

Abstract
AIMS AND OBJECTIVES:
The aim and objective of this study was to sort out the reasons for use and nonuse of dental services among people visiting a private dental hospital in urban India.
MATERIALS AND METHODS:
A descriptive cross-sectional study was carried out on 1800 people, aged 18–65 years, visiting a multispecialty dental hospital in urban India. A self-administered questionnaire was used to collect data about the history of dental visits and reasons for use and nonuse of dental services.
RESULTS:
For a majority of the people (45%), time since the last dental visit was more than 2 years, and the main reason for visiting a dentist was dental pain (38%). Majority of the people had received restoration of teeth in their previous dental visit (46%). The major reason cited for not visiting a dentist was lack of knowledge toward dental problems and their consequences (30%). Only few people visited dentists for preventive reasons. More patients with better educational levels visited dentists than patients with poor educational status.
CONCLUSION:
Majority of the people visited dentists when their problem was severe enough to have a dental appointment. Dental practitioners across locations should also educate the patients regarding the importance of regular dental care, discuss barriers for dental care, and promote attitudinal changes toward a positive health-seeking behavior.
Keywords: Dental services, private dental hospital, urban India, utilization
Introduction
Access to dental services is generally regarded as a necessary condition for achieving population-level oral health and well-being. Oral diseases such as dental caries, periodontitis, and oral cancer are major public health problems in low-income countries, and the burden of oral diseases is growing in many low- and middle-income countries.[1]
People in India have lower dental care utilization, higher rates of dental caries, periodontal diseases, and permanent loss of tooth at an earlier age than the population of developed countries for many reasons. Oral diseases are largely preventable by regular home oral care and preventive dental visits which help in the early detection and treatment of oral diseases. However, the provision of preventive dental care for adults depends on each patient's initiatives in utilizing dental care.[2]
The American Dental Association recommends that adults consult a dentist at least once every 6 months, and this is based on the belief that dentists cannot only treat the existing problems but that regular dental visits are necessary for the maintenance of healthy gums and teeth. Although in India dentists recommend regular dental visits, many people fail to comply with this due to several barriers that exist for the utilization of dental services. Limited knowledge about dental health, ineffective education and motivation, limited availability of dental care, and lower economical conditions are few among them. Dental indifference has been found to be associated with poorer oral health and nonattendance, as well as usually visiting for a problem rather than a checkup.[3]
Only few studies have actually asked people if they avoid going to the dentist and what are the reasons for their avoidance or delay might be. Understanding factors that initiate and hinder dental service use is necessary if decision makers are to develop policies that adequately address these issues. In this direction, utilization studies serve as an important tool for oral health policy decision-making and understanding oral health-related behavior. This study describes the reasons for utilization and nonutilization of dental services in urban Indian population and describes potential solutions to overcome them, thereby enhancing preventive and public health measures.
Materials and Methods
The study was carried out in a multispecialty dental hospital, in Vijayawada, Andhra Pradesh, India. The time limit set for collection of data was for a period of 6 months from July 2016 to December 2016. The sampling methodology adopted was deliberate sampling. The study sample comprised of all patients who were willing to participate in the study among those visiting the dental clinic during the 6-month period. A voluntary, written informed consent was obtained from the participants before the start of the study. The study sample consisted of 1800 people, aged 18–65 years.
A self-administered, anonymous questionnaire prepared in the local language was used to collect data about sociodemographic characteristics, educational status, and dental visit history. The internal consistency of the questionnaire was pilot tested on eighty patients.
The people who had previously visited a dentist were asked to report reason for their last dental visit, the time since their last dental visit, the treatment received during their last dental visit, and whether regular follow-up to dentist was there or not. The people who had never visited a dentist previously were asked to report reason for not having dental services. They were also asked whether they were aware of their dental condition or not. These people were asked to choose the reason that had prevented them from converting their need for treatment into demand for dental care from a list. A space was also provided for listing reasons not included in the choices.
After obtaining this information, they were screened for their oral health status and dental condition. The data were systematically compiled, and the results were expressed in percentages. Treatment needs were explained to patients and the needed treatments were done.
