

Abstract
Binge eating and purging behaviors are associated with significant harm and distress among adolescents. The process by which these behaviors develop (often in the high school years) is not fully understood. We tested the Acquired Preparedness (AP) model of risk involving transactions among biological, personality, and psychosocial factors to predict binge eating and purging behavior in a sample of 1,906 children assessed in the spring of 5th grade (the last year of elementary school), the fall of 6th grade (the first year of middle school), spring of 6th grade, and spring of 10th grade (second year of high school). Pubertal onset in spring of 5th grade predicted increases in negative urgency, but not negative affect, in the fall of 6th grade. Negative urgency in the fall of 6th grade predicted increases in expectancies for reinforcement from eating in the spring of 6th grade, which in turn predicted increases in binge eating behavior in the spring of 10th grade. Negative affect in the fall of 6th grade predicted increases in thinness expectancies in the spring of 6th grade, which in turn predicted increases in purging in the spring of 10th grade. Results demonstrate similarities and differences in the development of these two different bulimic behaviors. Intervention efforts targeting the risk factors evident in this model may prove fruitful in the treatment of eating disorders characterized by binge eating and purging.
Keywords: eating and feeding disorders, adolescents, developmental perspectives
Introduction
Eating disorder symptoms often develop during adolescence (Abebe, Lien, & von Soest, 2012; Culbert, Burt, McGue, Iacono, & Klump, 2009; Davis, Ortiz, Smith, in press), and symptoms can be predicted by childhood characteristics such as personality (Pearson, Combs, Zapolski, & Smith, 2012) and biological factors such as puberty (Klump, McGue, & Iacono, 2003). Adolescent eating disorder symptoms are predictive of long-term symptom engagement (Neumark-Sztainer, Wall, Larson, Eisenberg, & Loth, 2011) and diagnosable, clinical eating disorders in adulthood (Kotler, Cohen, Davies, Pine & Walsh, 2001), emphasizing the importance in understanding their development. This paper describes the results of a study testing a model of how biological, personality, and learning factors transact during elementary and middle school to confer risk for binge eating and purging during high school. We begin by describing each individual component of our integrative model. We then present our hypothesized model and the empirical literature supporting it.
Pubertal Onset as a Risk Factor for Bulimic Behaviors
Puberty is marked by dramatic changes across life domains, but particularly in psychological health (Mendle, 2014). The biological event of pubertal onset is widely acknowledged as a risk factor for eating disorders. Research indicates that heritability of bulimic behaviors is negligible prior to pubertal onset in girls and then rises significantly at the onset of puberty (Klump et al., 2003). Early pubertal onset in particular has been shown to be a risk factor for engagement in binge eating and purging concurrently (Combs, Pearson, & Smith, 2011; Day et al., 2011) and engagement in binge eating prospectively (Pearson et al., 2012). Because risk for disordered eating behaviors increases substantially with pubertal onset, we include puberty in our risk model.
Although the mechanisms for the relationship between pubertal onset and eating disorder behavior are unclear, pubertal onset seems to influence other individual characteristics that are important in considering risk factors for eating disorders. In particular, pubertal onset is associated with elevated negative affect and emotional volatility (Allen & Matthews, 1997; Spear, 2000) and predicts increases in rash, impulsive action taken while in highly emotional states (Luna & Sweeney, 2004; Steinberg, 2004). Racine et al. (2013) found evidence indicating that the heritability of bulimic behavior post-puberty may be expressed through two personality risk factors for eating disorders: negative affect and negative urgency (the tendency to act rashly when distressed). We thus emphasize transactions between pubertal status and these two risk factors.
Personality Underpinnings of Bulimic Behaviors: Negative Urgency and Negative Affect
For both theoretical and empirical reasons, our model emphasizes the impulsigenic trait of negative urgency, the disposition to act rashly when highly distressed. Theory identifies engagement in bulimic behaviors, particularly binge eating, as providing the negative reinforcement function of escape from, or avoidance of, subjective distress (Pearson, Wonderlich, & Smith, 2015a). Empirically, negative mood precedes binge eating episodes in women with bulimia nervosa (BN) and declines in the hours following such episodes (Smyth et al., 2007, but see Haedt-Matt & Keel, 2011). Negative urgency is understood to lead to behaviors that provide such negative reinforcement, and empirically it does for multiple behaviors, including binge eating (Fischer, Peterson, & McCarthy, 2013; Pearson et al., 2012), drinking, smoking, non-suicidal self-injury, and gambling (Smith & Cyders, 2016); there is some evidence it also predicts purging among college women (Fischer et al., 2013). A meta-analysis of impulsigenic traits found negative urgency to have moderate to high effect size associations with binge eating, while other impulsigenic traits had small or negligible effects (Fischer, Smith, & Cyders, 2008).
Negative affect, or the feeling of emotional distress (Watson, Clark, & Tellegen, 1988), also predicts eating disorders among youth (Gardner, Stark, Friedman & Jackson, 2000; Leon, Fulkerson, Perry, Keel, & Klump, 1999; Stice, 2002; Stice, Burton, & Shaw, 2004; Stice, Ng, & Shaw, 2010). It predicts loss of control binge eating (Tanofsky-Kraff et al., 2011) above and beyond prediction from negative urgency (Pearson, Zapolski, & Smith, 2015b). It also predicts purging behavior (Stice, Killen, Hayward, & Taylor, 1998). It thus appears important to model both negative urgency and negative affect risk pathways.
Psychosocial Learning and Bulimic Behaviors: Expectancies
One way to understand learning with regard to risky or maladaptive behavior is to consider expectancies for reinforcement from engaging in such behaviors. Expectancies are thought to represent summaries of one’s learning history about the outcomes of one’s behavioral choices (Bolles, 1972; Tolman, 1932). They are formed based on the various direct and indirect learning events that individuals experience throughout their lifetime. Learned expectancies are thought to influence one’s future behavioral choices. One tends to choose behaviors for which one expects rewards or reinforcement, and to avoid behaviors for which one anticipates punishment. Considerable support for this model, and for the explicit measurement of expectancies as markers of learned associations, has accrued over several decades with respect to multiple behaviors (Bolles, 1972; Goldman, Brown, Christiansen, & Smith, 1991; Goldman, Darkes, & Del Boca, 1999; Hohlstein, Smith, & Atlas, 1998; Tolman, 1932).
Expectancy theory can be applied to eating disorders: Due to variance in exposure to different learning experiences about thinness and eating, individuals form different thinness and eating expectancies (Hohlstein et al., 1998). Endorsement of the expectancy that eating helps manage negative affect can be understood to reflect a summary of learning experiences relating eating to negative reinforcement that contributes to emotional eating, and hence to loss of control eating. Endorsement of the expectancy that thinness leads to overgeneralized life improvement reflects a summary of learning experiences relating thinness to a wide range of reinforcers, and thus contributes to internalization of the thin ideal as well as body dissatisfaction that so frequently results from comparisons of the self to the ideal (Pearson et al., 2015a). Longitudinal research has shown that both thinness and eating expectancies predict future engagement in binge eating (Smith, Simmons, Flory, Annus, & Hill, 2007) and that thinness expectancies predict future engagement in purging (Fischer et al., 2013; Smith et al., 2007).
The Acquired Preparedness (AP) Model of Risk: Integrating Personality and Psychosocial Learning
The AP model provides an integration of personality and psychosocial learning risk processes (Davis, Ortiz, D’Agostino, & Smith, 2016; Pearson et al., 2015a). The basic science literature on person-environment transaction theory (Caspi, 1993) posits that individuals with different personality traits respond differently to the same environmental event. The AP model broadens the scope of this idea to propose that because individuals can respond differently to the same learning event, they can also learn different things from the same event. One’s learning, in turn, influences one’s behavior. Thus, one’s personality helps shape one’s learning experiences and predicts one’s behavior. When individuals are differentially prepared to acquire high-risk expectancies as a function of high-risk personality traits, dysfunction results (Davis et al., 2016; Smith, Williams, Cyders, & Kelley, 2006). We next describe this process in relation to disordered eating.
The eating disorders AP model holds that elevations in negative urgency increase the likelihood of learning that eating serves the negative reinforcement function of distress relief, and this learned expectancy potentiates binge eating (Davis et al., 2016; Pearson et al., 2015a). This model has received empirical support over a 12-month longitudinal window (Pearson et al., 2012). Specifically, Pearson and colleagues (2012) found that 5th grade negative urgency predicted increases in the expectancy that eating helps one manage negative affect six months later, and the expectancy in turn predicted the onset of, or increases in, binge eating behavior another six months after that. Similar models with other addictive behaviors have also been validated empirically. Negative urgency predicts subsequent increases in expectancies for reinforcement from smoking, which in turn predict smoking behavior (Doran et al., 2013); and negative urgency predicts subsequent increases in expectancies for reinforcement from drinking, which predicts drinking behavior (Settles, Cyders, & Smith, 2010).
