

Abstract
Background:
The number of HIV cases in Iran is increasing. Knowledge of the changing epidemiology of HIV is fundamental for service planning and prevention activities. This study aims to estimate the number of HIV-infected cases by the capture and recapture method for size estimation.
Materials and Methods:
From 2002 to 2009, we used three different centers – hospitals, the Voluntary Counseling and Testing (VCT) center, and a central prison in Fars Province for data retrieval. The overlaps between these centers were investigated to determine the true estimate of HIV cases. Finally, interactions were analyzed by a linear logarithm model with STATA version 9 software.
Results:
We observed 5167 HIV cases. The number of males was ten times more than that of females. The most frequent age range was between 15 and 44 years. The majority of cases (n = 3347) were retrieved from the VCT center. The least number of infected persons were located in the prison and hospitals. The estimated number of cases in Fars Province was 14,925 from 2002 to 2009. The best model consisted of three sources.
Conclusion:
Covering the system of medicine deputy for registering the number of infected cases with HIV is poor in Iran. Improvements in making arrangements for enhancing the quality of data related to HIV-infected cases are essential for solving this problem and must be on the agenda for medical policymaking.
Key words: Capture and recapture, human immunodeficiency virus, Iran
INTRODUCTION
Until the end of 2011, there were approximately 34 million people worldwide infected with HIV; however, the epidemic load varies among countries.[1] Currently, according to a WHO report, the prevalence rate of HIV/AIDS in Iran has risen from low to concentrated.[2] It is predicted that HIV/AIDS will be the third cause of death and the first cause for lost years of life in countries that have low-to-average income until 2030.[3] Knowledge about the epidemiological properties of this disease and process of changes for adequate planning and investigating the effect of preventive plans and fundamental policymaking is essential. Despite numerous efforts for perceiving the worldwide epidemiology of HIV, the Middle East and North Africa are regions in which the knowledge of epidemiology and its changing process is limited.[3]
The number of HIV cases in Iran is increasing. The WHO has emphasized the importance of HIV prediction and identification of the process at risk groups.[4,5] Despite the increased incidence of HIV infection, numerous countries such as Iran do not have a clear picture of the prevalence of HIV. Mostly, this is attributed to various problems faced by the care system.[6]
Numerous efforts have been made to identify the epidemiology of HIV in Iran. In a study which investigated the epidemiology of HIV, it was determined that the number of infected cases increased from 1.38/100,000 cases in 1997 to 4.6/100,000 in 2004.[7] In addition, in a recent study, it was shown that the estimated number of HIV-infected people were 89,000 in 2009 with a projected increase to 106,000 in 2014.[8]
There are different methods for identifying the number of underestimated cases and calculating the number of infected cases. Various studies have used the capture and recapture method for size estimation.[9,10] The capture and recapture method labels a sample population which is subsequently released. At a later time, another sample is recaptured, and the number of cases in each sample and common cases in both samples are taken into consideration.[11]
In this study, we used three sources. It has been suggested that prisons have essential roles in the HIV epidemic, and outbreaks among Iranian prisoners are significant as 74% of HIV-infected individuals in Iran are prisoners.[12] Key populations at higher risk of HIV also refer to the Voluntary Counseling and Testing (VCT) center.[13] In addition, hospitals are efficient, practical settings for HIV testing.[3]
Various comprehensive studies have not yet estimated the number of HIV cases in Iran by capture–recapture method. Therefore, in this study, we aimed to estimate the number of HIV cases using this method and determine the process of changes.
MATERIALS AND METHODS
This study was performed in Fars Province, Shiraz City, South Iran, a large area with a population of 4,336,878. We have used the capture and recapture method which evaluates the completeness of registries and estimates the true incidence rates of diseases, particularly those with stigma. This method has been extensively applied in health research for the estimation of various disease rates in populations.[14]
Three data sources were selected to use the capture–recapture method and to estimate the true number of HIV cases. Because we needed at least three independent data sources to apply the capture–recapture method, we used data from the VCT and two additional independent data sources that accounted for HIV in the Fars Province. The additional sources included the central prisons' data and follow-up of the hospital records. The subsequent paragraph describes the three data sources in detail. We determined that 2002–2009 was a stable time frame for these selected sources. Sources with available data before or after this time were not included in this analysis.
