

Abstract
Context:
Patients who undergo anterior cruciate ligament reconstruction (ACLR) present with strength and biomechanical deficits at return to activity (RTA). Deficits in strength and biomechanical symmetry impair function during activity and may predispose patients to subsequent injury.
Objective:
To compare strength and biomechanical function in patients with ACLR at RTA and more than 12 months post-ACLR.
Design:
Descriptive laboratory study.
Setting:
Research laboratory.
Patients or Other Participants:
A total of 20 participants (12 females, 8 males; age = 21.40 ± 5.60 years, height = 171.3 ± 10.2 cm, mass = 73.21 ± 19.41 kg) who had undergone ACLR and were cleared to RTA were recruited.
Intervention(s):
Strength was measured during knee extension and evaluated by the isometric and isokinetic quadriceps index. Biomechanical function was evaluated using symmetry values for sagittal-plane knee-joint rotations, changes in sagittal-plane knee-joint rotation, knee-extension moments, and changes in knee-extension moment that were recorded during a single-legged forward hop.
Main Outcome Measure(s):
Self-reported function was measured using the International Knee Documentation Committee Subjective Knee Evaluation Form. Participants were assessed at RTA (212.25 ± 28.11 days) and more than 12 months post-ACLR (556.25 ± 230.89 days).
Results:
At RTA, strength and biomechanical values were less than 80% symmetric. We observed improvements from RTA to more than 12 months post-ACLR for the isometric quadriceps index (F1,18 = 29.22, P < .001), isokinetic quadriceps index (F1,18 = 10.88, P = .004), sagittal-plane knee-joint rotations (F1,19 = 9.58, P = .006), change in sagittal-plane knee-joint rotations (F1,19 = 7.83, P = .01), knee-extension moments (F1,19 = 5.73, P = .03), change in knee-extension moments (F1,19 = 21.10, P < .001), and self-perceived function (F1,19 = 11.50, P = .003). Of the 7 variables that showed improvement at more than 12 months post-ACLR, only 3 met the recommended criteria (≥90%).
Conclusions:
Patients with ACLR showed asymmetry in strength and biomechanics at RTA. These asymmetries, along with self-perceived function, improved over time. However, despite improvements in strength and biomechanics at RTA, asymmetries of more than 10% were still present more than 12 months post-ACLR.
Key Words: asymmetry, return to activity, recurrent injury
Key Points
Patients with anterior cruciate ligament reconstruction (ACLR) had asymmetries in knee strength and biomechanics upon return to activity that were improved at more than 12 months post-ACLR.
Knee symmetry for several variables remained lower than the suggested standard of 90% more than 12 months post-ACLR.
More stringent criteria may be needed to clear patients for a safe return to activity post-ACLR.
Strength and biomechanical symmetry continued to improve over time after the patients were released from formal rehabilitation.
Anterior cruciate ligament (ACL) injuries continue to be highly prevalent in the United States, with approximately 250 000 occurring annually.1 The most common intervention for ACL rupture is reconstructive surgery to replace the damaged ligament and restore static stability to the knee. Patients who undergo ACL reconstruction (ACLR) are typically allowed to return to activity (RTA) at around 6 months postsurgery2 despite lingering deficits in strength and biomechanical function. In fact, at the time of RTA, patients often display substantial quadriceps weakness, with reported deficits exceeding 20% for the knee extensors when compared with the contralateral uninvolved limb.3–6 Biomechanical asymmetries are also present in this population during basic movements such as walking and jogging.7
Currently, no consensus exists on RTA criteria for patients with ACLR. Generally, the protocols that dictate a patient's RTA vary depending on the physician who performed the surgery and the rehabilitation facility the patient attends. Further increasing the difficulty of assessing consistencies in RTA protocols is the lack of reporting of the criteria used to clear patients for RTA. In a review, Barber-Westin and Noyes2 reported that in 40% of studies, no RTA criteria for patients with ACLR were listed. The assessments most commonly used for RTA protocols include a general orthopaedic examination of knee range of motion, joint effusion, a static knee-stability test (eg, Lachman test), and the length of time since surgery.2 However, whereas patients may have full range of motion, no apparent joint effusion, and anterior tibiofemoral translation within normal limits, deficits in strength and biomechanical function are likely still present.7
Returning to activity while deficient in strength, biomechanical function, or both may predispose the patient to reinjury or contralateral limb injury.2,8–10 Grindem et al10 recently reported that the rate of reinjury decreased with each month up to 9 months postsurgery that a patient with ACLR delayed RTA. Furthermore, these researchers10 also noted that participants who returned to sport with quadriceps strength symmetry and functional symmetry greater than 90% had an 84% reduced reinjury rate. Conversely, participants who had poor quadriceps strength symmetry and poor functional hop-test symmetry scores had an increased risk of reinjury.10 Deficits in quadriceps strength have been linked to poor biomechanical function.4,7 Participating in sports or demanding activity when strength10 and biomechanical asymmetries11 are present increases the risk of reinjury. Some investigators9 have even shown that the risk of injury to the contralateral limb post-ACLR is equal to that of the repaired limb. Prolonged deficits in quadriceps strength of patients with ACLR have also been linked to the onset of posttraumatic osteoarthritis.12
Researchers3,13,14 have suggested that patients with ACLR continue to show quadriceps strength improvement in the months after their RTA. This continued improvement is of particular interest because of the relationship between strength and biomechanical function. Quadriceps strength symmetry has been correlated with knee biomechanics and specifically related to symmetric peak knee flexion during gait and jump landings.4,7,15 It logically follows that, as strength improves over time, biomechanical function improves. With the continued recovery of strength and biomechanics occurring beyond the standard clearance time frame, it may be prudent for clinicians to use a criterion-based RTA assessment for patients with ACLR to obtain a better outcome with less risk of reinjury. Therefore, the purpose of our study was to examine the continued recovery of strength and biomechanical symmetry at the time of RTA and then at more than 12 months post-ACLR. We believed that comparing strength and biomechanics at these times would allow us to ascertain whether improvements continued to occur after patients were released from rehabilitation. We hypothesized that ACL limb deficits in strength and biomechanics would be present in patients with ACLR at the time of RTA and that these deficits would diminish with time.