We note two features of the eating disorder AP model. First, the prospective sequence from negative urgency through learned expectancy to binge eating behavior is understood to reflect a mediational process, such that part of the hypothesized mechanism by which negative urgency is thought to influence binge eating is through its influence on psychosocial learning. Statistical tests of mediation using longitudinal data can provide evidence consistent with this theoretical contention, although they of course cannot demonstrate a causal process. Second, the model proposes a reciprocal process (Davis et al., 2016). Because expectancies for reinforcement from eating are understood to reflect summaries of one’s learning history, engagement in eating disorder behaviors should predict subsequent changes in expectancies. Thus, expectancy endorsement should be predicted by both negative urgency and prior engagement in disordered eating behaviors.
The Current Study
We conducted a test of an extended version of the AP model. We extended this model in four ways. First, because negative affect predicts adolescent binge eating beyond prediction from negative urgency (Pearson et al, 2015b) and also predicts purging behavior (Stice et al., 1998), we studied the role of negative affect as a predictor of psychosocial learning, binge eating, and purging. Second, we hypothesized a risk pathway to predict purging behavior. This risk pathway is from negative affect through thinness expectancies to purging behavior. Third, we added pubertal onset as a predictor of increases in negative affect and negative urgency to the model. As noted above, pubertal onset is associated with elevated negative affect, emotional volatility, and rash, impulsive behavior when emotional. In addition, the post-pubertal heritability of bulimic behavior may be expressed through negative affect and negative urgency (Racine et al., 2013). Fourth, we conducted the first test of whether the AP risk process predicts disordered eating behavior over the extended period of time from elementary school to mid-high school, with prediction from expectancy to behavior spanning a 4-year time lag. The specifics of our model tests follow.
With respect to binge eating, we hypothesized that pubertal onset by the spring of 5th grade (elementary school) would predict increases in trait negative urgency by the fall of 6th grade (beginning middle school). Negative urgency would, in turn, predict increases in the expectancy that eating helps manage negative affect by the spring of 6th grade (middle school). Those expectancies would predict increases in binge eating behavior four years later, in the spring of 10th grade (second year of high school).
With respect to purging, we hypothesized that pubertal onset by spring of 5th grade would predict increases in trait negative affect by the fall of 6th grade. Negative affectivity would, in turn, predict increases in the expectancy that thinness leads to overgeneralized life improvement by the spring of 6th grade. Our reasoning was that individuals who are distressed may be more sensitive to societal messages for the benefits of thinness, and thus more likely to acquire such expectancies (Ricciardelli & McCabe, 2001). Those expectancies would predict increases in purging behavior four years later, in the spring of 10th grade (second year of high school). Hypothesizing an association between negative affect and purging is consistent with past research (Stice et al., 1998). In addition, we hypothesized that spring, 6th grade endorsement of expectancies for reinforcement from thinness would also predict increases in binge eating behavior in the spring of 10th grade. They have been shown to do so before (Smith et al., 2007) and models of BN risk emphasize efforts to restrict food intake to pursue the thin ideal as precursors to binge episodes (Goldschmidt, Aspen, Sinton, Tanofsky-Kraff, & Wilfley, 2008; Polivy & Herman, 1985).
As described below, we tested additional prospective relationships. The AP process is thought to be ongoing and reciprocal, such that binge eating predicts further increases in expectancies that eating helps manage negative mood. We tested for the presence of such pathways. We conducted these tests on a sample of 1,906 children who were assessed repeatedly over the course of adolescence. The current investigation was made possible by a continuation of the longitudinal study from 6th through 10th grade, and initial findings for these participants over a shorter initial time interval (e.g., 5th to 6th grade) have been reported previously (e.g., Pearson et al., 2012, 2015b).
Method
Participants
Data for this study were part of a larger study assessing the development of dysfunctional behaviors during the preadolescent to early adolescent years. A sample of 1906 children participated over nine waves: every six months from the spring of 5th grade (the last year of elementary school) through the spring of 8th grade (the last year of middle school) and then in the spring of 9th and 10th grades. The final wave of data collection took place in 2014. The mean age of the participants at the initiation of the study was 10.86 years, and the sample was made up of 968 (50.8%) boys and 938 (49.2%) girls. Most were European–American (60.9%), followed by African–American (18.7%); the remainder of the sample identified themselves as Hispanic (8.2%), Asian (2.9%), Middle Eastern (0.4%), or other (8.8%). African– American and Hispanic children were oversampled; hence, these groups are represented at higher rates than is characteristic of the local population.
Measures
Demographic and background questionnaire
Participants were asked to indicate their gender, current age (in years), and which label(s) best described their ethnic background.
Eating Disorder Examination- Questionnaire (EDE-Q; Fairburn & Beglin, 1994)
The EDE-Q is a self-report version of the Eating Disorders Examination semi-structured interview (Cooper & Fairburn, 1993) designed to assess the full range of behavioral and cognitive or attitudinal features of the specific psychopathology of eating disorders during the preceding four weeks. The EDE-Q has been shown to have good reliability and validity (Cooper & Fairburn, 1993; Luce & Crowther, 1999; Mond, Hay, Rodgers, Owen, & Beumont, 2004).
In this study, the EDE-Q was adapted for use with a younger population by using age-appropriate wording, defining concepts that could possibly be difficult to understand, and shortening the length of time referred to in the questions to the past two weeks, per past recommendations (Carter, Stewart, & Fairburn, 2001) and as done in Pearson et al. (2012). We defined binge eating as objective binge eating with loss of control (see Tanofsky-Kraff et al., 2011). To be scored positively for binge eating, youth had to endorse two items positively, one that assessed episodes of objective binge eating and one that assessed loss of control during these episodes. Purging status was determined by the participants’ response to a question asking if they had made themselves sick (vomit) in the past two weeks as a means of controlling their shape or weight. Participants indicated their engagement in binge eating and purging dichotomously (yes or no) and on an ordinal scale for Wave 4 (1 = 1-2 days, 2 = 3-4 days, 3 = 5-7 days, 4 = 8-10 days, 5 = 11-13 days, g = 14 days or every day). Due to lower base rates in binge eating and purging in 5th and 6th grade, the dichotomous response was used for Waves 2 and 3, and the ordinal response was used for Wave 4.
UPPS-P-Child Version (Zapolski, Stairs, Settles, Combs, & Smith, 2010)
The UPPS-P-Child Version was used to measure negative urgency. UPPS-P measures five impulsigenic traits, including negative urgency. The negative urgency scale consists of eight items and responses are on a 4-point Likert-type scale from 1 (not at all like me) to 4 (very much like me). A sample item is: “When I am upset I often act without thinking.” Internal consistency estimates of reliability were high: α = .91 at Wave 1 and higher subsequent waves. Scores were calculated as average item scores, so the range was from 1 to 4. Negative urgency scores correlate highly across method of assessment and very modestly with other impulsigenic traits (Cyders & Smith, 2007) and, as predicted by theory and noted above, negative urgency scores predict a range of maladaptive behaviors thought to provide negative reinforcement (Smith & Cyders, 2016).
Positive and Negative Affect Schedule- Child Version (PANAS-C; Laurent et al., 1999)
The PANAS was used to measure negative affectivity in children. It was based on the adult PANAS (Watson et al., 1988) and developed and validated for children in grades 4-8. Items were adapted to ask how one “generally” feels rather than how one feels “over the past few weeks.” There is impressive evidence for both scales’ reliability and validity (Laurent et al., 1999). Internal consistency estimate of reliability was α = .90 at wave 1 and slightly higher at subsequent waves.
The Pubertal Development Scale (PDS; Petersen, Crockett, Richards, & Boxer, 1988)
This scale consists of five questions for boys (“Do you have facial hair yet?”) and five questions for girls (“Have you begun to have your period?”). Evidence for reliability and validity are strong (Coleman & Coleman, 2002). We used the common dichotomous classification of the PDS (Culbert et al., 2009; Pearson et al., 2012) as prepubertal or pubertal, with mean scores above 2.5 indicative of pubertal onset.
