligibility based on exclusion criteria such as limits on the number of surveys one panellist is entitled to participate in every month. This automatic selection procedure is conducted with the Samplix software which allows to e‐mail invites to a preliminary sample whose composition assures a final sample that fits the quotas defined above. The response rate variations across demographics (the overall sample's response rate was 24%) were taken into account by Samplix so as to assure demographic quotas could be met. The questionnaire collected data regarding demographics, sun exposure, behaviours regarding prevention and tanning, risk knowledge, self‐examination, medical advice seeking and social attitude (Appendix S1).
Data from interviews were gathered and analysed according to the following variables: geographical area, country, age, gender, socio‐economic status, degree of education, parental status, outdoor occupation, phototype (according to Fitzpatrick classification). Chi‐squared tests of independence were used to examine the relation between attitudes and demographic characteristics of the population. All tests were two‐sided at 0.01 significance level, and all analyses have been performed using IBM SPSS Statistics software version 21.
Results
Nineteen thousand five hundred and sixty‐nine people returned a properly completed questionnaire. Details of respondents according to their geographical area of origin are shown in Table 1.
Table 1.
Mapping of participants
| Sample: 19 569 interviews | |
|---|---|
| Country | Number of interviews |
| Denmark | 502 |
| Finland | 502 |
| Norway | 500 |
| Sweden | 500 |
| Austria | 500 |
| Belgium | 500 |
| France | 1005 |
| Germany | 1002 |
| Ireland | 1000 |
| Switzerland | 502 |
| UK | 1002 |
| Greece | 1001 |
| Italy | 1005 |
| Portugal | 1030 |
| Spain | 1001 |
| Poland | 1004 |
| Russia | 1005 |
| Canada | 1005 |
| USA | 1000 |
| Brazil | 1000 |
| Chile | 1002 |
| Mexico | 1000 |
| Australia | 1001 |
| Gender | Number of interviews |
|---|---|
| Male | 9715 |
| Female | 9854 |
| Age | Number of interviews |
|---|---|
| 15–19 | 1510 |
| 20–24 | 2155 |
| 25–34 | 3974 |
| 35–44 | 4146 |
| 45–54 | 3998 |
| 55–65 | 3786 |
| Occupation | Number of interviews |
|---|---|
| Managers and professionals | 3487 |
| Technicians, clerks, service workers | 5152 |
| Workers, elementary occupation | 3751 |
| Inactive/unemployed | 7047 |
General findings for preventative measures
Overall, the use of sunscreens and wearing sunglasses were the most frequent preventative measures utilized: 59% always or often put sunscreen on the parts of their bodies exposed to the sun (arms, legs, etc) and 57% on their face. The use of protective clothes (19%) and wearing a hat/cap (38%) were far less cited by respondents. Applying sunscreen to children under 12 was the most common sun‐protection behaviour (cited by 87% of parents of children aged under 12). More detailed data are presented in Fig. 1.
Figure 1.
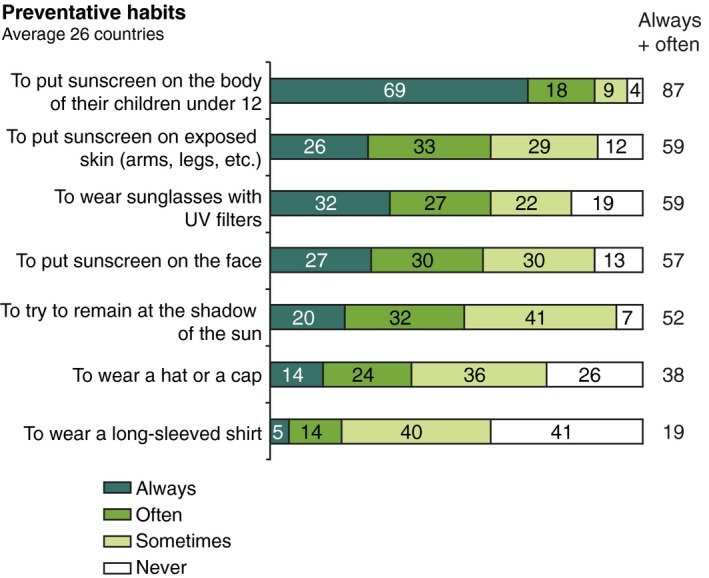
Response data regarding preventative behaviours.
