

Abstract
The current study addressed whether two institution-wide interventions in St. Petersburg, Russian Federation, that increased caregiver sensitivity (Training Only: TO) or both caregiver sensitivity and consistency (Training plus Structural Changes: T+SC) promoted better social-emotional and cognitive development than a No Intervention (NoI) institution during the first year of life for children who were placed soon after birth. It also assessed whether having spent less than 9 versus 9-36 months with a family prior to institutionalization was related to children’s subsequent social-emotional and cognitive development within these three institutions. The Battelle Developmental Inventory was used to assess the social-emotional and cognitive functioning of children in NoI (n = 95), TO (n = 104), and T+SC (n = 86) at 2-3 time points during their first 6-12 months of residency. Results suggest that improving caregiver sensitivity can improve the cognitive development of infants in the first year of institutionalization, whereas improving caregiver consistency in addition to sensitivity is more beneficial for social-emotional development than sensitivity alone. Similarly, for children in T+SC, longer time with a family prior to institutionalization (consistent caregiver, unknown sensitivity) was associated with better social-emotional but not cognitive baseline scores and more rapid cognitive than social-emotional development during institutionalization. These results suggest caregiver sensitivity is more highly related to cognitive development whereas caregiver consistency is more related to social-emotional development in the first years of life.
Keywords: Institution, Orphanage, Caregiver Intervention, HLM
Approximately 2-8 million children worldwide live in institutional care of varying, often poor, quality (Engle, Groza, Groark, Greenberg, Bunkers, & Muhamedrahimov, 2011; UNICEF, 2009). The current study assessed whether interventions to improve caregiver-child relationships within these institutions can improve social-emotional and cognitive development for resident children and what (if any) association living with a family prior to institutionalization has with subsequent development within the institution.
Although institutional care varies between and within countries, children in most institutions experience many changing caregivers who are often cold and unresponsive in their interactions with children (Chisholm, 1998). According to attachment theory (Ainsworth et al., 1978; Bowlby, 1962), children reared in typical families are hypothesized to transition through three phases of attachment development. From birth to approximately 4.5 months is a time of pre-attachment, in which children seek help and comfort indiscriminately from all humans. From approximately 4.5 to 6 months, children actively form attachments by seeking help and comfort from a discriminated figure but continue to accept comfort from most people. After about 6 months, children typically have a discriminated attachment, seeking help and comfort from specific people. Over the following years, interactions with attachment figures provide a framework for the child to develop internal working models of self, others, and the world (Ainsworth et al., 1978; Bowlby, 1962).
When describing attachment formation, it is important to consider both whether a familiar and consistently available figure is present in a child’s life (consistency) and whether that figure is responsive to the child’s social cues and needs for comfort and support (sensitivity). Assuming consistency, sensitive caregiver interactions are expected to help children develop secure attachment bonds and expectations that caregivers are responsive and safe. Secure attachments are associated with positive development in social-emotional (e.g., self-confidence, emotional regulation, prosocial behaviors) and cognitive (e.g., exploration, problem-solving, cognitive flexibility) domains (Ainsworth et al., 1978; Sroufe, 2005). Indeed, within typical families, parental sensitivity and attachment security have been found to be related to better executive functioning skills in three-year-old children (Bernier, Carlson, Deschenes, & Matte-Gagne, 2012; Bernier, Carlson, & Whipple, 2010). Executive functioning, in turn, has been associated with cognitive outcomes of academic achievement (Biederman et al., 2004) and verbal and nonverbal reasoning (van der Sluis, de Jong, & van der Leij, 2007), as well as social-emotional outcomes of communication, social competence (Clark, Prior, & Kinsella, 2002; Kochanska, Murray, & Harlan, 2000), and emotion regulation (Carlson & Wang, 2007).
Despite their theoretical distinction, research is lacking on the relative contribution of consistency to the development of children reared in families or institutions. For an infant to identify a discriminated attachment figure, a consistent figure must be present in the child’s life. Caregiver consistency is theorized to be necessary for children to develop expectations about caregivers and organize their understanding of the world (Ainsworth et al., 1978; Bowlby, 1969). Without a consistent caregiver, researchers propose that children may not form any attachment at all (Bakermans-Kranenburg et al., 2011). Studies of maltreatment assess consistency in responses (e.g., sometimes warm, sometimes harsh); however, this does not address having a consistent figure. Children in childcare experience multiple caregivers, and lack of caregiver continuity has been related to poorer self-control, initiative, and attachment during infancy (Horm et al., 2018), and to poorer social, cognitive, and emotional growth in older students (Hale-Jinks, Knopf, & Kemple, 2006); however, parents remain consistent. Children in foster care experience multiple primary caregivers (i.e., parents plus foster families), and more disruptions in care are related to poorer outcomes. However, researchers suggest that these negative child behaviors are both a cause and consequence of disruptions (Oosterman, Schuengel, Slot, Bullens, & Doreleijers, 2007). Even for foster children, the same figure is available for the duration of time in that person’s care. Thus, the problem of consistency for foster children could be defined as serial relationships. In contrast, institutional caregivers are often not consistently available from one day to the next due to their schedules and high rates of turnover (Chisolm, 1998). Thus, children in institutions experience daily inconsistency, but it is often also accompanied by insensitive care and other depriving aspects of the institution.
Additionally, for many children, the institution is not their only early environment. Some children first live with their birth families, only to be surrendered later. Information on the nature of the family experience is typically unavailable despite calls for more study of pre-institutional experiences (McCall, 2011). Only two known studies address this issue. One concludes that that early institutional abuse is related to higher levels of behavior problems (internalizing and externalizing) than early abuse in families (Hermanau, Hecker, Elbert, & Rug-Leuschner, 2014). The other concludes that prenatal risk and pre-institutional emotional neglect were related to higher rates of indiscriminate behavior among institutionalized toddlers than those without pre-institutional risk factors (Oliveira et al., 2012). Thus, there is mixed evidence for whether spending time with a family prior to institutionalization is more or less detrimental to children’s development than being placed in the institution earlier. However, both studies assessed only one time point, not longitudinal development in the institution, and neither assessed how pre-institutional environment interacts with institutional quality.
The amount of time children spend with their families should affect whether they form attachment relationships, which would be disrupted upon institutionalization. Thus, children who spent enough time with their families to have likely formed an attachment bond with parents may offer interesting insights; of specific interest is the role that the loss of attachment figures and early opportunities for one-on-one social interactions play in subsequent development within institutions when compared with infants placed earlier. Because researchers suggest that adoption is more difficult for children who are adopted after they have formed an attachment bond (Bodzinsky, 1987) and that children experience prolonged separation distress following the loss of an attachment figure (Bowlby, 1980), it is predicted that children who enter institutions after having spent enough time with a family to develop an attachment relationship will likewise have more difficulty with the transition, especially in social-emotional realms, than children who do not experience that same loss.
St. Petersburg Baby Home Intervention
Baby Homes (i.e., institutions for children ages 0-4 years) in St. Petersburg, Russian Federation, have been studied in depth and defined as selectively social-emotionally depriving (St. Petersburg-USA Orphanage Research Team, 2005, 2008). Because Baby Homes are federally funded by the Ministry of Health and directed by pediatricians, children receive adequate medical care, sanitation, nutrition, toys, and equipment. However, children experience 60-100 different caregivers over the course of two years and rarely see the same caregiver on two consecutive days (inconsistency), and caregivers perform their duties in a perfunctory manner with few contingent interactions and predominately in a caregiver- rather than child-directed manner (insensitivity).
The three institutions in the St. Petersburg-USA Orphanage Research Team’s (2008) intervention offer a unique opportunity to assess the effects of caregiver sensitivity and consistency on children’s development in a high-risk sample. A No Intervention (NoI) control Baby Home continued the insensitive and inconsistent care described above. In a Training Only (TO) intervention Baby Home, caregivers were trained to provide sensitive, response-contingent care, but their schedules remained inconsistent and similar to NoI. Finally, a Training plus Structural Changes (T+SC) intervention included both the training and structural changes that increased the consistency and sensitivity of caregivers. In an initial evaluation of the intervention, mean scores of children with 4-9 months of Baby Home exposure were compared to mean scores of children with 9+ months of exposure. Results indicated that children in T+SC had higher scores on all developmental scales than children in NoI and TO, and improved more with longer exposure. However, there were few differences between TO and NoI. While very promising, these analyses assessed mean differences rather than individual differences and did not assess whether other factors (e.g., age at exposure, pre-institutional experience) above and beyond the interventions were related to the outcomes. Details and documentation of these interventions and prior results are presented in St. Petersburg—USA Orphanage Research Team (2008).
Pre-Institutional Experiences
At the time of the intervention, approximately 1% of neonates in the Russian Federation were relinquished by their mothers within the first hours of life (Muhamedrahimov, 2000). Additional common reasons for Baby Home entry included social and financial hardship, parental illness, parental imprisonment, inappropriate living conditions, and child morbidity (St. Petersburg-USA Orphanage Research Team, 2005). Although the quality of early parental care is unknown and possibly poor, the amount of time children spend with their families could provide the opportunity for some children to form attachment relationships and to receive qualitatively different care than they receive in institutions. If children spend enough time with their families, institutionalization may also represent a loss of attachment figures and early caregiver consistency compared with infants placed earlier (Bowlby, 1969).
Current Study
The goal of this study was to examine the association of caregiver sensitivity and consistency with the social-emotional and cognitive development of young institutionalized children and to determine whether prior family experience impacts this association. Infants who entered institutions immediately following birth or post-natal hospitalization were followed longitudinally during their first year of residency in one of three Baby Homes: the NoI Baby Home in which children experienced neither sensitivity nor consistency, the TO Baby Home in which children experienced sensitivity but not consistency, and the T+SC Baby Home in which children experienced both sensitivity and consistency.
Because children learn through social interactions, the quality of caregiver-child interactions during the first year of life, including helping infants manage distress, promoting exploration, and providing perceptual-linguistic experiences to children in the context of response-contingent interactions, should be related to children’s cognitive, as well as social-emotional, development. Children tend to enter institutions with much lower than average functioning in all areas (St. Petersburg-USA Orphanage Research Team, 2005, 2008). This study builds on previous findings but expands them by utilizing multi-level modeling techniques that allow for an assessment of individual differences, focusing on a specific age range (i.e., enter the Baby Home between 0-3 months and remain until 6-12 months old), co-varying child-specific factors that could influence results, and including only children who entered the Baby Home directly from the hospital, thereby creating a relatively pure assessment of intervention effects. Hypotheses include:
When neither consistency nor sensitivity is available (NoI), children should show poor rates of social-emotional and cognitive development, maintaining their below average functioning.
Children should show faster skill acquisition in social-emotional and cognitive domains with sensitive but inconsistent caregiving (TO).
Social-emotional and cognitive development should be especially positive with both consistent and sensitive caregivers (T+SC).
To address interactions with family experience, children who first spent time with a family were followed during their first year of Baby Home residency. These children experienced no continuity of persons from family to Baby Home, and some who spent more than approximately nine months with their family also presumably lost their primary attachment figure(s). Hypotheses include:
- Children who spent at least 9 months with a family would have more negative social-emotional functioning soon after institutionalization than children with no or less than 9 months family experience.
- These children would gain social-emotional skills more slowly when no consistent caregiver is available (NoI and TO) vs. more quickly when children could form new relationships (T+SC).
- Children who spent less than 9 months with families would show similar trajectories as No-Family children.
- Time with family would not relate to cognitive and communicative abilities at intake.
- Baby Home environments that promote sensitive, response-contingent, and child-directed interactions (TO and T+SC) were expected to be related to faster cognitive and communicative skill acquisition than NoI for children who spent any time with a family, similar to that seen for children without family experience.
Methods
Participants
The total sample included 485 children residing in the three Baby Homes in St. Petersburg, Russian Federation, who entered the Baby Homes after full implementation of the interventions but before they were three years of age and who were without limiting disabilities (for details see St. Petersburg—USA Orphanage Research Team, 2008). Of these, 80 were omitted for missing crucial demographic data, 98 for having only one assessment, and 22 because they were in a children’s hospital for more than 3 months before entering the Baby Home. Thus, 285 children (147 male) participated, all completing at least two assessments. Children entered the Baby Homes at different ages, with a mean age at intake of 4.54 months (SD = 7.75).
Procedure
At intake, Baby Home workers obtained medical and legal records of the child and interviewed birth parents if possible about the child’s history. Children were assessed at 3, 6, 9, 12, 18, 24, 36, and 48 months (St. Petersburg-USA Orphanage Research Team, 2008). For children arriving after three months, an intake assessment was completed 1-2 months after arrival. Children who left the Baby Home before 48 months were assessed prior to discharge. During these assessments, trained independent examiners administered the tests to children accompanied by the caregiver the child knew best.
Baby Home Interventions
The interventions were implemented throughout each of three separate Baby Homes (The St. Petersburg-USA Orphanage Research Team, 2008). The Training plus Structural Changes (T+SC) intervention involved both caregiver training and structural changes. The Training Only (TO) intervention involved the same caregiver training without structural changes, and the No Intervention (NoI) Baby Home conducted care as usual.
Training Component
The training component, included in both TO and T+SC interventions, taught new information to caregivers and encouraged behaviors more similar to those of Russian birth parents. Specific goals included increasing warm and responsive child interactions, increasing child-directed activities, promoting independence and creativity in the children, and becoming more sensitive and responsive during care. The training emphasized a general way of interacting with children rather than providing specific behaviors or routines to perform. Caregivers were taught to be flexible and to match their behavior with the children to the specific child and situation. The information in the curriculum emphasized the importance of allowing children to choose their own activities and to form relationships and representations of self and others, supporting attachments with consistent caregivers, teaching caregivers to engage in child-directed activities, training caregivers to use behavioral contingencies and instruction to maintain a positive behavioral environment, and matching teaching to the children’s developmental abilities.
To evaluate the effectiveness of the training, two parallel versions of 40-item multiple-choice tests were administered to caregivers at the beginning and the end of training. Caregivers in both TO and T+SC had higher post-test than pre-test scores, indicating that they learned the training materials (partial η2 = .66). The HOME Inventory (Caldwell & Bradley, 1984), adapted for use in group care environments (NICHD Study of Early Child Care Manual), was used to assess caregiver behaviors and sensitivity. Caregiver HOME scores were higher in T+SC than TO and NoI during the first year post-intervention and remained high (partial η2 = .41). During the second year, HOME scores in NoI decreased, while scores in TO increased modestly, resulting in higher HOME scores for TO than NoI caregivers during the second year of intervention. During this time, caregivers in TO continued to show lower scores than caregivers in T+SC (for more detail see St. Petersburg-USA Orphanage Research Team, 2008).
Structural Change Component
The structural change component, included only in T+SC, altered physical structure, work schedules, and procedural circumstances to encourage caregiver consistency and attachment with the children. Group sizes were lowered from 10-14 children to 5-7 children per group. Two primary caregivers were assigned to each subgroup and worked staggered schedules so that one was on duty nearly all of the children’s waking hours seven days per week. Four secondary caregivers were allocated to each subgroup, and replacement and substitute staff were assigned to subgroups so that the same substitute would consistently work with the same children. These changes adjusted the number of caregivers per week from 9 to 6 on average.
Routine and periodic transitions to new wards were eliminated, so that children remained in their same group from arrival until departure. This “looping” decreased the total number of caregivers children experienced and resulted in groups with children ranging in age from birth to 4 years and with varying levels of disabilities. A procedural intervention of “family hour” was also established, consisting of one hour in the morning and one hour in the afternoon during which caregivers played with children in their subgroups without visitors or specialists interrupting the interactions. The specific activities or content of this time was not predetermined or assessed.
Examination of official employment records determined that in T+SC, children saw approximately six caregivers per month after changes were implemented, in contrast to the 10-12 caregivers per month seen by children in both NoI and TO. Including staff turnover, graduations, and reassignments, but not daily substitutions or special service providers, children who spent 19+ months in T+SC received care from approximately 30+ caregivers, whereas those in TO and NoI received care from 60-100 different caregivers. Caregivers in T+SC had approximately six children at a time versus 12-14+ children in NoI and TO. Primary caregivers in T+SC worked approximately 3.5 days in a row; whereas secondary caregivers in T+SC and all caregivers in TO and NoI worked only 1.2 days in a row. There were no differences in staff turnover between the Baby Homes. Over time, the mean age of children in each ward in T+SC converged on the mean for the entire Baby Home (i.e., age integration), but each ward in TO and NoI maintained stable mean age differences over time as a result of graduations (for further fidelity results see St. Petersburg-USA Orphanage Research Team, 2008).
Measures
Demographic Variables
All demographic and history variables were collected from Baby Home records and are presented in Table 1. Age at intake and time in the Baby Home were calculated from history information in the records (i.e., birth date, date of entry, date of assessment). Maternal alcohol and drug use was noted in narrative hospital records by the obstetrician, but not for all children, and for research purposes was coded as a binary variable (alcohol/drug use vs. none mentioned). Unfortunately, data were not available for all children and there was no information regarding whether mothers who kept their children continued to use alcohol or drugs. Birth weight, birth height, and gestational age were highly correlated (r = .72 - .91), raising the risk of collinearity. Because of the negative consequences associated with prematurity and the large range of gestational ages (27 – 42 weeks), gestational age was chosen, in combination with Apgar score, to represent birth characteristics.
Table 1.
Descriptive Statistics
| N | Mean | SD | Range | |
|---|---|---|---|---|
|
|
||||
| Battelle Developmental Inventory | ||||
| Personal-Social (1) | 260 | 56.69 | 23.19 | 10.53-115.79 |
| Personal-Social (3) | 170 | 59.17 | 17.71 | 8.33-100.00 |
| Communication (1) | 264 | 64.67 | 27.87 | 16.67-133.33 |
| Communication (3) | 170 | 62.17 | 21.53 | 11.11-122.22 |
| Cognitive (1) | 239 | 69.22 | 28.90 | 14.29-133.33 |
| Cognitive (3) | 169 | 79.64 | 19.37 | 11.11-125.00 |
| PCERA | ||||
| Caregiver Total (1) | 285 | 3.88 | 0.46 | 2.29-5.00 |
| Caregiver Total (3) | 170 | 3.73 | 0.46 | 2.43-4.85 |
| Dyadic Engagement (1) | 285 | 2.95 | 0.71 | 1.25-4.75 |
| Dyadic Engagement (3) | 170 | 2.94 | 0.65 | 1.00-4.50 |
| Baby Home and Family | ||||
| NoI | 95 (33.3%) | |||
| TO | 104 (36.5%) | |||
| T+SC | 86 (30.2%) | |||
| No-Family | 195 (68.4%) | |||
| Family < 9 Months | 41 (14.4%) | |||
| Family ≥ 9 Months | 49 (17.2%) | |||
| Voluntary Placement | 188 (66.0%) | |||
| Involuntary Relinquishment | 97 (34.0%) | |||
| Age at Intake (months) | 285 | 4.54 | 7.75 | 0.00-35.88 |
| Months in the Baby Home (1) | 285 | 1.97 | 0.87 | 0.23-7.59 |
| Months in the Baby Home (2) | 285 | 5.01 | 1.28 | 1.87-11.37 |
| Months in the Baby Home (3) | 170 | 7.83 | 1.24 | 5.16-12.02 |
| Child/Birth Characteristics | ||||
| Male | 147 (51.6%) | |||
| Female | 138 (48.4%) | |||
| Maternal Substance Use | 153 (53.7%) | |||
| FAI Total | 285 | 1.96 | 0.40 | 1.11-3.00 |
| Gestation Length (weeks) | 285 | 37.75 | 2.62 | 27.00-42.00 |
| Apgar 10 min | 285 | 8.28 | 0.68 | 5.00-10.00 |
Note. For categorical variables, only the number of participants fitting that description is shown.
Correspond to assessment number 1, 2, or 3;
NoI – No Intervention; TO – Training Only; T+SC – Training plus Structural Changes; FAI – Functional Abilities Index.
Records included pre-Baby Home location, and children were coded as entering the Baby Home from a birth hospital or children’s hospital (No-Family; N = 195), or from biological parent or kinship care (Family; N = 90). Children without family experience (i.e., No-Family) were removed or relinquished at birth and entered the Baby Home between 0-3 months of age depending on medical needs, whereas Family children arrived between 1 and 36 months of age after first spending time in a family. Because attachment theory suggests that discriminated attachments are not formed until 6-12 months, object permanence does not fully develop until approximately 9 months, and the number of children who arrived at different ages, Family children were divided into those who spent less than nine months with a family (Family <9 Months, N = 41) and those who spent nine or more months with a family (Family ≥9 Months, N = 49). Although no information was available regarding children’s experiences in the family, 66% (N = 188) of the sample was voluntarily placed in the Baby Home, whereas 34% (N = 97) of the sample were involuntarily relinquished.
Battelle Developmental Inventory
The Battelle Developmental Inventory (Newborg, Stock, Wnek, Guidubaldi, & Svinicki, 1988) measures the developmental progress of children aged birth to 95 months within Gross Motor, Fine Motor, Adaptive Behavior, Cognitive, Communication, and Personal-Social domains plus a total score. The current study uses the Personal-Social (interaction with others, affect expression, self-concept, coping), Communication (receptive, expressive), and Cognitive (perceptual discrimination, memory, reasoning, concepts) scales because they closely match the purpose of the intervention. Additionally, correlations with criterion measures (e.g., Peabody Picture Vocabulary Test, Kohn Social Competence Scale, Sells and Roff Scale of Peer Relations, Vineland Socialization scale) have been found to be highest and most consistent for Cognitive, Communication, and Personal-Social scales (Guidubaldi & Perry, 1984; Johnson, Cook, & Kullman, 1992). In the current sample, test-retest reliability for children 0-72 months ranged from .97-.99. Standard scores (Developmental Quotients) were created by converting the raw scores to mental age using Battelle conversion tables then dividing the mental age by chronological age multiplied by 100. Unfortunately, available norms were based on a 1988 sample of approximately 50 children for each 6-month age range and were not judged to be especially relevant to the Baby Home population. Thus, although the DQs provide an age-invariant score for comparisons across age, they should not be judged against the mean and percentiles used for IQ scores based on non-institutionalized USA children.
Functional Abilities Index
The Functional Abilities Index (FAI; Muhamedrahimov, Palmov, & Istomina, 2000) is a modification of the Abilities Index (Simeonsson & Bailey, 1991) designed to be specific to the institutional context. The FAI assesses nine domains and associated subdomains of physical and behavioral disability, including audition, behavior and social skills, intellectual functioning, motor functioning, intentional communication, tonicity, integrity of physical health, eyes, and structural status. Ratings for each subdomain were made by Baby Home neuropathologists and Special Teachers trained in educating children with disabilities using a 6-point scale (0 =normal/typical to 5= profound/extreme problems).
The FAI was used to exclude children with disabilities severe enough to interfere with growth or behavioral development. Disability was defined as having at least one of the nine FAI domain ratings equal to 5 or higher (severe or profound/extreme) or four or more scores rated 4 or higher (moderate problems). The current sample includes only those children not identified as having a disability; however, average FAI scores were still used as covariates in analyses to control for variability in functional abilities. Only scores on the first FAI are used here because change in disabilities is not the focus and the FAI classification showed substantial stability over time (St. Petersburg-USA Orphanage Research Team, 2008).
Parent-Child Early Relational Assessment
The Parent-Child Early Relational Assessment (PCERA; Clark, 1985) assessed the social-emotional behaviors of the child, caregiver, and caregiver-child dyad. The PCERA was originally developed to assess parent-child relationships; however, for this study children were assessed with the caregiver with whom they had the best relationship, who knew the child best, or who spent the most time with the child. Importantly, given the nature of the institution, this caregiver may be different at different assessments, and the same caregiver may have participated with multiple children. The assessment included three parts and proceeded in a standard order: feeding, structured task, and free play. The current study uses coding from the five-minute free play scenario.
The free play interaction was reviewed on video, and coders made global ratings for caregiver, child, and dyadic characteristics. Ratings were based on a 5-point Likert scale (1-2 = areas of concern, 3 = area of some concern, 4-5 = areas of strength), assessing intensity, duration, and frequency of behavioral characteristics. In total, 29 caregiver characteristics, 28 child characteristics, and 8 dyadic characteristics were assessed and combined to create mean scores. The current study uses Caregiver and Dyadic total scores as time-varying predictors of child Battelle scores. The caregiver characteristics refer to tone of voice, affect, mood, attitudes expressed toward the child, affective and behavioral involvement, and style. The dyadic characteristics describe the affective quality of interactions and mutuality. Correlations between pairs of coders on the 65 subscales ranged from .55 to .86, with 96% of the paired ratings of the 65 variables identical or within 1 point.
Modeling Procedures
Multilevel growth models were estimated using HLM 7 (Raudenbush, Bryk, Cheong, Congdon, & du Toit, 2011) to assess individual trajectories of cognitive and social-emotional development of children in the three Baby Homes during their first year of residency. All children had two (N = 285) and 60% of the sample had three (N = 170) assessments included in the analyses. HLM models were used to assess trajectories of Battelle Cognitive, Personal-Social, and Communication scores. In analyses, Level 1 corresponded to repeated measures of Battelle scores across approximately the first year in the Baby Home that were nested within individuals at Level 2.
Within all Level 1 models, chi-square tests of homogeneity of variance were violated (all p < .001). To correct for this violation, age at assessment was added as a predictor of level 1 variance (equation 1):
| 1) |
The following equation was then used to estimate the Level 1 model:
| 2) |
Here, Battelle scores were expressed as a function of time in the Baby Home centered at two months, which was the average time at first assessment (BHMONTHSij-2), and time-varying PCERA caregiver measures (CGij) and PCERA dyadic engagement measures (DYAD ij). Both PCERA measures were group-mean centered (Raudenbush & Bryk, 2002). Therefore, the intercept represents each individual’s average Battelle score two months after entering the Baby Home, while the coefficients on time in the Baby Home represent change in Battelle scores across assessments, and coefficients on the PCERA measures represent whether within-person changes in how the caregiver engages with the child predicted within-person changes in Battelle scores. εij is the Level 1 random effect for a particular observation.
Between-person effects were then assessed at Level 2 of the HLM models. Variability in the intercept and linear growth terms of Battelle scores were estimated as random effects at Level 2 using Equations 3 and 4 below. PCERA scores were fixed at Level 2.
| 3) |
| 4) |
Variation in baseline Battelle scores and change in Battelle scores over time were explained with the child’s Baby Home of residence (dummy variables T+SCi and TOi with children in NoI as the reference group), family experience (FAMILY<9i and FAMILY≥9i with No-Family children as the reference group), the interaction of Baby Home and family experience variables (BHxFAMILY), and time-invariant demographic characteristics (CHILD/BIRTH, all grand-mean centered). Thus, the Level-2 intercepts refer to children in NoI who had no family experience, TO and T+SC coefficients refer to children within those Baby Homes with no family experience, and FAMILY<9 and FAMILY≥9 coefficients refer to children in NoI with these types of family experience.
To determine whether the BHxFAMILY interaction added significantly to the main effects model, the Deviance statistic of this nested model was compared to that of the main effect only model. The interaction added significantly to the prediction of all baseline Battelle scores and longitudinal change (all p < .05) except the Cognitive subscale intercept, χ2(4) = 7.06, p = .13. Therefore, the BHxFAMILY interaction was not included in the Cognitive subscale intercept but was included in all other Level 2 equations.
In short, these growth models were used to assess two primary questions regarding how young children reared in institutions develop over their first year of residency: (1) Does exposure to the intervention Baby Homes alter cognitive and/or social-emotional development for infants with no exposure to a family environment? And (2) Does spending time with a family prior to entering the Baby Home predict differences in baseline cognitive and/or social-emotional abilities and/or differences in the development of these abilities for children in each Baby Home environment? Within both questions, analyses also addressed whether predictors have differential effects on cognitive vs. social-emotional development.
Results
Preliminary Analyses
Descriptive Results
At the time of baseline, second, and third testing, children had been in the Baby Home for 1.89 (SD = 0.88), 5.06 (SD = 1.54), and 8.18 months (SD = 2.26), respectively (see Table 1). Mean ages at assessment for these three testing periods were 7.83 (SD = 9.16; range = 2.33-37.06), 10.54 (SD = 8.96; range = 4.50-45.89), and 11.56 months (SD = 7.21; range = 6.70-48.42), respectively. The general developmental trends for each outcome measure are described with their unconditional growth models (Table 2). Including children from all Baby Homes, baseline Battelle scores were approximately 2-3 standard deviations below children in the standardization sample (M = 100; SD = 15), but children either developed more quickly than typical or at normative rates.
Table 2.
Unconditional Growth Models for Battelle Scores.
| β | SE | Deviance | |
|---|---|---|---|
| Cognitive | 6322.46 | ||
| Intercept | 73.19*** | 1.37 | |
| Slope | 1.29*** | 0.27 | |
| Communication | 6413.48 | ||
| Intercept | 64.69*** | 1.35 | |
| Slope | −0.15 | 0.29 | |
| Personal-Social | 6261.44 | ||
| Intercept | 57.20*** | 1.25 | |
| Slope | 0.88** | 0.28 |
Note. Deviance – a measure of model fit, lower numbers refer to a better fit (more explained variance) but only within a single model (i.e., compare Deviance here with that in the final model – Table 5).
p < .01
p<.001
Child Demographics
Analyses of variance (ANOVAs) and chi-square tests were conducted to compare children in different Baby Homes and with different family experiences on potential control variables (see Table 3). For Baby Home, contrasts compared T+SC vs. (NoI + TO) and NoI vs. TO. Children in different Baby Homes did not differ on gestational age, gender, or maternal substance use (p > .05). However, 10-minute Apgar scores and FAI total scores showed significant relationships with Baby Home (see Table 3). Whereas children in T+SC tended to have poorer birth circumstances (lower Apgar scores), those in NoI tended to have higher functional disability ratings, excluding children with diagnosed disabilities. For Family Experience, contrasts compared No-Family vs. (Family<9 + Family≥9 months) and Family<9 vs. Family≥9 months. Amount of family experience was not related to gender or Apgar scores (p > .05). However, maternal substance use, FAI total score, and gestational age were significantly related to Family Experience (see Table 3). Children who spent any time with a family were more likely to have a mother who used substances during pregnancy and a longer gestation. Children who spent more than nine months with families also had lower FAI scores. Due to their association with variables of interest, Apgar score, FAI, gestational age, and maternal substance use history were added as covariates in primary analyses.
Table 3.
Child Demographics by Baby Home and Family Experience
| Baby Home | Family Experience | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| NoI | TO | T+SC | No Family | Family <9 | Family≥9 | |
|
|
||||||
| Maternal Substance Use | 47 (49%) | 51 (49%) | 55 (64%) | 96 (49%)a | 22 (54%)b | 35 (71%)b |
| FAI Total | 2.19 (0.37)a | 1.86 (0.37)b | 1.82 (0.34)c | 2.05 (0.35)a | 1.94 (0.35)b | 1.63 (0.43)c |
| Gestation Length (weeks) | 37.30 (2.96) | 37.93 (2.41) | 38.02 (2.44) | 37.43 (2.96)a | 38.41 (1.69)b | 38.44 (1.27)b |
| Apgar 10 min | 8.39 (0.68)a | 8.38 (0.53)a | 8.05 (0.79)b | 8.29 (0.74) | 8.30 (0.39) | 8.27 (0.66) |
| Gender (male) | 50 (53%) | 57 (55%) | 40 (47%) | 102 (52%) | 21 (51%) | 24 (49%) |
Superscripts denote variables that differ at p < .05. For Baby Home, analyses first compared NoI vs. (TO + T+SC) and then TO vs. T+SC. For Family Experience, analyses first compared No Family vs. (Family<9 + Family≥9) and then Family<9 vs. Family≥9.
Caregiver Sensitivity and Consistency During the First Year of Life in Institutions
Table 4 displays the HLM analyses predicting Battelle Cognitive, Communication, and Personal-Social scores.
Table 4.
HLM Analyses Predicting Battelle Outcomes.
| Cognitive | Communication | Personal-Social | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| β | SE | β | SE | β | SE | |
|
|
||||||
| Fixed Effects | ||||||
| Initial status, π0i | ||||||
| Intercept | 73.10*** | 3.11 | 68.45*** | 3.24 | 66.99*** | 2.55 |
| T+SC | 0.30 | 3.69 | −3.09 | 5.52 | −16.02*** | 4.19 |
| TO | −8.09* | 3.66 | −3.49 | 4.36 | −13.58*** | 3.49 |
| Family <9 Months | 5.50 | 3.99 | −11.00† | 5.80 | −16.27** | 5.72 |
| Family ≥9 Months | 1.26 | 3.67 | −7.76 | 4.95 | −6.06 | 4.49 |
| T+SCxFamily<9 | 17.64* | 8.28 | 18.05* | 7.24 | ||
| TOxFamily<9 | 4.07 | 10.81 | 17.95* | 7.42 | ||
| T+SCxFamily≥9 | 5.79 | 6.97 | 24.37*** | 6.44 | ||
| TOxFamily≥9 | −3.97 | 6.99 | 6.99 | 7.03 | ||
| Gender (ce) | −0.39 | 2.53 | −0.002 | 2.63 | −2.57 | 2.28 |
| M. Substance (ce) | −0.22 | 2.67 | −0.50 | 2.79 | −5.81* | 2.36 |
| FAI total (ce) | −11.83** | 3.93 | −14.78*** | 4.06 | −8.38* | 3.49 |
| Gestation Age (ce) | 2.66*** | 0.53 | 1.48** | 0.56 | 2.18*** | 0.43 |
| Apgar 10 Min (ce) | 3.68† | 1.91 | 0.94 | 1.69 | 1.57 | 1.49 |
| Time in the Baby Home, π1i | ||||||
| Intercept | 0.39 | 0.70 | −2.67*** | 0.68 | −2.20*** | 0.63 |
| T+SC | 1.91* | 0.94 | 4.44*** | 1.11 | 5.34*** | 0.88 |
| TO | 3.22*** | 0.86 | 2.51* | 0.99 | 3.33*** | 0.87 |
| Family <9 Months | −0.64 | 0.92 | 2.18* | 1.10 | 2.71** | 1.04 |
| Family ≥9 Months | 0.53 | 1.00 | 3.88*** | 1.00 | 3.48*** | 0.82 |
| T+SCxFamily<9 | −0.05 | 1.15 | −3.56* | 1.81 | −2.79* | 1.38 |
| TOxFamily<9 | −2.69* | 1.32 | −1.43 | 2.36 | −3.64* | 1.46 |
| T+SCxFamily≥9 | −1.71 | 1.05 | −4.88*** | 1.35 | −5.45*** | 1.05 |
| TOxFamily≥9 | −4.11*** | 1.05 | −3.53** | 1.35 | −3.86** | 1.31 |
| Gender (ce) | 0.11 | 0.49 | 0.03 | 0.52 | 1.04* | 0.45 |
| M. Substance (ce) | −0.35 | 0.62 | −0.22 | 0.61 | 0.50 | 0.49 |
| FAI total (ce) | −1.72* | 0.78 | 0.71 | 0.85 | −1.16† | 0.67 |
| Gestation Age (ce) | −0.19 | 0.12 | −0.09 | 0.11 | −0.19* | 0.09 |
| Apgar 10 Min (ce) | −0.16 | 0.40 | 0.78* | 0.37 | 0.29 | 0.34 |
| PCERA Caregiver Total, π2i | ||||||
| Intercept | −7.44* | 2.91 | −0.88 | 2.76 | 0.17 | 2.28 |
| PCERA Dyad, π4i | ||||||
| Intercept | 5.09* | 2.09 | 0.46 | 1.69 | 2.13 | 1.55 |
| Goodness of Fit | ||||||
| Deviance | 6163.86*** | 6251.16*** | 6061.92*** | |||
Note. The intercept term refers to No-Family children in NoI (No Intervention). T+SC = Training plus Structural Change intervention. TO = Training only intervention. Family <9 Months = children who spent some time but less than 9 months with a family before Baby Home entry. Family ≥9 Months = children who spent 9 or more months with a family before Baby Home entry. (ce) denotes variables that have been centered. M. Substance = documented maternal substance use during pregnancy. FAI total = Functional Abilities Index Total Score. Blank cells occur when including interactions did not improve model fit.
p < .001
p < .01
p < .05
p < .10
The first analyses focused only on the first three variables (Intercept, T+SC, and TO), which represent children who spent no time with their families prior to entering NoI, T+SC, and TO, respectively. Because all No-Family children entered the Baby Homes before 3 months of age, the slope term (Time in the Baby Home) corresponds both to their first year in the Baby Home and to approximately their first year of life.
Baseline
Children had similar baseline Communication abilities across Baby Homes (all p > .05), but differed in Battelle Personal-Social and Cognitive scores at baseline assessments (see Table 4 – Initial Status). At baseline, children in TO and T+SC had Personal-Social scores approximately 1 SD lower than children in NoI; however, children in TO and T+SC did not differ, χ2(1) = 0.35, p > .50. Children in TO displayed Cognitive scores approximately .5 SD lower than children in NoI(see Table 4). The Cognitive ability scores of children in T+SC were 8.39 points higher than those in TO, χ2(1) = 5.38, p = .02, but not different than children’s scores in NoI.
NoI (Insensitive/Inconsistent)
Longitudinally, Personal-Social and Communication scores of children in NoI decreased by 2.20 and 2.67 points per month, respectively (see Figure 1, Table 4 – Time in the Baby Home). Thus, children’s standardized scores decreased by 1 SD within 6 - 7 months, suggesting that they develop these skills slower than same-aged non-institutionalized peers of similar starting skill levels. Regarding Cognitive scores, children’s rates of developmental change in NoI were not significantly different than 0 (see Figure 1, Table 4).
Figure 1.

Developmental trajectories (predicted values based on HLM analyses) of Battelle Cognitive, Communication, and Personal-Social scores during the first eight months of residency for children with no family experience in NoI, TO, and T+SC.
TO (Sensitive/Inconsistent)
Longitudinally in TO, children’s Personal-Social and Communication scores showed no significant change over time. They had typical rates of development (Personal-Social: simple slope = 1.13, t(271) = 1.77, p = .08; Communication: simple slope: −0.15, t(271) = −0.21, p > .50), as opposed to the decreases seen in NoI (see Figure 1). With the decreases in NoI, children in TO had scores approximately 1 SD above those in NoI after approximately 12 months for Personal-Social scores and after 5-6 months for Communication scores. For Cognitive scales, children in TO displayed faster than typical rates of development, improving 3.22 standard points per month more than children in NoI (see Table 4, Figure 1), resulting in scores approximately .5 SD above NoI after approximately 5-6 months of residency.
T+SC (Sensitive/Consistent)
Longitudinally for children in T+SC, Personal-Social, Cognitive, and Communication scores improved at a rate of 5.34, 1.91, and 4.44, respectively, points per month more than children in NoI (see Figure 1, Table 4). At this rate, children in T+SC improved their Personal-Social and Communication scores by 1 SD and their Cognitive scores by about .5 SD above children in NoI after 5-6 months of residency. There were no differences between children in TO and T+SC for Cognitive, χ2(1) = 1.92, p = .16, scores. Although the comparison with TO was not significant for Communication, χ2(1) = 2.93, p = .08., T+SC children’s scores increased by 1.77 points/month, t(271) = 2.08, p = .04. However, on Personal-Social scales, children in T+SC gained 2.01 points per month more than children in TO, χ2(1) = 4.95, p = .02, resulting in scores 1 SD higher than those in TO after approximately 8 months in the Baby Home.
Interaction of Family Experience and Baby Home Intervention
The HLM models also addressed whether spending time with a family prior to entering the Baby Home predicted differences in baseline cognitive and social-emotional abilities and/or differences in the development of these abilities for children in each Baby Home environment. Lines 4 through 9 of both Initial Status and Time in the Baby Home in the HLM analyses (Table 4) address these questions.
Baseline
The relation of family experience to baseline scores differed by Battelle scale, with no association for Cognitive or Communication scales but generally higher scores on Personal-Social scales for children who spent more time with families. Specifically, on the Personal-Social scale, there were no differences between children who spent at least versus less than 9 months with families in NoI or TO (both p > .10). In TO, No-Family children also did not differ from children who spent any time with their families (both p > .50). Children who entered NoI after less than 9 months with their family, however, had scores approximately 1 SD lower than No-Family children (see Table 4), whereas there was no difference between those who spent no time versus at least 9 months with their families. Children in T+SC who spent less than 9 months with their families had similar baseline Personal-Social scores as No-Family children, t(271) = 0.39, p > .50; whereas those who spent at least 9 months with their families had Personal-Social scores over 1 SD higher than children who both spent no time, t(271) = 3.74, p < .001, or less than nine months, χ2(1) = 12.70, p < .001, with their families (see Figure 4).
Figure 4.

Developmental trajectories (predicted values based on HLM analyses) of Battelle Personal-Social scores for children in NoI, TO, and T+SC with varying family experiences.
In contrast, there were no differences between Family and No-Family children (see Table 4) or between children who spent at least vs. less than nine months with families (all p > .05) on Cognitive or Communication scores at baseline. The single exception was that children who spent at least nine months with their families before entering TO had Communication scores approximately .67 SD lower than children who had entered TO with no family experience, t(271) = −1.99, p = .047 (see Figures 2 & 3).
Figure 2.

Developmental trajectories (predicted values based on HLM analyses) of Battelle Cognitive scores of children in NoI, TO, and T+SC with varying family experiences.
Figure 3.
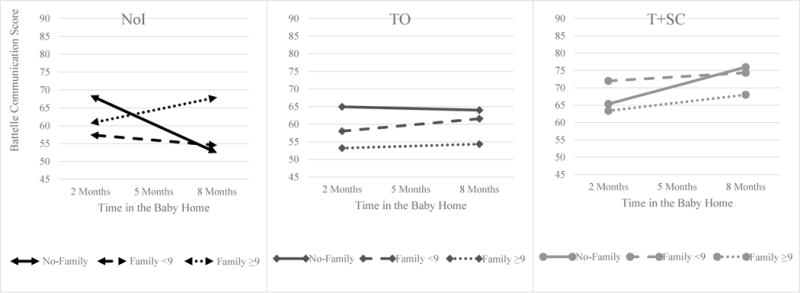
Developmental trajectory (predicted values based on HLM analyses) of Battelle Communication scores of children in NoI, TO, and T+SC with varying family experiences.
NoI (Insensitive/Inconsistent)
Longitudinally, family experience related to better outcomes for children in NoI on Personal-Social and Communication scales but not Cognitive Scales. Specifically, Family children showed similar, stable developmental trends as No-Family children on Cognitive scales (all p > .25; see Figure 2 – Panel 1). Children who spent at least vs. less than 9 months with their families also did not differ on the Personal-Social or Communication scales (all p > .15). However, they had rates of development approximately 2-3 points/month higher than No-Family children by not showing the decline over time seen in No-Family children (see Figures 3 & 4 - panel 1).
TO (Sensitive/Inconsistent)
Longitudinally for all measures, children in TO who spent any amount of time with a family displayed typical rates of development. There were no differences between those who spent at least vs. less than 9 months with a family on Personal-Social, Cognitive, or Communication scores, and no simple slopes were significantly different from 0 (all p > .50; see Figures 2, 3, 4 – Panel 2). On the Personal-Social and Communication scales, there was also no difference between Family and No-Family groups (all p > .50). However, on the Cognitive scale, this typical development resulted in approximately 3 points/month less than the increase in scores seen for No-Family children (all p < .008; see Figure 2 – Panel 2).
T+SC (Sensitive/Consistent)
Longitudinally children in T+SC reached similar standard scores for all measures, regardless of family experience, after only 6-8 months in the Baby Home. Children who spent at least and less than 9 months with families showed similarly faster than typical rates of Cognitive and Communication development as No-Family children and each other (all p > .20; see Figures 2 & 3 – Panel 3). Children who spent less than 9 months with a family showed similar increases in Personal-Social scores over time as No-Family children, (all p > .30; see Figure 4 – Panel 3). However, although they entered the Baby Home with higher baseline scores, children who spent at least 9 months with their families gained about 2-3 points/month less than children who spent less or no time with families on Personal-Social scores (all p < .01).
Child and Caregiver Factors
Child Demographics
As expected, children with a history of prenatal substance exposure, higher levels of assessed functional disabilities, and younger gestational ages had lower scores at baseline (see Table 4 – Initial Status control variables). Interestingly, child characteristics also had some association with developmental change. Boys’ Personal-Social skills increased at a rate of 1.04 points per month more than girls’, corresponding to a .5 standard deviation difference in scores between boys and girls after 7 months of Baby Home exposure. Younger than average gestational age was also related to faster rates of growth than older gestational age, possibly due to catch-up.
Caregiver Behaviors and Dyadic Engagement
The quality of caregiver positive social behaviors and dyadic engagement during a free play session, time-varying predictors, were not related to child Communication or Personal-Social skills, as assessed with structured questions, interviews, and observations, above and beyond differences accounted for by Baby Home, family experience, or child demographics(see Table 4). On the Cognitive scale, caregiver behaviors becoming more positive appeared to be related to within-person decreases in Cognitive skills, but dyadic engagement becoming more positive was related to within-person increases in Cognitive skills (see Table 4).
Discussion
The current study assessed the effects of an intervention that improved caregiver sensitivity only or sensitivity plus consistency within Baby Homes for children who experienced only these environments versus those who lived with families prior to institutionalization. It also assessed the influence of birth circumstances on subsequent development. Interestingly, most of the birth circumstances were related to baseline scores but not to developmental growth, suggesting that the Baby Home environment has a stronger influence on subsequent development than early birth complications.
Sensitivity and Consistency during the First Year of Institutionalization
For children without family experience, the interventions provide one of the purest assessments of the impact of caregiving on development within a high-risk sample. Two primary findings emerge from this sample. First, social-emotional skills are supported more when caregivers are both sensitive and consistent (i.e., T+SC) than sensitive but inconsistent (i.e., TO). Second, caregiver sensitive and response-contingent interactions support cognitive development during the first year of institutionalization regardless of caregiver consistency (i.e., TO is equivalent to T+SC).
Social-Emotional Development
Children in T+SC gained more personal-social skills per month than children in NoI and TO. These skills are precisely the types of behaviors that the intervention targeted and that would be expected to flourish within an environment of caregiver consistency and sensitivity (Rutter, 1979; St. Petersburg-USA Orphanage Research Team, 2008).
Caregiver sensitivity without consistency (TO) was also better able to support the development of personal-social behavior than insensitive and inconsistent care (NoI). Sensitivity alone (TO) helped children develop personal-social skills at a rate similar to that of non-institutionalized children their age and starting ability level (i.e., no change in standard score), at least for the first year of institutionalization, but not improve from their initially low standard scores. Potentially, children have more difficulty forming expectations about and consistent ways of behaving in social interactions when the person with whom they interact frequently changes. The lack of consistency may create difficulty for infants to learn how to discriminate between familiar and unfamiliar persons, to express different emotions, or to show affection (items from the Battelle Personal-Social scale) because caregivers generally are unfamiliar and may express and respond to emotions and affection differently. Conversely, without sensitivity or consistency (NoI), children developed fewer skills with age than non-institutionalized children, supporting the proposition that social-emotional neglect not only does not support contemporaneous functioning but actually impedes children’s subsequent social-emotional development (Naughton et al., 2013; Van IJzendoorn et al., 2011).
Cognitive Development
The NoI environment was related to slower than typical rates of communication development, consistent with the literature on responsive interactions (Sachs & Johnson, 1976; Snow et al., 1976). Children in NoI displayed typical rates of cognitive skill acquisition; however, they maintained very low standard scores (nearly 2 SD below average) and gained skills more slowly than children in TO and T+SC. Children learn through interactions (Weinfield, Sroufe, Egeland, & Carlson, 1999), and without this basic foundation, many areas of development seem to suffer.
The T+SC intervention produced the hypothesized faster than typical rates of cognitive skill acquisition, but the TO intervention also produced faster rates of skill acquisition than expected. That this strictly social-emotional intervention positively impacted children’s cognitive and communication development supports the literature documenting direct associations between parent-infant interactions and later intelligence and language abilities (Bornstein, 2014; Lunden & Silven, 2011; Pearson et al., 2011). Interestingly, these findings suggest that sensitive and response-contingent interactions with adults in general (even when the adults change over time) seem to be primary contributors to the observed association between caregiver-child interactions and rates of cognitive skill acquisition during the first year of life for children raised in institutions.
Family Experience Prior to Institutionalization
Children who lived with families prior to institutionalization presumably had more opportunities to engage in one-on-one interactions with consistent adults; however, the quality of these interactions is unknown and likely poor in many cases, and the children suffered the loss of these relationships upon institutionalization. Results suggest that the relation of this family experience to development within the Baby Homes depends upon the subsequent environment. Early family experience appears to protect children from the negative effects of a social-emotionally depriving Baby Home environment (NoI). However, with sensitive but inconsistent caregivers (TO), family experience kept the children from benefitting from the enhanced caregiving quality as much as children without family experience, possibly related to the loss of caregiver consistency. Within the T+SC intervention, results support the importance of early caregiver consistency for social-emotional development and caregiver sensitivity for cognitive development.
Maintenance of Standard Ability Levels in TO and NoI
Children who spent any amount of time with their families and then entered an environment without consistent caregivers (TO & NoI) showed typical rates of development on Battelle measures. The early family experience seemed both to protect children from the negative effects of NoI and to hinder children from attaining the positive effects of TO. The behavioral patterns that children who entered NoI learned in their families, even in as few as 3 months, may have promoted caregiver interaction or individual exploration at least enough to acquire new social-emotional and cognitive skills at the same rate as non-institutionalized children their age and initial ability level rather than acquiring these skills at slower rates. Indeed, these may be the children who use their social abilities to initiate interactions and to make interactions more rewarding for caregivers or who, through fussiness, demand the attention they need from caregivers (Bakermans-Kranenburg et al., 2011). Conversely, children in TO with family experience did not obtain the same cognitive benefits from the caregivers’ sensitive and response-contingent interactions as children who had only known the TO environment. Perhaps the loss of consistent family interactions followed by the confusion of having many changing caregivers kept them from excelling within this environment.
These findings could also suggest that the institutional environment has a larger effect on development during the first year of life than at later ages (i.e., children with family experience were older during the first year of institutionalization). However, some children with less than 9 months of family experience overlapped with No-Family children on both timing of exposure and age at assessment. That they showed rates of development more similar to children with at least 9 months of family experience than to children without family experience suggests that spending time with a family is an important predictor beyond timing of exposure and age.
Family Care before T+SC
Children who spent at least 9 months with their families benefitted more from their family experience than the T+SC intervention on social-emotional measures; however, they benefitted more from the T+SC intervention than family experience for cognitive measures. This conclusion is consistent with findings about the relative impact of caregiver sensitivity versus consistency in the No-Family sample. Children who spent at least 9 months with their families by definition entered T+SC at older ages than other children. Cognitive scores increased with age for children in T+SC who entered at younger ages. Therefore, children with at least 9 months of family experience were hypothesized to enter the Baby Home with higher scores than other children, assuming their early development followed similar trajectories as No-Family children. Instead, children with at least 9 months of family experience in T+SC had similar baseline cognitive scores and gained cognitive and communication skills at a similar rate as children with less or no family experience during their Baby Home residency. Perhaps this is more evidence that caregiver sensitivity and the quality of response-contingent interactions are more associated with early cognitive skill acquisition than the consistency of caregivers (Rutter, 1979).
In contrast, consistency again appeared especially salient for social-emotional development. Attachment theory predicts that the combination of consistency and sensitivity is the best environment for social-emotional skill development, but that of the two, consistency may be more important in this domain (Ainsworth et al., 1978; Bowlby, 1969; Rutter, 1979). The environment of consistency with unknown caregiver sensitivity in a family offered the opportunity to develop a discriminated attachment of unknown quality for children who remained with their families for at least 9 months. Within the family, children gained social-emotional skills at a pace presumably similar to children living in T+SC (i.e., children who spent at least 9 months with their families had higher scores at baseline). However, after entering T+SC, they gained skills slower than their Baby Home peers but continued to improve. This finding may be due to the loss of their attachment figure(s) and their difficulty gaining as much from new relationships in the Baby Home as children for whom the caregivers constituted their only primary relationships. Conversely, it may be that the T+SC intervention can support a certain level of development and that children who had spent more time with their families were closer to that level, with less room for improvement.
Expansion of the Original Intervention Report
The current study expands upon the original intervention report by using an analytic method that assessed developmental trajectories of individual children and by including family experience as a predictor. The initial report compared children with 4-9 months of Baby Home exposure and 9+ months of exposure (St. Petersburg-USA Orphanage Research Team, 2008). In these analyses, children in T+SC had higher scores on all Battelle scales than children in NoI and TO, and improved more with longer exposure.
In the current study, the intervention effects were more prominent, especially in TO, during the first year of institutionalization among children whose only early rearing environment was the Baby Home. Conversely, children in NoI who had family experience performed better over time than children without this experience, increasing the average scores in NoI, whereas, children in TO with family experience performed more poorly over time than children without this experience, decreasing the average scores in TO. Thus, when pre-institutional family experience is not considered, the true beneficial effects of training caregivers to be more sensitive, responsive, and child-directed in their interactions is masked in TO, as are the negative effects of social-emotional deprivation from birth in NoI.
Implications
Most professionals would agree that the best place to raise a child is in a warm, loving, stable family; however, when living with one’s family of origin is not feasible or desirable, child welfare systems often must provide for children by placing them into foster care or institutions. Children in foster care tend to have better developmental outcomes than children in institutions (Julian & McCall, 2011; Zeanah, Smyke, Koga, & Carlson, 2005), and a transition to entirely family-based care (i.e., support to keep children with parents, foster care, adoption) would be the most inexpensive and developmentally beneficial long-term solution for vulnerable children (Engle et al., 2011; McCall, 2011). Some government-level transitions to family-based rather than institutional care have been quite successful, such as in the Republic of Georgia (Greenberg & Partskhaladze, 2014) and parts of Russia (Johnson, Dovbnya, Morozova, Richards, & Bogdanova, 2014). However, such successes require multiple supportive circumstances that will not often be met in most countries, and therefore many children likely will be reared in institutions in the foreseeable future.
The current study demonstrates the negative impact of institutional rearing; however, it also suggests that institutional environments can be improved to foster better child development. The T+SC intervention consisted of changes mimicking a good family environment and produced substantial improvements in children’s development. Training caregivers to be more sensitive and responsive to children can lessen some of the deleterious consequences of traditional institutional care and improve children’s acquisition of cognitive skills. If, in addition to training in sensitivity and responsiveness, the physical environment and caregiver schedules are adjusted to promote consistency, children display additional gains in social-emotional and communication skills. These findings suggest that every effort should be made to transition children out of institutional care, but that the quality of life in institutions can be improved during the transition to family care and for those who must remain in institutions.
Strengths and Limitations
The current study uses data from the most comprehensive intervention of care within three working institutions. Unlike “add-on” interventions (e.g., Brossard & Decarie, 1971; Sparling, Dragomir, Ramey, & Florescu, 2005; Taneja et al., 2002), this design changes the institutional culture and the quality of care children receive from the institutional staff rather than only during specific designated intervention activities from specially trained non-staff. It also allows a more comprehensive test of theory than some interventions (e.g., Smyke, Dumitrescu, & Zeanah, 2002; Lecannelier, Silva, Hoffmann, Melo, & Morales, 2014), because the inclusion of both TO and T+SC interventions can address the relative impact of caregiver sensitivity versus sensitivity in the context of consistency. Further, it demonstrates that it is feasible to implement interventions to improve child outcomes within the institutional context, not only in foster care (Rutter, 2008).
These strengths are possible only because of the applied nature of the work; however, applied fieldwork always has its limitations. Specifically, sample sizes in the current study are small in certain family groups and for the third assessment. Children cannot be randomly assigned to enter the Baby Home after birth vs. spending different amounts of time with families. Thus, the child and family characteristics that lead to these placements cannot be controlled. Children’s birth and disability characteristics were included statistically to address group differences; however, other unmeasured factors may impact results, including whether children had insecure or disorganized attachments in their biological families or experienced abuse, neglect, and/or parental substance use. Future research should further examine these factors and address their impact on later development within institutions. Additionally, while the choice to use 9 months as a cut-off for time with a family was largely based on attachment theory, other factors (e.g., the delayed nature of the sample, sample sizes) also impacted this decision. Future research should further address the differences between children placed earlier versus later to determine whether 9 months is the most appropriate age predictor, or whether differences in outcomes could be predicted more sensitively with a different age cut-off.
Some children also left the Baby Homes for adoption or reunification, resulting in some being omitted from the study and others contributing only two assessments during their residency. Although selective adoption, which could lead to biased results, is possible, a study of children in these Baby Homes found that the length of institutionalization and pre-institutional family experience (i.e., children arrive later and are adopted at older ages) were the only factors related to age at adoption (Hawk et al., 2012). The HLM analyses are able to compensate for missing data, mitigating the effects of the limited number of children with three assessments.
With all measures it becomes more difficult to obtain reliable and valid assessment data the younger a child is. Given the age of this sample, it will be important for future studies to replicate these findings. Given the overlap in children’s development of cognitive and social-emotional skills, future research should look at more sensitive measures of cognition and social-emotional development, and perhaps the interaction of the two under similar circumstances.
Finally, only three Baby Homes were assessed in this study. Similar T+SC interventions have been implemented in Latin America with similarly positive outcomes (Groark et al., 2013; McCall et al., 2010), and follow-up studies of the current intervention showed that the intervention could be sustained with no external financial support for at least six years (McCall, Groark, Fish, Muhamedrahimov, Palmov, & Nikiforova, 2013). However, future research should assess the feasibility of implementing the T+SC intervention in other orphanages and in other countries, as well as assess intervention outcomes. In addition to child data, future studies should include providers’ and administrators’ perspectives regarding how to change and sustain such a cultural shift within the institution.
Acknowledgments
This project supported by grants HD050212 and HD39017 from the Eunice Shriver Kennedy National Institute of Child Health and Human Development to authors McCall and Groark. The interpretations and opinions expressed in this paper are those of the authors, not the funder.
Contributor Information
Brandi N. Hawk, University of California, Davis
Robert B. McCall, University of Pittsburgh
Christina J. Groark, University of Pittsburgh
Rifkat J. Muhamedrahimov, St. Petersburg State University
Oleg I. Palmov, St. Petersburg State University
Natalia V. Nikiforova, Baby Home 13, St. Petersburg, Russian Federation
References
- Ainsworth MDM, Blehar MC, Waters E, Wall S. Patterns of attachment. Hillsdale, NJ: Erlbaum; 1978. [Google Scholar]
- Bakermans-Kranenburg MJ, van IJzendoorn MH, Juffer F. Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin. 2003;129:195–215. doi: 10.1037/0033-2909.129.2.195. [DOI] [PubMed] [Google Scholar]
- Bakermans-Kranenburg MJ, Steele H, Zeanah CH, Muhamedrahimov RJ, Vorria P, Dobrova-Krol NA, Gunnar MR. Attachment and emotional development in institutional care: Characteristics and catch-up. Monographs of the Society for Research in Child Development. 2011;76:62–91. doi: 10.1111/j.1540-5834.2011.00628.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernier A, Carlson SM, Deschenes M, Matte-Gagne C. Social factors in the development of early executive functioning: A closer look at the caregiving environment. Developmental Science. 2012;15:12–24. doi: 10.1111/j.1467-7687.2011.01093.x. [DOI] [PubMed] [Google Scholar]
- Bernier A, Carlson SM, Whipple N. From external regulation to self-regulation: Early parenting precursors of young children’s executive functioning. Child Development. 2010;81:326–339. doi: 10.1111/j.1467-8624.2009.01397.x. [DOI] [PubMed] [Google Scholar]
- Biederman J, Monuteaux MC, Doyle AE, Seidman LJ, Wilens TE, Ferrero F, Faraone SV. Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. Journal of Consulting and Clinical Psychology. 2004;72:757. doi: 10.1037/0022-006X.72.5.757. [DOI] [PubMed] [Google Scholar]
- Bornstein MH. Human infancy … and the rest of the lifespan. Annual Reviews of Psychology. 2014;65:121–158. doi: 10.1146/annurev-psych-120710-100359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowlby J. Attachment and loss: Vol 1 Attachment. New York: Basic Books; 1969. [Google Scholar]
- Brossard M, Decarie TG. The effects of three kinds of perceptual-social stimulation on the development of institutionalized infants: preliminary report of a longitudinal study. Early Child Development and Care. 1971;1:111–130. [Google Scholar]
- Caldwell BM, Bradley RH. Home observation for measurement of the environment. Little Rock: University of Arkansas at Little Rock; 1984. [Google Scholar]
- Carlson SM, Wang TS. Inhibitory control and emotion regulation in preschool children. Cognitive Development. 2007;22:489–510. [Google Scholar]
- Chisholm K. A three year follow-up of attachment and indiscriminate friendliness in children adopted from Romanian orphanages. Child Development. 1998;69:1092–1106. [PubMed] [Google Scholar]
- Clark C, Prior M, Kinsella G. The relationship between executive function abilities, adaptive behaviour, and academic achievement in children with externalising behaviour problems. Journal of Child Psychology and Psychiatry. 2002;43:785–796. doi: 10.1111/1469-7610.00084. [DOI] [PubMed] [Google Scholar]
- Clark R. Unpublished manuscript. University of Wisconsin Madison Department of Psychiatry; Madison, WI: 1985. Early parent-child relationship assessment. [Google Scholar]
- Engle PL, Groza VK, Groark CJ, Greenberg A, Bunkers KM, Muhamedrahimov RJ. The situation for children without parental care and strategies for policy change. Monographs of the Society for Research in Child Development. 2011;76:190–222. Serial No. 301. [Google Scholar]
- Greenberg AL, Partskhaladze N. How the Republic of Georgia has nearly eliminated the use of institutional care for children. Infant Mental Health Journal. 2014;35:185–191. doi: 10.1002/imhj.21434. [DOI] [PubMed] [Google Scholar]
- Groark CJ, McCall RB, McCarthy SK, Eichner JC, Warner HA, Salaway J, Lopez ME. The effects of a social–emotional intervention on caregivers and children with disabilities in two Central American institutions. Infants & Young Children. 2013;26:286–305. [Google Scholar]
- Guidubaldi J, Perry JD. Concurrent and predictive validity of the Battelle Development Inventory at the first grade level. Educational and psychological measurement. 1984;44:977–985. [Google Scholar]
- Hale-Jinks C, Knopf H, Kemple K. Tackling teacher turnover in child care: Understanding causes and consequences, identifying solutions. Childhood Eduction. 2006;82:219–226. [Google Scholar]
- Hawk B, McCall RB, Groark CJ, Muhamedrahimov RJ, Palmov OI, Nikoforova NV. Age at adoption: A measure of time in the orphanage or child-specific factors. Adoption Quarterly. 2012;15(1):18–34. [Google Scholar]
- Hermanau K, Hecker T, Elbert T, Ruf-Leuschner M. Maltreatment and mental health in institutional care – Comparing early and late institutionalized children in Tanzania. Infant Mental Health Journal. 2014;35:102–110. doi: 10.1002/imhj.21440. [DOI] [PubMed] [Google Scholar]
- Horm DM, File N, Bryant D, Burchinal M, Raikes H, Forestieri N, Cobo-Lewis A. Associations between continuity of care in infant-toddler classrooms and child outcomes. Early Childhood Research Quarterly. 2018;42:105–118. [Google Scholar]
- Johnson DE, Dovbnya SV, Morozova TU, Richards MA, Bogdanova JG. From institutional care to family support: Development of an effective early intervention network in the Nizhny Novgorod region, Russian Federation, to support family care for children at risk for institutionalization. Infant Mental Health Journal. 2014;35:172–184. doi: 10.1002/imhj.21433. [DOI] [PubMed] [Google Scholar]
- Johnson LJ, Cook MJ, Kullman AJ. An examination of the concurrent validity of the Battelle Developmental Inventory as compared with the Vineland Adaptive Scales and the Bayley Scales of Infant Development. Journal of Early Intervention. 1992;16:353–359. [Google Scholar]
- Julian MM, McCall RB. The development of children within alternative residential care environments. International Journal of Child and Family Welfare. 2011;3:119–147. [Google Scholar]
- Kochanska G, Murray KT, Harlan ET. Effortful control in early childhood: Continuity and change, antecedents, and implications for social development. Developmental Psychology. 2000;36:220–232. [PubMed] [Google Scholar]
- Lecannelier F, Silva JR, Hoffmann M, Melo R, Morales R. Effects of an intervention to promote socioemotional development in terms of attachment security: A study in early institutionalization in Chile. Infant Mental Health Journal. 2014;35:151–159. doi: 10.1002/imhj.21436. [DOI] [PubMed] [Google Scholar]
- McCall RB. Research, practice, and policy perspectives on issues of children without permanent parental care. Monographs of the Society for Research in Child Development. 2011;76:223–272. doi: 10.1111/j.1540-5834.2011.00634.x. Serial No. 301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCall RB, Groark CJ, Fish L, Harkins D, Serrano G, Gordon K. A socioemotional intervention in a Latin American orphanage. Infant Mental Health Journal. 2010;31:521–542. doi: 10.1002/imhj.20270. [DOI] [PubMed] [Google Scholar]
- McCall RB, Groark CJ, Fish L, Muhamedrahimov RJ, Palmov OI, Nikiforova NV. Maintaining a social‐emotional intervention and its benefits for institutionalized children. Child Development. 2013;84:1734–1749. doi: 10.1111/cdev.12098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muhamedrahimov RJ. New attitudes: Infant care facilities in Saint-Petersburg (Russia) In: Osofsky JD, Fitzgerald HE, editors. WAIMH handbook of infant mental health. Vol. 1. New York: Wiley; 2000. pp. 247–294. [Google Scholar]
- Muhamedrahimov RJ, Palmov OI, Istomina LA. Unpublished manual. St Petersburg State University, Russian Federation; 2000. The Functional Abilities Index. [Google Scholar]
- Naughton AM, Maguire SA, Mann MK, Lumb RC, Tempest V, Gracias S, Kemp AM. Emotional, behavioral, and developmental features indicative of neglect or emotional abuse in preschool children: A systematic review. JAMA Pediatrics. 2013;167:769–775. doi: 10.1001/jamapediatrics.2013.192. [DOI] [PubMed] [Google Scholar]
- Newborg J, Stock JR, Wnek L, Guidubaldi J, Svinicki J. Battelle developmental inventory. Allen, Tex: DLM; 1988. [Google Scholar]
- Oliveira PS, Soares I, Martins C, Silva JR, Marques S, Baptista J, Lyons-Ruth K. Indiscriminate behavior observed in the strange situation among institutionalized toddlers: Relations to caregiver report and to early family risk. Infant Mental Health Journal. 2012;33:187–196. doi: 10.1002/imhj.20336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oosterman M, Schuengel C, Slot NW, Bullens RAR, Doreleijers TAH. Disruptions in foster care: A review and meta-analysis. Children and Youth Services Review. 2007;29:53–76. [Google Scholar]
- Pearson RM, Heron J, Melotti R, Joinson C, Stein A, Ramchandani PG, Evans J. The association between observed non-verbal maternal responses at 12 months and later infant development at 18 months and IQ at 4 years: A longitudinal study. Infant Behavioral Development. 2011;34:525–533. doi: 10.1016/j.infbeh.2011.07.003. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical Linear Models: Applications and data analysis methods. Thousand Oaks, CA: Sage; 2002. [Google Scholar]
- Raudenbush SW, Bryk AS, Cheong YF, Congdon RT, Jr, du Toit M. HLM 7: Hierarchical Linear and Nonlinear Modeling. Scientific Software International, Inc; Lincolnwood, IL: 2011. [Google Scholar]
- Rutter M. Maternal deprivation, 1972-1978: New findings, new concepts, new approaches. Child Development. 1979;50:283–305. [PubMed] [Google Scholar]
- Rutter M. Institutional effects on children: Design issues and substantive findings. Monographs of the Society for Research in Child Development. 2008;73(3):271–278. doi: 10.1111/j.1540-5834.2008.00497.x. [DOI] [PubMed] [Google Scholar]
- Sachs JS, Johnson M. Language development in a hearing child of deaf parents. In: von Raffler Engel W, LeBrun Y, editors. Baby talk and infant speech (Neurolinguistics 5) Amsterdam, NE: Swets & Zeitlinger; 1976. pp. 246–252. [Google Scholar]
- Simeonsson RJ, Bailey DB. The abilities index. Chapel Hill, NC: Frank Porter Graham Child Development Center; 1991. [Google Scholar]
- Smyke AT, Dumitrescu A, Zeanah CH. Attachment disturbances in young children. I: The continuum of caretaking casualty. Journal of the American Academy of Child and Adolescent Psychiatry. 2002;41:972–982. doi: 10.1097/00004583-200208000-00016. [DOI] [PubMed] [Google Scholar]
- Snow CE, Arlman-Rupp A, Hassing Y, Jobse J, Joosten J, Vorster J. Mother’s speech in three social classes. Journal of Psycholinguistic Research. 1976;5:1–20. [Google Scholar]
- Sparling JJ, Dragomir C, Ramey SL, Florescu L. An educational intervention improves developmental progress of young children in a Romanian orphanage. Infant Mental Health Journal. 2005;26:127–142. doi: 10.1002/imhj.20040. [DOI] [PubMed] [Google Scholar]
- Sroufe LA. Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development. 2005;7:349–367. doi: 10.1080/14616730500365928. [DOI] [PubMed] [Google Scholar]
- St. Petersburg-USA Orphanage Research Team. Characteristics of children, caregivers, and orphanages for young children in St. Petersburg, Russian Federation. Applied Developmental Psychology. 2005;26:477–506. [Google Scholar]
- St. Petersburg-USA Orphanage Research Team. The effects of early social-emotional and relationship experience on the development of young orphanage children. Monograph of the Society for Research in Child Development. 2008;73:1–262. doi: 10.1111/j.1540-5834.2008.00483.x. Serial No. 291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taneja V, Sriram S, Beri RS, Sreenivas V, Aggarwal R, