

Abstract
Accidental poisonongs are an important cause of morbidity and even mortality, especially in young children.
We performed a retrospective observational study on a group of children admitted at the Regional Center of Toxicology at the Children's Emergency Hospital “St. Mary” Iasi with accidental intoxication within a period of 3 years. Data were collected from patients’ files and processed with a SPPS 18.0 database and a 95% confidence interval.
During this period, 480 children were admitted with accidental intoxication. Most of them were in the age group of 1 to 2 years (120 cases—24.3%). The etiology of these intoxications was dominated by nonmedication (67%), the most frequent being household chemicals, carbon monoxide, and insecticides. Accidental drug intoxication accounted for 33% of the cases, the main drugs involved being anticonvulsants, nonsteroidal anti-inflammatory drugs, and paracetamol. The mortality caused by accidental poisoning was 0.62%, all deaths owing to nonmedication intoxication.
Identifying the epidemiological and evolutionary aspects of accidental intoxications must be a major objective for the health system, given that this pathology can be at least partially avoided and its incidence and severity may be reduced using appropriate measures.
Keywords: accidental poisoning, children, drug, household products
1. Introduction
Accidental poisonings represent a common pathology in pediatrics, occurring in virtually every country in the world, including well-developed ones.[1] Although there has been made progress regarding the prevention of accidental poisonings, by using more resistant packaging and raising awareness of the composition of toxic products, they are still frequent in children, particularly in those aged 2 to 3 years old.[2] This high rate of poisoning could be explained by children's curiosity, as well as by parents’ negligence in keeping and using medicine and chemical household substances.[3] The toxic substances involved include drugs, household products, plants, hygiene, and cosmetic products.[4] Identifying the epidemiological aspects of these intoxications in children is especially important for applying adequate preventive measures.[5] Provided that data restricted to our geographical area regarding accidental poisoning in children is limited, the aim of this study was to assess the epidemiological and clinical profile of accidental poisonings in children.
2. Materials and methods
We performed an observational retrospective study on a cohort of children aged 0 to 18 years old, admitted at the Regional Center for Toxicology of the Children's Emergency “St Mary” hospital from Iasi. The study lot consisted of 480 children, admitted for accidental poisonings between January 1, 2014 and December 12, 2016. We were able to identify the toxic substance by anamnesis, as well as clinical and biological exams. We excluded from the study all children admitted for insect and snake bites, as well as those with suspicion of accidental poisoning, in which identifying the toxic involved was impossible.
Data obtained from patients’ files was gathered and processed in a SPSS 18.0 database. Discrete variables were expressed as number and proportion. The comparison of the groups for the categorical variables was done by the Chi square test (χ2), the significance threshold being P = .1. We evaluated the relative risk (RR) and the 95% confidence interval (CI 95%), following statistical interpretation: RR > 1, the variable represents a risk factor; RR = 1, the variable represents an indifferent factor. The statistical signification was accepted at a value of P < .05.
The study was approved by the Institutional Ethical Committee of the Hospital.
3. Results
During the study period, among the children admitted for accidental poisoning, 67% (322 cases) were nondrugs poisonings, whereas 33% (158 cases) were drugs intoxications.
Table 1 depicts the results regarding the incidence of drugs and nondrugs accidental poisonings in various age groups.
Table 1.
Accidental poisonings by age groups.

We noticed the predominance of nondrugs poisonings in children aged 0 to 1 years old (13.7% vs 2.5%; P = ,001). Contrary, in children aged 2 to 3 years old, drug intoxications were more frequently encountered (31.2% vs 20.5%; P = .014), with an estimated risk of 1.52 times greater (CI 95%: 1.11–2.09).
The maximum frequency was registered for the age range of 1 to 2 years old. Tables 2 and 3 illustrate the gender and area distribution of the patients with accidental poisoning.
Table 2.
The distribution of nondrug poisoning by gender and the living environment.
