

Abstract
Risberg, MA, Steffen, K, Nilstad, A, Myklebust, G, Kristianslund, E, Moltubakk, MM, and Krosshaug, T. Normative quadriceps and hamstring muscle strength values for female, healthy, elite handball and football players. J Strength Cond Res 32(8): 2314–2323, 2018—This study presents normative values for isokinetic knee extension and flexion muscle strength tests in 350 elite, female, handball (n = 150) and football (n = 200) players. Isokinetic concentric muscle strength tests at 60°·sec−1 were recorded bilaterally using a dynamometer. Peak torque (in Newton meter [N·m]), body mass normalized peak torque (N·m·kg−1), and hamstring to quadriceps ratio (H:Q ratio) for dominant and nondominant legs were recorded. The female elite players were 20.9 ± 4.0 years, started playing at the elite level at the age of 18.2 ± 2.7 years, with a mean of 9.7 ± 2.2 hours of weekly in-season training. Handball players demonstrated greater quadriceps muscle strength compared with football players (11.0%) (p < 0.001), also when normalized to body mass (4.1%) (p = 0.012), but not for weight-adjusted hamstring muscle strength. The H:Q ratio was higher on the dominant compared with the nondominant leg for handball players only (p = 0.012).The H:Q ratio was significantly lower for handball players (0.58) compared with football players (0.60) (p < 0.02). These normative values for isokinetic knee extension and flexion torques of healthy, elite, female handball and football players can be used to set rehabilitation goals for muscle strength after injury and enable comparison with uninjured legs. Significantly greater quadriceps muscle strength was found for handball players compared with football players, also when normalized to body mass.
Key Words: isokinetic muscle strength, normative values, athletes, reference values
Introduction
Normative muscle strength data for defined populations of athletes are of importance to sport coaches, athletic trainer, medicine physicians, physical therapists, and others who are responsible for athletes' health and specifically for return-to-play criteria (29,42). Establishing reference values for muscle strength for athletes in specific sports, by age and gender allow comparison of an individual's values to his peers. Normative values may also provide a better understanding of normal variation within sport and gender.
Quadriceps and hamstring muscle strength of an athlete is an important part of the athlete's functional capacity and contribute significantly to lower limb biomechanics and performance (2,19,32). Regaining quadriceps and hamstring muscle strength are significant rehabilitation goals after lower extremity musculoskeletal injuries and commonly used as outcome measures (18,30). Isokinetic muscle strength tests have been used for decades and are the most commonly used measures to assess quadriceps and hamstring muscle strength both in the athletic and in the nonathletic populations (8,24). There are several studies on normative data from nonathletic populations (8,28), but normative muscle strength data for female athletes within different sports are lacking. Acute lower extremity injuries are most commonly observed in pivoting sports, with a significantly increased risk of knee injuries in female athletes compared with male athletes (27,37). It has been consistently reported that young, adult, female athletes display differences in lower limb neuromuscular control and associated biomechanics, as well as quadriceps and hamstrings muscle strength compared with their age- and activity-matched male peers, thus putting them at an increased risk of lower limb musculoskeletal injury (10,37). Hence, establishing normal values for muscle strength for athletes in specific sports, by age and sex, is important.
Muscle strength deficits, such as between-leg asymmetries and imbalances between hamstring and quadriceps muscle strength (H-Q ratio), have shown to be important for determining readiness to return to sport (2,16,32). The common approach is to use the uninjured leg as a control leg for assessing quadriceps and hamstring muscle strength, but the contralateral leg has also shown to be affected after an injury (5,20). Quadriceps and hamstring muscle strength in the contralateral uninjured leg of anterior cruciate ligament (ACL)-injured subjects have shown to be significantly impaired compared with healthy subjects with same activity level, gender, and body mass index (BMI) (5). Using the uninjured leg as control leg for muscle strength after ACL injuries may give false comparison measures (41). More recent studies have shown that the muscle strength of the contralateral leg is not restored after ACL reconstruction (5). Some has even stated that the increased risk to the contralateral uninjured knee after ACL reconstruction may result from deconditioning of the contralateral knee during recovery (43). Furthermore, athletes commonly have bilateral injuries, precluding the use of the contralateral leg as a control leg for comparison of muscle strength. Hence, establishing normative muscle strength values for comparison when making decisions regarding the athletes' muscle strength and readiness for return to sport are needed. Only 1 large scaled study on normative quadriceps and hamstring muscle strength in elite female athletes exist (N = 144), but it is 20 years old (26). To our knowledge, there are no studies on normative data in female football (soccer) players during the past 15 years, except for one including less than 20 subjects (1).
Hence, the objectives of this study were (a) to establish normative quadriceps and hamstring muscle strength values in female, healthy, elite handball and football players, (b) to compare quadriceps and hamstring muscle strength between handball and football players, (c) to examine differences in quadriceps and hamstring muscle strength between dominant (D) and nondominant (ND) legs, and (d) to compare our normative isokinetic knee extension and flexion values to other previously published studies on female athletes and nonathletic populations within the same age groups.
