

Abstract
Objective/Background
The purpose of this pilot study was to examine the effectiveness of standard earmuffs and noise-cancelling (NC) headphones in controlling behavioural problems related to hyper-reactivity to auditory stimuli in children with autism spectrum disorder (ASD).
Methods
Twenty-one children with ASD aged 4–16 years (16 boys and 5 girls), after a 2-week nonwearing baseline period, were asked to use standard earmuffs and NC headphones for 2 weeks, in a random order. Parents or teachers rated participants’ behaviours that were related to their reaction to auditory stimuli.
Results
Four participants refused to wear either the earmuffs or the NC headphones. It was found that the T-score on the Goal Attainment Scaling was significantly higher during the earmuff period than that in the baseline period (Z = 2.726, p = .006). The behaviours of 5 children with ASD improved during the NC headphone period as compared with those in the baseline period; there were no differences in the T-scores on the Goal Attainment Scaling between the NC headphone period and the baseline period (Z = 1.689, p = .091) and between the earmuff and NC headphone periods (Z = −0.451, p = .678).
Conclusion
This study demonstrated the effectiveness of standard earmuffs and NC headphones in helping children with ASD to cope with problem behaviours related to hyperreactivity to auditory stimuli, therefore, children with ASD could use earmuffs to help to deal with unpleasant sensory auditory stimuli.
Keywords: auditory hyperreactivity, autism spectrum disorder, earmuff, noise-cancelling headphone
Introduction
Hyper-reactivity to auditory stimuli is a common problem in children with autistic spectrum disorder (ASD). Bromley, Hare, Davison, and Emerson (2004) reported that 70% of children with ASD exhibit hyper-sensitivity to auditory stimuli. In children with higher functioning ASD, the most common sensory hypersensitivity was auditory hypersensitivity (Futoo et al., 2014). Various sounds provoked unpleasant sensory experiences in children with ASD. Loud and unexpected sounds such as fire alarms, toilet flushes in public restrooms, dogs barking, other children's crying voices, fireworks, loud coughing or clapping, and microphones with acoustic feedback were the most common examples (Dickie, Baranek, Schultz, Watson, & McComish, 2009). In their autobiographies, individuals with ASD often described their experiences of hyper-reactivity to auditory stimuli (Grandin & Scariano, 1994; Hall, 2001).
Children with ASD who have auditory hyper-reactivity (ASD-AH) are bothered by auditory stimuli that they find intolerable, therefore, it is very important to find a way to manage auditory stimuli in daily life. Earmuffs, earplugs, and noise-cancelling headphones (NC headphones) are examples of equipment designed to protect individuals from harmful auditory stimuli. Some authors suggested earmuffs, earplugs, or headphones to parents or practitioners working with children with ASD (Attwood 2008; Delaney 2008; Myles, Tapscott, Miller, Rinner, & Robbins, 2000). Attwood (2008, p. 278) described, “A barrier to reduce the level of auditory stimulation can be used, as silicone earplugs, kept in the person's pocket… These are particularly useful in situations known to be noisy, such as school cafeterias.” Myles et al. (2000) suggested that caregivers should provide headphones or earplugs for the child to wear during testing or seatwork after verbal directives are given. Although some specialists have introduced the use of earmuffs, earplugs, and headphones to parents of children with ASD or with sensory processing disorders, there have been no studies so far demonstrating their effectiveness for managing behavioural and emotional problems related to AH in children with ASD. Earplugs and earmuffs can block environmental auditory stimuli, including human speech (Morris, 2009). Headphones can block some auditory stimuli by providing another auditory stimulus such as music. NC headphones can reduce unwanted ambient sound by using active noise control engineering but cannot cancel human voices and sudden sounds. Different devices protect in different ways and attenuate sound differently. To identify which support equipment is helpful to children with ASD-AH, we need to know which type of device is more effective in improving AH. In this study, we focused on comparing earmuffs and NC headphones to examine which device would be better for blocking all sounds, including human voices, and examining if such equipment might reduce ambient sound using a NC system. We would also like to know which type of hyperreactivity in children with ASD could be controlled by these devices. Although earplugs are also sound-blocking devices, they might cause unwanted tactile stimuli to the ear canal. Therefore, in this study we investigated only two types of ear devices —- earmuffs and NC headphones, as earplugs are sound blocking devices that might cause unwanted tactile stimuli to the ear canal.