METHODS
Participants
A total of 20 volunteers (12 females, 8 males; age = 21.40 ± 5.60 years, height = 171.3 ± 10.2 cm, mass = 73.21 ± 19.41 kg) participated in our study as part of a larger investigation aimed at understanding muscle dysfunction after ACL injury (Table 1).16 All patients included in this substudy of our larger investigation had already participated in RTA testing, and we contacted them to participate in additional testing when they were at least 12 months post-ACLR. Patients were eligible for the larger study if they (1) were from 14 to 45 years of age, (2) were planning to complete rehabilitation at our sports medicine clinic, (3) had an acute ACL injury, (4) had no previous history of knee surgery, (5) had no history of previous knee-ligament injury, (6) were not pregnant, and (7) had no history of a heart condition. The ACL was reconstructed using a bone–patellar tendon–bone autograft in 17 participants and a semitendinosus-gracilis graft in 3 participants. One of 3 orthopaedic surgeons from our sports medicine clinic performed all reconstructions. All participants provided written assent or consent, and the legal guardian(s) of participants aged less than 18 years provided written informed consent. The study was approved by the University of Michigan Medical School Institutional Review Board.
Table 1.
Participant Demographic Data, Tegner Activity Scale Scores, Strength Data, and International Knee Documentation Committee Subjective Knee Evaluation Form Scores for Return to Activity and >12 Months After Anterior Cruciate Ligament Reconstruction Extended on Next Page
| Return to Activity |
|||||||||||||
| Participant Identification No. |
Demographics |
Preinjury Tegner Activity Scale Score |
Time After Anterior Cruciate Ligament Reconstruction, d |
Tegner Activity Scale Score |
Sagittal-Plane Knee-Joint Rotation Symmetry |
Knee-Extension Moment Symmetry |
Quadriceps Index |
||||||
| Sex |
Age, y |
Return to Activity? |
Sport |
Area Under the Curve |
Slope |
Area Under the Curve |
Slope |
Isometric |
Isokinetic |
||||
| 49 | Female | 16 | Yes | Softball | 9 | 259 | 9 | 76.25 | 77.67 | 74.76 | 75.41 | 60.83 | 87.54 |
| 57 | Female | 19 | Yes | Basketball | 9 | 233 | 7 | 87.60 | 93.73 | 81.94 | 89.95 | 70.46 | 58.75 |
| 58 | Female | 22 | Yes | Skiing | 7 | 276 | 4 | 71.98 | 67.59 | 45.83 | 56.28 | 78.37 | 94.22 |
| 64 | Female | 15 | No | Soccer | 8 | 199 | 6 | 91.50 | 81.29 | 80.85 | 91.05 | 83.72 | 97.18 |
| 72 | Male | 38 | Yes | Basketball | 7 | 220 | 7 | 78.98 | 46.47 | 60.33 | 58.53 | 65.73 | 85.01 |
| 74 | Male | 25 | Yes | Flag football | 8 | 223 | 8 | 63.49 | 94.98 | 77.79 | 73.12 | 60.07 | 43.44 |
| 77 | Female | 24 | No | Beach volleyball | 8 | 247 | 7 | 88.59 | 84.84 | 71.44 | 77.59 | 50.66 | 69.33 |
| 81 | Female | 24 | No | Soccer | 7 | 201 | 4 | 68.01 | 85.30 | 55.19 | 74.59 | 48.65 | 64.53 |
| 87 | Male | 16 | Yes | Cycling | 8 | 204 | 5 | 92.18 | 96.29 | 85.88 | 84.93 | 70.35 | 107.77 |
| 88 | Female | 23 | No | Skiing | 6 | 194 | 5 | 73.84 | 80.63 | 60.88 | 65.97 | 60.13 | 111.83 |
| 91 | Female | 18 | No | Ultimate | 9 | 169 | 5 | 50.36 | 63.17 | 42.51 | 64.00 | 74.59 | 75.98 |
| 92 | Female | 15 | Yes | Gymnastics | 9 | 206 | 9 | 82.32 | 72.64 | 57.94 | 63.92 | 69.41 | 95.04 |
| 95 | Female | 19 | No | Bouncy house | 7 | 247 | 7 | 74.81 | 89.39 | 73.67 | 101.43 | 80.34 | 103.60 |
| 96 | Male | 28 | Yes | Tae kwon do | 10 | 210 | 8 | 93.25 | 93.11 | 56.54 | 65.27 | 84.27 | 62.00 |
| 97 | Male | 22 | No | Soccer | 7 | 202 | 5 | 71.21 | 77.67 | 97.95 | 87.43 | 65.24 | 84.10 |
| 99 | Male | 23 | Yes | Soccer | 9 | 180 | 6 | 84.37 | 79.15 | 86.72 | 77.13 | 75.16 | 79.30 |
| 102 | Male | 24 | Yes | Basketball | 9 | 204 | 8 | 82.35 | 89.88 | 74.61 | 77.32 | 45.20 | 39.81 |
| 107 | Female | 17 | Yes | Soccer | 10 | 181 | 8 | 93.26 | 85.13 | 63.02 | 75.20 | 81.68 | 81.39 |
| 109 | Female | 25 | Yes | Soccer | 7 | 182 | 6 | 90.79 | 83.18 | 77.51 | 86.47 | 91.58 | 95.98 |
| 111 | Male | 15 | Yes | Football | 7 | 208 | 7 | 100.38 | 86.46 | 100.62 | 92.13 | 74.86 | 46.28 |
Abbreviation: NA, not available.
Table 1.
Extended From Previous Page
| Return to Activity |
>12 Months After Anterior Cruciate Ligament Reconstruction |
||||||||||
| International Knee Documentation Committee Subjective Knee Evaluation Form Score |
Central Activation Ratio |
Time After Anterior Cruciate Ligament Reconstruction, d |
Tegner Activity Scale Score |
Sagittal-Plane Knee-Joint Rotation Symmetry |
Knee-Extension Moment Symmetry |
Quadriceps Index |
International Knee Documentation Committee Subjective Knee Evaluation Form Score |
Central Activation Ratio |
|||
| Area Under the Curve |
Slope |
Area Under the Curve |
Slope |
Isometric |
Isokinetic |
||||||
| 95.40 | 80.13 | 1036 | 4 | 124.82 | 87.47 | 82.96 | 86.55 | 105.02 | 96.36 | 98.85 | 99.15 |
| 91.95 | 92.42 | 1091 | 9 | 100.10 | 101.01 | 91.87 | 106.58 | 93.93 | 74.57 | 98.85 | 98.82 |
| 82.76 | 82.58 | 890 | 7 | 100.35 | 74.52 | 67.37 | 81.93 | 95.92 | 124.65 | 93.10 | 94.52 |
| 87.36 | 97.80 | 766 | 5 | 143.86 | 96.96 | 121.98 | 103.49 | 90.45 | 82.80 | 95.40 | 88.15 |
| 86.21 | 85.27 | 759 | 7 | 98.90 | 85.56 | 80.13 | 95.93 | 96.96 | 107.84 | 95.40 | 99.04 |
| 82.76 | 92.11 | 587 | 8 | 65.77 | 88.50 | 52.39 | 70.13 | 61.82 | 54.07 | 81.61 | 86.93 |
| 78.16 | 93.18 | 569 | 8 | 105.64 | 94.08 | 95.77 | 95.25 | 62.59 | 125.89 | 93.10 | 93.59 |
| 87.36 | 86.76 | 532 | 5 | 89.69 | 85.68 | 64.31 | 80.55 | 72.80 | 100.38 | 68.97 | 91.83 |
| 80.46 | 89.63 | 507 | 7 | 89.46 | 103.47 | 92.79 | 100.75 | NA | NA | 89.66 | 93.00 |
| 80.46 | 98.63 | 460 | 6 | 71.00 | 74.38 | 67.85 | 73.22 | 127.25 | 103.12 | 93.10 | 97.66 |
| 77.01 | 96.60 | 504 | 9 | 78.52 | 85.49 | 73.92 | 92.88 | 98.55 | 109.25 | 98.85 | 90.49 |
| 91.95 | 88.36 | 409 | 9 | 85.16 | 85.41 | 72.47 | 80.39 | 82.29 | 95.93 | 95.40 | 94.42 |
| 87.36 | 98.98 | 387 | 6 | 89.60 | 83.79 | 89.98 | 104.95 | 88.78 | 89.10 | 91.95 | 99.10 |
| 83.91 | 99.53 | 416 | 10 | 90.24 | 93.24 | 74.45 | 77.90 | 92.31 | 78.06 | 91.95 | 95.36 |
| 74.71 | 93.89 | 354 | 7 | 60.23 | 78.04 | 75.65 | 91.50 | 75.24 | 102.92 | 91.95 | 91.33 |
| 82.76 | 90.91 | 354 | 9 | 103.66 | 89.50 | 87.06 | 68.88 | 88.28 | 87.86 | 85.06 | 96.55 |
| 89.66 | 84.03 | 365 | 7 | 82.48 | 81.88 | 58.54 | 65.96 | 56.99 | 41.04 | 81.61 | 92.34 |
| 94.25 | 99.95 | 398 | 8 | 141.11 | 89.79 | 102.18 | 101.95 | 108.28 | 103.41 | 97.70 | 99.11 |
| 80.46 | 98.46 | 372 | 7 | 82.08 | 91.75 | 93.11 | 106.74 | 98.46 | 93.15 | 100.00 | 96.33 |
| 73.56 | 90.72 | 369 | 7 | 87.84 | 95.26 | 82.76 | 104.19 | 90.22 | 104.35 | 87.36 | 96.11 |
Postoperative Rehabilitation and Testing Time Frame
All participants adhered to the same clinical postoperative rehabilitation protocol, which consisted of 2 to 3 sessions weekly. The rehabilitation protocol began with the initial postoperative visit (6.5 ± 2.9 days) and ended approximately 7 months post-ACLR (197.53 ± 28.92 days). The focus during the early stages was improving range of motion and progressed to muscle strengthening, quadriceps re-education, and functional exercise. The protocol was varied for each patient depending on his or her response to treatment.
A patient's ability to RTA was assessed after he or she completed the standard-of-care physical therapy protocol. To be considered for clearance, patients had to display appropriate joint laxity, no effusion, and full range of motion. Next, they had to complete a leg-press test and an agility program. The leg-press test required patients to perform 15 repetitions of a single-legged leg press using the ACLR limb with a load equal to 100% of body weight. A leg-press repetition was deemed acceptable only if the patient achieved 90° of knee flexion and returned to a neutral resting position. For the agility program, patients completed 3 weeks of agility-type activities. The program began with 6 exercises (week 1) and progressed to 9 exercises (week 2) and then 12 exercises (week 3).17 Exercises consisted of activities such as skipping (forward and backward), running (forward and backward), cariocas, cutting, shuttle runs, and double-legged hops.
Completion of the agility program was considered successful when patients could complete all sets and repetitions of the exercises with the highest degree of difficulty without pain or swelling of the involved knee. Patients who could not successfully complete either the agility program or the leg-press test were denied clearance for RTA. These patients continued their rehabilitation protocols and agility programs until they met the RTA criteria. Patients were not allowed to participate in the study until they met the RTA criteria.
All participants attended 2 testing sessions. The first session occurred after patients had been cleared for RTA (212.25 ± 28.11 days; range, 169–276 days), and the second occurred at more than 12 months post-ACLR (556.44 ± 230.89 days; range, 354–1091 days; Table 1). At each session, they underwent testing for quadriceps strength, quadriceps activation, knee-joint biomechanics, and patient-perceived function.
Quadriceps Strength and Activation Assessment
Quadriceps activation was measured using the superimposed-burst technique and quantified using the central activation ratio (CAR). Participants were seated in a dynamometer (model System 3; Biodex Medical Systems, Shirley, NY) with their hips and knees flexed to 90°, torsos secured to the chair, and test limbs fixed to the dynamometer arm per the manufacturer's guidelines. Electrodes (model Dura-Stick II [7 × 13 cm]; Chattanooga Group, Hixson, TN) were placed on the proximal vastus lateralis and distal vastus medialis. Participants were instructed to perform a maximal voluntary isometric contraction (MVIC) by kicking out as hard as possible while visualizing their torque in a custom-written program (LabVIEW version 8.5; National Instruments, Austin, TX). The MVIC trials were repeated until no increase in torque was apparent (a minimum of 3 contractions were always performed) and recorded for quantification of isometric quadriceps strength. Next, we instructed participants to complete 3 additional MVIC trials in which they held the contraction for approximately 5 seconds. During these additional trials, the LabView program triggered a supramaximal stimulus (model S88 Dual Output Square Pulse Stimulator/SIU8T Stimulus Isolation Unit; Grass Technologies, West Warrick, RI) to the quadriceps as performed in a previous study.15 The stimulus was delivered after the MVIC was reached and subsequently decreased by 1 Nm. The intrasession and intrarater reliability in patients with ACLR for isometric, isokinetic, and CAR values in our laboratory were excellent (intraclass correlation coefficient >0.90). The intersession reliability for patients with ACLR (sessions were separated by 2 to 5 days) was also excellent (intraclass correlation coefficient = 0.92).