Methods
Experimental Approach to the Problem
The study is based on data from a prospective cohort study of elite, healthy, female handball and football players with the aim of identifying risk factors for ACL injury (22,38).
Subjects
To be included in this present study on normative muscle strength data, players had to be able to fully participate in team training sessions and match play, and players who had been injured during the past 6 months were excluded (all injuries). Players with previous ACL injury (at any time) were excluded (Figure 1). New teams and players advancing to the premier league were invited for preseason screening. Players who were expected to play in the premier league from the 2007 handball season and the 2009 football season until 2012 were eligible for participation. In total, 412 players were included in this study (Figure 1). A comprehensive set of screening tests was conducted at our institution during preseason for the prospective cohort: February through March for football players and June through August for handball players. The current study include the isokinetic concentric muscle strength tests, previously published studies have reported data on vertical jump test (22), balance test (38), and sidestep cutting technique (21).
Figure 1.
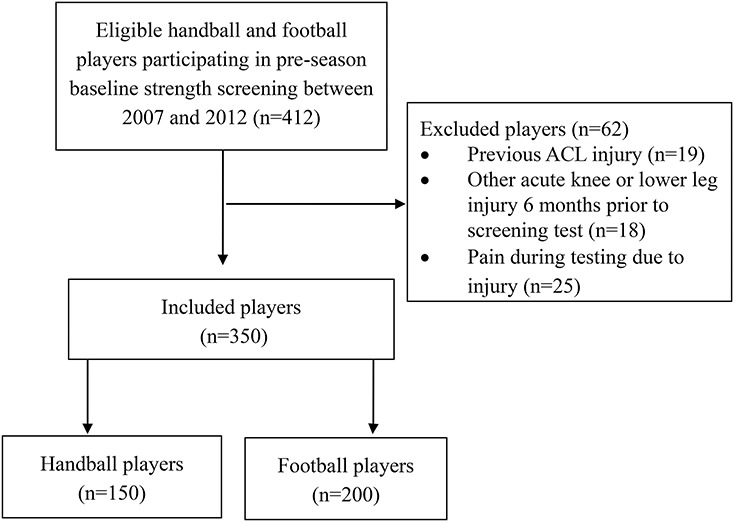
Flow chart of the eligible and included female, healthy, elite, handball and football players.
The study was approved by the Regional Committee for Medical Research Ethics at the Norwegian School of Sport Sciences. All players signed an approved informed written consent form to confirm participation in the study. For players under the age of 18 years, written consent was obtained from their parents to be eligible for participation (n = 35). Subjects under 18 years old also provided written consent.
A literature search in PubMed was conducted to find other studies on normative data on quadriceps and hamstring muscle strength performed on similar age group and BMI, female athletic or nonathletic populations. The following key words were included in the search: isokinetic[Text Word] AND strength[Text Word] AND knee[Text Word] AND normative[Text Word] AND female[Text Word]. Only studies that reported both isokinetic muscle knee extension and flexion tests at 60°·sec−1 on similar age groups to our.
Procedures
Isokinetic concentric knee extension and flexion muscle strength measurements were conducted using a Technogym REV 9000 dynamometer (Gambettola, Italy). We used a standardized test protocol and recorded concentric knee extension and flexion torques Newton meter (N·m) and joint angles with a 109-Hz sampling frequency (6,8,9,17). The range of motion (ROM) was set from 90 to 15° of knee flexion, and the angular velocity during the testing was 60°·sec−1. Torque values of the isokinetic curve between 15 and 0° of knee extension was not included because previous studies have shown that torque production toward the outer positions of the isokinetic curve must be interpreted with caution (23). All participants were tested on the same isokinetic muscle strength test machine (Technogym REV 9000 dynamometer). Isokinetic muscle strength testing at 60°·sec−1 is frequently referred to as a valid measurement for quadriceps muscle performance in ACL-injured individuals and in healthy individuals (34). The reliability of isokinetic muscle strength tests for both ACL-injured and for healthy individuals have proven high with intraclass correlation coefficients, between 0.81 and 0.97 (11, 36). During a 5-minute warm-up with moderate load on a stationary bike, the players were thoroughly informed about the test procedures. Before being positioned in the isokinetic strength testing device, the knee joint centers were defined. Next, the dynamometer's seat and back support were individually adjusted to each player. Two belts were used for fixation of the pelvis and the upper body. The player was instructed to sit in an upright position with both arms crossed in front of their chest and with the contralateral leg in a free and unloaded position. The isokinetic knee extension and flexion protocol consisted of 3 sets of 3 repetitions. In the first set, the player became familiar with the test procedure. The suggested effort level was 30–50% of their maximum, followed by a resting period of 20–30 seconds. In the second set, the effort increased up to 80% of their maximum. After 30 seconds of rest, a final set of 3 repetitions with maximal knee extension and flexion effort was conducted. Standardized verbal encouragements were provided during testing. The procedure was repeated for the contralateral leg. We furthermore asked the players for their D leg, defined as the preferred leg for kicking a ball (8,33).
