

Abstract
Purpose
The aim of this article is to review the current concepts in the indications, results and failure causes of the treatment of developmental dysplasia of the hip (DDH) with the Pavlik harness.
Methods:
The reported variables influencing the outcome in the Pavlik harness treatment were analyzed.
Results
Significant discrepancies about the clinical and radiological outcomes, the rates of failure and complications as well as the variables influencing the treatment outcome occur in the published studies due to the heterogeneity of the data and the differences in the methods used. The overall short-, mid- or long-term success rate of the treatment ranges from 45% to 100% and it is commonly over 75%. The rate of osteonecrosis of the femoral head ranges from 1% to 30%. Age, gender, laterality, radiological or clinical severity of the initial hip pathology and parents’ compliance are the commonly reported determinants of failure of the treatment.
Conclusion
The failure in treatment with the Pavlik harness is multifactorial, initial type of hip dysplasia being the most prominent followed by the treatment initiation age. This type of treatment cannot be considered as the best option in Graf IV hips (hip ultrasonography) or highly dislocated hips (plain radiography) and in infants older than three months of age, as the risk of failure and development of complications including osteonecrosis and femoral nerve palsy seem to increase in such circumstances. Large-scale, comparative studies including homogenous data are needed to answer the unsolved questions concerning indications.
Keywords: developmental dysplasia of the hip, treatment, Pavlik harness
Introduction
The fundamental goal of the treatment of developmental dysplasia of the hip (DDH) is to obtain a concentric reduction as early as possible and to maintain this early reduction for the achievement of normal development of the proximal femur and acetabulum. This basic treatment principle is applicable to all age groups in children.1 Arnold Pavlik developed his device ‘harness with stirrups’ in the 1940s. He considered active movement of the hip joint as the most important therapeutic factor in the treatment of DDH and named his method ‘functional treatment’. The main aim of Pavlik was to achieve spontaneous and harmless repositioning and centralization of the femoral head in order to reach the best anatomical and functional outcome in children up to one year of age.2,3 He hypothesized that his device, keeping the hips and knees in flexion and the hips in abduction, allowing active hip movements, first relaxed the adduction contracture and then a spontaneous reduction would occur during the abduction movements.2,3 Mubarak and Bialik4 have introduced the concept of ‘Pavlik’s method’ as it is the method not the device that leads to a higher success rate of treatment in DDH.
According to the clinical observations of Iwasaki5 and the 3D computer model of Ardila et al,6 the mechanism of femoral head reduction in a dislocated hip in Pavlik’s method is a result of movement of the femoral head from the superior position to the posterior aspect of the acetabulum. This is promoted by hip flexion and is followed by the sliding of the dislocated femoral head anteriorly over the posterior acetabular rim into the acetabulum. This in turn is promoted by the relaxation of the resistive factors, primarily the hip adductor muscles. According to Suzuki7 passive abduction of the hip by the weight of the lower limb, which only occurs in deep sleep is the main factor, which leads to spontaneous reduction of the hip.
Indications
Pavlik’s method is still the most common initial treatment for DDH in infants under the age of six months (Fig. 1). After six months of age its use is not recommended, as it may be difficult to maintain the active and crawling child in the harness.1,8 Pavlik initially considered the first eight to nine weeks of life as the best time to apply his harness, as the acetabulum was not filled with the interposed soft tissue in younger infants, and repositioning and recentralization of the femoral head could be easier in this group of patients.2 However, treatment with the Pavlik harness was found to be applicable to clinically reducible and sonographically Graf type III hips9 between six and 24 months of age in one study.10 Based on the published data in the literature, it can be said that a high level of scientific evidence regarding the commonly accepted six months upper age limit is currently not available.
Fig. 1.
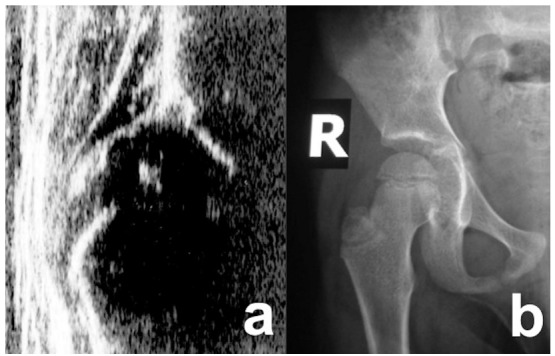
Initial right hip sonogram of five-month-old female patient who showed a Graf type D hip (a:43°, b:90°) (a). Pavlik harness treatment was initiated and the hip became normal within 12 weeks. Anteroposterior right hip radiograph of the same patient at 4.5 years of age (b) showed a satisfactory radiographic outcome.