Both isometric strength and CAR were calculated from the trials described. The isometric quadriceps index was calculated ([injured limb / uninjured limb] × 100) using the peak torque values recorded across the nonstimulation trials for each limb. The CAR was calculated (CAR = [MVIC / MVIC + superimposed burst] × 100) using both the peak MVIC torque and the peak MVIC with supramaximal stimulus torque; a value of 100 represented complete quadriceps activation.18
Bilateral isokinetic quadriceps strength was assessed using the dynamometer. Participants were secured in the dynamometer as in the isometric and superimposed-burst trials with the hip and knee flexed to 90°. Before performing the trial, they were instructed on the basic principles of isokinetic strength testing and asked to perform 3 submaximal knee extensions as a warm-up. After the warm-up, patients rested for 2 minutes and then performed 3 maximal concentric knee extensions at a speed of 60°/s. The highest torque of the 3 attempts was recorded for each limb and input to quantify the isokinetic quadriceps index ([injured limb / uninjured limb] × 100) for use in our statistical analyses. The order of limb testing was counterbalanced for all of the preceding dynamometer-involved tests, with the isokinetic strength trials performed after the isometric and superimposed-burst trials.
Single-Legged Forward Hop
Biomechanical data collection was accomplished using a motion-capture system (model Vicon MX; Oxford Metrics, London, United Kingdom) sampling at 240 Hz in conjunction with a force platform (model OR6-7; Advanced Mechanical Technologies Inc, Watertown, MA) sampling at 1200 Hz. We selected the single-legged forward hop for analysis because it places a large demand on the quadriceps muscle and, therefore, is preferable to walking gait, which would impose much less quadriceps demand. Participants wore comfortable athletic shoes during testing. We instructed them to hop forward onto the center of the force platform and “stick” the landing. The hop distance was normalized for each participant to 100% of his or her lower limb length.19 Participants were required to complete 3 successful hops for each limb. For a hop trial to be deemed successful, they had to hold their landing until balance was fully regained and maintained for 1 second with ground contact of the foot of the involved limb only. A trial was deemed unsuccessful if the participant missed the force platform or was unable to maintain balance on landing. The order of limb testing was counterbalanced.
Biomechanical Data Processing
Sagittal-plane knee-joint rotations (ie, knee-flexion angles) were determined using a 3-dimensional coordinate system and retroreflective markers. The markers were placed bilaterally in precise locations on the foot (calcaneus, dorsal navicular, head of the first metatarsal, and head of the fifth metatarsal), leg (tibial tuberosity, distal shank, lateral shank, medial malleoli, and lateral malleoli), thigh (greater trochanter, distal thigh, medial femoral epicondyle, and lateral femoral epicondyle), and pelvis (anterior-superior iliac spine, posterior-superior iliac spine, and iliac crest). Each participant performed a static trial that was recorded by the 3-dimensional coordinate system to generate a kinematic model of the hips and lower limbs using Visual3D software (version 4.0; C-Motion, Rockville, MD). The model provides 3 degrees of freedom for the knee and is the basis for comparing the marker trajectories during each single-legged hop trial. All knee-joint rotations were calculated in accordance with the Cardan rotation sequence (XYZ), with sagittal-plane data referenced as X, frontal-plane data referenced as Y, and transverse-plane data referenced as Z.20 Specifically, knee flexion was quantified in negative degrees of rotation in the X-plane, in which full extension equals zero. Marker trajectories were synchronized with the ground reaction force data collected. Both were filtered with a fourth-order, zero-lag, low-pass Butterworth filter at a 12-Hz cutoff frequency.21 Sagittal-plane external knee moments were calculated using the inverse-dynamics approach via Visual3D and normalized to participant mass and height.
The landing phase for each single-legged hop trial was time normalized to 100% of stance for graphic purposes, with initial contact equating to the time when the vertical ground reaction force exceeded 10 N and the end of the landing equating to 250 milliseconds after initial contact.22 Data analysis was performed on the first 50% of stance (ie, 125 milliseconds) because this time interval captures the primary loading phases of the knee (ie, peak knee-extension moment and peak vertical ground reaction force) and is when individuals are believed to tear their ACLs.1 Ensemble averages were calculated for the first 50% of stance for all sagittal-plane knee-joint rotations and knee-extension moments.23 From these ensemble averages, the area under the curve (AUC) and the slope of the line (Figure 1) were calculated as previously described.16 Our reason for choosing the AUC over peak angle or moment values was explained in an earlier study.16 The slope of the line accounts for the change in the degrees of knee-joint flexion and knee-extension moments over the first 50% of stance. The AUC and slope of the line for both the knee-joint flexion and knee-extension moments were then converted into symmetry values using the same method as described for peak isokinetic torque.
Figure 1.

Area under the curve for the ensemble average of all participants for sagittal-plane knee-flexion angle during the landing at A, return to activity, and B, >12 months after anterior cruciate ligament reconstruction and for knee-extension moment during the landing at C, return to activity, and D, >12 months after anterior cruciate ligament reconstruction. Sagittal-plane knee flexion is represented in negative values, so the area under the curve is a negative value, as is the slope. Sagittal-plane knee-extension moment is referenced as external knee moments, so the area under the curve is a negative value, as is the slope. Abbreviation: SD, standard deviation.