Eating Expectancy Inventory (EEI; Hohlstein et al., 1998)
This five-factor measure reflects expectancies for reinforcement from eating. For this study, we used the measure of the expectancy that eating helps one manage negative mood states. As with past samples, the scale was internally consistent (Wave 1 α = .93 and higher in subsequent waves). An example item is “Eating helps me forget bad feelings, like being sad, lonely, or scared.” In multiple longitudinal samples, the scale predicts subsequent increases in binge eating behavior (Davis et al., 2016).
Thinness and Restricting Expectancy Inventory (TREI: Hohlstein et al., 1998)
The TREI measures overgeneralized expectancies for life improvement from thinness and restricting food intake. Scores on the scale were internally consistent in this sample, as they have been in the past (Wave 1 α = .91 and higher in subsequent waves). An example item is, “If I were thin, I would feel more worthwhile.” Comparisons of multiple possible factor structures indicate the scale is unidimensional (Hohlstein et al., 1998). The scale predicts subsequent increases in both purging and binge eating behavior (Smith et al., 2007). An experimental manipulation to reduce thinness expectancies in high school and college women produced reductions in cognitive eating disorder symptoms (Annus, Smith, & Masters, 2008).
Procedure
Data collection
The following procedure was approved by the University of Kentucky’s Institutional Review Board (06-0900-F4S) and by the participating school systems and was utilized at all nine waves of the parent study and all four waves of the current study. The questionnaires were administered in school cafeterias or classrooms during school hours (23 public elementary schools for Wave 1, spring of 5th grade; 19 public middle schools for Waves 2 and 3, fall of 6th grade and spring of 6th grade; and seven public high schools and two private high schools for Wave 4, spring of 10th grade). A passive consent procedure was used. Each family was sent a letter, through the U.S. Mail, introducing the study. Families were asked to return an enclosed, stamped letter or call a phone number if they did not want their child to participate. Of 1,988 fifth grade students in the participating schools, 1,906 (95.8%) participated. Reasons for not participating included family or youth declination of consent, and other reasons such as language disabilities that precluded completing the measures.
It was made clear to the students that their responses on the questionnaires were to be kept confidential and no one outside of the research team would see them. The research team introduced a federal certificate of confidentiality for the project and emphasized that the team was legally bound to keep all responses confidential. After each participant signed the assent form, the researchers then passed out packets of questionnaires. The questionnaire administration took 60 minutes or less. There was no compensation for participation (except for those who moved out of district). Those who did move out of the study’s school districts were contacted and asked to complete the forms by mail and were paid $30 for doing so in 6th grade and $40 for doing so in 10th grade.
Data analysis
Structural equation modeling (SEM) was used to test the predictive model; the software we used was Mplus (Muthén & Muthén, 2004–2010). We modeled binge eating and purging at Waves 2 and 3 as dichotomous (presence or absence, due to low rates of the behaviors) and as ordered categorical variables at Wave 4. We allowed cross-sectional associations between all variables or disturbance terms. We used a weighted least squares estimation procedure (WLSMV), given the ordered categorical variables. We present effect sizes as odds ratios in the prediction of those outcomes. We tested mediation by using a bias-corrected bootstrapping method that increases statistical power and does not impose the assumption of normality on the data. The procedure generated 1,000 bootstrapped samples to empirically approximate the true sampling distribution because the assumption of a normal sampling distribution is not likely to be accurate. This procedure is available in MPlus (Muthén & Muthén, 2004–2010).
Figure 1 presents the model. It allowed for the following: (1) Cross-sectional associations among all variables or disturbance terms (not depicted). (2) Autoregressive paths from each variable at each wave to itself at the following wave. (3) Predictive effects representing hypotheses regarding the AP model. For negative urgency, the paths were from (a) pubertal onset at Wave 1 (5th grade spring) to negative urgency at Wave 2 (fall, 6th grade); (b) negative urgency at Wave 2 to eating expectancies at Wave 3 (spring, 6th grade); and (c) eating expectancies at Wave 3 to binge eating at Wave 4 (spring, 10th grade). For negative affect, the paths were from (a) pubertal onset at Wave 1 to negative affect at Wave 2; negative affect at Wave 2 to thinness expectancies at Wave 3; and from thinness expectancies at Wave 3 to purging and binge eating at Wave 4. (4) Predictive effects representing the hypothesized, reciprocal nature of the AP model, i.e., from (a) binge eating at Wave 2 to eating and thinness expectancies at Wave 3; (b) purging at Wave 2 to thinness expectancies at Wave 3; and the same associations from Wave 3 to Wave 4. (5) Predictive effects representing the possibility that binge eating behavior predicts subsequent increases in purging behavior; (6) Additional prediction of personality traits to expectancies, and from expectancies to behaviors, beyond those specified above. These additional paths included negative urgency at Wave 2 predicting thinness expectancies at Wave 3, negative affect at Wave 2 predicting eating expectancies at Wave 3, eating expectancies at Wave 3 predicting purging at Wave 4. The online supplement includes confidence intervals for all prospective effects (Table S1) and a figure that includes both significant and non-significant pathways (Figure S1).
Figure 1.
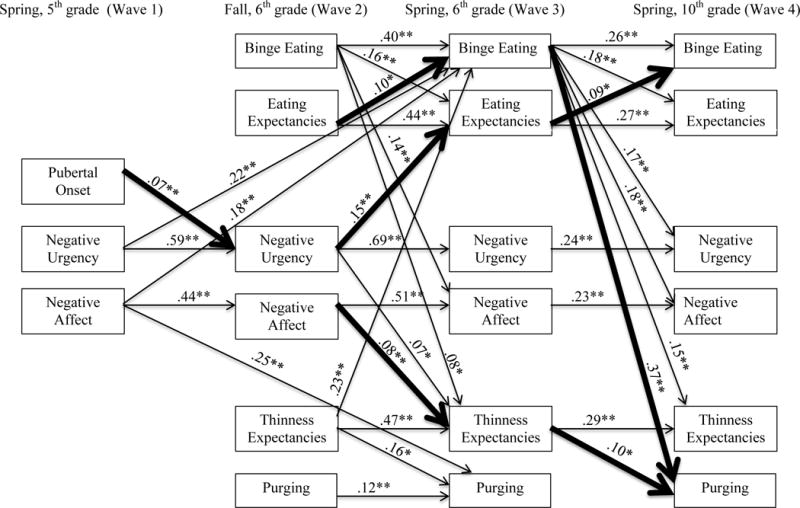
n = 1,906; * p < .01 **p < .001. Coefficients are standardized. For clarity of presentation, all cross-sectional associations, though modeled, are excluded from the Figure. Bolded paths represent the meditational pathways that were tested and found to be significant.
We next tested whether the model was invariant across gender (the AP model tested by Pearson et al. (2012) was invariant across gender). To do so, we compared two models. The first specified the same model for both genders with no additional constraints. The second added the constraint that all prospective paths be equal across gender. If there is no loss in model fit when adding these constraints, there is no basis for inferring that prospective prediction among the variables differs by gender. One analytic change was necessary for the invariance tests. Because one gender (female) had no members of one of the categories of purging behavior, invariance testing could not proceed with categorical variables. Accordingly, for the invariance testing we modeled binge eating and purging as interval scale variables. We note that all model results using an interval scale representation of binge eating and purging were the same as those using an ordered categorical representation of those variables.
For bivariate correlations, we used p < .001 to determine statistical significance. The SEM model involved tests of the net effects of each prediction, over and above the effects of other variables and over extended periods of time. We therefore included pathways significant at p < .01, if the corresponding bivariate correlation was significant at p < .001.
We measured SEM model fit using both an absolute fit index, the root mean square error of approximation (RMSEA) and a relative fit index, the comparative fit index (CFI) and, for gender invariance testing, the Standardized Root Mean Square Residual (SRMR) (Hu & Bentler, 1999). We also report the model chi-square.
Results
Attrition and Treatment of Missing Data
Retention from one wave to the next ranged from 94.2% to 98.3%. Of the full sample of 1906 youth, the percentage of participants ranged from 1843 at Wave 1 (96.7%: 63 youth with consent did not participate at wave 1 due to absence from school on each testing day) to 1416 (74.3%) at Wave 4. At each wave, participating and non-participating participants did not differ on any study variables, so we treated the data as missing at random. The WLSMV estimation method in Mplus includes a four-step approach to handling missing data, the first two of which involve maximum likelihood methods and the last two of which involve a pairwise deletion procedure.1
Possible Effects due to School Membership
In order to determine whether there was significant covariance among the study variables due to participants attending the same school, intraclass coefficients were calculated for each variable (using elementary school membership, n = 23, as the nesting variable). Intraclass coefficients were all .00; therefore, we concluded that school membership was essentially unrelated to study variables.