Geographical comparisons regarding protection
When comparing countries and geographical areas (continents and subcontinents) for sunscreen use, inhabitants of countries in Southern and Western Europe were particularly more likely than the average of overall respondents to protect the face (66% for Southern Europe; χ2 = 111.69, df = 1, P < 0.001, and 63% for Western Europe; χ2 = 63.68, df = 1, P < 0.001, compared to 57% on average for the total of 23 countries) and their body (66% for Southern Europe; χ2 = 68.44, df = 1, P < 0.001, and 68% for Western Europe; χ2 = 146.38, df = 1, P < 0.001, compared to 60% on average for the 23 countries).1 In Latin America, avoidance of the sun was much more common (73% always or often try to stay in the shade compared to 52% on average; χ2 = 420.09, df = 1, P < 0.001). Respondents from Australia exhibited a more diverse set of protective behaviours, resorting more than the average to less common behaviours like trying to stay in the shade (72% compared to 52% on average; χ2 = 152.91, df = 1, P < 0.001), wearing a hat/cap (58% compared to 38% on average; χ2 = 160.16, df = 1, P < 0.001) or wearing protecting clothing (33% compared to 19% on average; χ2 = 118.07, df = 1, P < 0.001). Moreover, geographical areas at higher risk of sun exposure such as Southern Europe and Australia were associated with more systematic protection: inhabitants of these countries were indeed more likely to protect themselves from the sun even if they were out for a short time – <1 h – (43% of Southern Europeans and 40% of Australians compared to 31% on average, respectively, χ2 = 217.79 and χ2 = 35.79, df = 1, P < 0.001). Education level as well as gender and skin type influenced the degree of sun prevention: among those who declared they protected themselves more than the average were people with a high level of education who said they protect themselves from the sun even when out for a very short time (33% compared to 31%; χ2 = 22.65, df = 1, P = 0.002); women (36%;χ2 = 74.48, df = 1, P < 0.001), and people with skin type 1 (50%; χ2 = 207.24, df = 1, P < 0.001).
State of knowledge
Overall, the level of knowledge regarding risks associated with sun exposure and regarding early signs of skin cancer was thought to be high. Respondents assigned more weight to current behaviour as compared with past behaviour, skin type and state of skin regarding nevi (88% thought it was linked to a lack of protection during sun exposure and 81% to the regular use of tanning beds compared to 68% for the fairness of the skin or 72% for the number and size of moles). Women appeared to be slightly better informed (for example, 78% of women knew the risk was linked with the level of exposure during childhood/adolescence compared to 75% on average; χ2 = 32.34, df = 1, P < 0.001).
Also, the level of information increased with age, socio‐economic status and education level: the same risk factor (exposure during childhood) was for example better identified by people aged 45 and over (77% compared to 75%; χ2 = 11.93, df = 1, P = 0.001), by managers and professionals 6 (78%; χ2 = 14.38, df = 1, P < 0.001) or people with a high level of education (79%; χ2 = 26.87, df = 1 P < 0.001).
When comparing between countries regarding the level of knowledge, Australia, Ireland, Brazil and Greece were remarkably more informed than the others surveyed, both regarding risks and early signs of skin cancer. Confronted with six risk factors of skin cancer (level of exposure to the sun during childhood or adolescence, history of severe sunburn during childhood or adolescence, lack of protection during exposure to the sun, fairness of the skin, number and size of moles and regular use of tanning beds), 50% of Australians demonstrated a higher level of knowledge (knowledge of at least five risks out of six), as well as 45% of Irish people and 52% of Greek citizens (compared to 36% on average for the 23 countries, respectively, χ2 = 80.36, χ2 = 33.27 and χ2 = 104.85, df = 1, P < 0.001). Conversely, the representative subjects from Mexico, Russia and Italy were among the least informed, with only 26% of Mexican participants exhibiting a high level of knowledge on risk factors (compared to 36% on average for the 23 countries; χ2 = 41.54, df = 1, P < 0.001), and 14% of Russian and 16% of Italian participants (respectively, χ2 = 203.57 and χ2 = 168.02, df = 1, P < 0.001 versus the result obtained for the total of the 23 countries). Other data regarding state of knowledge are presented in Figs 2 and 3.
