

An 8-year-old Saudi boy presented with a skin eruption consisting of a persistent, migratory non-pruritic erythematous maculopapular rash involving the whole body, which had been present since the neonatal period. The rash never completely resolved. At the age of 9 months, he developed joint pain and progressive swelling involving both the knees and left ankle. The child was able to walk, but with a limp. He also had a history of intermittent high-grade fever and headache. He had normal developmental milestones. His systemic review was unremarkable. The parents were non-consanguinous. There was no similar condition in the family.
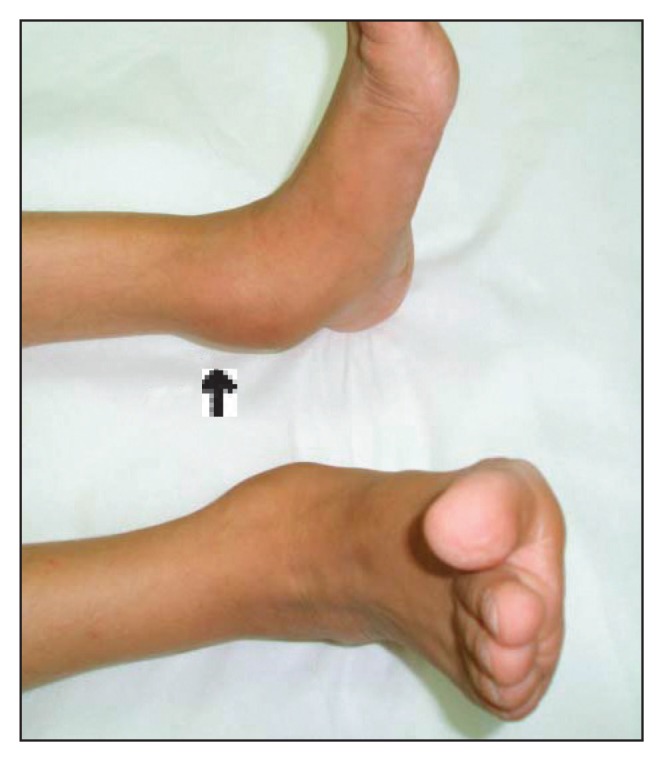
Physical examination revealed a height and weight below the fifth percentile for his age, a big head with frontal bossing, low set ears and a beaked nose. There was generalized lymphadenopathy and hepatosplenomegaly. Both knees and the left ankle were swollen, with mild tenderness and a decreased range of motion in the joints (Figures 1 and 2). There was marked wasting of both thigh muscles. The rest of the examination was unremarkable.
Figure 1.

Figure 2.
Results of laboratory investigations included a white blood cell count of 23×109/L, with 72% neutrophils and 24% lymphocytes, hemoglobin 89 g/L with a microscopic hypochromic picture, and platelets 522×109/L. The erythrocyte sedimentation rate (ESR) was 65 mm/h. Electrolytes and hepatic profiles were within normal limits. Autoantibodies, including antinuclear antibodies (ANA) and rheumatoid factor (RF), were negative. Radiographs of both knees and ankles were abnormal (Figures 3 and 4). CT of the brain was unremarkable.
Figure 3.

Figure 4.
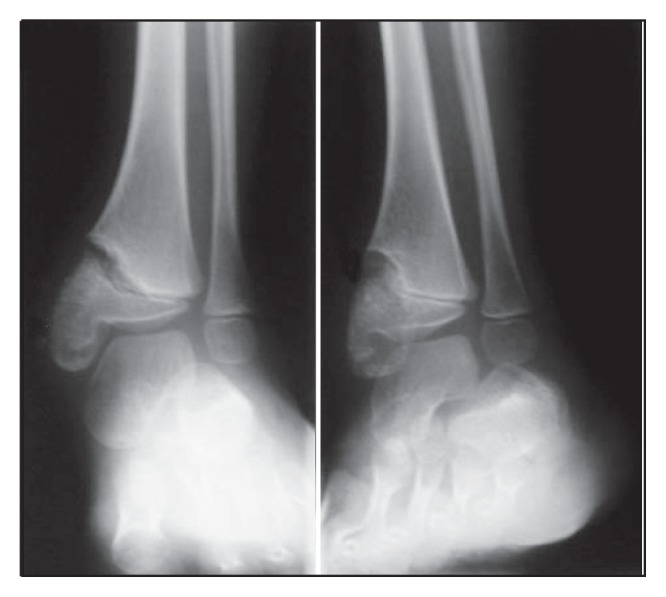
What are the abnormalities seen in the radiographs?
What is the diagnosis?