Descriptive Statistics
The sample of 1906 children includes 938 girls and 968 boys. By the spring of 5th grade, 27.7% of the girls and 21.8% of the boys had experienced pubertal onset. Table 1 presents the means and standard deviations for negative urgency, negative affect, eating expectancies, and thinness expectancies at each wave for both boys and girls and Table 2 presents the presence or frequencies of binge eating and purging behavior by gender over the two weeks preceding the assessments. At each wave, over 9.9% of girls and 8.5% of boys reported at least some objective binge eating over the preceding two weeks. At each wave, over 2.4% of girls and 3.0% of boys endorsed purging over the preceding two weeks.
Table 1.
Descriptive Statistics of all study variables
| Factor and Wave | Female Mean (SD) |
Male Mean (SD) |
|---|---|---|
| NU-1 | 2.20 (.69) | 2.21 (.74) |
| NA-1 | 2.10 (.76) | 2.12 (.80) |
| NU-2 | 2.11 (.70) | 2.10 (.71) |
| NA-2 | 1.82 (.75) | 1.83 (.75) |
| EE-2 | 1.91 (1.27) | 1.92 (1.30) |
| TE-2 | 2.66 (1.70) | 2.57 (1.63) |
| NU-3 | 2.15 (.73) | 2.14 (.73) |
| NA-3 | 1.74 (.70) | 1.75 (.73) |
| EE-3 | 1.86 (1.22) | 1.86 (1.29) |
| TE-3 | 2.62 (1.75) | 2.56 (1.69) |
| NU-4 | 2.27 (.69) | 2.26 (.69) |
| NA-4 | 1.83 (.76) | 1.88 (.79) |
| EE-4 | 2.23 (1.37) | 2.22 (1.36) |
| TE-4 | 2.70 (1.72) | 2.65 (1.71) |
Note. Means based on available data at each wave (e.g., n = 1843 at Wave 1 and n = 1417 at Wave 4). Total sample n = 1906.
NU = Negative Urgency; NA = Negative Affect; EE = Eating Expectancies (EE); and TE = Thinness Expectancies (TE); each number following the variable represents the wave in which the data was collected. (i.e., NU-1 = Negative Urgency, Wave 1)
Table 2.
Descriptive Statistics for Binge Eating and Purging Behavior
| Presence of behavior | ||||
|---|---|---|---|---|
| Female | Male | |||
|
| ||||
| Yes | No | Yes | No | |
| Binge Eating Wave 2 | 83 | 818 | 88 | 837 |
| Purging Wave 2 | 31 | 870 | 33 | 892 |
| Binge Eating Wave 3 | 79 | 802 | 71 | 836 |
| Purging Wave 3 | 21 | 860 | 26 | 881 |
| Frequency of behavior at Wave 4 | ||
|---|---|---|
|
| ||
| Number of binge eating episodes in past 14 days | Female | Male |
| None | 606 | 630 |
| 1 – 2 | 57 | 59 |
| 3 – 4 | 15 | 14 |
| 5 – 7 | 1 | 9 |
| 8 – 10 | 4 | 1 |
| 11 – 13 | 3 | 0 |
| 14 days or everyday | 11 | 7 |
|
| ||
| Number of purging episodes in past 14 days | Female | Male |
|
| ||
| None | 658 | 688 |
| 1 – 2 | 23 | 18 |
| 3 – 4 | 9 | 5 |
| 5 – 7 | 2 | 2 |
| 8 – 10 | 0 | 0 |
| 11 – 13 | 0 | 0 |
| 14 days or everyday | 5 | 7 |
Note. Means based on available data at each wave (e.g., n = 1843 at Wave 1 and n = 1417 at Wave 4). Total sample n = 1906. At Waves 2 and 3, binge and purge were measured dichotomously. At Wave 4, they were measured as ordered categorical variables.
Correlations among Pubertal Status, Negative Urgency, Negative Affect, Eating Expectancies, Thinness Expectancies, Binge Eating, and Purging Across all Three Waves
Table 3 presents correlations among all study variables. As the table shows, binge eating and purging were positively correlated. As expected, eating and thinness expectancies were each positively correlated with bulimic behaviors. Eating and thinness expectancies were also positively correlated with each other at each wave, as were negative urgency and negative affect. Negative urgency and negative affect were positively correlated with bulimic behaviors and eating and thinness expectancies at each wave as well.
Table 3.
Correlations among study variables at each wave
| Pub-1 | NU-1 | NA-1 | B-2 | P-2 | NU-2 | NA-2 | EE-2 | TE-2 | B-3 | P-3 | NU-3 | NA-3 | EE-3 | TE-3 | B-4 | P-4 | NU-4 | NA-4 | EE-4 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NU-1 | .12* | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| NA-1 | .03 | .37* | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| B-2 | .06 | .10* | .14* | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| P-2 | .08 | .07 | .13* | .20* | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| NU-2 | .12* | .54* | .27* | .15* | .09* | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| NA-2 | .03 | .22* | .41* | .14* | .13* | .32* | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| EE-2 | .04 | .19* | .21* | .35* | .16* | .29* | .32* | – | – | – | – | – | – | – | – | – | – | – | – | – |
| TE-2 | .04 | .15* | .17* | .16* | .12* | .23* | .29* | .42* | – | – | – | – | – | – | – | – | – | – | – | – |
| B-3 | .04 | .15* | .13* | .34* | .09* | .14* | .16* | .24* | .16* | – | – | – | – | – | – | – | – | – | – | – |
| P-3 | .05 | .03 | .12* | .06 | .18* | .05 | .12* | .12* | .10* | .10* | – | – | – | – | – | – | – | – | – | – |
| NU-3 | .10* | .50* | .24* | .13* | .07 | .62* | .23* | .20* | .19* | .16* | .07 | – | – | – | – | – | – | – | – | – |
| NA-3 | .06 | .20* | .33* | .13* | .10* | .25* | .49* | .20* | .19* | .19* | .09* | .33* | – | – | – | – | – | – | – | – |
| EE-3 | .07 | .20* | .16* | .25* | .11* | .26* | .21* | .54* | .24* | .31* | .13* | .29* | .26* | – | – | – | – | – | – | – |
| TE-3 | .08* | .16* | .16* | .16* | .10* | .19* | .22* | .26* | .52* | .21* | .14* | .24* | .26* | .43* | – | – | – | – | – | – |
| B-4 | .01 | .08 | .06 | .07 | .02 | .12* | .06 | .08* | .05 | .08* | −.02 | .10* | .12* | .10* | .07 | – | – | – | – | – |
| P-4 | −.00 | .06 | −.02 | .06 | .02 | .05 | −.01 | .01 | .05 | .11* | .05 | .07 | .03 | .09* | .05 | .41* | – | – | – | – |
| NU-4 | .05 | .28* | .12* | .08 | .03 | .31* | .10* | .12* | .14* | .13* | .05 | .38* | .16* | .16* | .17* | .18* | .13* | – | – | – |
| NA-4 | .01 | .14* | .19* | .06 | .05 | .19* | .23* | .07 | .15* | .15* | .02 | .21* | .31* | .12* | .19* | .29* | .16* | .43* | – | – |
| EE-4 | .00 | .11* | .07 | .10* | .04 | .11* | .10* | .22* | .15* | .16* | .08 | .14* | .21* | .31* | .15* | .37* | .18* | .33* | .38* | – |
| TE-4 | −.01 | .08* | .11* | .07 | .05 | .08 | .12* | .13* | .30* | .15* | .07 | .12* | .23* | .22* | .32* | .27* | .13* | .28* | .35* | .59* |
Note. Correlations based on available data at each wave. Total sample n = 1906. Pub = Puberty; B = Binge eating; P = Purging; NU = Negative Urgency; NA = Negative Affect; EE = Eating Expectancies; and TE = Thinness Expectancies; each number following the variable represents the wave in which the data was collected. (i.e., NU-1 = Negative Urgency, Wave 1). Correlations with puberty, binge eating (Waves 2 and 3) and purging (Waves 2 and 3) are point-biserial correlations.
p < .001.
Model Test
We next summarize the results of the model test. The RMSEA value indicated good model fit (RMSEA = .04, 90% confidence interval .04 - .05), CFI = .91, and χ2 (118) = 618.77, p < .001. Beta weights for prospective effects are provided in Figure 1. As shown in the figure, all autoregressive pathways were significantly greater than zero and of at least moderate magnitude, indicating stability in personality (negative urgency, negative affect), expectancies (eating, thinness), and behavior (binge eating, purging) over time, as expected.