Figure 2.
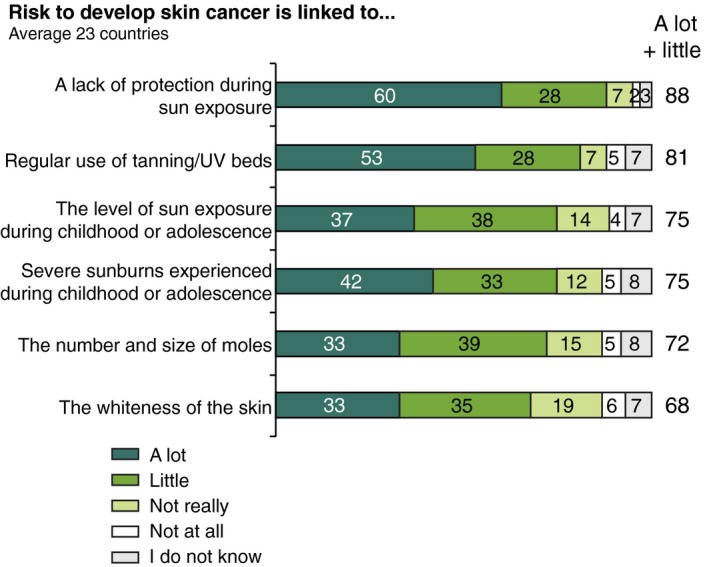
Response data regarding risk knowledge.
Figure 3.
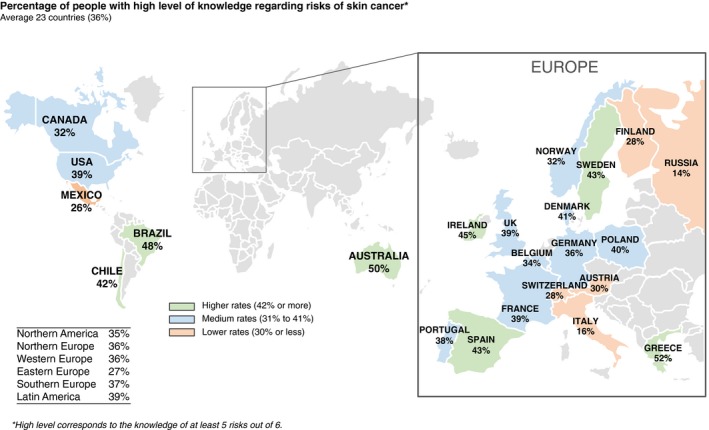
Geographical data regarding risk knowledge of skin cancer.
Self‐examination and medical advice seeking
Overall, the level of skin screening, whether through self‐examination or by a dermatologist, was often found to be insufficient compared to medical recommendations, that is once a month for self‐examinations and once a year by a dermatologist. Women were more likely to proceed with self‐examination (78% had already self‐checked their moles compared to 69% of men; χ2 = 203.60, df = 1, P < 0.001). Self‐examination also increased with age. The proportion of patients resorting to self‐check was slightly higher than the average for people aged 55‐65: 79% for a self‐check compared to 74% (χ2 = 40.90, df = 1, P < 0.001).
Self‐examination and consultation with a dermatologist were positively correlated with socio‐economic status and education level as well: for example, 51% of managers and professionals already had their moles checked by a dermatologist at least once in their life (compared to 48% on average; χ2 = 10.67, df = 1, P = 0.001), with a similar trend seen of 52% of participants who recorded having undertaken a higher level of education (χ2 = 34.97, df = 1, P < 0.001). Skin type was also significantly associated with this screening measure, with 50% of those associating themselves as skin types I and II already having been seen by a dermatologist check for skin cancer screening (compared to 48%, the average percentage obtained for the 23 countries; χ2 = 8.83, df = 1, P = 0.003).
When comparing geographical areas regarding cancer screening, again Australia and Southern Europe exhibited higher rates of preventative behaviour than the average: 82% of Australians and 84% of those from Southern Europe reporting prior self‐checks of their moles (compared to 74% on average, respectively, χ2 = 31.99 and χ2 = 181.98, df = 1, P < 0.001). The complete data are presented in Fig. 4.
