

Abstract
Background and study aims
The efficacy of per oral endoscopic myotomy (POEM) in non-achalasia esophageal motility disorders such as esophagogastric junction outflow obstruction (EGJOO), diffuse esophageal spasm (DES), and jackhammer esophagus (JE) has not been well demonstrated. The aim of this international multicenter study was to assess clinical outcomes of POEM in patients with non-achalasia disorders, namely DES, JE, and EGJOO, in a large cohort of patients.
Patients and methods
This was a retrospective study at 11 centers. Consecutive patients who underwent POEM for EGJOO, DES, or JE between 1/2014 and 9/2016 were included. Rates of technical success (completion of myotomy), clinical response (symptom improvement/Eckardt score ≤ 3), and adverse events (AEs, severity per ASGE lexicon) were ascertained .
Results
Fifty patients (56 % female; mean age 61.7 years) underwent POEM for EGJOO (n = 15), DES (n = 17), and JE (n = 18). The majority of patients (68 %) were treatment-naïve. Technical success was achieved in all patients with a mean procedural time of 88.4 ± 44.7 min. Mean total myotomy length was 15.1 ± 4.7 cm. Chest pain improved in 88.9 % of EGJOO and 87.0 % of DES/JE ( P = 0.88). Clinical success was achieved in 93.3 % of EGJOO and in 84.9 % of DES/JE ( P = 0.41) with a median follow-up of 195 and 272 days, respectively. Mean Eckardt score decreased from 6.2 to 1.0 in EGJOO ( P < 0.001) and from 6.9 to 1.9 in DES/JE ( P < 0.001). A total of 9 (18 %) AEs occurred and were rated as mild in 55.6 % and moderate in 44.4 %.
Conclusion
POEM is effective and safe in management of non-achalasia esophageal motility disorders, which include DES, JE, and EGJOO.
Introduction
Peroral endoscopic myotomy (POEM) was introduced in 2008 by Inoue and colleagues as the endoscopic alternative to laparoscopic Heller myotomy for treatment of achalasia 1 . Multiple studies have been published since then assessing efficacy and safety of POEM in achalasia patients and have shown excellent clinical response in more than 80 % to 90 % of patients 2 3 4 5 6 7 . In addition, serious adverse events (AEs) are rare and most AEs can be managed intraprocedurally 8 . More recently, POEM has been described for treatment of patients with non-achalasia esophageal motility disorders; these include spastic esophageal disorders, namely diffuse esophageal spam (DES), jackhammer esophagus (JE), and esophagogastric junction outflow obstruction (EGJOO) 9 10 . However, the role POEM plays in management of these disorders is not clear, mainly due to scarcity of studies on this topic.
DES is characterized by normal mean Integrated Relaxation Pressure (IRP) and ≥ 20 % premature contractions. JE is an extreme pattern of hypercontractility and is defined manometrically as at least one swallow with a distal contractile integral (DCI) (the metric of contractile vigor), greater than 8000 mm Hg-s-cm. EGJOO is defined as an elevated IRP > 15 mmHg with evidence of peristalsis such that a diagnosis of achalasia is not met 11 .
Medical and endoscopic (e. g. calcium channel blockers and botulinum toxin injection) therapy of DES and JE is ineffective in the majority of patients 12 13 . POEM is potentially an ideal treatment for these disorders. Spastic contractions can extend proximally in patients with DES and JE. Extending the myotomy into the proximal esophagus may not be possible surgically due to anatomic reasons. A short myotomy may potentially result in an ineffective procedure. POEM permits easy access to the proximal and mid-esophagus without limit to the extent of myotomy. Nonetheless, few reports that included a small number of patients have suggested potential effectiveness of POEM in DES and JE 9 14 . The aim of this international multicenter study was to assess clinical outcomes of POEM in patients with non-achalasia disorders, namely DES, JE, and EGJOO, in a large cohort of patients.