Tests of Extended AP Model
Negative urgency
As hypothesized, spring of 5th grade puberty predicted increases in fall of 6th grade negative urgency, controlling for 5th grade negative urgency, and fall of 6th grade negative urgency predicted increases in spring, 6th grade eating expectancies, controlling for fall, 6th grade eating expectancies. The expectancies, in turn, predicted spring, 10th grade binge eating, controlling for spring, 6th grade binge eating. Statistical tests of mediation found evidence supporting two, sequential mediational processes: (1) spring, 5th grade puberty’s prediction of spring, 6th grade eating expectancies appears to have been mediated by fall, 6th grade negative urgency (b = .01, z = 2.89, p < .01), and (2) fall, 6th grade negative urgency’s prediction of 10th grade binge eating appears to have been mediated by spring, 6th grade eating expectancies (b = .01, z = 2.17, p < .02). To give an indication of the magnitude of this mediation effect, the odds ratio for predicting a one unit increase in 10th grade binge eating from a one unit increase in fall, 6th grade negative urgency dropped from a direct effect of 1.64 to 1.47 when the mediator was included in the model.
Negative affect
Counter to our hypothesis, spring, 5th grade puberty did not predict increases in fall, 6th grade negative affect. Consistent with our hypotheses, fall, 6th grade negative affect predicted spring, 6th grade thinness expectancies, controlling for fall, 6th grade thinness expectancies, and spring, 6th grade thinness expectancies predicted spring, 10th grade purging behavior, controlling for spring, 6th grade purging behavior. Statistical tests of mediation found evidence supporting this AP process: fall, 6th grade negative affect’s prediction of spring, 10th grade purging appears to have been mediated by spring, 6th grade thinness expectancies (b = .01, z = 1.69, p < .05). The odds ratio for predicting a one unit increase in 10th grade purging from fall, 6th grade negative affect dropped from a direct effect of 1.30 to 1.15 when the mediator was included in the model. Counter to hypothesis, spring, 6th grade thinness expectancies did not predict spring, 10th grade binge eating behavior, controlling for spring, 6th grade binge eating behavior.
Additional Pathways Tested
The ongoing, reciprocal nature of the AP process
As hypothesized, fall, 6th grade binge eating predicted spring, 6th grade eating expectancies, controlling for fall, 6th grade eating expectancies, and spring, 6th grade binge eating predicted spring, 10th grade eating expectancies, controlling for spring, 6th grade eating expectancies. The experience of binge eating results in heightened endorsement of the expectancy that eating helps alleviate negative affect. Fall, 6th grade binge eating also predicted spring, 6th grade thinness expectancies, controlling for fall, 6th grade thinness expectancies, and spring, 6th grade binge eating predicted spring, 10th grade thinness expectancies, controlling for spring, 6th grade thinness expectancies. It thus appears that the experience of binge eating also results in heightened endorsement of expectancies for reinforcement from thinness. By contrast, purging did not predict subsequent changes in either eating or thinness expectancies.
Binge eating as predictor of purging
Although not part of the AP model, it was important also to model binge eating as a predictor of subsequent increases in purging behavior. Fall, 6th grade binge eater status did not predict spring, 6th grade purger status. However, spring, 6th grade binge eater status did predict spring, 10th grade purging behavior. A test of mediation was consistent with the possibility that the influence of eating expectancies on purging behavior is through their influence on binge eating (b = .04, z = 2.34, p < .01).
Magnitude of Prediction from the Model
To provide an indication of the magnitude of the predictive effects presented in Figure 1, we calculated odds ratios for the prediction of (a) the dichotomous measures of binge eating and purging at Wave 3, spring of 6th grade and (b) the ordinal measures of binge eating and purging at Wave 4, spring of 10th grade. We present those values in Table 4. Not surprisingly, prediction of binge eating and purging behavior from the same behavior six months earlier was very strong, such that membership in either the binge eating or purging group in fall of 6th grade increased the probability approximately 7-fold of being in that group in the spring of 6th grade. Prediction of 10th grade binge eating and purging from 6th grade engagement in those behaviors, though not as strong as prediction across six months, was noteworthy. Engagement in earlier binge eating increased the probability of a higher level of engagement in the same behavior four years later by 113%. Engagement in earlier binge eating increased the probably of a higher level of engagement in purging four years later by over 400%, and earlier purging further increased that probability by 14%. In addition, for each outcome variable, both eating and thinness expectancies increased prediction beyond prior engagement in the behavior. For example, the probability of being in the binge eating group in spring, 6th grade increased by 24% for each one-unit increase in eating expectancy and by 17% for each one-unit increase in thinness expectancy.
Table 4.
Binge eating and purging odds ratios
| Behavior | Predictor | Odds ratio |
|---|---|---|
| Wave 3 binge eating | Wave 1 negative urgency | 1.29 |
| Wave 1 negative affect | 1.19 | |
| Wave 2 binge | 6.68 | |
| Wave 2 eating expectancies | 1.24 | |
| Wave 2 thinness expectancies | 1.17 | |
| Wave 3 purging | Wave 1 negative affect | 1.98 |
| Wave 2 purging | 7.24 | |
| Wave 2 eating expectancies | 1.27 | |
| Wave 2 thinness expectancies | 1.18 | |
| Wave 4 binge eating | Wave 3 binge eating | 2.13 |
| Wave 3 eating expectancies | 1.15 | |
| Wave 4 purging | Wave 3 binge eating | 4.08 |
| Wave 3 thinness expectancies | 1.14 |
Note. Odds Ratios are based on available data at each wave (e.g., n = 1843 at Wave 1 and n = 1417 at Wave 4). Total sample n = 1906.
Model Invariance Across Gender
We next tested whether the structural model represented in Figure 1 was invariant across gender. The first step in doing so was to test the same theoretical model for both genders: CFI = .93; RMSEA = .05 (CI = .046-.054); SRMR = .07; χ2 (244) = 800.31, p < .001. We next tested a model in which each predictive path was constrained to be the same for boys and girls (53 paths). The increase in chi-square with the additional model constraints was non-significant and there was no meaningful decline in other fit indices: CFI = .92; RMSEA = .05 (CI = .044-.051); SRMR = .07; χ2 (289) = 883.51) p < .001. We thus concluded that the predictive model was invariant across gender.
Discussion
Stemming from the view that risk for the emergence of disordered eating behaviors is likely to involve transactions among multiple factors, we tested one model specifying transactions among three sets of variables: pubertal onset, personality, and psychosocial learning. Specifically, we tested a new extension of the AP model of eating disorder risk across a five-year longitudinal window spanning elementary school, through middle school, to high school. We found that high school binge eating and purging, which (a) is associated with the emergence of diagnosable eating disorders (Neumark-Sztainer et al., 2011) and (b) predicts dysfunction and eating disorder diagnosis in adulthood (Kotler et al., 2001), can itself be predicted by characteristics identifiable in elementary and middle school.
Support for AP Model of Risk
The findings of this study provide clear support for the extended AP model of eating disorder risk. We highlight four key findings from this research. First, as hypothesized, we found sequential longitudinal prediction from 5th grade pubertal status through trait negative urgency to elevated expectancies that eating helps one manage negative affect. Those expectancies, in turn, predicted increased binge eating behavior four years later; the predictive influence of negative urgency on later binge eating operated in part through increases in eating expectancies. In each case, statistical tests of mediation were consistent with the AP hypothesis of mediational processes. This sequence of effects was present when controlling for all autoregressive effects as well as the predictive roles of trait negative affect, expectancies for reinforcement from thinness, and binge eating behavior on subsequent purging.
The findings are consistent with the following theory. Perhaps the experience of puberty heightens adolescent tendencies to act rashly when distressed (Boyle, Riley, Crosby, & Smith, 2018; Racine et al., 2013), which in turn biases psychosocial learning to increase the likelihood of learning that eating serves a negative reinforcement function. Learning such an association increases risk for binge eating behavior (Davis et al., 2016; Pearson et al., 2015a). This process appears to operate over an extended, five-year period and across the multiple developmental transitions associated with progression from elementary school to high school.
Second, as hypothesized we found sequential, longitudinal prediction from 6th grade negative affect through expectancies for reinforcement from thinness to purging behavior four years later, again appearing to reflect a mediational process. These effects were also present when controlling for all autoregressive effects, the predictive roles of negative urgency and expectancies for reinforcement from eating, and prediction of purging behavior from prior binge eating.