Hip ultrasonography provides early and accurate diagnosis of the hip pathology as well as safe follow-up of the hips treated by the Pavlik harness.11 It facilitates the treatment and allows early recognition of treatment failure, lessens the radiation exposure during the entire treatment, decreases the duration of treatment and reduces complication rates.12,13 Besides, checking the reducibility of the dislocated hips by the Ortolani maneuver can be a useful clinical diagnostic tool while making the treatment decision and following the treated hips.1
The optimal duration of treatment with the Pavlik harness remains controversial. The harness application hours per day and discontinuation protocols are variable in many case series. However, minimizing the time spent in the harness can be advantageous to avoid several complications. In a comparative study, immediate cessation of the harness application whenever the hip became sonographically normal was recommended, as no differences in the radiological outcomes and rate of complications including reintervention and osteonecrosis of the femoral head (ON) were found between immediate cessation and gradual weaning in Pavlik’s method.14 It may be better to individualize the treatment for each hip and not to determine strict time limits for the treatment.15
Closed or open reduction and casting is commonly preferred whenever treatment by Pavlik’s method fails in subluxated or dislocated hips1 (Fig. 2). Higher rate of success and lower rate of ON were reported by closed or open reduction following a failed Pavlik harness treatment attempt within the first three months of life.16 On the other hand, the hips treated by closed or open reduction following a previous failed Pavlik harness treatment attempt were found to be at about four times higher risk of developing a severe type of ON than the hips treated by solely closed or open reduction due to late referral of the patients after three months of age with no attempt of Pavlik’s method made.17 Alternatively, static bracing was considered as the treatment of choice in cases with a history of failed Pavlik harness treatment before proceeding with the closed reduction and casting, as satisfactory outcomes and lower complication rates could be obtained by static braces in selected cases.18,19
Fig. 2.
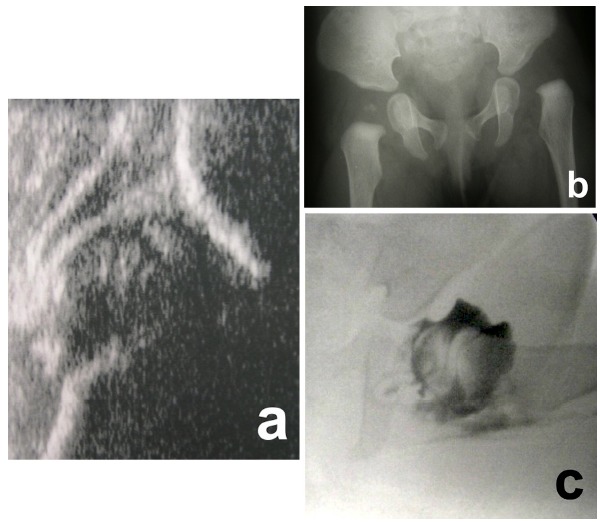
Initial left hip sonogram of a female patient at six months of age who showed a Graf type IIIb hip (a:40°, b:100°) (a). A Pavlik harness was initially used but the treatment was considered to fail within four weeks. Anteroposterior pelvic radiograph of the same patient at seven months of age (b) showed that the left hip was still dislocated, so an immediate closed/open reduction and casting was planned. Intraoperative arthrogram of the same patient (c) following iliopsoas and adductor tenotomies through the posteromedial approach showed that the labrum was inverted, transverse acetabular ligament was hypertrophied and there was still medial pooling of the dye due to hypertrophied ligamentum teres. An open reduction was performed to obtain a concentric reduction.
Results of treatment
Although Pavlik’s method has gained widespread use in many parts of the world for the treatment of DDH, significant discrepancies about the clinical and radiological outcomes, the rates of failure and complications as well as the variables influencing the treatment outcomes occur in the published studies. This issue mainly depends on the heterogeneity of the data and the differences in the methods used. Treatment initiation age, definition of the failure or success of the treatment, treatment protocol used (solely Pavlik’s method or combination with another method, duration of treatment), diagnostic methods (clinical examination, plain radiographs and radiographic indicators, ultrasonography and ultrasonographic techniques or combination of more than one diagnostic method), dysplastic hip types included in the study, follow-up protocol and period, statistical analysis (univariate or multivariate), determination of ON rates (used criteria and classification type, ON rates of successfully treated hips or all hips) and the geographic area where the study has been conducted, show significant variances in the published studies. The treatment protocols including diagnostic methods, recommended time for treatment, follow-up and discontinuation regimens vary between North America and Europe.8 Even the definition of Graf type III and IV hips in some studies is not compatible with the clear description of these hip types that has already been made by Graf.9
Pavlik2 reported his experience in 640 dysplastic, 640 subluxated and 632 dislocated hips in 1957. The success rate was 100% and ON rate was zero in dysplastic and subluxated hips. Among the dislocated hips 84.1% reduced spontaneously and ON rate was zero in the spontaneously reduced hips.
The number of studies reporting the outcomes of Pavlik’s method in a considerable number of patients is limited; there only are a couple of multicentre studies. In the European Paediatric Orthopaedic Society’s multicentre study20 including 3611 hips treated with the Pavlik harness under 11 months of age (mean age 4.1 months), 92% of the hips graded radiographically as grades II and III according to the ‘commission for the study of hip dysplasia of the German society’ (CSHD) classification system21 were found to be reducible. The overall mid-term radiographic healing rate was found to be 95% and ON rate 2.4%. Infants between three and six months of age and CSHD grade IV hips had higher rates of failure and ON.20 In a multicentre study from Japan22 including nearly 4000 hips with complete dislocations (mean treatment initiation ages range from 3.5 to 4.8 months) that were followed until skeletal maturity, the rate of hip relocation by Pavlik’s method was around 80%, the rate of ON was about 11% and a satisfactory radiographic outcome without any additional osteotomies in the long-term follow-up was obtained in about 75% of the hips. The overall success rates in other studies ranged from 45% to 100% and in about two-thirds of these studies it was more than 75%.5,10,12,13,23–48
The rate of ON related to Pavlik’s method shows a wide range from 1% to 30% in the literature8 (Fig. 3). The correlation between the severity of hip dysplasia and development of ON was assessed in several publications. The risk of development of ON was found to be higher in sonographical Graf type IV35,46,48 or radiographically dislocated hips.31 On the other hand, a correlation between the type of hip pathology and the development of ON was not confirmed in another study.45 Initiation of the treatment over three months of age,49 non-visible ossific nucleus at the time of treatment initiation,40 prolonged duration of treatment49 and accompanying significant adductor muscle contracture30 were the other reported variables related to an increased risk of development of ON. The rate of ON in the contralateral healthy hip in unilateral cases treated by Pavlik’s method was found to be 2.9% and almost all such affected hips had mild type ON.49
Fig. 3.
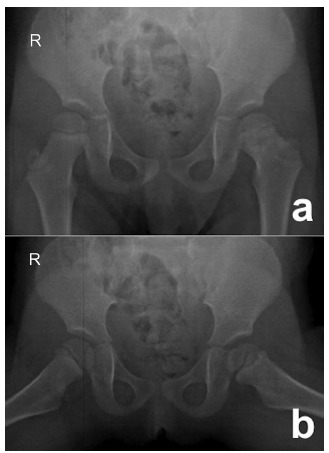
Anteroposterior (a) and frog-leg (b) pelvic radiographs of a three-year-old female patient who had been treated by Pavlik’s method due to Graf type IIb hip on the left side at four months of age. This revealed osteonecrosis of the femoral head (ON) involving the ossific nucleus and central physis. Although the hip became normal (Graf type I) following eight weeks treatment, ON could not be prevented.
Treatment failures
The faults leading to failure in Pavlik’s method can be physician-related, parent-related or idiopathic.50 The physician-related faults include inappropriate indication or the poor quality of the harness. Patient-related variables such as age, gender, laterality and severity of hip dysplasia will be evaluated as separate entities in this article.
Treatment initiation age
‘The younger the patient, the lower the risk of failure’ is a widely accepted concept. However, there are conflicting reports concerning this concept. The reported failure rates in sonographically pathological hips under the age of three to four weeks were 4% and 7% in two different studies including Graf type IIc and worse hips,32,48 whereas they stood at 20% and 37% in two other studies including only dislocated hips.28,43 A considerable increase in the failure rate of Pavlik’s method was noted in infants older than three weeks with highly dislocated hips.28 A treatment initiation age of seven weeks and older was considered a risk for failure in two studies.24,51 In the published case series including only infants younger than three months of age, the overall failure rate of Pavlik’s method ranged from 3% to 42% (mostly around 10% to 15%).23,25–27,35,38,39,48 Pavlik’s method was found to fail in infants 120 days and older (sensitivity 66%, specificity 76%), with sonographically stable and unstable dysplastic hips.37 The same age limit was reported as a risk factor for failure in another study including infants with dislocated hips.29
Gender
Male gender was considered a significant risk factor correlated with the failure of Pavlik’s method in two studies.36,52 In one study, 93% of the male patients treated with the Pavlik harness at a mean age of seven weeks needed other treatment modalities.52 Besides, the treatment duration was found to be somewhat longer in male than in female patients.39
Laterality
Bilateral involvement was found to be associated with the failure of Pavlik’s method in some studies24,30,51 whereas it was not in others.25,37,38
Radiographic indicators
Increased lateral and superior displacement of the femoral head assessed by quantitative measurements,29,30 complete dislocation of the femoral head (CSHD grade III and IV hips)12,26,31,44 and an initial acetabular index of more than 36°29 were reported as the radiographic indicators for failure.
Ultrasonographic indicators
As different infantile hip ultrasonography techniques have been defined in the literature, different ultrasonographic indicators for failure exist. In the studies using Graf’s classification system,9 dislocated hips (Graf type III and IV) were found to have higher rates of failure than the other hip types (Fig. 2). The reported failure rates of Graf type III and Graf type IV hips ranged from 0% to 74%, (mostly less than 25%) and from 0% to 100%, (mostly between 50% and 100%), respectively.10,24,27,34,35,37–39,42,45,46,48 Besides, the risk of failure in Graf type IV hips was found to be about four times higher than in Graf type III hips.36 It is evident that the Graf type IV hip has the highest rate of failure among the hip types in Graf’s classification system. Besides, an alpha angle of less than 47° (sensitivity 47%, specificity 86%) was found to be the threshold value for the failure in Pavlik’s method.37 A higher beta angle was found to correlate with the failure as well.47 In the studies using other methods, the reported ultrasonographic indicators for short- or mid-term failures were dislocated, irreducible hips during dynamic examination, coverage percentage less than 20% and an initial abnormal echogenicity of the cartilaginous roof.23,33,46,53
Clinical examination
Clinical reducibility or irreducibility of the radiologically dislocated hip was reported to correlate with the treatment outcome in several studies. The rate of failure was found to be about 60% in dislocated, irreducible hips33,51 whereas it was about 40% in dislocated, reducible hips.10,33,47
Femoral nerve palsy
The rate of femoral nerve palsy was reported to be 2.5% in a large case series.54 Higher body mass index and older age were found to be risk factors correlated with the occurrence of femoral nerve palsy. Graf type IV hip was present in 70% of the cases with femoral nerve palsy.54
Parents’ compliance
Parents may fail to properly apply the harness or to keep the harness on the child.50 The harness may be reapplied incorrectly or reapplication may fail completely if the parents are not well-instructed.55 The most common problems stated by parents are difficulties during reapplication after bathing, the foot slipping from the harness, difficulties in clothing, carrying and seating the child in in the car and skin problems.56,57 Mothers’ mental reactions and emotional difficulties are other factors that may influence the parents’ compliance.57 A simulated training module may improve the confidence and skill levels of parents in the application of the Pavlik harness.55 Cultural traditions may also affect parents’ compliance.
Other variables
Accompanying risk factors for DDH including post-natal swaddling history, multigravida and foot deformities were considered to increase the risk for failure.37,43 Full-term babies had a tendency to fail Pavlik’s method.47
Discussion
There are few published data comparing the efficacy of the Pavlik harness with other abduction braces. The Von Rosen splint was considered to have a better ultrasonographic improvement and lesser need for further treatment than Pavlik’s method had in infants younger than 4.5 months with Graf type III and IV hips.58 It was hypothesized that a non-rigid splint might not maintain the femoral head in the centre of a very dysplastic acetabulum.58 Custom-made static bracing was found to have higher success rate than Pavlik’s method had in sonographically stable but dysplastic hips.59 The rates of failure and ON were found to be similar in two studies comparing Pavlik harness and Frejka’s pillow.60,61
We have developed an algorithm while treating babies with Pavlik’s method for the last 20 years (Fig. 4). Our upper treatment initiation age limit is six months and we have been using hip ultrasonography by Graf’s method9 for diagnosis and follow-up, looking for whether or not sonographic improvement of certain hip types can be achieved in a certain period of time. If Graf type D, III or IV hips (decentred hips) do not progress into a better ultrasonographic hip type or worsen within three to four weeks, or Graf type IIa-, IIb or IIc hips (stable hips) do not progress into a better ultrasonographic hip type or worsen within eight weeks, or femoral nerve palsy occurs, then we consider these situations as the failure of the treatment and switch to another treatment modality (Figs 1 and 2). We discontinue the treatment on the day when the hip becomes Graf type I. The success rate of this algorithm was reported to be 96% in infants under the age of four weeks32 and more than 90% in infants under the age of three months.37 However, we have some concerns about the use of Pavlik’s method, especially in older infants and in certain hip types, particularly Graf type IV hips.
Fig. 4.
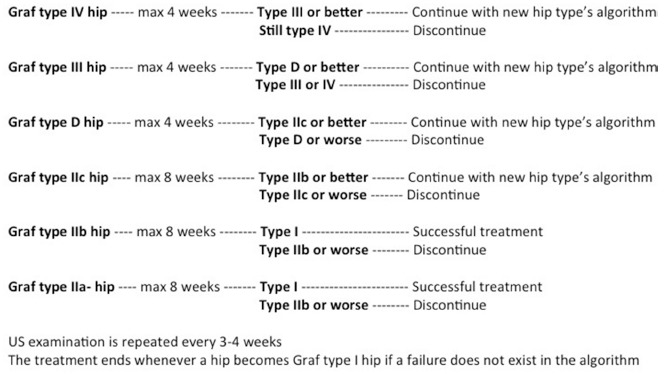
Our algorithm in the treatment of developmental dysplasia of the hip (DDH) with the Pavlik harness (US, ultrasound).
Four important prerequisites for the success of treatment have been pointed out:41
an appropriate indication;
typical DDH;
cooperative parents with adequate knowledge about DDH;
a good quality harness.
Besides, the importance of health professionals’ training should be taken into consideration. A simulation-based learning module can be an effective tool for residents and allied health professionals to teach and improve the skills in the application of a Pavlik harness.62
Based on the existing knowledge in the literature four questions need further research:
Is Pavlik’s method the best one in the conservative treatment of DDH?
Should we attempt Pavlik’s method in every infant with typical DDH under the age of six months?
Is Pavlik’s method the first choice of treatment in Graf type IV or highly dislocated hips until six months of age?
Should closed/open reduction be the first choice of treatment in infants older than three months of age with Graf type IV hips?
Conclusions
Correct treatment indication followed by a close collaboration with the parents and a careful radiological follow-up, preferably by hip ultrasonography, are the main key points for success in Pavlik’s method. A limited high level of scientific evidence concerning the efficacy of Pavlik’s method in the treatment of DDH currently exists due to the heterogeneity of the available data in the literature. Based on the existing knowledge drawn from the literature, it can be concluded that the failure of Pavlik’s method is multifactorial, the initial type of hip dysplasia being the most prominent followed by the treatment initiation age of the patient. Pavlik’s method cannot be considered as the best treatment option in Graf IV hips (hip ultrasonography) or highly dislocated hips (plain radiography) and in infants older than three months of age, as the risk of failure and development of complications including ON and femoral nerve palsy seem to increase in such circumstances. Large-scale, prospective randomized trials including homogenous data with long-term follow-up are needed to clarify all the controversial points and to answer the unsolved questions.
Compliance with ethical standards
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
OA Licence Text
This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) license (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.
Ethical statement
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent: Not required.
ICMJE Conflict of interest statement
None declared.
References
- 1.Weinstein SL. Developmental hip dysplasia and dislocation In: Weinstein SL, Flynn JM, eds Lovell and Winter’s pediatric orthopaedics. 7th ed Philadelphia: Wolter-Kluwer, 2014:983–1111. [Google Scholar]
- 2.Pavlik A. The functional method of treatment using a harness with stirrups as the primary method of conservative therapy for infants with congenital dislocation of the hip. 1957. Clin Orthop Relat Res 1992;281:4–10. [PubMed] [Google Scholar]
- 3.Pavlik A. To the question of originality of treatment of congenital hip dysplasias by active movement in the stirrups. 1959. J Pediatr Orthop B 2001;10:165–168. [PubMed] [Google Scholar]
- 4.Mubarak SJ, Bialik V. Pavlik: the man and his method. J Pediatr Orthop 2003;23:342–346. [PubMed] [Google Scholar]
- 5.Iwasaki K. Treatment of congenital dislocation of the hip by the Pavlik harness. Mechanism of reduction and usage. J Bone Joint Surg [Am] 1983;65-A:760–767. [PubMed] [Google Scholar]
- 6.Ardila OJ, Divo EA, Moslehy FA, et al. Mechanics of hip dysplasia reductions in infants using the Pavlik harness: a physics-based computational model. J Biomech 2013;46:1501–1507. [DOI] [PubMed] [Google Scholar]
- 7.Suzuki S. Reduction of CDH by the Pavlik harness. Spontaneous reduction observed by ultrasound. J Bone Joint Surg [Br] 1994;76-B:460–462. [PubMed] [Google Scholar]
- 8.Tibrewal S, Gulati V, Ramachandran M. The Pavlik method: a systematic review of current concepts. J Pediatr Orthop B 2013;22:516–520. [DOI] [PubMed] [Google Scholar]
- 9.Graf R. Hip sonography. Diagnosis and management of infant hip dysplasia. 2nd ed. Berlin, Heidelberg: Springer-Verlag, 2006. [Google Scholar]
- 10.Pollet V, Pruijs H, Sakkers R, Castelein R. Results of Pavlik harness treatment in children with dislocated hips between the age of six and twenty-four months. J Pediatr Orthop 2010;30:437–442. [DOI] [PubMed] [Google Scholar]
- 11.Omeroğlu H. Use of ultrasonography in developmental dysplasia of the hip. J Child Orthop 2014;8:105–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hangen DH, Kasser JR, Emans JB, Millis MB. The Pavlik harness and developmental dysplasia of the hip: has ultrasound changed treatment patterns? J Pediatr Orthop 1995;15:729–735. [DOI] [PubMed] [Google Scholar]
- 13.Taylor GR, Clarke NMP. Monitoring the treatment of developmental dysplasia of the hip with the Pavlik harness. The role of ultrasound. J Bone Joint Surg [Br] 1997;79-B:719–723. [DOI] [PubMed] [Google Scholar]
- 14.Westacott DJ, Mackay ND, Waton A, et al. Staged weaning versus immediate cessation of Pavlik harness treatment for developmental dysplasia of the hip. J Pediatr Orthop B 2014;23:103–106. [DOI] [PubMed] [Google Scholar]
- 15.Bialik V. Pavlik’s method in developmental dysplasia of the hip. Acta Orthop Traumatol Turc 2007;41:19–24. [PubMed] [Google Scholar]
- 16.Senaran H, Bowen JR, Harcke HT. Avascular necrosis rate in early reduction after failed Pavlik harness treatment of developmental dysplasia of the hip. J Pediatr Orthop 2007;27:192–197. [DOI] [PubMed] [Google Scholar]
- 17.Tiruveedhula M, Reading IC, Clarke NMP. Failed Pavlik harness treatment for DDH as a risk factor for avascular necrosis. J Pediatr Orthop 2015;35:140–143. [DOI] [PubMed] [Google Scholar]
- 18.Hedequist D, Kasser J, Emans J. Use of an abduction brace for developmental dysplasia of the hip after failure of Pavlik harness use. J Pediatr Orthop 2003;23:175–177. [PubMed] [Google Scholar]
- 19.Sankar WN, Nduaguba A, Flynn JM. Ilfeld abduction orthosis is an effective second-line treatment after failure of Pavlik harness for infants with developmental dysplasia of the hip. J Bone Joint Surg [Am] 2015;97:292–297. [DOI] [PubMed] [Google Scholar]
- 20.Grill F, Bensahel H, Canadell J, et al. The Pavlik harness in the treatment of congenital dislocating hip: report on a multicenter study of the European Paediatric Orthopaedic Society. J Pediatr Orthop 1988;8:1–8. [DOI] [PubMed] [Google Scholar]
- 21.Tönnis D. Congenital dysplasia and dislocation of the hip in children and adults. Berlin, Heidelberg: Springer-Verlag, 1987. [Google Scholar]
- 22.Wada I, Sakuma E, Otsuka T, et al. The Pavlik harness in the treatment of developmentally dislocated hips: results of Japanese multicenter studies in 1994 and 2008. J Orthop Sci 2013;18:749–753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Alexiev VA, Harcke HT, Kumar SJ. Residual dysplasia after successful Pavlik harness treatment: early ultrasound predictors. J Pediatr Orthop 2006;26:16–23. [DOI] [PubMed] [Google Scholar]
- 24.Atalar H, Sayli U, Yavuz OY, Uraş I, Dogruel H. Indicators of successful use of the Pavlik harness in infants with developmental dysplasia of the hip. Int Orthop 2007;31:145–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Borowski A, Thawrani D, Grissom L, Littleton AG, Thacker MM. Bilaterally dislocated hips treated with the Pavlik harness are not at a higher risk for failure. J Pediatr Orthop 2009;29:661–665. [DOI] [PubMed] [Google Scholar]
- 26.Cashman JP, Round J, Taylor G, Clarke NMP. The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. J Bone Joint Surg [Br] 2002;84-B:418–425. [DOI] [PubMed] [Google Scholar]
- 27.Choudry Q, Paton RW. Pavlik harness treatment for pathological developmental dysplasia of the hip: meeting the standard? J Pediatr Orthop B 2017;26:293–297. [DOI] [PubMed] [Google Scholar]
- 28.Harding MG, Harcke HT, Bowen JR, Guille JT, Glutting J. Management of dislocated hips with Pavlik harness treatment and ultrasound monitoring. J Pediatr Orthop 1997;17:189–198. [DOI] [PubMed] [Google Scholar]
- 29.Inoue T, Naito M, Nomiyama H. Treatment of developmental dysplasia of the hip with the Pavlik harness: factors for predicting unsuccessful reduction. J Pediatr Orthop B 2001;10:186–191. [PubMed] [Google Scholar]
- 30.Kitoh H, Kawasumi M, Ishiguro N. Predictive factors for unsuccessful treatment of developmental dysplasia of the hip by the Pavlik harness. J Pediatr Orthop 2009;29:552–557. [DOI] [PubMed] [Google Scholar]
- 31.Kokavec M, Makai F, Olos M, Bialik V. Pavlik’s method: a retrospective study. Arch Orthop Trauma Surg 2006;126:73–76. [DOI] [PubMed] [Google Scholar]
- 32.Köse N, Omeroğlu H, Ozyurt B, et al. Our three-year experience with an ultrasonographic hip screening program conducted in infants at 3 to 4 weeks of age. Acta Orthop Traumatol Turc 2006;40:285–290. [PubMed] [Google Scholar]
- 33.Lerman JA, Emans JB, Millis MB, et al. Early failure of Pavlik harness treatment for developmental hip dysplasia: clinical and ultrasound predictors. J Pediatr Orthop 2001;21:348–353. [PubMed] [Google Scholar]
- 34.Malkawi H. Sonographic monitoring of the treatment of developmental disturbances of the hip by the Pavlik harness. J Pediatr Orthop B 1998;7:144–149. [DOI] [PubMed] [Google Scholar]
- 35.Mostert AK, Tulp NJ, Castelein RM. Results of Pavlik harness treatment for neonatal hip dislocation as related to Graf’s sonographic classification. J Pediatr Orthop 2000;20:306–310. [PubMed] [Google Scholar]
- 36.Novais EN, Kestel LA, Carry PM, Meyers ML. Higher Pavlik harness treatment failure is seen in Graf type IV Ortolani-positive hips in males. Clin Orthop Relat Res 2016;474:1847–1854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ömeroğlu H, Köse N, Akceylan A. Success of Pavlik harness treatment decreases in patients ≥ 4 months and in ultrasonographically dislocated hips in developmental dysplasia of the hip. Clin Orthop Relat Res 2016;474:1146–1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Palocaren T, Rogers K, Haumont T, Grissom L, Thacker MM. High failure rate of the Pavlik harness in dislocated hips: is it bilaterality? J Pediatr Orthop 2013;33:530–535. [DOI] [PubMed] [Google Scholar]
- 39.Peled E, Bialik V, Katzman A, Eidelman M, Norman D. Treatment of Graf’s ultrasound class III and IV hips using Pavlik’s method. Clin Orthop Relat Res 2008;466:825–829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Suzuki S, Kashiwagi N, Kasahara Y, Seto Y, Futami T. Avascular necrosis and the Pavlik harness. The incidence of avascular necrosis in three types of congenital dislocation of the hip as classified by ultrasound. J Bone Joint Surg [Br] 1996;78-B:631–635. [PubMed] [Google Scholar]
- 41.Swaroop VT, Mubarak SJ. Difficult-to-treat Ortolani-positive hip: improved success with new treatment protocol. J Pediatr Orthop 2009;29:224–230. [DOI] [PubMed] [Google Scholar]
- 42.Uçar DH, Işiklar ZU, Kandemir U, Tümer Y. Treatment of developmental dysplasia of the hip with Pavlik harness: prospective study in Graf type IIc or more severe hips. J Pediatr Orthop B 2004;13:70–74. [DOI] [PubMed] [Google Scholar]
- 43.Vadillo P, Encinas-Ullan CA, Moraleda L, Albiñana J. Results of the Pavlik harness when treating Ortolani-positive hips: predictors of failure and arthrographic findings. J Child Orthop 2015;9:249–253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.van de Sande MAJ, Melisie F. Successful Pavlik treatment in late-diagnosed developmental dysplasia of the hip. Int Orthop 2012;36:1661–1668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.van der Sluijs JA, De Gier L, Verbeke JI, et al. Prolonged treatment with the Pavlik harness in infants with developmental dysplasia of the hip. J Bone Joint Surg [Br] 2009;91-B:1090–1093. [DOI] [PubMed] [Google Scholar]
- 46.Walton MJ, Isaacson Z, McMillan D, Hawkes R, Atherton WG. The success of management with the Pavlik harness for developmental dysplasia of the hip using a United Kingdom screening programme and ultrasound-guided supervision. J Bone Joint Surg [Br] 2010;92-B:1013–1016. [DOI] [PubMed] [Google Scholar]
- 47.White KK, Sucato DJ, Agrawal S, Browne R. Ultrasonographic findings in hips with a positive Ortolani sign and their relationship to Pavlik harness failure. J Bone Joint Surg [Am] 2010;92-A:113–120. [DOI] [PubMed] [Google Scholar]
- 48.Zajonz D, Strobel S, Wojan M, et al. Pavlik harness for the treatment of congenital hip dysplasia types D III and IV. Orthopade 2016;45:72–80. [DOI] [PubMed] [Google Scholar]
- 49.Pap K, Kiss S, Shisha T, Marton-Szücs G, Szöke G. The incidence of avascular necrosis of the healthy, contralateral femoral head at the end of the use of Pavlik harness in unilateral hip dysplasia. Int Orthop 2006;30:348–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Mubarak S, Garfin S, Vance R, McKinnon B, Sutherland D. Pitfalls in the use of the Pavlik harness for treatment of congenital dysplasia, subluxation, and dislocation of the hip. J Bone Joint Surg [Am] 1981;63-A:1239–1248. [PubMed] [Google Scholar]
- 51.Viere RG, Birch JG, Herring JA, Roach JW, Johnston CE. Use of the Pavlik harness in congenital dislocation of the hip. An analysis of failures of treatment. J Bone Joint Surg [Am] 1990;72-A:238–244. [PubMed] [Google Scholar]
- 52.Borges JL, Kumar SJ, Guille JT. Congenital dislocation of the hip in boys. J Bone Joint Surg [Am] 1995;77-A:975–984. [DOI] [PubMed] [Google Scholar]
- 53.Suzuki S. Ultrasound and the Pavlik harness in CDH. J Bone Joint Surg [Br] 1993;75-B:483–487. [DOI] [PubMed] [Google Scholar]
- 54.Murnaghan ML, Browne RH, Sucato DJ, Birch J. Femoral nerve palsy in Pavlik harness treatment for developmental dysplasia of the hip. J Bone Joint Surg [Am] 2011;93-A:493–499. [DOI] [PubMed] [Google Scholar]
- 55.Gargan KE, Bradley CS, Maxwell A, et al. Education of parents in Pavlik harness application for developmental dysplasia of the hip using a validated simulated learning module. J Child Orthop 2016;10:289–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hassan FA. Compliance of parents with regard to Pavlik harness treatment in developmental dysplasia of the hip. J Pediatr Orthop B 2009;18:111–115. [DOI] [PubMed] [Google Scholar]
- 57.McHale KA, Corbett D. Parental noncompliance with Pavlik harness treatment of infantile hip problems. J Pediatr Orthop 1989;9:649–652. [DOI] [PubMed] [Google Scholar]
- 58.Wilkinson AG, Sherlock DA, Murray GD. The efficacy of the Pavlik harness, the Craig splint and the von Rosen splint in the management of neonatal dysplasia of the hip. A comparative study. J Bone Joint Surg [Br] 2002;84-B:716–719. [DOI] [PubMed] [Google Scholar]
- 59.Ömeroğlu H, Köse N, Akceylan A. Is the use of static abduction brace better than Pavlik harness in the treatment of ultrasonographically stable hips under the age of 6 months? [abstract]. 18th EFORT Congress 2017, Vienna, Austria. [Google Scholar]
- 60.Atar D, Lehman WB, Tenenbaum Y, Grant AD. Pavlik harness versus Frejka splint in treatment of developmental dysplasia of the hip: bicenter study. J Pediatr Orthop 1993;13:311–313. [DOI] [PubMed] [Google Scholar]
- 61.Czubak J, Piontek T, Niciejewski K, et al. Retrospective analysis of the non-surgical treatment of developmental dysplasia of the hip using Pavlik harness and Frejka pillow: comparison of both methods. Ortop Traumatol Rehabil 2004;6:9–13. [PubMed] [Google Scholar]
- 62.Moktar J, Bradley CS, Maxwell A, et al. Skill acquisition and retention following simulation-based training in Pavlik harness application. J Bone Joint Surg [Am] 2016;98:866–870. [DOI] [PMC free article] [PubMed] [Google Scholar]