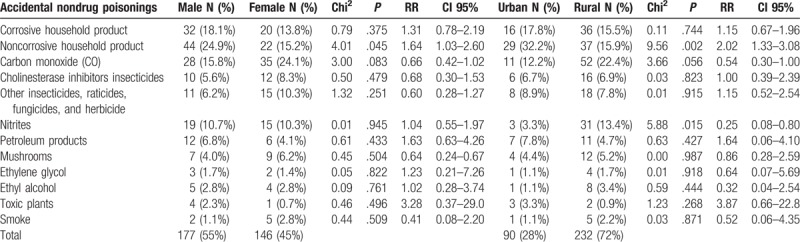
Table 3.
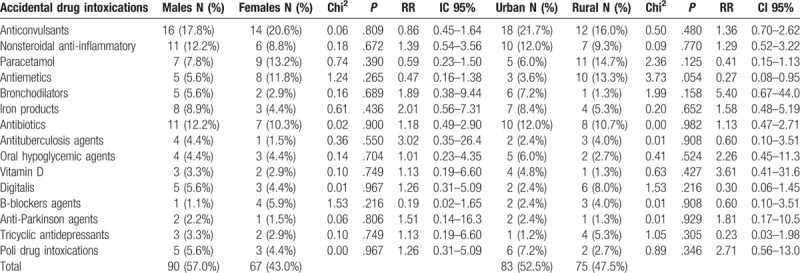
Drug intoxications by gender and the living environment.
We noted that the most frequent causes of nondrug poisonings were: household substances, carbon monoxide, as well as insecticides, raticides, fungicides, and herbicides. The most commonly involved medicines were: anticonvulsants, nonsteroidal anti-inflammatories, and paracetamol.
We registered a higher incidence of intoxications with noncorrosive household products in males (24.9% vs 15.2%; P = .045), with an estimated risk of 1.64 times greater than females. On the other hand, these intoxications were more frequent in urban area (32.2% vs 15.9%; P = .002), with an estimated risk of 2 times higher than in rural area. In 10.8% cases, corrosive substances were involved, especially caustic soda (sodium hydroxide), which is an ingredient of some cleaning products. Poisonings with corrosive substances were more frequent also in males (18.1% vs 13.8%; P = .375), but the difference was not statistically significant.
Other intoxications, ordered by frequency, were with insecticides, raticides, fungicides, and herbicides (48 cases—14.8%). Among these, the most serious were those caused by cholinesterase inhibitors insecticides (22 cases poisoned with organophosphate compounds). Eight of these children were admitted in coma, requiring intubation and mechanical ventilation, supportive treatment and antidote: atropine, sometimes in high doses.
The next one was the intoxication with methemoglobinemia-inducing substances (34 cases—10.5%). These intoxications were more frequently encountered in rural area (13.4% vs 3.3%; P = .015), where the estimated risk was 4 times higher than in urban area. In 6 cases the value of methemoglobinemia was >70%, but the outcome was still favorable with rapid use of antidote —intravenous methylene blue. Intoxications with petroleum products were less frequent (5.4%). Among them, 3 cases had severe chemical pneumonia.
Accidental drug poisonings represented 32.8% from the total number of accidental intoxications. Among drugs poisonings, anticonvulsant substances were the most frequently involved (30 cases—19%). Barbiturates were the most consumed (14 cases), followed by valproate (10 cases) and carbamazepine (6 cases). All cases manifested neurological symptoms and evolved favorably, even in the absence of antidote.
Nonsteroidal anti-inflammatory drugs and paracetamol (acetaminophen) were also encountered (17 cases each). The patients poisoned with nonsteroidal anti-inflammatory drugs had digestive symptoms, but the outcome was good for all cases. Six children with acetaminophen intoxication had severe liver impairment, but all cases evolved favorable due to early antidote treatment (N-acetylcysteine). All cases of intoxication with digitalis evolved favorably with supportive treatment, even though the antidote (anti-digoxin monoclonal antibodies) was not available in our hospital. Antiemetic drugs were the cause for intoxications in 13 cases. The most frequently involved drug was metoclopramide.