The purpose of this study was to examine the effectiveness of earmuffs and NC headphones in controlling behaviours related to hyper-reactivity to auditory stimuli in children with ASD. To the best of our knowledge, this was the first study that examined the effectiveness of these devices in controlling behavioural and emotional problems in children with ASD-AH.
Methods
Participants
Participants were recruited from 220 families who were members of the Autism Society of Nagasaki, Japan, from April 2013 to September 2014. We informed the parents about our plan to hold workshops on sensory problems in children with ASD, then two workshops were run during the study period. In the workshops, after explaining the study methods and inclusion criteria, we invited 65 parents (mothers or fathers) who were present in these workshops to participate in the study with their verbal and written consent. The same procedure was repeated for eight families who were not present at these workshops. Inclusion criteria were: (1) the child was diagnosed with autistic disorder; (2) Asperger's disorder; (3) pervasive developmental disorder not otherwise specified; (4) was aged between 3 years to 17 years; and (5) had hyper-reactivity to auditory stimuli. Parents of 25 children with ASD who met the inclusion criteria (age range 4—16 years, mean age 8 years 2 months ± 36 months; 19 boys and 6 girls) expressed their willingness to participate in this study. All participants had already been diagnosed by paediatricians based on Diagnostic and Statistical Manual of Mental Disorders-IV criteria (American Psychiatric Association, 1994). We asked the parents to report the grade of intelligence disabilities of their children as described in the “Rehabilitation Certificate Handbook for Individuals with Intellectual Disabilities” by the prefectural government (Nagasaki Prefectural Government, 1977).
This study received prior approval from the Human Investigation Committee of the Nagasaki University Graduate School of Biomedical Sciences (Number 08091132).
Equipment
Earmuffs (PELTOR Optime 1 Earmuffs 3M H510A-401-GU, 2016) and NC headphones (SONY Digital Noise Cancelling Headpone MDR-NC500D, 2016) were used. Earmuffs are headphone style devices designed to reduce sound levels. The attenuation rating (noise reduction rating) and weight of the earmuffs (PELTOR H510) were 27 dB and 180 g, respectively. Earmuffs protect children from loud noises that may bother them or even be harmful to their hearing and attenuate not only bothersome environmental sounds but also human speech (Morris, 2009). NC headphones reduce unwanted ambient sounds using active noise control engineering. The noise reduction rating and weight of the NC headphones (Sony MDR-NC500D) were 20 dB and 195 g, respectively. NC headphones primarily work well on low frequency bands, such as motor and air duct noises (Sony Noise Cancelling Headphones, 2012) but do not work well on sounds that continuously change in frequency and amplitude, such as human voices or thunder.
Outcome measure
Goal Attainment Scaling
To evaluate changes in behaviour during the baseline control period, earmuff period, and NC headphone period, Goal Attainment Scaling (GAS) was used. The GAS provides a standardised means to capture the diversity of meaningful functional outcomes (Kiresuk & Sherman, 1968). In various studies, GAS has been determined to be an effective outcome measure and has been used to evaluate the effectiveness of intervention in children with developmental disabilities (Mailloux et al., 2007; Miller, Coll, & Schoen, 2007; Schaaf et al., 2014). Ruble, McGrew, and Toland (2012, p. 1982) demonstrated that the GAS was a valid and reliable method for the measurement of progress on individualized goals for children with ASD, and concluded that the GAS is a “promising ideographic approach for measuring intervention effectiveness.” Palisano (1993) demonstrated the content validity and responsiveness of the GAS, and concluded that the GAS could be recommended for use in clinical practice and treatment outcome research. In the GAS, a specific goal is selected on a composed scale that ranges from least to most favourable outcomes. The GAS has rating scale ranging from −2 to +2; 0 being the anticipated performance by the end of the study intervention (Kiresuk, Smith, & Cardillo, 1994). Negative numbers represent less-than-expected outcomes, and positive numbers represent greater-than-expected outcomes. After carefully reading each child's prior assessment reports, the first author developed the goals together with the parents and teachers to ensure that the goals were relevant and at appropriate levels for the participants. The first author was blinded to the experimental schedule assignment, because the third author was responsible for randomization and was blinded to the assigned schedules. The second author was responsible for a double-check on each GAS item to ensure that it met all quality criteria based on the GAS literature (Turner-Stokes, 2009, p. 363).
The attainment levels for the chosen personal goals were then combined in a single aggregated T-score by applying the recommended formula which accounts for variable numbers of goals, inter-correlation of goal areas, and variable weighting (Kiresuk & Sherman, 1968; Turner-Stokes, 2009):
where wi = weight assigned to the ith goal and xi = the score of the ith goal.
Procedure
Participants were randomly assigned to one of two experimental schedules that consisted of a sequence of a 2-week control period followed by 2 weeks of earmuff use and 2 weeks of NC headphone use, or a sequence of a 2-week control period followed by 2 weeks of NC headphone use and 2 weeks of earmuff use. Randomisation of the experimental schedule was done using the RAND and SORT functions in MS Excel (Microsoft Excel 2013) by the third author. Each participant had to decide whether to use earmuffs or NC headphones for the whole day or part time, however, the parents and teachers had to record the total time of using earmuffs or NC headphones per day.
Because it was necessary to observe the children's behaviour at all time, the children's GAS rating was checked by the teacher at school and by the parent at home.
Statistical analysis
The GAS T-scores for each period were calculated for each participant. The T-scores of all the participants were compared between the control period, the NC headphone period, and the earmuff period. The Shapiro—-Wilk test indicated that the T-scores in the baseline period were not normally distributed (W = 0.826, p = .021), therefore, we used the Wilcoxon rank sum test, which is used for nonparametric comparisons. If there were missing values due to participants refusing to wear earmuffs or NC headphones or not encountering disliked auditory stimuli during the assessment period, the data were excluded from the analysis.
Sample size calculations were performed using the G-Power software version 3.1 (G*Power: Universität Dusseldorf, Düsseldorf, Germany; 2010—2016) with “a priori calculation” that is an analysis method to calculate sufficient sample sizes to achieve adequate power prior to the research study. For this calculation, an alpha value of 0.05, an effect size of 1, and a power of 80% were set, which identified that 11 participants were sufficient to detect a significant change in the GAS T-score.
Results
Medians and quartiles of the GAS scores in each period are presented in Figure 1.
Figure 1.
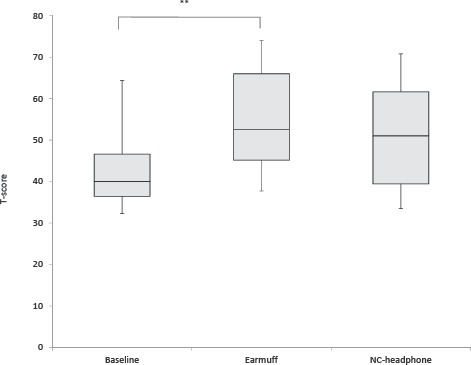
Medians and quartiles of T-scores on the Goal Attainment Scaling in each period. The Wilcoxon rank sum test revealed significant differences between the control period, earmuff period, and noise-cancelling (NC) headphone period. **: p < 0.01.
Four participants (3 boys and 1 girl) refused to wear either the earmuffs or NC headphones. Their mothers reported that their children disliked the tactile impression or pressure. No children wore earmuffs or NC headphones continuously during waking hours. Among the participants who used the earmuffs and NC headphones, the use time per day ranged from 65 minutes to 360 minutes (mean = 136.9 minutes, standard deviation = 69.4 minutes) for earmuffs and from 30 minutes to 360 minutes (mean = 94.6 minutes, standard deviation = 50.6 minutes) for NC headphones according to the parents' and teachers' reports. Three participants (Cases A, K, and M) used them at school only. Five participants (Cases C, F, H, I, and J) used them at home only. Other participants used them both at home and at school.
Table 1 shows the age and sex of each participant, the auditory stimuli that induce behaviour problems, and problem behaviours induced by auditory stimuli in each child, excluding participants who had refused to wear either earmuffs or NC headphones. One to four goals were prepared for each child.
Table 1.
Participant Characteristics, Auditory Stimuli that Induced Behavioural problems, Behaviour after sounds, and Goal Attainment Scaling (GAS) Scores.
| Participants | Sex | Age (y) | Intelligence | Auditory stimuli that induce behaviour problems | Behaviours after sounds | GAS scores |
||
|---|---|---|---|---|---|---|---|---|
| 1st period |
2nd period |
3rd period |
||||||
| Control period | Use of earmuff or NC headphones | |||||||
| Case A | Female | 13 | Normal | Many voices of other students | The child becomes nervous and aggressive | -1 | -1 | 0 |
| Loud music | The child becomes nervous and aggressive | 2 | 2 | 1 | ||||
| Grinding sound of sharpening a pencil | The child becomes nervous and aggressive | 2 | 0 | 0 | ||||
| Case B | Male | 11 | Normal | High-pitched voices of girls | The child covers his ears with his hands | -1 | -1 | 0 |
| Sounds from a television | The child covers his ears with his hands | -1 | 1 | 1 | ||||
| Sounds of construction work | The child covers his ears with his hands | -1 | 1 | 1 | ||||
| Sound of an electric sharpener | The child covers his ears with his hands | -1 | -1 | -1 | ||||
| Case C | Male | 8 | Severe | Sound of a motorcycle engine | The child covers his ears with his hands | 0 | 1 | 2 |
| Sounds of sirens | The child squats, groans, and covers his ears with his hands | 2 | 2 | 2 | ||||
| Names of certain persons | The child hates hearing the name of a certain person. He cries and runs away | 1 | 1 | 1 | ||||
| Sound of the engine of big trucks | The child covers his ears with his hands | 1 | 2 | 2 | ||||
| Case D | Male | 7 | Severe | Sound of a chime | The child flurries, bites his fingers, and talks furiously | -1 | 2 | 2 |
| Sounds of thunder, rain, and storm | The child flurries and runs around. | -1 | 1 | 2 | ||||
| He becomes pessimistic. | ||||||||
| Singing voice of another person | The child flutters and disturbs | 1 | 1 | 1 | ||||
| Sound of a siren | The child withdraws to his room | -1 | 1 | - | ||||
| Case E | Male | 7 | Normal | Sounds of construction machines | The child covers his ears with his hands | 1 | 0 | |
| Sounds of dental treatment machines | The child covers his ears with his hands | -1 | - | - | ||||
| Sound of dance music used during physical education and musical instruments | The child covers his ears with his hands | 0 | 1 | |||||
| Barking of dogs | The child covers his ears with his hands | 0 | - | -1 | ||||
| Case F | Male | 4 | Mild | High-pitched voices of children | The child complains by yelling | -1 | 2 | -2 |
| Loud conversation voices | The child says, “Shut up!” | -1 | 1 | - | ||||
| Case G | Female | 4 | Normal | Sounds of an engine, slamming doors, construction work, high-pitched metallic sounds, drums, cymbals, fireworks, whistles, and a child's screaming | The child covers her ears with her hands, cries, or stands motionlessly | -1 | 1 | 0 |
| Case H | Male | 9 | Normal | Noise of a crowd | The child lingers close to his mother or becomes absentminded | -1 | 0 | -1 |
| Children's voices outside his house | The child stops the ongoing activity and hides | -1 | 1 | -1 | ||||
| Father's voice | The child screams in order to deaden his father's voice. If the father does not stop talking, the child has a & of rage | -1 | 2 | -1 | ||||
| Sound of the toilet flush | The child avoids using the toilet or hits family members who flush the toilet | -1 | 1 | |||||
| Case I | Female | 11 | Normal | Sound of a spray | The child expresses disgust or irritation | -2 | 1 | -1 |
| Sounds of scratching, writing on, and erasing the blackboard | The child's face becomes tense | -1 | 1 | -1 | ||||
| Classroom noise | The child's face shows displeasure | -1 | 0 | -1 | ||||
| Sounds of a drum, starter pistol, or cracker | The child covers her ears with her hands | -1 | 0 | -1 | ||||
| Sounds of motorcycles | The child covers her ears with her hands | -1 | 0 | -1 | ||||
| Case J | Male | 7 | Most severe | Sound of a baby crying | The child runs away shouting “Ah!” Sometimes, he hits people around him | -1 | - | - |
| Noisy crowded place (such as a hotel lobby) | The child cries and runs around | -1 | -1 | |||||
| Scolding with a loud voice | The child looks like he is angry, anxious, or is going to cry. Sometimes, he throws objects | -1 | -1 | |||||
| Crowing of a cock | The child runs away shouting “Ah!” | -1 | —- | —- | ||||
| Case K | Male | 4 | Mild | Sounds of a starter pistol or fireworks (also in a movie or story) | The child screams and has a & of rage | —-1 | -1 | -1 |
| Case L | Male | 15 | Normal | Sound effects before presenting an answer in a television quiz program | The child covers his ears with his hands and moves away from the television | —-1 | Refusal | 0 |
| Just before a character was scolded by his/her parent in an animation program | The child covers his ears with his hands and changes the channel | -1 | Refusal | |||||
| Commercial music in the department store or supermarket | The child covers his ears with his hands or says unrelated things (to himself) | —-1 | Refusal | 0 | ||||
| Case M | Male | 8 | Severe | Older sister's screaming | The child cries and runs away covering his ears. The child bites or hits his older sister | —-1 | -1 | Discontinuation |
| Loud sound in the large hall | The child covers his ears with his hands and freezes or runs away | -1 | 0 | |||||
| Music or sound of a jet towel | The child cannot enter the bathroom or leaves from there | -1 | ||||||
| Case N | Male | 7 | Most severe | Sneeze | After crying, the child becomes aggressive | 0 | -1 | Discontinuation |
| Sound of a motorcycle engine | The child cries and rolls around on the floor | 2 | ||||||
| Sound of sniffling | The child becomes aggressive and hits those around him | 2 | ||||||
| Noise in an assembly hall | The child cries and angrily wishes to leave the hall | 2 | 0 | |||||
| Sound of a baby crying | The child grabs anyone standing nearby | —- | -2 | |||||
| Music with a quick tempo | The child growls | —- | -1 | |||||
| Case 0 | Male | 8 | Normal | Other children's voice in the classroom | The child covers his ears with his hands | 0 | -1 | Discontinuation |
| Sound of alarm bell | The child covers his ears with his hands or leaves the place | — | — | |||||
| Case P | Male | 8 | Normal | Sound of thunder | The child shudders, covers his ears with his hands, and clings to the teacher | — | — | Discontinuation |
| Loud voice when child was directed or scolded | The child hits his own face | 1 | 1 | |||||
| White noise on the television screen | The child freezes | -1 | 0 | |||||
| Sound occurring suddenly | The child freezes after being startled | -1 | — | |||||
| Case Q | Male | 8 | Normal | Other children's voice in the classroom | The child covers his ears with his hands | 0 | 2 | Discontinuation |
| Sound of alarm bell | The child covers his ears with his hands or leaves the place | -1 | 2 | |||||
Note. The bold numbers shows the GAS score during the use of an NC headphone. The italic numbers shows the GAS score during earmuff use. —: No opportunity.
One child refused to wear earmuffs because he disliked the pressure they exerted. Five children refused or discontinued to wear NC headphones because they could hear human voices better and disliked other students' voices. As a result, we compared the T-scores between the baseline control and earmuff use period in 16 children with ASD, and between the baseline control and NC headphone period in 12 children with ASD.
Fifty-six behaviours induced by auditory stimuli were evaluated using the GAS. Since most of the participants exhibited some problem behaviours induced by auditory stimuli, the GAS T-score for each participant was calculated from the GAS scores in each period.
The GAS T-score was significantly higher for the earmuff period than that for the control period (Z = 2.726, p = .006). There were no significant differences in the GAS T-scores between the NC headphone period and the control period (Z = 1.689, p = .091) and between the earmuff period and NC headphone period (Z = −0.451, p = .678). Although there were no significant differences between the NC headphone period and control period, the GAS T-scores of five children improved during the NC headphone period.
Parents of participants whose GAS T-scores during the NC headphone period were better than those during the earmuff period reported the following: “He was pleased by the diminished sound of the piano,” “He could tolerate noise from the big trucks,” “He disliked the pressure of the earmuffs, but he tolerated the NC headphones.” Parents of participants whose GAS T-scores were better during the earmuff period than those during the NC headphone period reported the following: “If he wore earmuffs, he could enter the bathroom” (this participant disliked the sound of water flushing), “He could tolerate the noise of the air towel,” “He may have felt stressed when he wore the NC headphones because he could hear human voices clearly when the other noises diminished.”
Discussion
Development of treatment or support for individuals with ASD-AH is an important issue; however, evidence supporting therapies such as auditory integration therapy and sound therapy for children with ASD has not been reported (Sinha, Silove, Hayen, & Williams, 2011).
Special education directors reported that occupational therapists provide relatively more service in assistive technology consultation (30.3%) and task or environment modification (25.8%) to improve student performance (Spencer, Emery, & Schneck, 2003). Spencer, Turkett, Vaughan, and Koenig (2006) also stated that occupational therapy intervention focused on changing or adapting the performance environment was perceived to be helpful. Although these opinions were not solely about occupational therapy for ASD, they indicated that occupational therapists should work on modifying learning environments and provide assistive technology to enable better performance in children with ASD, especially for those with ASD-AH. Providing earmuffs and NC headphones, for example, are possible ways to support children with ASD-AH through occupational therapy.
To adapt earmuffs and NC headphones for use in children with ASD-AH, treatment evidence is necessary. To date, a few researchers have reported the benefits of earmuffs and earplugs for children with central auditory processing disorders who have difficulty concentrating and processing auditory input in busy environments (Hasbrouck, 1980; Willford & Burleigh, 1985). However, the effectiveness of these devices for children with ASD-AH has not been demonstrated.
Our results showed improvement of GAS T-scores during earmuff use, therefore, earmuffs can have a positive effect for coping with behavioural problems related to hyperreactivity to auditory sensory stimuli in children with ASD. Since earmuffs reduce auditory stimuli from the environment, they might reduce the stress or anxiety caused by auditory stimuli. Kinnealey et al. (2012) demonstrated that sound-absorbing walls and halogen lighting can benefit students with sensory hyper-sensitivity and improve their attention and engagement in the classroom. Although the control methods were different between the sound-absorbing walls in their study and the earmuffs in our study, both strategies might be effective in helping children with ASD-AH because both could diminish intolerable sounds. Since earmuffs might be effective equipment for children with ASD-AH and could be used in various situations, practitioners, including occupational therapists, could recommend earmuffs to individuals with ASD-AH and their parents. Morris (2009) pointed out that because sound isolators such as earmuffs have fairly nonspecific broadband sound-attenuating characteristics, bothersome environmental sounds are attenuated, but so are the speech sounds, which are very important to the individual. Therefore, practitioners should also consider this disadvantage of sound reduction equipment.
Although an improvement in the GAS T-scores was observed in some participants, there was no effect of NC headphones on behavioural problems related with hyperreactivity to auditory sensory stimuli. The parents of participants whose GAS T-scores during the earmuff period were better than those during the NC headphone period suggested that earmuffs improved hyper-reactivity behaviour to air towels and flushing water. One mother complained that her child felt stressed when he wore NC headphones because he could hear human voices clearly when other noises diminished. Since NC headphones cannot eliminate auditory stimuli except for low frequency noises, human voices and some other sounds might not be reduced. Therefore, NC headphones may not be effective for participants who have auditory sensitivity to human voices. Interestingly, our study found that behaviours of five children with ASD (Cases C, D, E, G, and I) improved during the NC headphone period as compared with those in the baseline control period, and that the intolerable sounds related with the behaviours of these five participants were not voices but were “noisy sounds in the classroom.” Thus, NC headphones might not be effective in coping with behavioural problems caused by human voices. Occupational therapists should consider the specific sounds related to hyper-reactivity when recommending earmuffs or NC headphones to individuals with ASD who exhibit hyperreactivity to auditory stimuli.
This study has some limitations. One of them is the small number of participants. Since four participants refused to wear either earmuffs or NC headphones, and another five refused NC headphones, the behavioural data from the NC headphone period were limited. Further study should be conducted with larger samples. Additionally, we did not examine adverse and long-term effects of earmuff and NC headphone use. Habitual use of sound isolators may actually exacerbate sound sensitivity over time, as suggested in tinnitus patients (Jastreboff & Hazell, 2008). Therefore, we should further examine the benefits and disadvantages of prolonged use of earmuffs and NC headphones in children with ASD. Furthermore, age, sex, general intelligence, functional level of participants, frequency of intervention, and duration of using the devices were not controlled. These factors should be considered in future randomised, controlled studies when comparing the effectiveness between different devices using intervention and control groups. We did not investigate other sound isolation devices such as earplugs or headphones without a NC system, therefore, further study should be conducted to examine the effects of other sound isolation devices.
Conclusion
This was a pilot study, and although there were some limitations in this study, the usefulness of earmuffs for children with ASD-AH, even for such a short period of wearing time, was demonstrated. Although the effectiveness of NC headphones was not statistically significant, we concluded that earmuffs that block sound might be useful for children with ASD-AH, and that NC headphones, which reduce ambient sounds, might also be useful for children with ASD-AH who are not affected by human voices.
Funding/Support:
This study was supported by a grant-in-aid for Scientific Research (C) no. 21500473 from the Japan Society for the Promotion of Science.
Conflicts of interest:
All contributing authors declare that they have no conflicts of interest.
References
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association. [Google Scholar]
- Attwood T.. (2008). The complete guide to Asperger's syndrome. London, UK and Philadelphia: Jessica Kingsley Publishers. [Google Scholar]
- Bromley J., Hare D. J., Davison K., & Emerson E.. (2004). Mothers supporting children with autistic spectrum disorders. Autism, 8, 409–423. [DOI] [PubMed] [Google Scholar]
- Delaney T.. (2008). The sensory processing disorder answer book. Naperville: Sourcebook Inc. [Google Scholar]
- Dickie V. A., Baranek G. T., Schultz B., Watson L. R., & McComish C. S.. (2009). Parent reports of sensory experiences of preschool children with and without autism: a qualitative study. American Journal of Occupational Therapy, 63, 172–181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Futoo E., Miyawaki D., Goto A., Okada Y., Asada N., Iwakura Y. et al. (2014). Sensory hypersensitivity in children with high-functioning pervasive developmental disorder. Osaka City Medical Journal Osaka City University, 60, 63–71. [PubMed] [Google Scholar]
- Grandin T., & Scariano M. M.. (1994). Emergence labelled autistic. New York: Grand Central Publishing. [Google Scholar]
- G* Power: Universität Düsseldorf. (2010. –2016). http://www.gpower.hhu.de/.