Patients and methods
This was a retrospective study at 11 centers (5 North America, 4 Europe, 2 Asia) between January 2014 and September 2016. Only patients with DES, JE and EGJOO were included. Patients diagnosed with achalasia, including spastic (type III) subtype, were excluded. Diagnosis was based on high-resolution manometric findings according to the Chicago classification of esophageal motility disorders ( Fig. 1 ). Overall, 21 patients have been reported in previous publications (9 patients 15 16 , 6 patients 16 , 5 patients 17 , and 1 patient 15 ). The study was approved by the local ethics committees at all participating centers.
Fig. 1 a.
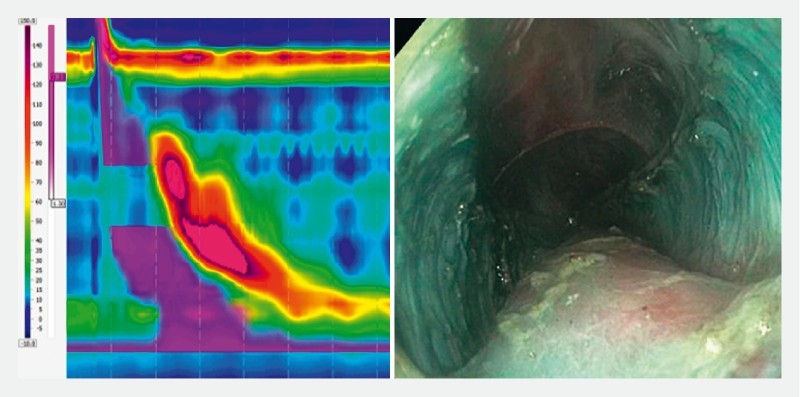
High-resolution manometry with findings consistent with jackhammer esophagus (distal contractile integral > 8000 mmHg-s-cm). b Per oral endoscopic myotomy with long myotomy (17 cm) for management of jackhammer esophagus
Data collection
Relevant patient and procedural data were abstracted by chart reviews and entered into a de-identified database. Preprocedural data included demographics, type of esophageal motility disorder, patient symptoms, Eckardt score, duration of disease, and prior medical, endoscopic and/or surgical therapy. Procedural data included date of procedure, extent (partial or complete) of myotomy, length of esophageal and gastric myotomies, intraprocedural AEs and procedure duration. Post-procedural data included length of hospital study, delayed AEs, symptoms and Eckardt score, reflux symptoms and medication (e. g. proton pump inhibitors) usage, and length of follow-up.
Measured outcomes
Technical success was defined as successful completion of myotomy, while clinical response was defined as symptom improvement and Eckardt score ≤ 3. AEs were recorded and their severity was graded according to the ASGE lexicon as defined by Cottton et al. 18
Procedural technique and periprocedural care
POEM was performed as previously described 19 in patients with achalasia with the major difference in length of esophageal myotomy. This was determined by the proximal extent of spastic contractions above the LES as determined by review of high-resolution esophageal manometric tracings and observation of the esophagus during endoscopy for visible spasms. A high-definition gastroscope with jet injection capability with a clear cap mounted on its tip was used for all procedures with patients under general anesthesia using carbon dioxide for insufflation. A submucosal bleb was then created using saline and blue dye in the proximal or mid-esophagus above the spastic esophageal segment. A 1.5-cm longitudinal incision was performed over the bleb using an Endocut Q (ERBE, Tübingen, Germany) current with either a triangle tip knife (Olympus, Tokyo, Japan) or Hybridknife (ERBE). The gastroscope was then introduced into the submucosal space and submucosal tunneling was performed using spray-coagulation mode. The tunnel was extended across the LES and into the gastric cardia. It is unknown if LES and cardia myotomy are essential in patients with DES and JE as the main pathology possibly does not involve the LES. However, all operators in the current study performed LES and cardia myotomy. Following completion of the tunnel, endoscopic myotomy was commended 2 to 3 cm below the mucosal incision and extended to the end of the tunnel. Direction (anterior vs posterior) and extent (selective inner circular vs full-thickness) of myotomy were determined at the treating endoscopist’s discretion. After completion of myotomy, the mucosal incision was closed using through-the-scope clips.
All patients received periprocedural antibiotics and were admitted to the hospital for observation. An esophagram was obtained the following day to exclude esophageal leak followed by commencement of liquid and then soft diet. Patients were discharged home if they were able to tolerate soft diet without significant pain.
Statistical analysis
Results are reported as mean and standard deviation/range for quantitative variables while percentages were used for categorical variables. Comparison of continuous variables was performed with the student’s t -test and Mann-Whitney U test and categorical variables by using the chi-square test and Fisher exact. A level of significance of P < 0.05 was adopted for all inferential testing. Statistical analysis was performed by using SPSS version 16 (SPSS Inc, Chicago, Ill).
Results
During the study period, 50 patients (56 % female; mean age 61.7 ± 16.3 years) underwent POEM for EGJOO (n = 15), DES (n = 17), or JE (n = 18) ( Table 1 ). Mean duration of symptoms was 53.2 ± 84.4 months. The mean preprocedural Eckardt score was 6.9 ± 2.3. Chest pain was present in 36 patients. The majority of patients with DES/JE were treatment-naïve (77.1 %, n = 27) while three patients (8.5 %) had pneumatic dilation (PD) alone, three patients (8.5 %) had previous botulinum injection (BT) alone, one patient (2.9 %) had previous PD and Heller myotomy, and one patient (2.9 %) had previous BT and Heller myotomy. As for EGJOO, nine patients (60 %) were treatment-naïve, four (26.7 %) had previous PD alone, one (6.6 %) had previous BT alone, and one patient (6.6 %) had previous BT and PD.
Table 1. Baseline characteristics.
| Age (years, mean [SD]) | 61.7 (16.3) |
| Gender | |
| Female n = (%) | 28 (56.0) |
| Male n = (%) | 22 (44.0) |
| Duration of symptoms (months, mean [SD]) | 53.2 (84.4) |
| Chest pain (missing data = 3) n = (%) | 36 (76.6) |
| None | 11 (23.4) |
| Occasional | 13 (27.7) |
| Daily | 11 (23.4) |
| Each Meal | 12 (25.5) |
| Total Eckardt Score, mean (SD)/median (IQR) | 6.9 (2.3)/7 (5 – 8) |
| Medical therapy (some patients on more than one) n = (%) | 20 (40.0) |
| Calcium channel blocker (CCB) | 16 (32.0) |
| Nitric oxide | 7 (14.0) |
| Tricyclics | 1 (2.0) |
| Others | 2 (4.0) |
| Endoscopic treatment-naïve n = (%) | 36 (72.0) |
| Prior botulinum toxin injection and pneumatic dilation n = (%) | 1 (2.0) |
| Prior pneumatic dilation alone n = (%) | 7 (14.0) |
| Prior botulinum toxin injection alone n = (%) | 4 (8.0) |
| Prior pneumatic dilation and Heller myotomy n = (%) | 1(2.0) |
| Prior botulinum toxin injection and Heller myotomy n = (%) | 1 (2.0) |
SD, standard deviation; IQR, interquartile range
POEM was successfully completed (technical success) in all 50 patients (100 %) with a mean procedural time of 88.4 ± 44.7 minutes. Selective inner circular myotomy was implemented in 48.0 % of patients and full-thickness myotomy in 44.0 % (8.0 % unspecified). Mean total myotomy length was 15.1 ± 4.7 cm. Mean length of esophageal myotomy was 12.5 ± 4.3 cm, while mean length of gastric myotomy was 2.5 ± 1.05 cm. All patients underwent myotomy of the LES with myotomy extension into the gastric cardia. All patients were hospitalized after completion of POEM with a median length of hospital stay of 2 days (IQR 1 – 5). Nine AEs (18 %) (55.6 % mild and 44.4 % moderate) occurred in 8 patients, including two symptomatic capno-thorax/peritoneum, one bleed, one esophageal leak, one post-procedure pain, one inadvertent mucosotomy, one aspiration pneumonia, one submucosal hematoma, and one unspecified ( Fig. 2 ). During a median follow-up duration of 242.5 days (IQR 40.5 – 505.5), 42 patients (87.5 %) achieved clinical success (2 patients were lost to follow-up) with an Eckardt score ≤ 3. The majority of patients (52 %) had either complete or almost complete (Eckardt score 0 or 1) resolution of symptoms. Chest pain improved in 87.5 % of patients who had chest pain prior to POEM. Mean post-procedural Eckardt score was 1.6 ± 2.2. Reflux symptoms developed in 22.2 % of patients, all of whom were successfully treated with proton pump inhibitors. Repeat high-resolution esophageal manometry was available in 35 patients and showed resolution of initial manometric abnormalities in 29 (82.9 %). Mean integrated relaxation pressures (IRP) pre- and post-POEM for EGJOO were 25.5 ± 8.48 mmHg and 9.6 ± 7.95 mmHg, respectively.