Results
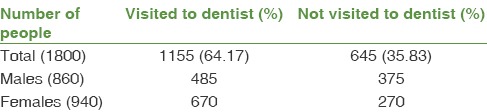
Out of the 1800 people, 1155 people (64.17%) had previously visited a dentist and 645 people (35.83%) had never previously visited a dentist. Majority of people who had previously visited a dentist belonged to the age group of 18–25 years (36%), and majority of people who had never previously visited a dentist belonged to the age group of 26–35 years (45%).
A higher number of females had a dental visit previously (58%) as compared to males (46%) [Table 1]. Among the people who had previously visited a dentist, a higher percentage of people had college level of education (47%) followed by school level of education (31%), whereas majority of the people who had never previously visited a dentist had education levels below the 7th grade (45%).
Table 1.
Demographic data of sample
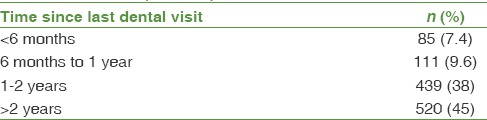
Among the people who had previously visited a dentist, majority of the people (42%) had an income of Indian rupees >30,000/month. Majority of the people who had never previously visited a dentist (80%) had an income of Indian rupees <10,000/month. Majority of the people who had previously visited a dentist said that the time since their last dental visit was >2 years (45%) followed by <2 years and more than 1 year (38%) [Table 2].
Table 2.
Distribution of data according to time since last dental visit (n=1155)
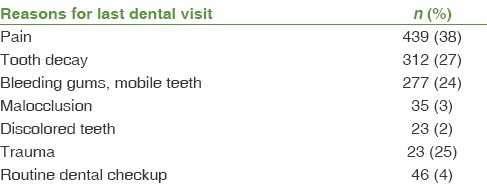
Majority of them said that they had visited dentist because of dental pain (38%) followed by decayed teeth (27%) and bleeding gums (24%). Only 46 of them (4%) said that they had visited dentist for routine dental examination [Table 3]. Majority of the people said that they had received restorations for their teeth (46%) followed by oral prophylaxis (26%).
Table 3.
Distribution of data according to prime reasons for last dental visit (n=1155)
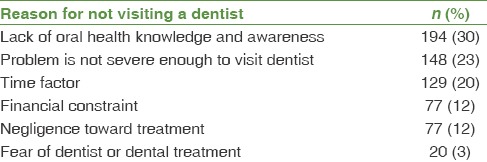
Among people who had never previously visited a dentist, the reasons most frequently cited for not visiting were lack of oral health knowledge (30%) and the presence of a dental problem which was not severe enough to go to a dentist (23%). This was followed by the reason that they “did not have free time without disturbing their work” or they “neglected” their dental problems (20%). The “cost of dental treatment” was a barrier for 12% of the people. The “fear of dentist or dental treatment” was a barrier for a small number of people (3%) [Table 4].
Table 4.
Data of “nonvisitors” according to reasons for not visiting a dentist (n=645)
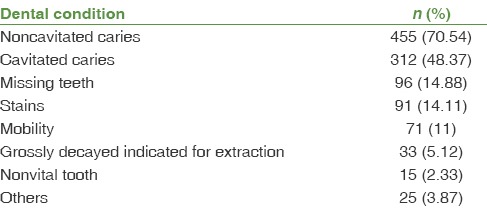
On oral examination, it was found that all the 645 people who had never previously visited a dentist had some dental problems that required treatment. Out of the 645 people who had never visited a dentist previously, 455 (70.54%) people had noncavitated caries lesions needing treatment in at least one of their teeth, 312 (48.37%) people had a cavity in at least one of their teeth, 96 (14.88%) people had one or more missing teeth, 91 (14.11%) people had stains and deposits on their teeth, 71 (11%) people had mobility of Grade 2 or more in one or more teeth, 66 (10.23%) people had root stumps that needed extraction, 33 (5.12%) people had malocclusion that needed correction, and 15 (2.33%) people had nonvital tooth. These people were asked whether they knew about their dental condition or not. Out of 645 patients, 525 (81.4%) people knew that they had some dental problems, if not knowing the exact dental problem and its consequences [Table 5].
Table 5.
Data regarding dental status of patients who never visited dentist previously (n=645)
Discussion
The study results showed that majority of the people visited a dentist >2 years ago followed by <2 years and more than 1 year ago. Similar results have been reported in some other studies.[4,5]
Time since the last dental visit represents dental care that was initiated by the people and therefore could reflect personal motivation and decision-making toward dental treatment. Not visiting a dentist regularly, at least once in a year, means that the people have poor preventive oral health practices and they delay visiting a dentist until they have an acute dental problem.
Although 6-monthly dental visits are recommended by most dentists, only a few individuals comply with this recommendation. Pain was the primary reason for visiting a dentist for the majority of people followed by the decayed teeth similar to many other studies.[6,7,8,9]
Education levels of patients seem to have a strong role in their dental visits. Among the people who had previously visited a dentist, 78% had education above high school level, whereas majority of the people who had never previously visited a dentist had education levels below the 7th grade (45%). Although this result shows a direct relationship between the educational status of patient and their dental visits, we cannot conclude that it is because of oral health education at schools and colleges, since only 4% of them visited dentist for routine checkup and majority of them visited for the reasons of pain and some other emergency.
Dental pain adversely affects the quality of life, normal functioning, and daily living of people, and most dental visits are aimed at immediate relief of pain. Majority of patients in India often visit dentist at the later stages of dental disease when symptoms such as pain and extreme discomfort appear, rather than earlier, i.e., a problem-oriented visit rather than a prevention-oriented one. Very few people interviewed said that they had visited a dentist for routine oral examination. This shows that people do not believe in the value of regular dental visits and they need to be educated toward the preventive aspects of dentistry.
During their previous dental visits, majority of the people had received dental restorations (46%) followed by oral prophylaxis (26%). This may indicate that patients present themselves for care at the later stage of dental disease, where noninterventive, preventive procedures are not effective. This kind of early intervention may result in earlier endodontic treatment and also may also result in earlier tooth loss.
The most frequently cited reason for not visiting a dentist was lack of oral health knowledge (30%) followed by a dental problem that was not severe enough to initiate a dental visit (23%). This shows that people do not go to a dentist unless the symptoms are severe enough to visit a dentist. Majority of the Indian population perceive dentistry as a useful service only when necessary but is not a crucial part of overall health.[10] This kind of belief that there was no need to visit a dentist unless pain was present was reported in some other studies also.[4] The neglect of dental problems that were not severe enough was the second most commonly cited reason for not visiting a dentist. This shows the low priority given to oral problems as people think dental problems are not life-threatening.
Lack of time without interference with daily routine or work was another reason reported in our study for not visiting a dentist. This finding is similar to that of a study reported from Malaysia.[8] A visit to a dentist may lead to the loss of wages for salaried people. Getting sick leave for dental problems may be difficult as they are not considered to be serious enough to take a leave. Similar to the results of many studies, the cost of treatment was reported as a barrier for using dental services by 12% of people.[11,12]
Although the dental services are offered at a reasonable fee, majority of Indians do not have personal health insurance policies when compared to the Western countries. Noncoverage of dental disease in the majority of medical insurance policies in India is another factor toward these financial constraints to a dental visit at an earlier stage where preventive treatment would be effective.
One surprising finding of the study was that the fear of dentist or dental treatment was cited by a very few people as a reason for not visiting the dentist. Contrary to the finding in this study, fear has been reported as a significant barrier for utilization of dental services in many studies from developed countries.[4,5] This may be because of uncanny faith toward a doctor among Indian population.
One limitation of the study is that it was a self-report survey. Hence, there is a possibility of response bias. Since the study was performed on patients visiting a private dental clinic where majority of patients represented moderate or higher economic status and employed deliberate sampling, the results cannot be generalized at the community level. The study may provide an initial step in understanding which variables are important in the utilization or nonutilization of dental care, since understanding treatment-seeking behavior is a complex process.
It is necessary to do further studies and extend the analysis to a larger sample of individuals at different socioeconomical and community levels.
Conclusion
Despite an increase in the rate of people visiting dentists among urban population of India, widespread disparities exist in the provision of care to poor and populations with lower levels of education because of a cluster of access and financial issues.
Lack of knowledge, negligence, and financial constraints were the main reasons for not seeking care early. Education on the importance of early reporting to dental facility for care is recommended. Prevention needs to be at the front line of oral health care, with systematic approaches that cross oral health profession. Availability of coverage and provider reimbursement rates and dental awareness programs for general population seem to make a difference in access to care and in quality of care.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank all the patients participated in the study.
References
- 1.Petersen PE. Global policy for improvement of oral health in the 21st century – Implications to oral health research of World Health Assembly 2007, World Health Organization. Community Dent Oral Epidemiol. 2009;37:1–8. doi: 10.1111/j.1600-0528.2008.00448.x. [DOI] [PubMed] [Google Scholar]
- 2.Stewart DC, Ortega AN, Dausey D, Rosenheck R. Oral health and use of dental services among Hispanics. J Public Health Dent. 2002;62:84–91. doi: 10.1111/j.1752-7325.2002.tb03427.x. [DOI] [PubMed] [Google Scholar]
- 3.Jamieson LM, Thomson WM. The dental neglect and dental indifference scales compared. Community Dent Oral Epidemiol. 2002;30:168–75. doi: 10.1034/j.1600-0528.2002.300302.x. [DOI] [PubMed] [Google Scholar]
- 4.Al-Shammari KF, Al-Ansari JM, Al-Khabbaz AK, Honkala S. Barriers to seeking preventive dental care by Kuwaiti adults. Med Princ Pract. 2007;16:413–9. doi: 10.1159/000107733. [DOI] [PubMed] [Google Scholar]
- 5.Manski RJ, Magder LS. Demographic and socioeconomic predictors of dental care utilization. J Am Dent Assoc. 1998;46:432–9. doi: 10.14219/jada.archive.1998.0177. [DOI] [PubMed] [Google Scholar]
- 6.Cohen LA, Bonito AJ, Eicheldinger C, Manski RJ, Macek MD, Edwards RR, et al. Behavioral and socioeconomic correlates of dental problem experience and patterns of health care-seeking. J Am Dent Assoc. 2011;142:137–49. doi: 10.14219/jada.archive.2011.0056. [DOI] [PubMed] [Google Scholar]
- 7.Ekanayake L, Mendis R. Self reported use of dental services among employed adults in Sri Lanka. Int Dent J. 2002;52:151–5. doi: 10.1111/j.1875-595x.2002.tb00620.x. [DOI] [PubMed] [Google Scholar]
- 8.Jaafar N, Jalalluddin RL, Razak IA, Esa R. Investigation of delay in utilization of government dental services in Malaysia. Community Dent Oral Epidemiol. 1992;20:144–7. doi: 10.1111/j.1600-0528.1992.tb01549.x. [DOI] [PubMed] [Google Scholar]
- 9.Kuthy RA, Odom JG, Salsberry PJ, Nickel JL, Polivka BJ. Dental utilization by low-income mothers. J Public Health Dent. 1998;58:44–50. doi: 10.1111/j.1752-7325.1998.tb02989.x. [DOI] [PubMed] [Google Scholar]
- 10.Devaraj C, Eswar P. Reasons for use and non-use of dental services among people visiting a dental college hospital in India: A descriptive cross-sectional study. Eur J Dent. 2012;6:422–7. [PMC free article] [PubMed] [Google Scholar]
- 11.Pedersen PH, Vigild M, Nitschke I, Berkey DB. Dental care for aging populations in Denmark, Sweden, Norway, United Kingdom and Germany. J Dent Educ. 2005;69:987–97. [PubMed] [Google Scholar]
- 12.Heaton LJ, Smith TA, Raybould TP. Factors influencing use of dental services in rural and urban communities: Considerations for practitioners in underserved areas. J Dent Educ. 2004;68:1081–9. [PubMed] [Google Scholar]