Statistical Analyses
Torque and angle signals were postprocessed in MatLab (The MathWorks, Natick, MA, USA). Signals were filtered using second-order Butterworth filters with a cutoff frequency of 10 Hz. We extracted the torques for the repetition with the greatest peak torque (could be different for the flexion and extension repetition) and calculated the group average and standard deviation for each 5 degree between 90 and 15° of knee flexion. The H:Q ratio was calculated as (hamstring strength [N·m]/quadriceps strength [N·m]) × 100.
Statistical analyses were performed on SPSS version 18 (SPSS, Inc., Chicago, IL, USA). Descriptive results are presented as mean values, SDs, and confidence intervals. Student's paired t-test was used to analyze differences between D and ND legs, and Student's independent t-test was used to analyze differences between sports.
The Number Cruncher Statistical System, version 10.0.3 (NCSS 10 Statistical Software 2015, NCSS, LLC, Kaysville, UT, USA), was used to calculate differences between our knee torque data and data from previously published studies. Two sample t-test was used based on mean, SD, and sample size of our study compared with previously published studies. Significance level was set to p < 0.05 for all analyses.
Results
Of the 412 eligible players in this study, 62 players were excluded because of the following reasons: (a) previous ACL injury (n = 19) or other previous lower extremity acute injuries (including fractures) during the past 6 months (n = 18) and (b) pain during screening tests because of lower extremity injury (n = 25). Three-hundred fifty, female, elite handball (n = 150) and football (n = 200) players were included (Figure 1) with a mean age of 20.9 ± 4.0 years, BMI of 23.1 ± 2.3, and reported training on average 9.7 ± 2.2 hours per week inseason (Table 1). We had complete data for all 350 handball and football players, except for 11 players with missing information on D leg (n = 7 for handball players and n = 4 for football players).
Table 1.
Mean and SD for female elite handball and football players and mean difference between sports with 95% confidence interval (CI).*

There were no significant differences between handball and football players with regard to age, BMI, or years of elite play, but handball players were significantly taller, had higher body mass, and were older when they started elite play compared with football players (Table 1). Handball players reported significantly more inseason training hours but less offseason training hours compared with football players (Table 1).
Isokinetic peak torques (N·m) and peak torques normalized to body mass (N·m·kg−1) for handball and football players are given in Table 2. Figures 2–5 demonstrate normative knee extension and flexion torques from 90 to 15° of knee flexion. Handball players demonstrated greater quadriceps muscle strength compared with football players (p < 0.0001) when normalized to body mass (p = 0.017) (Table 2). But no significant between-sport differences were found for hamstrings muscle strength when normalized to body mass (Table 2). Hence, handball players revealed lower H:Q ratio compared with the football players (Table 2; p = 0.022). Figures 2 and 3 visualize the differences in knee extension and flexion torques between handball and football players through the whole ROM from 90 to 15° of knee flexion. In contrast, when normalized to body mass (N·m·kg−1), these differences were not as noticeable (Figures 4 and 5). The H:Q ratio was lower for D leg for handball players (57.8) compared with that of D leg for football players (59.6) (p = 0.02) (Table 2).
Table 2.
Mean and SD for peak knee extension and flexion torques (in Newton meter [N·m]), normalized peak extension and flexion torques (N·m·kg−1), and H:Q ratio* for female, elite, handball and football players, presented as mean differences (95% confidence interval, CI) between dominant (D) and nondominant (ND) legs, and between sports.

Figure 2.
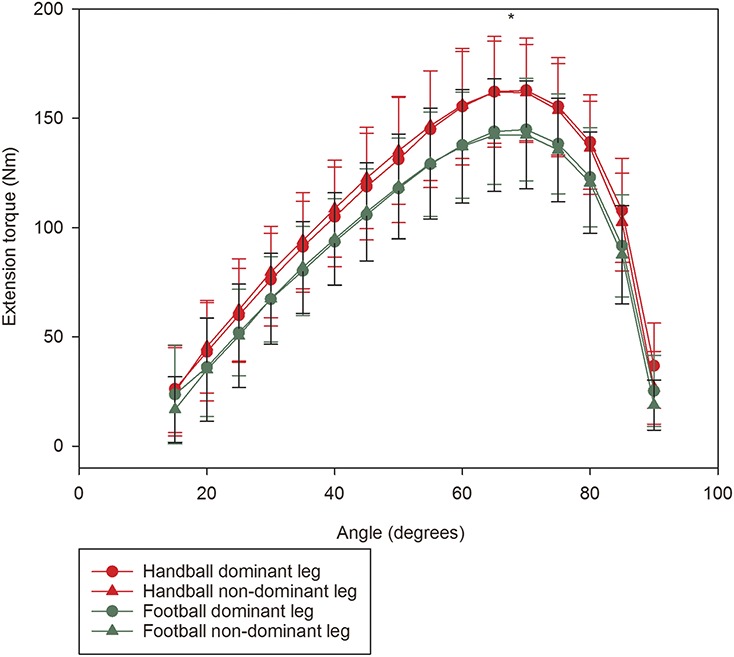
Mean and standard deviation for extension torque at 600/sec (Nm) from 15 to 90 degrees of knee flexion for handball (red) (n=143) and football players (green) (n=196), dominant and non-dominant legs. A symbol (*) is given at peak torque for significant differences between sports (see Table 2 for peak torque values).