Figure 4.
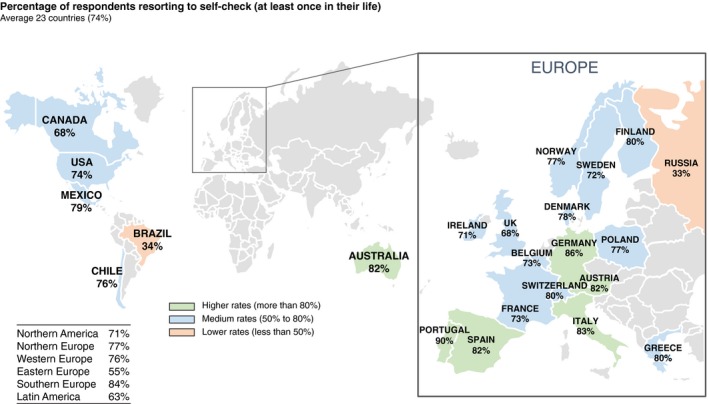
Geographical data of respondents resorting to self‐check.
Discussion
In the current study, we found that in general, the surveyed populations were aware of risks related to sun exposure but that primary prevention suffered from imperfections and inequality between countries. Moreover, individual risk factors (skin type and number and size of moles) were overall not well known by respondents. Lastly, self‐examination and medical seeking is frequently underused and early signs of skin cancer that should prompt medical consultation are not universally known based on our finding. Women, in general, also were found to be overall more knowledgeable then men regarding the aforementioned risk factors as well as utilized the appropriate measures and resources to prevent and monitor for skin cancer. This finding is consistent with past studies7 and even more recently a survey study conducted by the American Academy of Dermatology. (http://www.aad.org).
The current survey raises several issues worth considering regarding primary and secondary prevention of melanoma and non‐melanoma skin cancer at a global scale. The practice of primary prevention related to sun protection can be improved. Sun avoidance through seeking shade and protecting clothes was often not a first‐line option for many respondents despite their well‐known impact, in congruence with past large, although regional, population‐based surveys.8 Interestingly, even with the expansion of this study to include multiple countries throughout the world, similar behaviours and demographic‐based differences were still noted. However, even though the most at‐risk geographical areas seemed to be associated with greater protective activity, some discrepancies persisted and social and educational factors likely contributed to these deficits in specific populations (populations with a low education level, workers and elementary occupations), thereby highlighting the need for targeted campaigns for specific demographics. When specifically examining the state of knowledge, we also measured differences between locations of respondents and among subpopulations according to gender and age. Those insights suggest that awareness campaign could be intensified in some countries and (or) tailored to specific populations that seemed to be less informed. Similar differences were also observed regarding secondary prevention. Our findings indicate that self‐examination and medical advice seeking should be encouraged, in particular in areas where they were found to be less common. From these data, there is a clear and continued need to disseminate education on identifying early signs of melanoma as prognosis is still inversely correlated to the stage of disease. Haluza et al.9 reported that patients/consumers identify print media and television as the two most relevant sources for skin health information, with physicians ranking third to these outlets. Yet, when information was received from a physician, there was a significant increase in the participants’ skin health knowledge and sun‐protective behaviour, highlighting the importance of the print and digital media to encourage the public to seek out information from medical professionals.
This study has several strengths. First, it is an international global survey conducted in 23 countries with a very large study sample. Second, respondents were not selected on the basis of a condition or a predefined behaviour. Included subjects were selected as a means to create representative cohorts of the general population. Third, the surveying technique was quite homogenous, mostly conducted online with very few exceptions. Fourth, the period of study was very short, thereby reducing the risk of behavioural change along the time elapsed between the start and the closure of the survey. Lastly, the questionnaire addressed most facets of skin cancer prevention, in particular primary prevention regarding sun exposure and secondary prevention related to self‐examination and seeking medical consultation.
Nevertheless, this study has some limitations. First, like any survey of this type, there is a possibility of selection bias. However, quota method is likely to reduce this risk. Secondly, as the study is based on self‐reported data, one cannot exclude some conformism, that is socially acceptable answers with regard to rational protection behaviours. Finally, in this article, low‐ and high‐risk areas are defined at a country level, according to their location to equator as the exact geolocation of each respondent was not available. A further limitation is the lack of controlling for jobs where sun exposure is generally high (e.g. blue collar occupations) as occupations were not used as quotas. Furthermore, concerns regarding the reliability or consistency of survey based studies have been raised.10 Questions focusing on proactive sun‐protective behaviours and descriptive questions on perceptions/knowledge were deemed the most reliable, which was the focus of the survey utilized in our study. Nevertheless, scales used in the questionnaire have not yet been validated.
In conclusion, the current survey provides new insights regarding global adherence and education on primary and secondary prevention of skin cancer. Even though some of the documented trends are thought to be encouraging, discrepancies between countries were observed and deficits still measured. Our data suggest that messaging needs to be specifically targeted for at‐risk demographics (especially by age, gender, skin type and country). The importance of using sunscreen as an adjunct to the primary sun‐protective (i.e. protective clothing) method rather than instead of it needs to be included in future health promotion campaigns. Educational campaigns will both need to be regularly updated and utilize outlets used by the most at‐risk groups including young individuals, men and individuals belonging to a lower socio‐economic class or having a lower education level.
Supporting information
Appendix S1. Questionnaire used in this survey.
Acknowledgements
The authors wish to thank all the subjects that took time to participate to the current survey and Ipsos Public Affairs, France, the monitoring centre in this survey.
Conflicts of interest
S. Seité and D. Moyal are employees of La Roche‐Posay Dermatological Laboratories, Asnières, France.
Funding Source
This study was funded by La Roche‐Posay Dermatological Laboratories, Asnières, France.
The copyright line for this article was changed on 27 July 2018 after original online publication.
Note
For regional analysis, countries were aggregated as follows: Northern Europe (includes Denmark, Finland, Norway and Sweden), Western Europe (includes Austria, Belgium, France, Germany, Ireland, Switzerland and UK), Southern Europe (Greece, Italy, Portugal and Spain), Eastern Europe (Poland and Russia), North America (includes Canada and USA), Latin America (Mexico, Brazil and Chile).
References
- 1. American Cancer Society . Cancer facts and figures 2016. URL http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-047079.pdf (last accessed: 17 March 2016).
- 2. Postow MA, Chesney J, Pavlick AC et al Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med 2015; 372: 2006–2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Larkin J, Hodi FS, Wolchok JD. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med 2015; 373: 1270–1271. [DOI] [PubMed] [Google Scholar]
- 4. Hodis E, Watson IR, Kryukov GV et al A landscape of driver mutations in melanoma. Cell 2012; 150: 251–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Erdmann F, Lortet‐Tieulent J, Schüz J et al International trends in the incidence of malignant melanoma 1953–2008‐are recent generations at higher or lower risk? Int J Cancer 2013; 132: 385–400. [DOI] [PubMed] [Google Scholar]
- 6. International Labour Organization 2008. ISCO International Standard Classification of Occupations. Retrieved from http://www.ilo.org/public/english/bureau/stat/isco/isco08/index.htm
- 7. Alberg AJ, Herbst RM, Genkinger JM, Duszynski KR. Knowledge, attitudes, and behaviors towards skin cancer in Maryland youths. J Adolesc Health 2002; 31: 372–377. [DOI] [PubMed] [Google Scholar]
- 8. Stanton WR, Janda M, Baade PD, Anderson P. Primary prevention of skin cancer: a review of sun protection in Australia and internationally. Health Promot Int 2004; 19: 369–378. [DOI] [PubMed] [Google Scholar]
- 9. Haluza D, Schwab M, Simic S, Cervinka R, Moshammer H. Perceived relevance of educative information on public (skin) health: results of a representative, population‐based telephone survey. Int J Environ Res Public Health 2015; 12: 14260–14274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bränström R, Kristjansson S, Ullen H, Brandberg Y. Stability of questionnaire items measuring behaviours, attitudes and stages of change related to sun exposure. Melanoma Res 2002; 12: 513–519. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Questionnaire used in this survey.