Theory is not as well-developed to explain the association between negative affect and thinness expectancies. One possibility is that some of those experiencing heightened negative affect are disposed to seek behaviors that improve their lives by meeting societal standards for thinness, which can be perceived as providing many benefits, including meeting a core human need by enhancing social acceptance and connection (Cacioppo, Cacioppo, & Boomsma, 2014), as well as achieving heightened levels of self-confidence and respect from others. As a result, they may be biased to inculcate societal messages lauding thinness and thus more likely to learn expectancies that thinness leads to overgeneralized life improvement. Thinness expectancies have been shown to predict purging behavior in a separate longitudinal sample (Smith et al., 2007) and are elevated in women with anorexia nervosa and BN diagnoses (Hohlstein et al., 1998). Unlike negative urgency and counter to our hypothesis, negative affect was not predicted by pubertal onset.
Third, as hypothesized in the AP model, the transactional process has a reciprocal quality. The experience of binge eating is a behavior that can be expected to influence learned expectancies for reinforcement from eating. We found that it did so across both a 6-month period in the first year of middle school and a 4-year period from middle school into the second year of high school. Interestingly, the experience of binge eating did not provide a corrective effect; that is, expectancies that eating is reinforcing did not decline. Instead, expectancy endorsement rose. Binge eating led adolescents to endorse more strongly the expectancy that eating helps manage negative affect. This finding is consistent with the idea that binge eating does provide the negative reinforcement of distress reduction.
It was also the case that binge eating predicted subsequent increases in expectancies for reinforcement from thinness. This effect was not hypothesized and the reasons for this effect are not clear. One possibility is that those who engaged in binge eating and did not purge experienced weight gain and associated negative effects, such as loss of confidence or self-esteem (Paxton, Neumark-Sztainer, Hannan, & Eisenberg, 2006), that heighten the expectation that thinness can provide positive outcomes such as confidence. It seems best not to speculate on effects associated with those individuals who binged then purged, because we found no associations between purging behavior and subsequent change in thinness expectancies. Of course, the absence of such an effect may have occurred due to the low rates of purging behavior in the sample.
Fourth, the importance of understanding disordered eating in males as well as females lead to examination of gender differences in our model. As it turns out, the predictive effects were invariant across gender. We found no evidence that any of the predictive paths differed for boys and girls.
Implications of Findings
The finding that there are two different starting points and progression pathways for binge eating (involving negative urgency) and purging behavior (involving negative affect) is clinically relevant. An adolescent who is binge eating, but not purging, may benefit from intervention strategies recommended for negative urgency (Zapolski & Smith, 2017 for children and Weiss, Sullivan, & Tull, 2015 for adults), together with treatment of expectancies for reinforcement from eating, using methods similar to those used in enhanced cognitive behavioral therapy for eating disorders (CBT-E; Fairburn, Cooper, & Shafran, 2008). Perhaps adolescents who endorse only purging might be better treated with interventions targeting negative affect, along with CBT-E interventions focused on challenging thinness expectancies. Those engaging in both binge eating and purging may benefit from both forms of treatment. Intervention for eating disorders clearly cannot be a one-size-fits-all approach, and a greater understanding of the risk and maintenance factors evident in this research may help tailor treatment to target specific symptoms or sets of symptoms.
We return briefly to the finding that negative urgency is potentiated by pubertal onset. The impact of puberty on functioning is understood to include biological and socio-contextual components (Dick, Rose, Viken, & Kaprio, 2000; Ellis, 2004). With respect to eating disorders specifically, it is noteworthy that heritable effects of risk appear to emerge during puberty (Klump, Perkins, Burt, McGue, & Iacono, 2007) and that those heritable effects overlap with negative urgency and negative affect (Racine et al., 2013). It may be that pubertal onset’s prediction of increases in negative urgency reflects in part a biological influence on eating disorder risk. Surely the experience of puberty on disordered eating behavior operates through biological, social, and contextual processes as it does for other behaviors.
Relation to other Risk Models
Pearson et al. (2015a) provide an in-depth discussion of existing prospective models of bulimic behaviors and the roles of negative urgency, negative affect, and the AP model in that context. Briefly, the AP model builds on existing models, such as the dual pathway model (Stice, 2001), emotion regulation models (Agras & Telch, 1998), and restraint models (Polivy & Herman, 1985). It does so both by incorporating recent advances in basic personality science and by specifying mechanisms by which risk factors transact to increase risk. Concerning advances in basic science, recognition of the trait of negative urgency led to the identification of that trait as helping to explain not just distress, but the disposition to act rashly or impulsively when distressed. The trait accounts for substantial variance in bulimic behaviors and predicts their occurrence above and beyond negative affect (Fischer, Smith, & Cyders, 2008; Pearson et al., 2015b). Inclusion of the trait thus builds directly on emotion regulation and dual pathway models that seek to explain the pathway from distress to binge eating and purging (Agras & Telch, 1998; Stice, 2001). Concerning transactions among risk factors, the AP model recognition that traits help shape learning processes (Smith et al., 2006) provides a new integration of personality-based risk with learning-based risk, the latter of which is implicated in restraint models. That is, one factor that predicts forming expectancies for reinforcement from thinness and from eating, beyond environmental experience and societal pressure, is elevations in negative urgency and negative affect. The current study’s support for the AP model suggests the model may increase our understanding of the risk process.
Limitations
There are limitations to these findings. First, this study was a temporal demonstration of effects designed to be consistent with a causal model. Although the findings were consistent with our causal model, they are not a demonstration of the validity of causal processes. Second, retention was high and multiple methods of handling missing data produced the same results. However, we cannot know if the results of this study would have differed with even higher retention. Third, all risk and behavioral symptom data were self-reported by questionnaire. Although the measures used demonstrated good psychometric properties in this and previous studies of adolescents, face-to-face interviews provide the opportunity for clarification of terms, which may be particularly useful in a sample of youth. Fourth, it is important to recognize that most effect sizes were of small to moderate magnitude. We expected small and moderate effects, because of the lengthy longitudinal period across multiple developmental transitions, the use of tight controls, and the reality that we studied only three sets of risk factors among the many forces that heighten eating disorder risk. Ultimately, integration of the AP model with other risk mechanisms, such as genetic and hormonal processes (Klump, Keel, Sisk, & Burt, 2010), is necessary. It is also likely that negative urgency and negative affect-based AP processes apply to a subset, but not all, individuals with bulimic symptoms. Fifth, we represented purging behavior only with self-induced vomiting. We did so because the base rates of other forms of purging were extremely low. Sixth, although EDE-Q assessment of binge eating episodes correlates very highly with daily food records of binge eating, one study found higher binge episodes from the questionnaire than the daily food record (Berg, Peterson, Frazier, & Crow, 2011). Seventh, we assessed gender dichotomously and thus have no information as to the nature or presence of these effects among individuals with fluid or changing gender identities.
In sum, high school bulimic behavior can be predicted by elementary and middle school risk factors. Our integrated model of risk specified transactions among pubertal onset, negative urgency, negative affect, high-risk psychosocial expectancies for reinforcement from eating and thinness, and binge eating and purging behavior to explain the longitudinal risk process over a five-year period in early adolescence dense with developmental transitions. The current findings may prove useful to prevention scientists and we hope they stimulate new, improved risk models.
The problem behaviors of binge eating and purging in the high school years are associated with current and future eating disorder diagnoses. Those behaviors can be predicted by a combination of biological, personality, and learning risk factors assessed in late elementary and early middle school. Risk processes for binge eating and for purging have both similarities and differences.
Supplementary Material
Acknowledgments
This work was supported by NIAAA grant RO1 AA016166 to Gregory T. Smith.
Footnotes
The WLSMV method does not rely on full information maximum likelihood (FIML) estimation procedures for missing data. To evaluate whether the current findings were an artifact of the method of handling missing data, we estimated our model using two other procedures. First, we used maximum likelihood robust to violations of normality (MLR), which does use FIML. Results were the same. Second, we used a single imputation procedure available in SPSS that includes a correction for what would otherwise be biased-small standard error values, and again the results were the same. We chose to report the WLSMV results because the method makes possible reporting of standardized beta coefficients and classic fit index values such as RMSEA and CFI and does not rely on single imputation.