Figure 5.
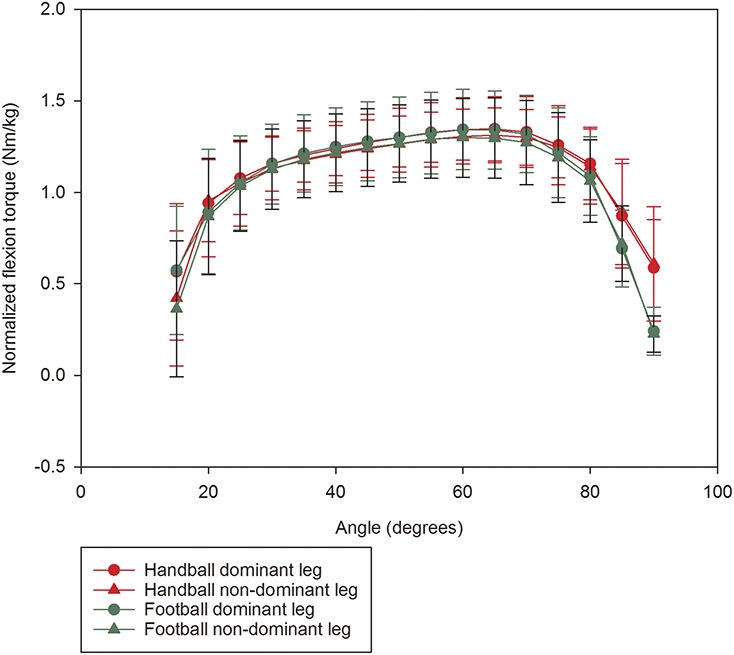
Mean and standard deviation for flexion torque at 600/sec normalized to body weight (Nm/kg) from 15 to 90 degrees of knee flexion for handball (red) (n=143) and football players (green)(n=196), dominant and non-dominant legs.
Figure 3.

Mean and standard deviations for flexion torque at 600/sec (Nm) from 15 to 90 degrees of knee flexion for handball (red) (n=143) and football players (green) (n=196), dominant and non-dominant legs. A symbol (*) is given at peak torque for significant differences between sports (see Table 2 for peak torque values).
Figure 4.
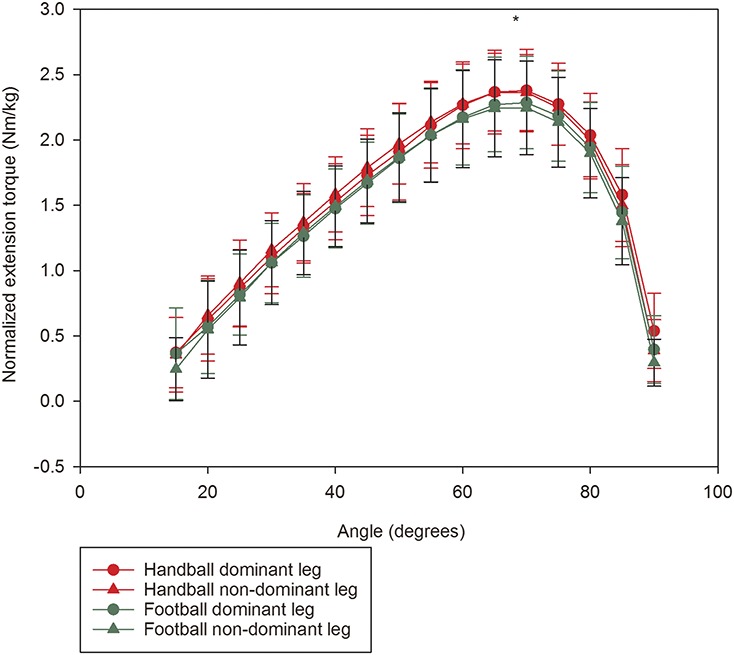
Mean and standard deviation for extension torque at 600/sec normalized to body weight (Nm/kg) from 15 to 90 degrees of knee flexion for handball (red) (n=143) and football players (green) (n=196), dominant and non-dominant legs. A symbol (*) is given at peak torque for significant differences between sports (see Table 2 for peak torque values).
Handball players demonstrated no significant differences between D and ND legs for quadriceps muscle strength but stronger hamstring muscles on D compared with ND legs (p = 0.001) (Table 2). Hence, the H:Q ratio was higher for D compared with ND legs for handball players (p = 0.012) (Table 2).
Football players demonstrated no significant differences in quadriceps muscle strength between D and ND legs (Table 2), but greater hamstring muscle strength values were recorded for D compared with ND legs (p < 0.0001) (Table 2). Table 2 shows data for mean difference between sports for D leg only, but similar values were revealed between sports for ND leg. Football players demonstrated no significant H:Q ratio differences between D and ND legs (Table 2).
Our literature search in PubMed on normative data for female, isokinetic knee extension, and flexion peak torques for similar age groups disclosed 15 studies. Twelve studies were excluded because of the following reasons: children (n = 3), other muscle groups (n = 3), other health conditions or injuries (n = 4), and no data in N·m for isokinetic knee extension and flexion (n = 2). Furthermore, 5 studies were included from reference lists from studies. A total of 8 studies were included for comparison to our data (Table 3 and Figure 6).
Table 3.
Mean and SD for peak isokinetic muscle strength at 60°·sec−1 in Newton meter (N·m), normalized peak torque (N·m·kg−1), H:Q ratio for dominant (D) and nondominant (ND) legs from our and other studies of athletic and nonathletic female populations of similar age.*

Figure 6.
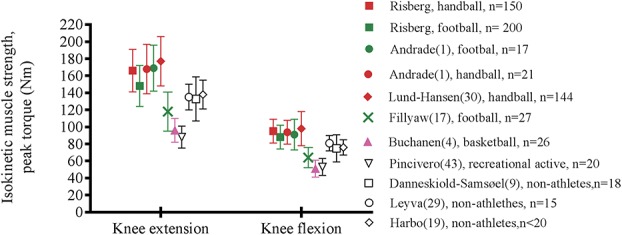
Mean and standard deviation for isokinetic peak torque values (Nm) for knee extension and flexion for dominant leg from our study and for previously published studies for athletic and non-athletic populations. Normative data for handball players (red), football players (green), basketball players (pink), and for non-athletes or recreational active (black without fill).
Lund-Hanssen et al. (26) found higher knee extension peak torque for handball players, also when normalize to body mass (p = 0.001), but similar knee flexion peak torque, hence, lower H:Q ratio, compared with our data. Andrade et al. (1) disclosed similar data for handball players as our data (Table 3). The other studies on football players disclosed higher (1) or lower (16) quadriceps strength compared with our data (Table 3). All the studies on the nonathletic populations (9,18,28,36) showed lower quadriceps and hamstring muscle strength compared with the athletic populations (p < 0.05), except for the younger population of basketball players (5) (Table 3 and Figure 6).
Discussion
Normative values for quadriceps and hamstrings muscle strength were reported for 350 female, healthy, elite handball and football players (Table 2). Although the BMI in handball and football players were similar, handball players were significantly taller and heavier, with significantly stronger quadriceps muscle, also when normalized to body mass (N·m·kg−1).
The standard error of measurement (SEM) for isokinetic knee extension and flexion tests have reported to be between 5 and 10% (36). In a more recent study (9), SEMs of 3.6–4.9% for isokinetic knee extension and flexion, respectively, were reported. Minimal detectable change for isokinetic knee extension and flexion has reported to be between 9.9 and 13.5%, respectively (9). Hence, these thresholds are required to detect individual changes in isokinetic quadriceps and hamstring muscle strength over time.
Chung et al. (5) reported significantly weaker quadriceps and hamstring muscle strength in the contralateral uninjured leg for previously ACL-injured athletes compared with healthy controls (5), with approximately 5% lower values for quadriceps and hamstring muscles strength in the contralateral knee compared with the control subjects. Weakened contralateral muscle strength may give false comparison parameters when the results of the operated ACL limb are assessed (5). When these ACL reconstructed subjects return to sport, they might have quadriceps and hamstring muscle strength deficits in both involved and uninvolved legs (35). Therefore, the use of symmetry index would have significant limitations; hence, normative muscle strength values matched for age, sport, and gender should be preferred. The risk of contralateral ACL injury has also shown to be greater than the first-time ACL injury for subjects participating in the same activity (39).
We found less than 3% differences between D and ND legs for peak torque values, which is the same as the accuracy of the force measuring system of isokinetic torques of 3% (14). Hence, we could not conclude that there is a real difference between D and ND legs for handball and football players. Both handball and football players demonstrated significantly greater hamstring strength on their D leg compared with ND leg. As expected, smaller SEMs have been reported for right and left legs differences (or D and ND legs) for knee extension and flexion (5% and 2%) (9).
A previous study has reported that male football players were more likely to injure their D leg while kicking the ball, whereas female football players injured their ACL more often while standing on their ND leg (3). Handball players would often state that their D leg is their jumping leg (most often left leg), but would answer the right leg if they were asked which leg they kicked a ball with. Football players would most often state that their D leg is the leg they kick with and that would be their strongest leg (24).
Hamstring to quadriceps ratios have been reported in many studies (Table 3), but have shown large variations (50–80%) (6,13,35). Comettti et al. (6) showed that football players at the elite level had a higher H:Q ratio than subelite level and amateur players and that this ratio increased with increased angular velocities. Another study found no differences in H:Q ratio between football players and recreationally active male subjects (13). A recent study found significant H:Q ratio differences across different field positions for football players (35). We found significantly lower H:Q ratio for handball players (57–58%) compared with football players (59–60%) but within the same range as reported for football players by Ruas et al. (35) (55–64%). One study found lower ratios for female elite handball (56%) and football players (54%) (1), but most studies seem to agree that the H:Q ratio is influenced by sports-specific demands (1,35) and that one should aim to increase the H:Q ratio to reduce injury risk in pivoting sports (31). However, other studies have found no effect of changing the H:Q ratio on injury risk (38), hence, what these H:Q ratios really mean are still debated. Others have also highlighted the use of hamstring eccentric to quadriceps concentric ratio that may better reflect the injury mechanisms, in particular for hamstring injuries (7).