Hospitals
First, referral centers with high numbers of HIV-infected cases were selected. Among the state hospitals, most referable of them and the semi-private hospitals allowed us to access their data, whereas other hospitals declared that the proper data were not available. The private hospitals that report these data to the educational deputy did not agree to cooperate. On the other hand, patients referred to hospitals for numerous reasons; those who have been identified by medical personnel as having potentially high-risk behavior were sent for HIV testing which was performed by an ELISA test. In these data banks, the list of patients who were HIV positive was extracted. Next, their files were investigated and the diagnosis was recorded. Because these patients were diagnosed solely by the ELISA test, we conducted phone calls to the patients to inquire about their diagnoses for confirmation. In addition, patients were requested to refer to the HIV Research Centers at Shiraz University of Medical Sciences to undergo additional testing for confirmation of the HIV diagnosis. Initially, approximately 224 patients entered the hospital. After making contact with the patients and their families to request additional examinations, there were 71% of these patients who were eligible to enter the hospital sources. The remaining cases were eliminated because they were only diagnosed by the ELISA test with the possibility of a mistaken diagnosis, they had expired, or they refused to give blood samples for additional HIV testing.
Central prison
Another source expected to have a large number of HIV-infected patients was the central prison, Adel Abad, of Fars Province. Adel Abad is a general public prison composed of four wards, each with several rooms. There are separate female and male wards. In each ward, approximately 1000 people with various criminal records are incarcerated. Prisoners are considered to be one of the high-risk groups for HIV in Iran. In this prison, we have found a considerable number of HIV-positive cases which were not recorded in other sources.
Voluntary counseling and testing center
The VCT center has several goals that include prevention of HIV/AIDS transmission, decreasing HIV-related stigma and discrimination, and case finding. This center is under the control of Shiraz University of Medical Sciences which offers free services for patients at high-risk behavior. It is presumed that numerous at-risk patients such as injecting drug users refer to this center for voluntary testing. On the other hand, other sources such as hospitals, blood transmission center, caring centers, harm reduction center, and methadone maintenance therapy centers were used. Hence, VCT center was expected to be the most comprehensive source.
Data analysis
Following the elimination of duplicates in each of the three data sources and patients who resided outside of the Fars Province, we performed a data linkage using the Microsoft Office Excel. The criteria for linkage were sharing six variables including names, family name, father's name, age, date of birth, and place of residence. The combination of the variables was used to define a unique identifier for every patients in statistical analyses.
Capture–recapture method and log-linear modeling were used to estimate HIV-infected patients in the Fars Province. Observed numbers of HIV from the three data sources were included separately and jointly in the log-linear model. Dependency on the data sources was modeled by adding the interaction terms to the log-linear model. We estimated confidence intervals (CIs) for the estimated number of cases through the profile likelihood method. Overall, we ran eight models for our statistical analyses. Akaike information criterion (AIC) and Bayesian information criterion (BIC) were used for the model selection. For the log-linear model, the value for this criterion was AIC and BIC. The model with the smallest AIC and BIC was selected as the optimal model for our estimation.[15,16] The use of the capture–recapture method requires two or three data sources. Since we used log-linear model for our statistical analyses, it is not crucial to use independent data sources. In this analysis, STATA version 9 (StataCorp, Texas, USA) was used. Trend of HIV-infected cases was depicted to investigate time-trend changes.
RESULTS
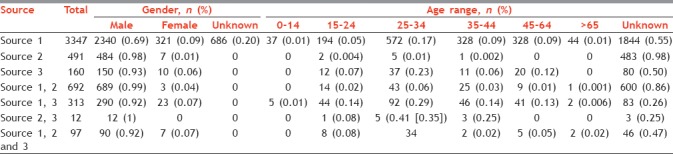
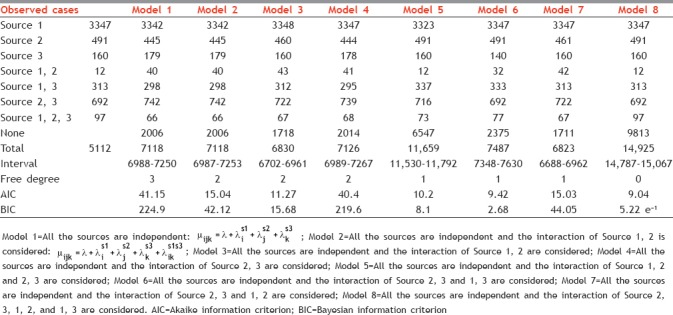
Finally, by omitting repetitive cases and combining cases from the three sources, we analyzed 5112 cases. The number of males was ten times more than the number of females. The most frequent age range was 25–35 years. The ages of more than half of the cases were unknown. Most (3347) were found in the VCT and the least, as expected, were common cases in the prison and hospitals. [Table 1] The number of recorded cases in prison was twice the number of cases in the hospitals. The prison was considered to be the center with the most at-risk cases. In van graph, the manner of overlapping the sources and the number of cases in each source is shown [Graph 1]. We performed data analysis of the three sources with the log-linear model [Table 2]. The lowest frequency was related to the common cases between the prison and hospitals (Model 4) whereas the highest frequency was attributed to the existence of cases in all the three sources (Model 8). This model simultaneously investigated the VCT center, the hospital, prisons, and interactions between them (Model 8) showed the highest frequency and was selected as the best model because it had the lowest AIC (9.04) and BIC (5.22) e−1 criteria. On the other hand, in this model, the coefficients were significant in all the three sources with P < 0.05. Thus, the number of HIV-infected cases in Fars Province was estimated to be 14,925 (95% CI: 14787–15067) from 2002 to 2009 [Table 2]. According to the data, the most recorded cases were detected in 2007 and the least in 2004. The trend for increases and decreases in estimated and recorded data throughout Iran and Fars Province were approximately the same. Although not expected, from 2004, the cases reported in Iran were less than the estimated cases in Fars Province [Graph 2].
Table 1.
The characteristics of patients with HIV between 1991 and 2010 which was reported by the consultation center (Source 1), prison (Source 2), and hospitals (Source 3)
Graph 1.
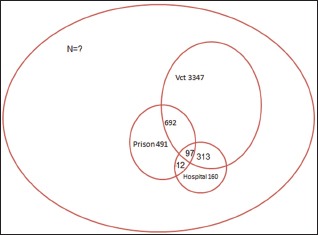
Van graph, the number of recorded cases with HIV in Fars Province from 1991 to 2010 which was recorded in three sources of consultation center of behavioral disorders, hospitals, and prison
Table 2.
Estimating the number of HIV-infected cases from 1991 to 2010 in Fars Province by capture and recapture model with three sources
Graph 2.
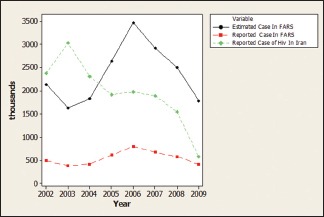
Comparison of reported and estimated cases with HIV/AIDS in Fars Province and the statistics of the Ministry of Health
DISCUSSION
We used the capture and recapture method and determined that the current HIV registry has underestimated the true number of HIV-infected people by approximately 67% in Fars Province, Iran. The capture and recapture method is an established validation tool widely used for the estimation of different disease rates. One of the issues that needed to be considered was improving the registration and caring system for HIV, and correcting this issue can help the medical officials.[17]
Estimating the hidden population is difficult; however, these types of statistics and data are important for planning. The data are useful for the establishment of medical policies.[17] Numerous methods are available that have the capability to solve this problem; the most important are the capture and recapture method, multiplier method, and networks scale-up.[18] Worldwide, the capture and recapture method has been used to estimate the number of HIV-infected cases. For example, according to a Bangkok study where the number of HIV-infected injecting drug users was estimated by two sourced analysis, using the capture and recapture model was appropriate.[19] In Italy, the number of HIV-infected cases was estimated by four sources and in France by three sources.[20,21]
In the current study, we found that the estimated number of HIV-infected cases in Fars Province was more than that reported by the Ministry of Health of the Islamic Republic of Iran (IR). In 2010, there were 22,000 HIV-infected cases, of which 4000 were residents of Fars Province.[8] In addition, the estimate derived in the current study was similar to that of the UNAIDS data. According to the UNAIDS, the number of HIV-infected cases was 80,000 which was four times the number of recorded cases by the Ministry of Medicine.[1] In this study, we considered the total number of estimated cases (15,000) in Fars Province to the total number of actual registered cases (5000) in a comparison with the UNAIDS estimate to Iran registered cases (80,000–22,000) which is nearly the same.[1] Therefore, we approved the validity of the obtained estimates.
On the other hand, we know that the caring system for HIV is limited in Iran. Therefore, the reported information may be incomplete. In Iran, there are a few studies which estimate the number of HIV-infected cases. According to the Modes of Transmission (MOT) study, it has been suggested the number of infected people with HIV was 89,000 and 106,000 for 2009 and 2014, respectively;[8] this was in concordance with our estimation [Graph 2] which has suggested a discrepancy in recording. It is not possible for the number of registered cases in Iran to be less than the reported cases from one province in this country. Therefore, the HIV registration system in Iran has a serious problem and should be modified.
Totally, a few HIV-infected cases have been diagnosed because of the long-term hidden period of HIV infection, discrimination between the patients, taboo, and the accessibility to the people who are the high risk behavior is not easy.[12]
According to a report by the Ministry of Health of the IR, the most frequent age range of infected cases was 25–34 years,[8] which confirmed the results of the current study.
One of the issues related to the recording of HIV-infected patients was that numerous cases in hospitals, consultation centers, or blood transmission centers were diagnosed as infected cases. These patients have been ignored in this system. The only information from these patients were codes from which their identification was not possible, which could have damaged both the society and patients. It is essential to have detailed information and principles for recording and determining the number of infected cases in Iran.
One of the most important limitations of this study is the limitation in collecting detailed information. However, for the capture and recapture model, a sample for estimation will suffice. Thus, the use of this method does not contradict the lack of information. The caring system faces different problems such as improper reporting and unavailability of complete information among other issues. To solve this problem, specific forms can be used for all health centers, prisons, and blood transmission centers so that everyone can use common variables for reporting. On the other hand, sending this form to caring centers for behavioral disorders, which are the major centers for data collection of HIV patients, will be appropriate for gathering patient data. In addition, it is essential to make the system uniform to follow the patients' conditions.
CONCLUSION
Covering the system of medicine deputy for registering the number of infected cases with HIV is poor in Iran. Improvements in making arrangements for enhancing the quality of data related to HIV-infected cases are essential for solving this problem and must be on the agenda for medical policymaking. it is essential to make the system uniform to follow the patients' conditions. Further research are needed for more clarification
Financial support and sponsorship
This project was founded by HIV/AIDS Research Center, Shiraz University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors wish to thank the staff of the central prison in Shiraz who assisted with this study. We express our sincere gratitude to all staff members of hospitals and the VCT center of Shiraz for their kind cooperation. We also appreciate the Health Deputy at SUMS for technical support.
REFERENCES
- 1.HIV/AIDS JUNPo. Global Report: UNAIDS Report on the Global AIDS Epidemic: 2012. UN Joint Programme on HIV/AIDS (UNAIDS) PUBLISHER:UNAIDS. 2012 [Google Scholar]
- 2.April K, Köster R, Koch MG. Worldwide HIV incidence – Aspects and dynamics of a tardive epidemic. Schweiz Med Wochenschr. 1997;127:1853–61. [PubMed] [Google Scholar]
- 3.Stoicescu C. The Global State of Harm Reduction: Towards an Integrated Response. London: Harm Reduction International; 2012. [Google Scholar]
- 4.Obermeyer CM. HIV in the middle east. BMJ. 2006;333:851–4. doi: 10.1136/bmj.38994.400370.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jenkins CL, Robalino DA. HIV/AIDS in the Middle East and North Africa: The Costs of Inaction. Washington, DC: World Bank Publications; 2003. World Health Organization, HIV/AIDS JUNPo. [Google Scholar]
- 6.Nejat S, Feyzzadeh A, Asghari S, Keshtkar A, Heshmat R. HIV risk factors in Iran; systematic review, meta-analysis and generalized impact fraction approaches. Payesh. 2007;5:45–57. [Google Scholar]
- 7.Shokoohi M, Baneshi MR, Haghdoost AA. Size estimation of groups at high risk of HIV/AIDS using network scale up in Kerman, Iran. Int J Prev Med. 2012;3:471–6. [PMC free article] [PubMed] [Google Scholar]
- 8.Nasirian M, Haghdoost AA, Doroudi F, Gooya MM, Sedaghat A, Rabbori ED. Modelling HIV modes of transmission in Iran. Retrovirology. 2012;9(Suppl 1):121. [Google Scholar]
- 9.Luan R, Liang B, Yuan P, Fan L, Huang Y, Zeng G, et al. A study on the capture-recapture method for estimating the population size of injecting drug users in Southwest China. J Health Sci. 2005;51:405–9. [Google Scholar]
- 10.Héraud-Bousquet V, Lot F, Esvan M, Cazein F, Laurent C, Warszawski J, et al. A three-source capture-recapture estimate of the number of new HIV diagnoses in children in France from 2003-2006 with multiple imputation of a variable of heterogeneous catchability. BMC Infect Dis. 2012;12:251. doi: 10.1186/1471-2334-12-251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Amstrup SC, McDonald TL, Manly BF. Handbook of Capture-Recapture Analysis. New Jersey, USA: Princeton University Press; 2010. [Google Scholar]
- 12.Zamani S, Kihara M, Gouya MM, Vazirian M, Nassirimanesh B, Ono-Kihara M, et al. High prevalence of HIV infection associated with incarceration among community-based injecting drug users in Tehran, Iran. J Acquir Immune Defic Syndr. 2006;42:342–6. doi: 10.1097/01.qai.0000219785.81163.67. [DOI] [PubMed] [Google Scholar]
- 13.Painter TM. Voluntary counseling and testing for couples: A high-leverage intervention for HIV/AIDS prevention in sub-Saharan Africa. Soc Sci Med. 2001;53:1397–411. doi: 10.1016/s0277-9536(00)00427-5. [DOI] [PubMed] [Google Scholar]
- 14.Bailey NT. On estimating the size of mobile populations from recapture data. Biometrika. 1951;38:293–306. [Google Scholar]
- 15.Burnham KP, Anderson DR. Multimodel inference understanding AIC and BIC in model selection. Sociol Methods Res. 2004;33:261–304. [Google Scholar]
- 16.Kuha J. AIC and BIC comparisons of assumptions and performance. Sociol Methods Res. 2004;33:188–229. [Google Scholar]
- 17.Update AE. Geneva, Joint United Nations Programme on HIV/AIDS and World Health Organization. 2009. Nov, [Last accessed on 2016 Feb 01]. Available from: http://data.unaids.org/pub/Report/2010/2009_annual_report_en.pdf .
- 18.Vadivoo S, Gupte MD, Adhikary R, Kohli A, Kangusamy B, Joshua V, et al. Appropriateness and execution challenges of three formal size estimation methods for high-risk populations in India. AIDS. 2008;22(Suppl 5):S137–48. doi: 10.1097/01.aids.0000343772.82647.2d. [DOI] [PubMed] [Google Scholar]
- 19.Mastro TD, Kitayaporn D, Weniger BG, Vanichseni S, Laosunthorn V, Uneklabh T, et al. Estimating the number of HIV-infected injection drug users in Bangkok: A capture – Recapture method. Am J Public Health. 1994;84:1094–9. doi: 10.2105/ajph.84.7.1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Abeni DD, Brancato G, Perucci CA. Capture-recapture to estimate the size of the population with human immunodeficiency virus type 1 infection. Epidemiology. 1994;5:410–4. doi: 10.1097/00001648-199407000-00006. [DOI] [PubMed] [Google Scholar]
- 21.Lewden C, Jougla E, Alioum A, Pavillon G, Lièvre L, Morlat P, et al. Number of deaths among HIV-infected adults in France in 2000, three-source capture-recapture estimation. Epidemiol Infect. 2006;134:1345–52. doi: 10.1017/S095026880600639X. [DOI] [PMC free article] [PubMed] [Google Scholar]