References
- Abebe DS, Lien L, von Soest T. The development of bulimic symptoms from adolescence to young adulthood in females and males: A population-based longitudinal cohort study. International Journal of Eating Disorders. 2012;45(6):737–745. doi: 10.1002/eat.20950. [DOI] [PubMed] [Google Scholar]
- Agras WS, Telch CF. The effects of caloric deprivation and negative affect on binge eating in obese binge-eating disordered women. Behavior Therapy. 1998;29(3):491–503. [Google Scholar]
- Allen MT, Matthews KA. Hemodynamic responses to laboratory stressors in children and adolescents: The influences of age, race, and gender. Psychophysiology. 1997;34(3):329–339. doi: 10.1111/j.1469-8986.1997.tb02403.x. [DOI] [PubMed] [Google Scholar]
- Annus AM, Smith GT, Masters K. Manipulation of thinness and restricting expectancies: Further evidence for a causal role of thinness and restricting expectancies in the etiology of eating disorders. Psychology of Addictive Behaviors. 2008;22(2):278–287. doi: 10.1037/0893-164X.22.2.278. [DOI] [PubMed] [Google Scholar]
- Berg KC, Peterson CB, Frazier P, Crow SJ. Convergence of scores on the interview and questionnaire versions of the Eating Disorder Examination: a meta-analytic review. Psychological Assessment. 2011;23(3):714–724. doi: 10.1037/a0023246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bolles RC. Reinforcement, expectancy, and learning. Psychological Review. 1972;79:394–409. [Google Scholar]
- Boyle L, Riley ER, Crosby R, Smith GT. Pubertal onset predicts increases in high-risk personality traits and drinking behavior. Manuscript submitted for publication 2018 [Google Scholar]
- Cacioppo JT, Cacioppo S, Boomsma DI. Evolutionary mechanisms for loneliness. Cognition & Emotion. 2014;28(1):3–21. doi: 10.1080/02699931.2013.837379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter JC, Stewart DA, Fairburn CG. Eating disorder examination questionnaire: Norms for young adolescent girls. Behaviour Research and Therapy. 2001;39(5):625–632. doi: 10.1016/s0005-7967(00)00033-4. [DOI] [PubMed] [Google Scholar]
- Caspi A. Why maladaptive behaviors persist: Sources of continuity and change across the life course. In: Funder DC, Parke RD, Tomlinson-Keasey C, Widaman K, editors. Studying lives through time: Personality and development. Washington, DC: American Psychological Association; 1993. pp. 343–376. [Google Scholar]
- Coleman L, Coleman J. The measurement of puberty: a review. Journal of Adolescence. 2002;25(5):535–550. doi: 10.1006/jado.2002.0494. [DOI] [PubMed] [Google Scholar]
- Combs JL, Pearson CM, Smith GT. A risk model for preadolescent disordered eating. International Journal of Eating Disorders. 2011;44(7):596–604. doi: 10.1002/eat.20851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper MJ, Fairburn CG. Demographic and clinical correlates of selective information processing in patients with bulimia nervosa. International Journal of Eating Disorders. 1993;13(1):109–116. doi: 10.1002/1098-108x(199301)13:1<109::aid-eat2260130113>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- Culbert KM, Burt SA, McGue M, Iacono WG, Klump KL. Puberty and the genetic diathesis of disordered eating attitudes and behaviors. Journal of Abnormal Psychology. 2009;118:788–796. doi: 10.1037/a0017207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, Smith GT. Mood-based rash action and its components: Positive and negative urgency. Personality and Individual Differences. 2007;43(4):839–850. [Google Scholar]
- Davis HA, Ortiz AM, D’Agostino AR, Smith GT. A two-stage risk model for bulimic behavior. In: Morton N, editor. Eating Disorders: Prevalence, Risk Factors, and Treatment Options. New York: Nova Science Publishers; 2016. pp. 97–120. [Google Scholar]
- Davis HA, Ortiz AML, Smith GT. The occurrence and covariation of binge eating and compensatory behaviors across early to mid-adolescence. Journal of Pediatric Psychology. :jsx113. doi: 10.1093/jpepsy/jsx113. in press. [DOI] [PMC free article] [PubMed]
- Day J, Schmidt U, Collier D, Perkins S, Van den Eynde F, Treasure J, Keville S. Risk factors, correlates, and markers in early-onset bulimia nervosa and EDNOS. International Journal of Eating Disorders. 2011;44(4):287–294. doi: 10.1002/eat.20803. [DOI] [PubMed] [Google Scholar]
- Dick DM, Rose RJ, Viken RJ, Kaprio J. Pubertal timing and substance use: associations between and within families across late adolescence. Developmental Psychology. 2000;36(2):180–189. [PubMed] [Google Scholar]
- Doran N, Khoddam R, Sanders PE, Schweizer CA, Trim RS, Myers MG. A prospective study of the acquired preparedness model: The effects of impulsivity and expectancies on smoking initiation in college students. Psychology of Addictive Behaviors. 2013;27(3):714–722. doi: 10.1037/a0028988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis BJ. Timing of pubertal maturation in girls: an integrated life history approach. Psychological Bulletin. 2004;130(6):920–958. doi: 10.1037/0033-2909.130.6.920. [DOI] [PubMed] [Google Scholar]
- Enders CK, Peugh JL. Using an EM covariance matrix to estimate structural equation models with missing data: Choosing an adjusted sample size to improve the accuracy of inferences. Structural Equation Modeling. 2004;11(1):1–19. [Google Scholar]
- Fairburn CG, Beglin SJ. Assessment of eating disorders: Interview or self-report questionnaire? International Journal of Eating Disorders. 1994;16(4):363–370. [PubMed] [Google Scholar]
- Fairburn CG, Cooper Z, Shafran R. Enhanced cognitive behavior therapy for eating disorders (“ CBT-E”): An overview. In: Fairburn CG, editor. Cognitive behavior therapy and eating disorders. New York: Guilford Press; 2008. pp. 23–24. [Google Scholar]
- Fischer S, Peterson CM, McCarthy D. A prospective test of the influence of negative urgency and expectancies on binge eating and purging. Psychology of Addictive Behaviors. 2013;27(1):294–300. doi: 10.1037/a0029323. [DOI] [PubMed] [Google Scholar]
- Fischer S, Smith GT, Cyders MA. Another look at impulsivity: A meta-analytic review comparing specific dispositions to rash action in their relationship to bulimic symptoms. Clinical Psychology Review. 2008;28(8):1413–1425. doi: 10.1016/j.cpr.2008.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gardner RM, Stark K, Friedman BN, Jackson NA. Predictors of eating disorder scores in children ages 6 through 14: A longitudinal study. Journal of Psychosomatic Research. 2000;49(3):199–205. doi: 10.1016/s0022-3999(00)00172-0. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Brown SA, Christiansen BA, Smith GT. Alcoholism and Memory- broadening the scope of alcohol-expectancy research. Psychological Bulletin. 1991;110:137–146. doi: 10.1037/0033-2909.110.1.137. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Darkes J, Del Boca FK. Expectancy mediation of biopsychosocial risk for alcohol use and alcoholism. In: Kirsch I, editor. How Expectancies Shape Experience. Washington, DC: American Psychological Association; 1999. pp. 233–262. [Google Scholar]
- Goldschmidt AB, Aspen VP, Sinton MM, Tanofsky-Kraff M, Wilfley DE. Disordered eating attitudes and behaviors in overweight youth. Obesity. 2008;16(2):257–264. doi: 10.1038/oby.2007.48. [DOI] [PubMed] [Google Scholar]
- Haedt-Matt AA, Keel PK. Revisiting the affect regulation model of binge eating: A meta-analysis of studies using ecological momentary assessment. Psychological Bulletin. 2011;137:660–681. doi: 10.1037/a0023660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hohlstein LA, Smith GT, Atlas JG. An application of expectancy theory to eating disorders: Development and validation of measures of eating and dieting expectancies. Psychological Assessment. 1998;10(1):49–58. [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6(1):1–55. [Google Scholar]
- Klump KL, Keel PK, Sisk C, Burt SA. Preliminary evidence that estradiol moderates genetic influences on disordered eating attitudes and behaviors during puberty. Psychological Medicine. 2010;40(10):1745–1753. doi: 10.1017/S0033291709992236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klump KL, McGue M, Iacono WG. Differential heritability of eating attitudes and behaviors in prepubertal versus pubertal twins. International Journal of Eating Disorders. 2003;33(3):287–292. doi: 10.1002/eat.10151. [DOI] [PubMed] [Google Scholar]
- Klump KL, Perkins PS, Burt SA, McGue M, Iacono WG. Puberty moderates genetic influences on disordered eating. Psychological Medicine. 2007;37(5):627–634. doi: 10.1017/S0033291707000189. [DOI] [PubMed] [Google Scholar]