International Knee Documentation Committee Subjective Knee Evaluation Form
Self-reported knee function was assessed using the International Knee Documentation Committee Subjective Knee Evaluation Form (IKDC). The IKDC is a questionnaire that is used to measure symptoms, athletic activity, daily activity, and general function for patients with knee injuries. The questionnaire contains 18 items scored in 1 of 3 ways: 11-point Likert scale, 5-point Likert scale, or dichotomous yes or no. After the participant completes the questionnaire, the scores are summed, and the total score is transformed to a value on a scale of 0 to 100, with 100 representing highest knee function. The transformed score was used for statistical analysis and is a reliable and valid measure of self-reported knee function after ACL injury.24
Statistical Analysis
We calculated separate 1 × 2 repeated-measures analyses of variance for between-limbs differences at RTA for biomechanical function (sagittal-plane knee-joint rotation AUC, sagittal-plane knee-joint rotation slope, knee-extension moment AUC, and knee-extension moment slope), strength (peak isokinetic quadriceps, peak isometric quadriceps), and muscle activation (CAR). The dependent variable in this statistical analysis was limb (ACL, healthy). We also performed separate 1 × 2 repeated-measures analyses of variance for biomechanical symmetry (sagittal-plane knee-joint rotation AUC, sagittal-plane knee-joint rotation slope, knee-extension moment AUC, knee-extension moment slope), strength (isokinetic quadriceps index, isometric quadriceps index), muscle activation (CAR), and self-perceived function (IKDC). The independent variable was testing time (RTA, >12 months post-ACLR). We set the α level a priori at ≤.05 for all tests. We used SPSS (version 22; IBM Corp, Armonk, NY) for all statistical analyses.
RESULTS
During data collection for 1 participant, a power outage occurred in the research facility and prevented us from performing muscle strength and activation trials for the uninvolved limb. Therefore, we were able to analyze quadriceps strength variables for only 19 participants; for all other variables, 20 participants were included in the statistical models.
At RTA, we observed differences between the ACL and healthy limbs for all biomechanical variables: sagittal-plane knee-joint rotation AUC (F1,19 = 47.61, P < .001), sagittal-plane knee-joint rotation slope (F1,19 = 48.23, P < .001), knee-extension moment AUC (F1,19 = 59.20, P < .001), and knee-extension moment slope (F1,19 = 65.13, P < .001). Between-limbs differences were also found in quadriceps strength and activation at RTA with peak isometric strength (F1,19 = 53.32, P < .001), peak isokinetic strength (F1,19 = 12.06, P = .003), and CAR (F1,19 = 9.60, P = .006). Means, standard deviations, and P values for between-limbs comparisons at RTA are reported in Table 2. All biomechanical symmetry variables exhibited improvement (ie, greater symmetry between limbs) from RTA to more than 12 months post-ACLR: sagittal-plane knee-joint rotation AUC (F1,19 = 9.58, P = .006), sagittal-plane knee-joint rotation slope (F1,19 = 7.83, P = .01), knee-extension moment AUC (F1,19 = 5.73, P = .03), and knee-extension moment slope (F1,19 = 21.10, P < .001). Quadriceps strength demonstrated improvement for both the isometric index (F1,18 = 29.22, P < .001) and isokinetic (F1,18 = 10.88, P = .004) quadriceps index. Self-perceived function also improved (F1,19 = 11.50, P = .003). Quadriceps activation did not improve over time according to the CAR (F1,19 = 2.81, P = .11).
Table 2.
Between-Limbs Differences at Return to Activity (Mean ± SD)
| Measure |
Limb |
P Value |
|
| Anterior cruciate ligament |
Healthy |
||
| Biomechanical function | |||
| Sagittal-plane knee-joint rotation | |||
| Area under the curve | −1162.33 ± 338.62 | −1432.14 ± 346.98 | <.001a |
| Slope | −0.789 ± 0.135 | −0.970 ± 0.099 | <.001a |
| Knee-extension moment | |||
| Area under the curve | −39.35 ± 9.41 | −55.74 ± 8.98 | <.001a |
| Slope | −0.038 ± 0.009 | −0.050 ± 0.008 | <.001a |
| Quadriceps strength, Nm | |||
| Peak isometric | 163.26 ± 58.45 | 237.14 ± 80.27 | <.001a |
| Peak isokinetic | 106.69 ± 31.84 | 151.06 ± 76.79 | .003a |
| Quadriceps muscle activation | |||
| Central activation ratio | 92.00 ± 6.08 | 95.75 ± 3.66 | .006a |
Difference between limbs at return to activity.
DISCUSSION
The purpose of our study was to determine whether strength and biomechanical function in patients with ACLR would improve from the time they were cleared to RTA until formal rehabilitation ceased at more than 12 months post-ACLR. Researchers3–5,10,11,15,25 have reported deficits in patients with ACLR at RTA. We hypothesized that the ACL limb would exhibit strength and biomechanical deficits compared with the healthy limb at RTA and that these deficits would decrease over time. Both hypotheses were confirmed.
At the time patients were cleared to RTA, a lack of sagittal-plane biomechanical symmetry was present for both the AUC and slope for knee-joint rotations and knee-extension moments (Table 2), revealing smaller values in the affected limb than in the unaffected limb. When examining peak knee flexion at 6 months postsurgery, Di Stasi et al25 observed that patients with ACLR who presented with similar asymmetries performed poorly during functional assessments. The asymmetry for the knee-extension moment AUC seen in our participants was similar to the findings of DeVita et al,26 who demonstrated less knee-extensor torque magnitude in the involved limb during gait, which coincided with altered knee function. The knee-flexion slope showed a lack of symmetry in the change of knee-flexion angle while landing, wherein the involved limb was unable to match the angular velocity of the uninvolved limb. Similarly, the asymmetric slope for knee-extension moment reflected the inability of the involved limb to match the rate of knee-extension force production compared with the uninvolved limb during landing. Given that healthy participants displayed symmetric knee biomechanics,16,27 we contend that the asymmetries stemmed from the ACL injury or ACLR, or both. All the knee biomechanical variables that we examined revealed asymmetries greater than 18%, which is more than the allowable 10% asymmetry suggested by Hartigan et al28 for patients with ACLR to return to sport participation. Our participants did not recover preinjury levels of biomechanical function at RTA and instead had biomechanical asymmetries similar to those found in other patients with ACLR that have been linked to secondary ACL injury.11
In addition to the biomechanical asymmetries noted, quadriceps strength asymmetries were present at RTA (Table 1, Figure 2). Lewek et al7 suggested that an acceptable strength level in patients with ACLR is a quadriceps index ≥90% and low or weak strength is characterized by a quadriceps index ≤80%. The group means of our 20 participants for the isometric and isokinetic quadriceps indices showed less than 80% symmetry at RTA, which was demonstrated by 15 participants for isometric quadriceps strength and 9 participants for isokinetic quadriceps strength (Table 1). This finding is supported by recent reports that patients with ACLR who had been cleared to RTA still presented with low values for both the isometric4,7 and isokinetic15 quadriceps index. The recurring findings of strength deficits at RTA indicate a problem that is widespread among those who undergo ACLR. No one has determined whether this deficit is due to ineffective strengthening techniques in the standard rehabilitation protocol or a limitation of the muscular structures' ability to recover strength by the standard RTA time frame.