Our normative data for handball and football players are in line with a few other studies on female handball and football players but with smaller sample sizes (Table 3). No differences were disclosed between our knee extension peak torque data and those reported by Andrade et al. (1) for handball or football players. Lund-Hanssen et al. (26) reported greater quadriceps muscle strength for handball players (p = 0.001) compared with our data, but similar hamstring strength data, also when normalized to body mass (Table 3). Finally, isokinetic peak torque data for the nonathletic populations disclosed significantly lower knee extension and flexion peak torques compared with our handball and football players (Table 3 and Figure 6) (8,17). Our study on normative isokinetic muscle strength data for knee extension and flexion adds to the body of knowledge with a large group of healthy handball and football players compared with previously published studies (Table 3). Lund-Hanssen et al. (26) from 1996 is the only study with a large sample size (n = 144), but they reported only data on handball players.
Reporting only isokinetic peak torque value has limitations. Previous studies have highlighted the importance of reporting quadriceps muscle performance during the whole ROM, identifying possible irregularities or asymmetries of muscle performance (12). Studies have identified the largest strength deficits in ACL-injured individuals between 40° of knee flexion toward full extension and not at peak torque (approximately 60° of knee flexion) (12,40). The use of isokinetic angle–specific torque values thus provide more information on quadriceps and hamstrings muscle performance than reporting a single peak torque value in ACL-, meniscus-, and articular cartilage–injured individuals (12). Hence, normative angle–specific curves shown in this study could be used clinically to compare isokinetic curves in knee-injured athletes. The whole isokinetic knee extension and flexion torque curves in healthy athletes can thus be used as reference curves in comparison to those with knee injury (Figures 2–5).
The major strength of this study is the large population of female elite athletes within 2 sports with a high risk of lower limb injuries. Furthermore, we have reported knee extension and flexion torque curves, not only peak torque values. These torque curves for knee extension and flexion could be used as reference curves when isokinetic knee extension and flexion testing are used for testing knee-injured individuals. A limitation of this study is the lack of other functional performance tests, such as single-leg hop tests, that would be of great interest to enable comparison of muscle strength to functional performance among female elite handball and football players. However, the scope of this article was to serve as normative data on muscle strength; hence, we did not include normative data for any functional performance tests. Several studies have also recommended using functional H:Q ratio where eccentric strength is included (2,13). We do not have any eccentric data on these individuals and only assessed the conventional H:Q ratio including concentric strength tests, which was also used and reported by many authors (1,35). One should also be cautious of interpreting injury risk from these H:Q ratios because we have no information about their future risk of injury.
Practical Applications
These normative isokinetic knee extension and flexion muscle strength values during knee ROM of healthy, elite, female handball and football players can be used to set rehabilitation goals for muscle strength after injury and enable comparison with uninjured legs. This study included a large number of subjects and showed that there are sport-specific differences in quadriceps and hamstring muscle strength for healthy individuals.
Acknowledgments
The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS. The authors have no conflicts of interest to disclose. The study was approved by the Regional Committee for Medical Research Ethics; South-Eastern Norway Regional Health Authority, Norway, and by the Norwegian Social Science Data Services.
References
- 1.Andrade MS, De Lira CA, Koffes FC, Mascarin NC, Benedito-Silva AA, and Da Silva AC. Isokinetic hamstrings-to-quadriceps peak torque ratio: The influence of sport modality, gender, and angular velocity. J Sports Sci 30: 547–553, 2012. [DOI] [PubMed] [Google Scholar]
- 2.Ardern CL, Pizzari T, Wollin MR, and Webster KE. Hamstrings strength imbalance in professional football (soccer) players in Australia. J Strength Cond Res 29: 997–1002, 2015. [DOI] [PubMed] [Google Scholar]
- 3.Brophy R, Silvers HJ, Gonzales T, and Mandelbaum BR. Gender influences: The role of leg dominance in ACL injury among soccer players. Br J Sports Med 44: 694–697, 2010. [DOI] [PubMed] [Google Scholar]
- 4.Buchanan PA, and Vardaxis VG. Lower-extremity strength profiles and gender-based classification of basketball players ages 9-22 years. J. Strength. Cond. Res 23:406–419, 2009. [DOI] [PubMed] [Google Scholar]
- 5.Chung KS, Ha JK, Yeom CH, Ra HJ, Lim JW, Kwon MS, and Kim JG. Are muscle strength and function of the uninjured lower limb weakened after anterior cruciate ligament Injury? Two-year follow-up after reconstruction. Am J Sports Med 43: 3013–3021, 2015. [DOI] [PubMed] [Google Scholar]
- 6.Cometti G, Maffiuletti NA, Pousson M, Chatard JC, and Maffulli N. Isokinetic strength and anaerobic power of elite, subelite and amateur French soccer players. Int J Sports Med 22: 45–51, 2001. [DOI] [PubMed] [Google Scholar]
- 7.Coombs R. and Garbutt G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med 1: 56–62, 2002. [PMC free article] [PubMed] [Google Scholar]
- 8.Danneskiold-Samsoe B, Bartels EM, Bulow PM, Lund H, Stockmarr A, Holm CC, Watjen I, Appleyard M, and Bliddal H. Isokinetic and isometric muscle strength in a healthy population with special reference to age and gender. Acta Physiol (Oxf) 197(Suppl 673): 1–68, 2009. [DOI] [PubMed] [Google Scholar]
- 9.de Carvalho Froufe Andrade AC, Caserotti P, de Carvalho CM, de Azevedo Abade EA, and da Eira Sampaio AJ. Reliability of concentric, eccentric and isometric knee extension and flexion when using the REV9000 isokinetic dynamometer. J Human Kinetics 37: 47–53, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Decker MJ, Torry MR, Wyland DJ, Sterett WI, and Richard Steadman J. Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin Biomech (Bristol, Avon) 18: 662–669, 2003. [DOI] [PubMed] [Google Scholar]
- 11.Drouin JM, Valovich-mcLeod TC, Shultz SJ, Gansneder BM, and Perrin DH. Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. Eur J Appl Physiol 91: 22–29, 2004. [DOI] [PubMed] [Google Scholar]
- 12.Eitzen I, Eitzen TJ, Holm I, Snyder-Mackler L, and Risberg MA. Anterior cruciate ligament-deficient potential copers and noncopers reveal different isokinetic quadriceps strength profiles in the early stage after injury. Am J Sports Med 38: 586–593, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Evangelidis PE, Pain MT, and Folland J. Angle-specific hamstring-to-quadriceps ratio: A comparison of football players and recreationally active males. J Sports Sci 33: 309–319, 2015. [DOI] [PubMed] [Google Scholar]
- 14.Farrell M. and Richards JG. Analysis of the reliability and validity of the kinetic communicator exercise device. Med Sci Sports Exerc 18: 44–49, 1986. [PubMed] [Google Scholar]
- 15.Fillyaw M, Bevins T, and Fernandez L. Importance of correcting isokinetic peak torque for the effect of gravity when calculating knee flexor to extensor muscle ratios. Phys Ther 66:23–31, 1986. [DOI] [PubMed] [Google Scholar]
- 16.Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, and Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. Br J Sports Med 50: 804–808, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Harbo T, Brincks J, and Andersen H. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur J Appl Physiol 112: 267–275, 2012. [DOI] [PubMed] [Google Scholar]
- 18.Holm I, Risberg MA, Aune AK, Tjomsland O, and Steen H. Muscle strength recovery following anterior cruciate ligament reconstruction. Isokinet Exerc Sci 8: 57–63, 2000. [Google Scholar]
- 19.Kim HJ, Lee JH, Ahn SE, Park MJ, and Lee DH. Influence of anterior cruciate ligament tear on thigh muscle strength and hamstring-to-quadriceps ratio: A meta-analysis. PLoS One 11: e0146234, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Konishi Y, Konishi H, and Fukubayashi T. Gamma loop dysfunction in quadriceps on the contralateral side in patients with ruptured ACL. Med Sci Sports Exerc 35: 897–900, 2003. [DOI] [PubMed] [Google Scholar]
- 21.Kristianslund E, Faul O, Bahr R, Myklebust G, and Krosshaug T. Sidestep cutting technique and knee abduction loading: Implications for ACL prevention exercises. Br J Sports Med 48: 779–783, 2014. [DOI] [PubMed] [Google Scholar]
- 22.Krosshaug T, Steffen K, Kristianslund E, Nilstad A, Mok KM, Myklebust G, Andersen TE, Holme I, Engebretsen L, and Bahr R. The vertical drop jump is a poor screening test for ACL injuries in female elite soccer and handball players: A prospective cohort study of 710 athletes. Am J Sports Med 44: 874–883, 2016. [DOI] [PubMed] [Google Scholar]
- 23.Kurdak SS, Ozgunen K, Adas U, Zeren C, Aslangiray B, Yazici Z, and Korkmaz S. Analysis of isokinetic knee extension/flexion in male elite adolescent wrestlers. J Sports Sci Med 4: 489–498, 2005. [PMC free article] [PubMed] [Google Scholar]
- 24.Lanshammar K. and Ribom EL. Differences in muscle strength in dominant and non-dominant leg in females aged 20-39 years–a population-based study. Phys Ther Sport 12: 76–79, 2011. [DOI] [PubMed] [Google Scholar]
- 25.Leyva A, Balachandran A, and Signorile JF. Lower-body torque and power declines across six decades in three hundred fifty-seven men and women: a cross-sectional study with normative values. J Strength. Cond. Res 30:141–158, 2016. [DOI] [PubMed] [Google Scholar]
- 26.Lund-Hanssen H, Gannon J, Engebretsen L, Holen K, and Hammer S. Isokinetic muscle performance in healthy female handball players and players with a unilateral anterior cruciate ligament reconstruction. Scand J Med Sci Sports 6: 172–175, 1996. [DOI] [PubMed] [Google Scholar]
- 27.Myklebust G, Maehlum S, Holm I, and Bahr R. A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports 8: 149–153, 1998. [DOI] [PubMed] [Google Scholar]
- 28.Neder JA, Nery LE, Shinzato GT, Andrade MS, Peres C, and Silva AC. Reference values for concentric knee isokinetic strength and power in nonathletic men and women from 20 to 80 years old. J Orthop Sports Phys Ther 29: 116–126, 1999. [DOI] [PubMed] [Google Scholar]
- 29.Niederer D, Wilke J, Vogt L, and Banzer W. Return to play after injuries—A survey on the helpfulness of various forms of assistance in the shared decision-making process in semi-professional athletes in Germany. Arch Phys Med Rehabil 99: 690–698, 2017. [DOI] [PubMed] [Google Scholar]
- 30.Oiestad BE, Holm I, Aune AK, Gunderson R, Myklebust G, Engebretsen L, Fosdahl MA, and Risberg MA. Knee function and prevalence of knee osteoarthritis after anterior cruciate ligament reconstruction: A prospective study with 10 to 15 years of follow-up. Am J Sports Med 38: 2201–2210, 2010. [DOI] [PubMed] [Google Scholar]
- 31.Orchard J, Marsden J, Lord S, and Garlick D. Preseason hamstring muscle weakness associated with hamstring muscle injury in Australian footballers. Am J Sports Med 25: 81–85, 1997. [DOI] [PubMed] [Google Scholar]
- 32.Palmieri-Smith RM. and Lepley LK. Quadriceps strength asymmetry after anterior cruciate ligament reconstruction alters knee joint biomechanics and functional performance at time of return to activity. Am J Sports Med 43: 1662–1669, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pincivero DM, Gandaio CM, and Ito Y. Gender-specific knee extensor torque, flexor torque, and muscle fatigue responses during maximal effort contractions. Eur J Appl Physiol 89: 134–141, 2003. [DOI] [PubMed] [Google Scholar]
- 34.Probst MM, Fletcher R, and Seelig DS. A comparison of lower-body flexibility, strength, and knee stability between karate athletes and active controls. J Strength Cond Res 21: 451–455, 2007. [DOI] [PubMed] [Google Scholar]
- 35.Ruas CV, Minozzo F, Pinto MD, Brown LE, and Pinto RS. Lower-extremity strength ratios of professional soccer players according to field position. J Strength Cond Res 29: 1220–1226, 2015. [DOI] [PubMed] [Google Scholar]
- 36.Sole G, Hamren J, Milosavljevic S, Nicholson H, and Sullivan SJ. Test-retest reliability of isokinetic knee extension and flexion. Arch Phys Med Rehabil 88: 626–631, 2007. [DOI] [PubMed] [Google Scholar]
- 37.Steffen K, Nilstad A, Kristianslund EK, Myklebust G, Bahr R, and Krosshaug T. Association between lower extremity muscle strength and noncontact ACL. Injuries Med Sci Sports Exerc 48: 2082–2089, 2016. [DOI] [PubMed] [Google Scholar]
- 38.Steffen K, Nilstad A, Krosshaug T, Pasanen K, Killingmo A, and Bahr R. No association between static and dynamic postural control and ACL injury risk among female elite handball and football players: A prospective study of 838 players. Br J Sports Med 51: 253–259, 2017. [DOI] [PubMed] [Google Scholar]
- 39.Sward P, Kostogiannis I, and Roos H. Risk factors for a contralateral anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 18: 277–291, 2010. [DOI] [PubMed] [Google Scholar]
- 40.Thomee R, Kaplan Y, Kvist J, Myklebust G, Risberg MA, Theisen D, Tsepis E, Werner S, Wondrasch B, and Witvrouw E. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 19: 1798–1805, 2011. [DOI] [PubMed] [Google Scholar]
- 41.Urbach D. and Awiszus F. Impaired ability of voluntary quadriceps activation bilaterally interferes with function testing after knee injuries. A twitch interpolation study. Int J Sports Med 23: 231–236, 2002. [DOI] [PubMed] [Google Scholar]
- 42.van der Horst N, Backx F, Goedhart EA, and Huisstede BM. Return to play after hamstring injuries in football (soccer): A worldwide Delphi procedure regarding definition, medical criteria and decision-making. Br J Sports Med 51: 1583–1591, 2017. [DOI] [PubMed] [Google Scholar]
- 43.Wright RW, Magnussen RA, Dunn WR, and Spindler KP. Ipsilateral graft and contralateral ACL rupture at five years or more following ACL reconstruction: A systematic review. J Bone Joint Surg Am 93: 1159–1165, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]