- Kotler LA, Cohen P, Davies M, Pine DS, Walsh BT. Longitudinal relationships between childhood, adolescent, and adult eating disorders. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40(12):1434–1440. doi: 10.1097/00004583-200112000-00014. [DOI] [PubMed] [Google Scholar]
- Laurent J, Catanzaro SJ, Joiner TE, Jr, Rudolph KD, Potter KI, Lambert S, Gathright T. A measure of positive and negative affect for children: scale development and preliminary validation. Psychological Assessment. 1999;11(3):326–338. [Google Scholar]
- Leon GR, Fulkerson JA, Perry CL, Keel PK, Klump KL. Three to four year prospective evaluation of personality and behavioral risk factors for later disordered eating in adolescent girls and boys. Journal of Youth and Adolescence. 1999;28(2):181–196. [Google Scholar]
- Luce KH, Crowther JH. The reliability of the eating disorder examination—Self-report questionnaire version (EDE-Q) International Journal of Eating Disorders. 1999;25(3):349–351. doi: 10.1002/(sici)1098-108x(199904)25:3<349::aid-eat15>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- Luna B, Sweeney JA. The emergence of collaborative brain function: FMRI studies of the development of response inhibition. Annals of the New York Academy of Sciences. 2004;1021(1):296–309. doi: 10.1196/annals.1308.035. [DOI] [PubMed] [Google Scholar]
- Mendle J. Beyond pubertal timing: New directions for studying individual differences in development. Current Directions in Psychological Science. 2014;23(3):215–219. [Google Scholar]
- Mond JM, Hay PJ, Rodgers B, Owen C, Beumont PJ. Validity of the Eating Disorder Examination Questionnaire (EDE-Q) in screening for eating disorders in community samples. Behaviour Research and Therapy. 2004;42(5):551–567. doi: 10.1016/S0005-7967(03)00161-X. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. User’s guide. 3rd. Los Angeles, CA: Muthén & Muthén; 2004–2010. Mplus: The comprehensive modeling program for applied researchers. [Google Scholar]
- Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, Loth K. Dieting and disordered eating behaviors from adolescence to young adulthood: findings from a 10-year longitudinal study. Journal of the American Dietetic Association. 2011;111(7):1004–1011. doi: 10.1016/j.jada.2011.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paxton SJ, Neumark-Sztainer D, Hannan PJ, Eisenberg ME. Body dissatisfaction prospectively predicts depressive mood and low self-esteem in adolescent girls and boys. Journal of Clinical Child and Adolescent Psychology. 2006;35(4):539–549. doi: 10.1207/s15374424jccp3504_5. [DOI] [PubMed] [Google Scholar]
- Pearson CM, Combs JL, Zapolski TC, Smith GT. A longitudinal transactional risk model for early eating disorder onset. Journal of Abnormal Psychology. 2012;121(3):707–718. doi: 10.1037/a0027567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearson CM, Wonderlich SA, Smith GT. A risk and maintenance model for bulimia nervosa: From impulsive action to compulsive behavior. Psychological Review. 2015a;122(3):516–535. doi: 10.1037/a0039268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearson CM, Zapolski TC, Smith GT. A longitudinal test of impulsivity and depression pathways to early binge eating onset. International Journal of Eating Disorders. 2015b;48(2):230–237. doi: 10.1002/eat.22277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: Reliability, validity, and initial norms. Journal of Youth and Adolescence. 1988;17(2):117–133. doi: 10.1007/BF01537962. [DOI] [PubMed] [Google Scholar]
- Polivy J, Herman CP. Dieting and binging: A causal analysis. American Psychologist. 1985;40(2):193–201. doi: 10.1037//0003-066x.40.2.193. [DOI] [PubMed] [Google Scholar]
- Racine SE, Keel PK, Burt SA, Sisk CL, Neale M, Boker S, Klump KL. Exploring the relationship between negative urgency and dysregulated eating: Etiologic associations and the role of negative affect. Journal of Abnormal Psychology. 2013;122:433–444. doi: 10.1037/a0031250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Settles RF, Cyders M, Smith GT. Longitudinal validation of the acquired preparedness model of drinking risk. Psychology of Addictive Behaviors. 2010;24(2):198–208. doi: 10.1037/a0017631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith GT, Cyders MA. Integrating affect and impulsivity: The role of positive and negative urgency in substance use risk. Drug and Alcohol Dependence. 2016;163:S3–S12. doi: 10.1016/j.drugalcdep.2015.08.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith GT, Simmons JR, Flory K, Annus AM, Hill KK. Thinness and eating expectancies predict subsequent binge-eating and purging behavior among adolescent girls. Journal of Abnormal Psychology. 2007;116(1):188–197. doi: 10.1037/0021-843X.116.1.188. [DOI] [PubMed] [Google Scholar]
- Smith GT, Williams SF, Cyders MA, Kelley S. Reactive personality-environment transactions and adult developmental trajectories. Developmental Psychology. 2006;42(5):877–887. doi: 10.1037/0012-1649.42.5.877. [DOI] [PubMed] [Google Scholar]
- Smyth JM, Heron KE, Sliwinski MJ, Wonderlich SA, Crosby RD, Mitchell JE, et al. Daily and momentary mood and stress are associated with binge eating and vomiting in bulimia nervosa patients in the natural environment. Journal of Consulting and Clinical Psychology. 2007;75:629–638. doi: 10.1037/0022-006X.75.4.629. [DOI] [PubMed] [Google Scholar]
- Spear LP. Neurobehavioral changes in adolescence. Current Directions in Psychological Science. 2000;9:111–114. [Google Scholar]
- Steinberg L. Risk taking in adolescence: what changes, and why? Annals of the New York Academy of Sciences. 2004;1021(1):51–58. doi: 10.1196/annals.1308.005. [DOI] [PubMed] [Google Scholar]
- Stice E. A prospective test of the dual-pathway model of bulimic pathology: mediating effects of dieting and negative affect. Journal of Abnormal Psychology. 2001;110(1):124–135. doi: 10.1037//0021-843x.110.1.124. [DOI] [PubMed] [Google Scholar]
- Stice E. Risk and maintenance factors for eating pathology: a meta-analytic review. Psychological Bulletin. 2002;128(5):825–848. doi: 10.1037/0033-2909.128.5.825. [DOI] [PubMed] [Google Scholar]
- Stice E, Burton EM, Shaw H. Prospective relations between bulimic pathology, depression, and substance abuse: unpacking comorbidity in adolescent girls. Journal of Consulting and Clinical Psychology. 2004;72:62–71. doi: 10.1037/0022-006X.72.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Killen JD, Hayward C, Taylor CB. Age of onset for binge eating and purging during late adolescence: a 4-year survival analysis. Journal of Abnormal Psychology. 1998;107(4):671. doi: 10.1037//0021-843x.107.4.671. [DOI] [PubMed] [Google Scholar]
- Stice E, Ng J, Shaw H. Risk factors and prodromal eating pathology. Journal of Child Psychology and Psychiatry. 2010;51(4):518–525. doi: 10.1111/j.1469-7610.2010.02212.x. [DOI] [PubMed] [Google Scholar]
- Ricciardelli LA, McCabe MP. Children’s body image concerns and eating disturbance: A review of the literature. Clinical Psychology Review. 2001;21(3):325–344. doi: 10.1016/s0272-7358(99)00051-3. [DOI] [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Shomaker LB, Olsen C, Roza CA, Wolkoff LE, Columbo KM, Yanovski JA. A prospective study of pediatric loss of control eating and psychological outcomes. Journal of Abnormal Psychology. 2011;120(1):108–118. doi: 10.1037/a0021406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tolman EG. Purposive Behavior in Animals and Men. New York: Century; 1932. [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology. 1988;54(6):1063–1070. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- Weiss NH, Sullivan TP, Tull MT. Explicating the role of emotion dysregulation in risky behaviors: A review and synthesis of the literature with directions for future research and clinical practice. Current Opinion in Psychology. 2015;3:22–29. doi: 10.1016/j.copsyc.2015.01.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TC, Smith GT. Pilot Study: Implementing a brief DBT skills program in schools to reduce health risk behaviors among early adolescents. The Journal of School Nursing. 2017;33(3):198–204. doi: 10.1177/1059840516673188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TC, Stairs AM, Settles RF, Combs JL, Smith GT. The measurement of dispositions to rash action in children. Assessment. 2010;17(1):116–125. doi: 10.1177/1073191109351372. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.