- Hall K.. (2001). Asperger Syndrome, the Universe and Everything. London: Jessica Kingsley Publishers. [Google Scholar]
- Hasbrouck J. M.. (1980). Performance of students with auditory figure-ground disorders under conditions of unilateral and bilateral ear occlusion. Journal of Learning Disabilities, 13, 548–551. [PubMed] [Google Scholar]
- Jastreboff P. J., & Hazell J. W. P.. (2008). Tinnitus Retraining Therapy: Implementing the Neurophysiological Model. Cambridge, MA: Cambridge University Press. [Google Scholar]
- Kinnealey M., Pfeiffer B., Miller J., Roan C., Shoener R., & Ellner M. L.. (2012). Effect of classroom modification on attention and engagement of students with autism or dyspraxia. American Journal of Occupational Therapy, 66, 511–519. [DOI] [PubMed] [Google Scholar]
- Kiresuk T. J., & Sherman R. E.. (1968). Goal attainment scaling: A general method for evaluating community mental health programs. Community Mental Health Journal, 4, 443–453. [DOI] [PubMed] [Google Scholar]
- Kiresuk T. J., Smith A., & Cardillo J. E.. (1994). Goal Attainment Scaling: applications, theory and measurement. Hillsdale: Erlbaum. [Google Scholar]
- Mailloux Z., May-Benson T. A., Summers C. A., Miller L. J., Brett-Green B., Burke J. P. et al. (2007). Goal attainment scaling as a measure of meaningful outcomes for children with sensory integration disorders. American Journal of Occupational Therapy, 61, 254–259. [DOI] [PubMed] [Google Scholar]
- Miller L. J., Coll J. R., & Schoen S. A.. (2007). A randomised controlled pilot study of the effectiveness of occupational therapy for children with sensory modulation disorder. American Journal of Occupational Therapy, 61, 228–238. [DOI] [PubMed] [Google Scholar]
- Morris R.. (2009). Managing sound sensitivity in autism spectrum disorder: New technologies for customized intervention. Cambridge: Massachusetts Institute of Technology. [Google Scholar]
- Myles B. S., Tapscott K., Miller N. E., Rinner L., & Robbins L. A.. (2000). Asperger syndrome and sensory issues. Shawnee Mission: Autism Asperger Publishing Co. [Google Scholar]
- Nagasaki Prefectural Government. (1977). Rehabilitation certificate handbook for individuals with intellectual disabilities. Nagasaki: Nagasaki Prefectural Government. [Google Scholar]
- Palisano R. J.. (1993). Validity of goal attainment scaling in infants with motor delays. Physical Therapy Journal, 73, 651–658. [DOI] [PubMed] [Google Scholar]
- PELTOR H510. (2016). http://solutions.3m.com/wps/portal/3M/en_EU/PPE_SafetySolutions_EU/Safety/Product_Catalogue/∼/3M-PELTOR-Optime-l-Ear-Muffs-Headband-27-dB-Yellow-H510A-401-GU?N=5023508+3294471230+3294857473art=rud. Retrieved May 15, 2016.
- Ruble L., McGrew J. H., & Toland M. D.. (2012). Goal attainment scaling as an outcome measure in randomized controlled trials of psychosocial interventions in autism. Journal of Autism and Developmental Disorders, 42, 1974–1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaaf R. C., Benevides T., Mailloux Z., Faller P., Hunt J., van Hooydonk E. et al. (2014). An intervention for sensory difficulties in children with autism: a randomised trial. Journal of Autism and Developmental Disorders, 44, 1493–1506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sinha Y., Silove N., Hayen A., & Williams K.. (2011). Auditory integration training and other sound therapies for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews, 7, CD003681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sony MDR-NC500D. (2016). https://www.sony.co.uk/support/en/product/MDR-NC500D. Retrieved May 15, 2016.
- Sony Noise Cancelling Headphones. (2012). https://docs.sony.com/release/MDR1RNC_EN_FR_ES.pdf. Retrieved May 15, 2016.
- Spencer J. E., Emery L. J., & Schneck C. M.. (2003). Occupational therapy in transitioning adolescents to postsecondary activities. American Journal of Occupational Therapy, 57, 435–441. [DOI] [PubMed] [Google Scholar]
- Spencer K. C., Turkett A., Vaughan R., & Koenig S.. (2006). School-based practice patterns: a survey of occupational therapists in Colorado. American Journal of Occupational Therapy, 60, 81–91. [DOI] [PubMed] [Google Scholar]
- Turner-Stokes L.. (2009). Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clinical Rehabilitation, 23, 362–370. [DOI] [PubMed] [Google Scholar]
- Willeford J., & Burleigh J.. (1985). Handbook of central auditory processing disorders in children. New York: Grune and Stratton. [Google Scholar]