Among all 480 patients, there were 3 deaths (0.62%): 1 patient with smoke poisoning and 2 patients intoxicated with organophosphate compounds. In all other cases, the evolution was favorable.
4. Discussion
Accidental poisonings are still highly common in most countries, despite the improvement of preventive measures, which consist of proper packaging of medicines and household products, doubled by raising awareness of the toxic items which should not be kept in children's reach.
In 2014, 55 of Antitoxic Centers from the United States released information regarding 2.2 million cases of intoxications. Among these, 42.6‰ occurred in children aged <6 years old.[5]
In Romania live almost 3.5 millions of children. In the absence of a national register of intoxications in Romania, the etiology of poisonings is not very well known. The most ample study published in Romania is a regional, retrospective one, regarding patients admitted at the Toxicology Departments of Clinic Emergency “Grigore Alexandrescu” Children's Hospital and “Floreasca” Hospital in Bucharest, as well as other 6 hospitals from the south of Romania. Out of 9642 cases of intoxications admitted between 2009 and 2011, accidental poisonings were the most frequent (78%). A great majority of accidental poisonings (95%) took place at home.[3] The second study was conducted at Children's Hospital “Luis Turcanu” Timisoara between 2013 and 2015 on 406 children admitted at the Toxicology Department for acute poisoning. More than half of the cases (53%) were accidental poisonings, nonmedicamentary causes being the most common. The frequency of intoxications was slightly higher in males (1.24:1) and in children aged <3 years old.[6]
Our study was conducted at the Regional Center of Toxicology at the Children's Emergency Hospital “St. Mary” Iasi, where children from northeast Romania are being cared for. In this region, the infant population of about 800,000 children and the number of annual admissions at the above mentioned hospital is approximately 150,000/per year. In our study, during the aforementioned period, out of 147,611 patients aged between 0 and 18 years admitted at the hospital, only 0.03% (480 cases) were hospitalized for accidental poisoning. Other studies report different proportions for accidental intoxications: 0.58%,[7] 1.3%, [8] and 2.31% from all the admissions.[9] Among all patients admitted for intoxication during the same period, those admitted for accidental poisoning represented only 28%. On the other hand, the aforementioned study conducted in Bucharest shows a greater frequency of accidental intoxications (78%); so does the study conducted in Timisoara (53%). This fact may be due to the increasing number of voluntary poisonings with designer drugs in our geographical area. Other studies also report a higher frequency of accidental intoxications: 53%,[9] 94.2%,[10] and even 97%.[11]
In our study, accidental poisonings involved mostly nonmedicamentary products (67%). A study conducted in Spain during June 2012 and December 2014, on 588 patients with accidental intoxications, reports an incidence of 51.3% for drug poisonings.[12] Other studies’ results are similar with those we reported: 68.2% [13] and 68.5%.[14]
Household products poisonings were the most common, representing one-third of the total number of nondrugs intoxications. The household products are packaged in containers with labels advertising about toxicity and possible effects, similar with others European countries. Unfortunately, in Romania, at home, especially in rural areas, household products are often kept in unlabeled containers or plastic bottles of soft drinks that leads to confusion and attract children to explore them. Parents should be more careful not to they leave toxic substances in places accessible to their children. Moreover, educational measures are needed to be implemented in the media, including advertisements on the importance of keeping safe and out of reach of children of these products.