Figure 2.
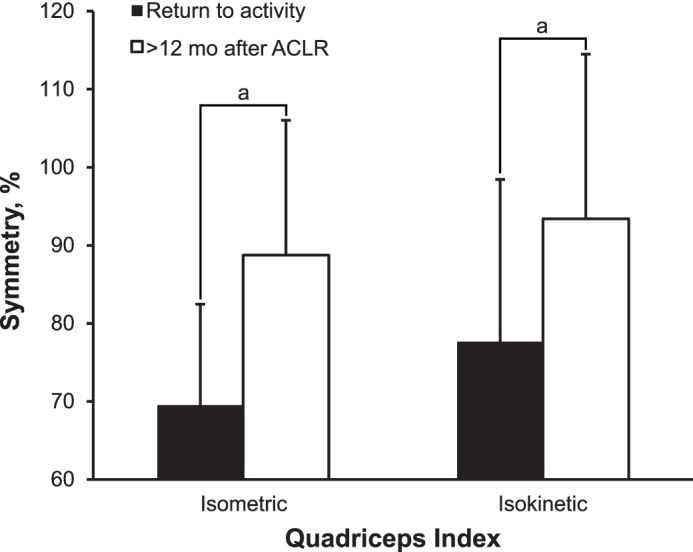
Quadriceps strength symmetry for participants at time of return to activity and at >12 months after anterior cruciate ligament reconstruction (ACLR). Data represent mean ± standard deviation. a Indicates improvements from return to activity to >12 months after ACLR.
Our participants presented at the RTA test date with a unilateral CAR of 92.00% ± 6.08%. Findings vary as to the maximum acceptable loss of muscle activation for biomechanical function. Snyder-Mackler et al29 noted the commonly cited minimum for healthy unilateral CAR of 95%, whereas Kuenze et al30 found a unilateral CAR greater than 89.3% was needed for healthy group membership among patients with ACLR at 6 months post-ACLR. The mean unilateral CAR of our participants met the criteria set by Kuenze et al30 and was within 1 standard deviation of the commonly cited minimum.29 With this in mind, we believe the presence of a muscle-activation deficit at RTA is still possible but unlikely. It is logical to infer that at RTA, the strength deficits displayed by our participants were not related to quadriceps activation but instead might have been related to changes in muscle volume, which have been found in previous research.5
After ACLR, a patient's perceived level of function is an important indicator of readiness for activity. The IKDC is often used to assess the level of function.24,31 The suggested standard for healthy function set forth by Irrgang et al32 is a score ≥90%. Our participants had an IKDC score of 84.43% ± 6.28% at the time of RTA. When considering the asymmetry found in both biomechanics and strength, we are not surprised that our participants scored less than the suggested standard for perceived function.
We found improvements from RTA to more than 12 months post-ACLR for all biomechanical (Figure 1), strength (Figure 2), and self-perceived function variables. Similar improvements over time have been noted through 12 months28,33 and 24 months34 postsurgery. However, Myer et al35 observed contrary findings: improvements in limb symmetry for single-legged vertical jump height and vertical ground reaction force in patients with ACLR were not related to the amount of time post-ACLR. The difference in findings between Myer et al35 and our own work may be the difference in the measures used to assess biomechanical function. We also tested participants twice, whereas Myer et al35 measured participants on only 1 occasion (8.2 to 11.3 months post-ACLR), limiting the ability to determine whether improvements would be seen as time progressed.
The improvements we found over time may be due to the participants returning to activity or the possible recovery of muscle volume. Of the 20 individuals in our study, 14 declared that they had returned to sport participation after completing their rehabilitation. Participation in physical activity and sports is known to improve muscle strength and biomechanical function.36–38 Muscle atrophy has been associated with strength deficits after ACLR and has been found to explain more of the variance in quadriceps strength than CAR.5 The contributions of muscle atrophy and activation failure together have been reported39 to account for 60% of quadriceps weakness. The mean unilateral CAR of our participants at RTA was within 3% of the suggested standard. It is thereby logical to infer that another factor, such as muscle atrophy, was contributing to the strength deficits in our participants and that recovery of muscle volume may have led to the strength improvements found after 12 months.
Whereas a slight improvement in mean CAR (2.69%) occurred between RTA and more than 12 months post-ACLR, it was not different. This was most likely due to the high initial unilateral CAR found at RTA, which was within 4% of the commonly cited minimum. With the percentage of muscle activation at RTA, it is not surprising that only a slight improvement was seen at more than 12 months post-ACLR.
Despite the substantial overall improvement in biomechanical function and quadriceps strength at more than 12 months post-ACLR, few variables met the previously discussed suggested criteria. Only sagittal-plane knee-joint rotation AUC (94.53% ± 21.94%), isokinetic quadriceps index (93.41% ± 21.08%), and self-perceived function (91.49% ± 7.58%) had mean values above the suggested standard of 90%. The remaining variables that showed improvement at more than 12 months post-ACLR had a mean range of 81.38% to 89.49%. If our participants were required to meet the aforementioned suggested standards (≥90% for biomechanical symmetry, strength symmetry, CAR symmetry, and self-perceived function and 95% for unilateral CAR) for all of our variables before RTA, none would have been cleared at our initial test date, and only 1 would have been cleared at more than 12 months post-ACLR. We contend that current rehabilitation paradigms are inadequate in targeting the mechanisms that lead to muscle weakness after ACLR. Possible improvements in rehabilitation strategies include early targeting of neurologic inhibition and lingering muscle atrophy, which may lead to superior gains in strength and biomechanical function.16,40 Furthermore, without changing rehabilitation paradigms, clinicians need to consider whether the time from surgery alone is appropriate for clearing a patient to RTA. Researchers suggested objective RTA criteria for quadriceps strength,7 biomechanical function,28 and muscle function.29 We strongly believe that these research-based objective measures of strength and biomechanical function should be used to establish an appropriate time frame for patients to RTA or competition.
Given the deficits found at RTA and more than 12 months post-ACLR, investigators need to re-evaluate the current path of care for patients with ACLR. The presence of strength, biomechanical, and functional deficits at RTA led us to question the efficacy of the current standard of release-to-activity criteria. As stated, many authors have not published their criteria for RTA.2 Among those who have published their criteria, large variations and no definitive consensus exist. The most common criteria for RTA are assessments of knee-joint effusion, range of motion, and laxity. These assessments in conjunction with a minimum time from surgery compose a typical release protocol. Whereas meeting these criteria at a satisfactory level is necessary for a minimum level of function during activity, these criteria do not consider strength and biomechanical symmetry. Therefore, a consensus on RTA criteria, including assessments that will evaluate these areas of function, is necessary. The current lack of consensus on the minimum criteria for RTA allows for large variations in patient outcomes and impairs the universal standard of care.
LIMITATIONS
Our study had limitations. A substantial variation in the time of testing existed for the more-than-12-months time frame, with an average time to testing of 556.25 days and a range of 354 to 1091 days. Our participants were a subgroup of a larger investigation. Recruiting for this study was performed by identifying patients in our database who were 12 months post-ACLR and beyond. Whereas this range in testing time undoubtedly led to variations in our main outcome measures, substantial improvements in strength, biomechanics, and self-perceived function were shown. In future work, collecting data serially between the time of RTA and approximately 24 months post ACLR would help indicate when patients generally achieve full strength and biomechanical symmetry.
Another limitation was the lack of specific data collected on patients' exercise levels, strengthening-program participation, and athletic activity between testing dates. A more in-depth analysis of the types of exercise participation may provide insight about which activities enhance functional improvement. Comparing the effects of activities of daily living and competitive athletics on the improvement found in the recovery of strength and biomechanical function is of particular interest. The relationship between recovery and patient participation in physical activity should be examined in future studies.
CONCLUSIONS
At the time of RTA, patients with ACLR had asymmetries in knee strength and biomechanics. We observed improvement in these asymmetries at more than 12 months post-ACLR. However, despite the improvements, several variables remained lower than the suggested standard of 90%. Our findings suggest that more stringent RTA criteria may be necessary to clear patients for safe RTA. Furthermore, improvements in strength and biomechanical symmetry occurred over time after the release from formal rehabilitation.
REFERENCES
- 1.Griffin LY, Albohm MJ, Arendt EA, et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med. 2006;34(9):1512–1532. doi: 10.1177/0363546506286866. [DOI] [PubMed] [Google Scholar]
- 2.Barber-Westin SD, Noyes FR. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27(12):1697–1705. doi: 10.1016/j.arthro.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 3.Palmieri-Smith RM, Thomas AC, Wojtys EM. Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med. 2008;27(3):405–424. doi: 10.1016/j.csm.2008.02.001. vii–ix. [DOI] [PubMed] [Google Scholar]
- 4.Schmitt LC, Paterno MV, Ford KR, Myer GD, Hewett TE. Strength asymmetry and landing mechanics at return to sport after anterior cruciate ligament reconstruction. Med Sci Sports Exerc. 2015;47(7):1426–1434. doi: 10.1249/MSS.0000000000000560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thomas AC, Wojtys EM, Brandon C, Palmieri-Smith RM. Muscle atrophy contributes to quadriceps weakness after anterior cruciate ligament reconstruction. J Sci Med Sport. 2016;19(1):7–11. doi: 10.1016/j.jsams.2014.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lepley LK, Palmieri-Smith RM. Pre-operative quadriceps activation is related to post-operative activation, not strength, in patients post-ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):236–246. doi: 10.1007/s00167-014-3371-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lewek M, Rudolph K, Axe M, Snyder-Mackler L. The effect of insufficient quadriceps strength on gait after anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon) 2002;17(1):56–63. doi: 10.1016/s0268-0033(01)00097-3. [DOI] [PubMed] [Google Scholar]
- 8.Laboute E, Savalli L, Puig P, et al. Analysis of return to competition and repeat rupture for 298 anterior cruciate ligament reconstructions with patellar or hamstring tendon autograft in sportspeople. Ann Phys Rehabil Med. 2010;53(10):598–614. doi: 10.1016/j.rehab.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 9.Wright RW, Dunn WR, Amendola A, et al. Risk of tearing the intact anterior cruciate ligament in the contralateral knee and rupturing the anterior cruciate ligament graft during the first 2 years after anterior cruciate ligament reconstruction: a prospective MOON cohort study. Am J Sports Med. 2007;35(7):1131–1134. doi: 10.1177/0363546507301318. [DOI] [PubMed] [Google Scholar]
- 10.Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804–808. doi: 10.1136/bjsports-2016-096031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Paterno MV, Schmitt LC, Ford KR, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38(10):1968–1978. doi: 10.1177/0363546510376053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tourville TW, Jarrell KM, Naud S, Slauterbeck JR, Johnson RJ, Beynnon BD. Relationship between isokinetic strength and tibiofemoral joint space width changes after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(2):302–311. doi: 10.1177/0363546513510672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lepley LK. Deficits in quadriceps strength and patient-oriented outcomes at return to activity after ACL reconstruction: a review of the current literature. Sports Health. 2015;7(3):231–238. doi: 10.1177/1941738115578112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Logerstedt D, Di Stasi S, Grindem H, et al. Self-reported knee function can identify athletes who fail return to activity criteria up to 1 year after anterior cruciate ligament reconstruction: a Delaware-Oslo ACL cohort study. J Orthop Sports Phys Ther. 2014;44(12):914–923. doi: 10.2519/jospt.2014.4852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Palmieri-Smith RM, Lepley LK. Quadriceps strength asymmetry after anterior cruciate ligament reconstruction alters knee joint biomechanics and functional performance at time of return to activity. Am J Sports Med. 2015;43(7):1662–1669. doi: 10.1177/0363546515578252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lepley LK, Wojtys EM, Palmieri-Smith RM. Combination of eccentric exercise and neuromuscular electrical stimulation to improve biomechanical limb symmetry after anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon) 2015;30(7):738–747. doi: 10.1016/j.clinbiomech.2015.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lepley LK, Wojtys EM, Palmieri-Smith RM. Does concomitant meniscectomy or meniscal repair affect the recovery of quadriceps function post-ACL reconstruction? Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2756–2761. doi: 10.1007/s00167-014-3093-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kent-Braun JA, Le Blanc R. Quantitation of central activation failure during maximal voluntary contractions in humans. Muscle Nerve. 1996;19(7):861–869. doi: 10.1002/(SICI)1097-4598(199607)19:7<861::AID-MUS8>3.0.CO;2-7. [DOI] [PubMed] [Google Scholar]
- 19.Webster KE, Gonzalez-Adrio R, Feller JA. Dynamic joint loading following hamstring and patellar tendon anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2004;12(1):15–21. doi: 10.1007/s00167-003-0400-9. [DOI] [PubMed] [Google Scholar]
- 20.Cole GK, Nigg BM, Ronsky JL, Yeadon MR. Application of the joint coordinate system to three-dimensional joint attitude and movement representation: a standardization proposal. J Biomech Eng. 1993;115(4A):344–349. doi: 10.1115/1.2895496. [DOI] [PubMed] [Google Scholar]
- 21.Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in “high-risk” versus “low-risk” athletes. BMC Musculoskelet Disord. 2007;8:39. doi: 10.1186/1471-2474-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McLean SG, Fellin RE, Suedekum N, Calabrese G, Passerallo A, Joy S. Impact of fatigue on gender-based high-risk landing strategies. Med Sci Sports Exerc. 2007;39(3):502–514. doi: 10.1249/mss.0b013e3180d47f0. [DOI] [PubMed] [Google Scholar]
- 23.McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech (Bristol, Avon) 2004;19(8):828–838. doi: 10.1016/j.clinbiomech.2004.06.006. [DOI] [PubMed] [Google Scholar]
- 24.van Meer BL, Meuffels DE, Vissers MM, et al. Knee injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: which questionnaire is most useful to monitor patients with an anterior cruciate ligament rupture in the short term? Arthroscopy. 2013;29(4):701–715. doi: 10.1016/j.arthro.2012.12.015. [DOI] [PubMed] [Google Scholar]
- 25.Di Stasi SL, Logerstedt D, Gardinier ES, Snyder-Mackler L. Gait patterns differ between ACL-reconstructed athletes who pass return-to-sport criteria and those who fail. Am J Sports Med. 2013;41(6):1310–1318. doi: 10.1177/0363546513482718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.DeVita P, Hortobagyi T, Barrier J. Gait biomechanics are not normal after anterior cruciate ligament reconstruction and accelerated rehabilitation. Med Sci Sports Exerc. 1998;30(10):1481–1488. doi: 10.1097/00005768-199810000-00003. [DOI] [PubMed] [Google Scholar]
- 27.Teichtahl AJ, Wluka AE, Morris ME, Davis SR, Cicuttini FM. The associations between the dominant and nondominant peak external knee adductor moments during gait in healthy subjects: evidence for symmetry. Arch Phys Med Rehabil. 2009;90(2):320–324. doi: 10.1016/j.apmr.2008.07.030. [DOI] [PubMed] [Google Scholar]
- 28.Hartigan EH, Axe MJ, Snyder-Mackler L. Time line for noncopers to pass return-to-sports criteria after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2010;40(3):141–154. doi: 10.2519/jospt.2010.3168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Snyder-Mackler L, De Luca PF, Williams PR, Eastlack ME, Bartolozzi AR., III Reflex inhibition of the quadriceps femoris muscle after injury or reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am. 1994;76(4):555–560. doi: 10.2106/00004623-199404000-00010. [DOI] [PubMed] [Google Scholar]
- 30.Kuenze C, Hertel J, Saliba S, Diduch DR, Weltman A, Hart JM. Clinical thresholds for quadriceps assessment after anterior cruciate ligament reconstruction. J Sport Rehabil. 2015;24(1):36–46. doi: 10.1123/jsr.2013-0110. [DOI] [PubMed] [Google Scholar]
- 31.Spindler KP, Huston LJ, Wright RW, et al. MOON Group, Dunn WR. The prognosis and predictors of sports function and activity at minimum 6 years after anterior cruciate ligament reconstruction: a population cohort study. Am J Sports Med. 2011;39(2):348–359. doi: 10.1177/0363546510383481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Irrgang JJ, Anderson AF, Boland AL, et al. Responsiveness of the International Knee Documentation Committee Subjective Knee Form. Am J Sports Med. 2006;34(10):1567–1573. doi: 10.1177/0363546506288855. [DOI] [PubMed] [Google Scholar]
- 33.White K, Logerstedt D, Snyder-Mackler L. Gait asymmetries persist 1 year after anterior cruciate ligament reconstruction. Orthop J Sports Med. 2013;1(2):232596711349696. doi: 10.1177/2325967113496967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Abrams GD, Harris JD, Gupta AK, et al. Functional performance testing after anterior cruciate ligament reconstruction: a systematic review. Orthop J Sports Med. 2014;2(1):2325967113518305. doi: 10.1177/2325967113518305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Myer GD, Martin L, Jr, Ford KR, et al. No association of time from surgery with functional deficits in athletes after anterior cruciate ligament reconstruction: evidence for objective return-to-sport criteria. Am J Sports Med. 2012;40(10):2256–2263. doi: 10.1177/0363546512454656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Rochcongar P, Morvan R, Jan J, Dassonville J, Beillot J. Isokinetic investigation of knee extensors and knee flexors in young French soccer players. Int J Sports Med. 1988;9(6):448–450. doi: 10.1055/s-2007-1025049. [DOI] [PubMed] [Google Scholar]
- 37.Graf C, Koch B, Kretschmann-Kandel E, et al. Correlation between BMI, leisure habits and motor abilities in childhood (CHILT-project) Int J Obes Relat Metab Disord. 2004;28(1):22–26. doi: 10.1038/sj.ijo.0802428. [DOI] [PubMed] [Google Scholar]
- 38.Burgi F, Meyer U, Granacher U, et al. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: a cross-sectional and longitudinal study (Ballabeina) Int J Obes (Lond) 2011;35(7):937–944. doi: 10.1038/ijo.2011.54. [DOI] [PubMed] [Google Scholar]
- 39.Williams GN, Buchanan TS, Barrance PJ, Axe MJ, Snyder-Mackler L. Quadriceps weakness, atrophy, and activation failure in predicted noncopers after anterior cruciate ligament injury. Am J Sports Med. 2005;33(3):402–407. doi: 10.1177/0363546504268042. [DOI] [PubMed] [Google Scholar]
- 40.Lepley LK, Wojtys EM, Palmieri-Smith RM. Combination of eccentric exercise and neuromuscular electrical stimulation to improve quadriceps function post-ACL reconstruction. Knee. 2015;22(3):270–277. doi: 10.1016/j.knee.2014.11.013. [DOI] [PMC free article] [PubMed] [Google Scholar]