Fig. 2.
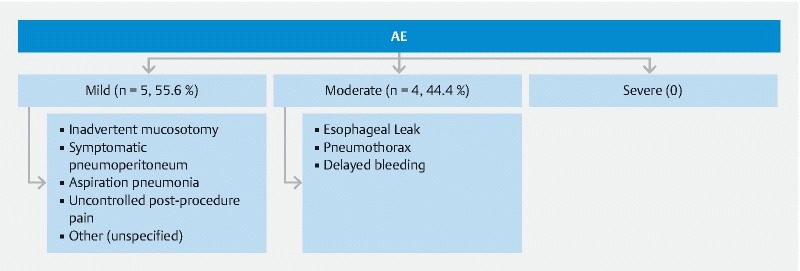
Adverse events stratified according to severity as per the ASGE Lexicon 18 .
Subgroup analysis
The mean procedural time was 73.9 ± 22.1 minutes in EGJOO and 94.7 ± 50.5 minutes in DES/JE ( P = 0.13). Mean length of esophageal myotomy was greater in DES/JE at 13.8 ± 4.1 cm (range: 7 – 23 cm) vs. 9.6 ± 3.5 cm (range: 4 – 17 cm) in EGJOO ( P = 0.001). Myotomy of the lower esophageal sphincter (LES) was performed in all patients with EGJOO and DES/JE with a mean gastric myotomy length of 2.93 ± 0.59 cm (range: 2 – 4 cm) and 2.34 ± 1.16 cm (range: 1 – 7 cm), respectively ( P = 0.07). Full-thickness myotomy was undertaken in 53.3 % of EGJOO and 40.0 % of DES/JE ( P = 0.001), with the remaining patients undergoing selective inner circular myotomy. Chest pain improved in 88.9 % of EGJOO and 87.0 % of DES/JE (90.9 % in DES and 83.3 % in JE) ( P = 0.88) ( Table 2 ). Clinical success was achieved in 93.3 % of EGJOO and in 84.9 % of DES/JE (94.1 % in DES and 75.0 % in JE, P = 0.41) with a median follow-up of 195 days interquartile range (IQR): 139 – 617 and 272 days IQR:36 – 500, respectively. Mean Eckardt score decreased from 6.2 to 1.0 in EGJOO ( P < 0.001) and from 6.9 to 1.9 in DES/JE (6.8 to 1.4 in DES and 7.5 to 2.5 in JE) ( P < 0.001). A higher proportion of patients in the EGJOO group achieved complete or almost complete (Eckardt score 0 or 1) resolution of symptoms (60.0 % vs. 48.6 %, P = 0.46). Rates of AEs were comparable between both groups (13.3 % vs 20.0 %, P = 0.58). Post-POEM symptomatic reflux was also similar (35.7 % vs. 16.1 %, P = 0.15). Median length of hospitalization was 3 days (IQR 1 – 4) in EGJOO and 2 days (IQR 1.5 – 5.5) in DES/JE.
Table 2. Clinical outcomes stratified according to type of esophageal motility disorder.
| Outcome | EGJOO | DES/JH | P -value |
| (n = 15) | (m = 35) | ||
| Improvements in chest pain (%, 95 %CI) | 88.9 (51.7 – 99.7) | 87 (66.4 – 97.2) | 0.88 |
| Clinical success (%, 95 %CI) | 93.3 (68.1 – 99.8) | 84.9 (68.1 – 94.9) | 0.41 |
| Mean post POEM Eckardt score, mean (95 % CI) | 1.0 (0.55 – 1.68) | 1.9 (1.41 – 2.42) | 0.24 |
| Post-POEM symptomatic reflux (%, 95 %CI) | 35.7 (12.8 – 64.9) | 16.1 (5.5 – 33.7) | 0.14 |
| Median length of hospitalization (days, IQR) | 3 (1 – 4) | 2 (1.5 – 5.5) | 0.85 |
| Median length of follow-up (days, IQR) | 195 (139 – 617) | 272 (36 – 500) | 0.96 |
| HRM performed post-POEM (%, 95 %CI) | 93.3 (68.1 – 99.8) | 60 (42.1 – 76.1) | 0.02 |
| Resolution of EGJOO/DES/JE on post-procedure HRM (%, 95 %CI) | 71.4 (41.9 – 91.6) | 90.5 (69.6 – 98.8) | 0.14 |
| Adverse events (%, 95 %CI) | 13.3 (1.6 – 40.4) | 20 (8.4 – 36.9) | 0.71 |
SD, standard deviation; IQR, interquartile range; POEM, per oral endoscopic myotomy; EGJOO, esophagogastric junction outflow obstruction; DES, diffuse esophageal spasm; JE: jackhammer esophagus; HRM, high-resolution manometry
Discussion
POEM has revolutionized management of achalasia since its inception in 2008 1 . More than 300 reports have been published to date on POEM, the vast majority of which described POEM for management of achalasia. In recent years, POEM has also been introduced for management of non-achalasia esophageal motility disorders 9 , but the scarcity of reports has led to low dissemination and suboptimal knowledge of the role of POEM in managing these disorders. This multicenter international study assessed efficacy and safety of POEM in management of patients with EGJOO, DES and JE. POEM resulted in clinical success in the majority of patients (87.5 %). Although AEs occurred in 18 % of patients, 55.6 % were rated as mild and 44.4 % as moderate with no severe events. All complications could be managed intraprocedurally or with conservative management. There was no need for surgical intervention in any of the patients. On subgroup analysis, patients with EGJOO had a numerically higher response rate as compared to patients with spastic disorders (DES and JE) at 93.3 % and 84.9 %, respectively. The difference, however, was not statistically significant ( P = 0.41), likely a type II error due to the relatively small number of included patients. Remarkably, chest pain improved in > 85 % of patients in both groups. Chest pain is frequently the major presenting symptom in these disorders and is difficult to treat 20 21 .
A previous multicenter study investigated the role of POEM in 73 patients with spastic esophageal disorders 9 . However, the vast majority of patients (n = 54) in that study had type III (spastic) achalasia. A total of nine patients had DES and 10 had JE and clinical response was achieved in 100 % and 70 % of patients, respectively. Chest pain significantly improved in 87 % of patients who reported chest pain before POEM. Results from the current study along with published data suggest POEM as an effective technique for these difficult-to-treat spastic disorders. It is important to mention that a long esophageal myotomy is essential to ensure that proximal esophageal spasms are effectively covered and treated. Mean length of esophageal myotomy in patients with DES and JE in the current study was about 14 cm, which is more than twice the length of a typical endoscopic or surgical myotomy performed in achalasia patients.
Patients with DES and JE do not typically have EGJ outflow obstruction 22 23 . It is arguable whether they require myotomy of the LES. Unfortunately, the necessity of LES myotomy cannot be inferred from the current study as LES was included in myotomy in all patients. However, inclusion of the LES seems warranted by the potential after-effects of myotomy, even in the setting of normal LES pressure, because preserving LES pressure may result in postoperative dysphagia caused by induced aperistalsis. Recently, Bechara and colleagues reported four cases of JE treated with POEM, three of whom had LES myotomy and one who did not 14 . Patients in whom the LES was included during POEM had resolution or significant improvement in symptoms. The one patient in whom the LES was preserved developed significant dysphagia and regurgitation. Subsequently, this latter patient underwent repeat POEM which included the LES; this resulted in symptom resolution. The expert authors concluded that myotomy of the LES is advisable to reduce risk of symptom development from iatrogenic ineffective esophageal motility or subsequent progression to achalasia.
EGJOO is characterized by elevated median IRP > 15 mmHg with sufficient evidence of peristalsis such that criteria for types I-III achalasia are not met 22 23 . It is believed to be a variant of achalasia and that at least some patients with EGJOO will later progress to having achalasia. An extensive myotomy is not essential in this disorder. There currently exist no dedicated studies that have evaluated the role of POEM is this newly defined clinical entity. In the current study, a total of 15 patients with EGJOO were treated with POEM and clinical success was achieved in 93 % of patients. This is in line with response rates reported in patients with achalasia who undergo POEM.
The current study had several limitations. The study included a relatively small number of patients and, thus, comparative data are prone to type II error. However, the studied disorders are very rare and the compiled cohort represents the largest of non-achalasia patients who underwent POEM. The study was retrospective with inherent limitations due to its design. All patients were treated at tertiary institutions with extensive expertise in POEM and management of motility disorders; therefore, results may not be generalizable. As mentioned above, the value of performing LES myotomy could not be concluded from the current study.
Conclusion
In conclusion, POEM is effective and safe in management of non-achalasia esophageal motility disorders, which include diffuse ES, JE, and EJOO. Randomized trials are needed to confirm the primary role of POEM in management of these disorders.
Footnotes
Competing interests Mouen Khashab is a consultant for Olympus and Boston Scientific. Peter V. Draganov is a consultant for Olympus and Cook Medical. Michael Ujiki is a consultant for Olympus and Boston Scientific. Jeffrey Marks is a consultant for Olympus and Boston Scientific. Dennis Yang is a consultant for Cook Medical and Boston Scientific. Yen-I Chen is a consultant for Boston Scientific.
References
- 1.Inoue H, Minami H, Kobayashi Y et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010;42:265–271. doi: 10.1055/s-0029-1244080. [DOI] [PubMed] [Google Scholar]
- 2.Khashab M A, El Zein M, Kumbhari V et al. Comprehensive analysis of efficacy and safety of peroral endoscopic myotomy performed by a gastroenterologist in the endoscopy unit: a single-center experience. Gastrointest Endosc. 2016;83:117–125. doi: 10.1016/j.gie.2015.06.013. [DOI] [PubMed] [Google Scholar]
- 3.Khashab M A, Kumbhari V, Kalloo A N et al. Peroral endoscopic myotomy: a 4-step approach to a challenging procedure. Gastrointest Endosc. 2014;79:997–998. doi: 10.1016/j.gie.2013.12.004. [DOI] [PubMed] [Google Scholar]
- 4.Kumbhari V, Khashab M A. Peroral endoscopic myotomy. World J Gastrointest Endosc. 2015;7:496–509. doi: 10.4253/wjge.v7.i5.496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ngamruengphong S, Inoue H, Chiu P W et al. Long-term outcomes of per-oral endoscopic myotomy in patients with achalasia with a minimum follow-up of 2 years: an international multicenter study. Gastrointest Endosc. 2017;85:927–93300. doi: 10.1016/j.gie.2016.09.017. [DOI] [PubMed] [Google Scholar]
- 6.Bechara R, Onimaru M, Ikeda H et al. Per-oral endoscopic myotomy, 1000 cases later: pearls, pitfalls, and practical considerations. Gastrointest Endosc. 2016;84:330–338. doi: 10.1016/j.gie.2016.03.1469. [DOI] [PubMed] [Google Scholar]
- 7.Werner Y B, Costamagna G, Swanstrom L L et al. Clinical response to peroral endoscopic myotomy in patients with idiopathic achalasia at a minimum follow-up of 2 years. Gut. 2016;65:899–906. doi: 10.1136/gutjnl-2014-308649. [DOI] [PubMed] [Google Scholar]
- 8.Zhang X C, Li Q L, Xu M D et al. Major perioperative adverse events of peroral endoscopic myotomy: a systematic 5-year analysis. Endoscopy. 2016;48:967–978. doi: 10.1055/s-0042-110397. [DOI] [PubMed] [Google Scholar]
- 9.Khashab M A, Messallam A A, Onimaru M et al. International multicenter experience with peroral endoscopic myotomy for the treatment of spastic esophageal disorders refractory to medical therapy (with video) Gastrointest Endosc. 2015;81:1170–1177. doi: 10.1016/j.gie.2014.10.011. [DOI] [PubMed] [Google Scholar]
- 10.Stavropoulos S N, Modayil R J, Friedel D et al. The International Per Oral Endoscopic Myotomy Survey (IPOEMS): a snapshot of the global POEM experience. Surg Endosc. 2013;27:3322–3338. doi: 10.1007/s00464-013-2913-8. [DOI] [PubMed] [Google Scholar]
- 11.Roman S, Pandolfino J E, Chen J et al. Phenotypes and clinical context of hypercontractility in high-resolution esophageal pressure topography (EPT) Am J Gastroenterol. 2012;107:37–45. doi: 10.1038/ajg.2011.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Drenth J P, Bos L P, Engels L G. Efficacy of diltiazem in the treatment of diffuse oesophageal spasm. Aliment Pharmacol Ther. 1990;4:411–416. doi: 10.1111/j.1365-2036.1990.tb00487.x. [DOI] [PubMed] [Google Scholar]
- 13.Vanuytsel T, Bisschops R, Farre R et al. Botulinum toxin reduces Dysphagia in patients with nonachalasia primary esophageal motility disorders. Clin Gastroenterol Hepatol. 2013;11:1115–1121 e1112. doi: 10.1016/j.cgh.2013.03.021. [DOI] [PubMed] [Google Scholar]
- 14.Bechara R, Ikeda H, Inoue H. Peroral endoscopic myotomy for Jackhammer esophagus: to cut or not to cut the lower esophageal sphincter. Endosc Int Open. 2016;4:E585–E588. doi: 10.1055/s-0042-105204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Haito-Chavez Y, Inoue H, Beard K W et al. Comprehensive analysis of adverse events associated with per oral endoscopic myotomy in 1826 patients: an international multicenter study. Am J Gastroenterol. 2017;112:1267–1276. doi: 10.1038/ajg.2017.139. [DOI] [PubMed] [Google Scholar]
- 16.Khashab M A, Messallam A A, Onimaru M et al. International multicenter experience with peroral endoscopic myotomy for the treatment of spastic esophageal disorders refractory to medical therapy (with video) Gastrointest Endosc. 2015;81:1170–1177. doi: 10.1016/j.gie.2014.10.011. [DOI] [PubMed] [Google Scholar]
- 17.Perbtani Y B, Mramba L K, Yang D et al. Life after per-oral endoscopic myotomy: long-term outcomes of quality of life and their association with Eckardt scores. Gastrointest Endosc. 2018;6:1415–14200. doi: 10.1016/j.gie.2018.01.019. [DOI] [PubMed] [Google Scholar]
- 18.Cotton P B, Eisen G M, Aabakken L et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454. doi: 10.1016/j.gie.2009.10.027. [DOI] [PubMed] [Google Scholar]
- 19.Committee N PWP, Stavropoulos S N, Desilets D J et al. Per-oral endoscopic myotomy white paper summary. Gastrointest Endosc. 2014;80:1–15. doi: 10.1016/j.gie.2014.04.014. [DOI] [PubMed] [Google Scholar]
- 20.Katz P O, Dalton C B, Richter J E et al. Esophageal testing of patients with noncardiac chest pain or dysphagia. Results of three yearsʼ experience with 1161 patients. Ann Intern Med. 1987;106:593–597. doi: 10.7326/0003-4819-106-4-593. [DOI] [PubMed] [Google Scholar]
- 21.Mujica V R, Mudipalli R S, Rao S S. Pathophysiology of chest pain in patients with nutcracker esophagus. Am J Gastroenterol. 2001;96:1371–1377. doi: 10.1111/j.1572-0241.2001.03791.x. [DOI] [PubMed] [Google Scholar]
- 22.Kahrilas P J, Bredenoord A J, Fox M et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motility. 2015;27:160–174. doi: 10.1111/nmo.12477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Roman S, Gyawali C P, Xiao Y et al. The Chicago classification of motility disorders: an update. Gastrointest Endosc Clin North Am. 2014;24:545–561. doi: 10.1016/j.giec.2014.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]