Children with corrosive substances intoxications had major digestive injuries during the acute phase, almost one-third (31%) developing oesophageal stenosis. It is estimated that up to 70% of patients with grade 2B esophagitis and more than 90% of those with grade 3 are susceptible to developing stenosis.[15] In a study of 115 children with varying degrees of postcaustic esophagitis, 46 of them (40%) developed esophageal stenosis.[16]
The second frequent intoxication was that caused by carbon monoxide, which often occurred at home, during the cold season, due to flaws in the heating system. Lots of homes are still heated with wood and pallets of sawdust in the rural areas on northeast Romania. These intoxications occurred in small children as well as in teenagers, but they were more serious in babies and toddlers, due to higher respiratory rate at this age, which allows a rapid absorption of carbon monoxide. The outcome was favorable in all cases. Some studies suggest a possible correlation between carbon monoxide intoxications and the risk of subsequent development of cardiac arrhythmias.[17] Smoke poisoning during fires was rare (7 cases). These cases represent a medical emergency due to double intoxication: carbon monoxide and cyanide compounds, added to the thermic lesions of the respiratory tract. We recorded one death, representing 0.2% from the total number of accidental intoxications.
The mortality in children with organophosphate compounds poisoning was lower compared to other studies, with 2 deaths being registered (9% of the number of organophosphate poisoning and 0.47% of total number of intoxications). A recent study reports a higher mortality with this type of insecticides: 20% of the total number of organophosphate compounds poisoning and 4% of the total number of accidental intoxications.[18] Another study mentions a mortality rate due to poisoning with cholinesterase inhibitors (organophosphorus and carbamate) of 12.7%.[19]
The intoxication with methemoglobinemia-inducing substances is caused by using water with high concentration of nitrates for milk and food preparation for infants. Statistical data in our hospital during 3 years before the actual study (2011–2013) showed a greater number of patients (124) admitted with acquired methemoglobinemia coming from the same area. This downward trend may be due to the intensive measures of raising awareness of people from the risk areas.
Ethylene glycol intoxication caused by accidental ingestion of antifreeze was encountered in 5 cases. All cases evolved favorable, even though some intoxications were serious, due to neurological and renal impairment.
Accidental drug poisonings are a real medical emergency due to the rapid absorption of some medicines. The prevalence in our study is similar with those from other studies: 39.3% [16] and 34%.[7] On the other hand, in another study, drug intoxications accounted 72%—the majority of accidental poisonings.[20]
In our study the mortality was 0.62%. Other studies reported higher mortality rate up to 9%.[21]
This study has some limits, although it comprises a significant number of patients. One of them is the retrospective character, data being collected from patients’ files, so there could be a risk of erroneous registrations. Another limit consists of including only those patients with accidental intoxications admitted in a tertiary hospital from the northeast part of Romania, but there were patients with mild form of intoxications who were cared for at home or at the emergency department, without being admitted.
5. Conclusions
Accidental intoxications represent a public health issue in all countries. In our study, they represented 28% from the total number of intoxications in children admitted during a 3 year period. Nondrugs substances were mostly involved (67%). The highest incidence was noticed in children aged 1 to 2 years old (24.3%). The mortality rate was 0.62%. Many accidental toxic exposures could be avoided by simple, active family preventive measures, by using more resistant packaging and by locating these substances in places where children do not have access. The continual presence of new toxic substances and drugs on the market makes this pathology a topical issue. This requires practitioners to permanently adapt to the current situation and constantly improve their knowledge on this topic.
Author contributions
Conceptualization: Nicolai Nistor.
Data curation: Nicolai Nistor.
Investigation: Otilia Frasinariu, Aniela Rugină, Irina Mihaela Ciomaga, Cristina Jitareanu, Violeta Steanga.
Writing – original draft: Nicolai Nistor.
Writing – review & editing: Otilia Frasinariu, Violeta Steanga.
Footnotes
Abbreviations: CI = confidence interval, RR = relative risk.
The authors have no funding and no conflicts of interest to disclose.
References
- [1].Lingeswaran A. Patterns of accidental poisoning in children in Puducherry, India. Paripex—Indian J Res 2016;5:301–2. [Google Scholar]
- [2].Claudet I. Intoxications domestiques accidentelles de l’enfant. J Pédiatr Puéricult 2016;29:244–68. [Google Scholar]
- [3].Ulmeanu C, Nitescu Viorela. Intoxicatiile acute la copil si adolescent. Ed Tridona Bucuresti 2015;7–12. [Google Scholar]
- [4].Pulce C. Intoxications accidentelles domestiques. Pathol Prof Environ 2009;1:1–0. [Google Scholar]
- [5].Sahin S, Carman KB, Dinleyei EC. Acute poisoning in children: data of pediatric emergency unit. Iran J Pediatr 2011;21:479–84. [PMC free article] [PubMed] [Google Scholar]
- [6].Isac R, Gafencu M, Nastasie IA, et al. Accidental poisoning in paediatric patients—latest folow-up. Arch Dis Child 2017;102:A178–178. [Google Scholar]
- [7].Movry JB, Spyker DA, McMillan N, et al. 2014 annual report of the American Association of Poison Control Centers National Poison Data System NPDS 32 annual report. Clin Toxicol 2015;53:962–1147. [DOI] [PubMed] [Google Scholar]
- [8].Abbas SK, Tikmani SS, Siddiqui NT. Accidental poisoning in children. J Pak Med Assoc 2012;62:331–4. [PubMed] [Google Scholar]
- [9].Koueta F, Dao L, Ye D, et al. Acute accidental poisoning in children: aspects of their epidemiology, aetiology and outcome at the Charles de Gaule Paediatric Hospital in Ouagadougon. Sante 2009;19:53–9. [DOI] [PubMed] [Google Scholar]
- [10].Aggarval B, Rana SK, Chhavi N. Pattern of poisoning in children, an experience from a Teaching Hospital in Northern India. JK Science 2014;16:174–8. [Google Scholar]
- [11].Mendonça DR, Menezes MS, Matos MAA, et al. Acute poisoning in children in Bahia, Brazil. Global Pediatr Health 2016;3:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Keka A, Ramosaj A, Toro H, et al. Acute poisoning in children; changes over the years, data of pediatric clinic department of toxicology. J Acute Dis 2014;3:56–8. [Google Scholar]
- [13].Martinez HJ, Simo NS, Martinez SL, et al. Unintentional intoxications in children: detecting risk. Emerg Med 2015;5:1–4. [Google Scholar]
- [14].Naseem A, Khurram MSA, Khan SS, et al. Accidental poisoning its magnitude and implications in children. Int J Pediatr Res 2016;3:400–9. [Google Scholar]
- [15].Katz A, Kluger Y. Caustic material ingestion injuries-paradigm shift in diagnosis and treatment. Health Care Curr Rev 2015;3:1–4. [Google Scholar]
- [16].Lupu VV, Ignat A, Paduraru G, et al. The study of effects regarding ingestion of corrosive substances in children. Rev Chim 2016;67:2501–3. [Google Scholar]
- [17].Lee FY, Chen WK, Lin CL, et al. Carbon monoxide poisoning and subsequent cardiovascular disease risk. Medicine (Baltimore) 2015;94:e624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Azaba SMS, Hirshonb JM, Hayesd BD, et al. Epidemiology of acute poisoning in children presenting to the poisoning treatment center at Ain Shams University in Cairo, Egypt, 2009–2013. Clin Toxicol (Phila) 2016;54:20–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Huang HS, Hsu CC, Weng SF, et al. Acute anticholinesterase pesticide poisoning caused a long-term mortality increase. Medicine (Baltimore) 2015;94:e1222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Mahdeb N, Mariem S, Abdelouahab B. Etude epidemiologique des cas d’ intoxications aigues traites a l’hopital de Setif entre janvier 2008 et avril 2012 (Est Algerie). Eur Scient J 2013;9:157–65. [Google Scholar]
- [21].Ramos CLJ, Barros HMT, Stein AT, et al. Risk factors contributing to childhood poisoning. J Pediatr 2010;86:435–40. [DOI] [PubMed] [Google Scholar]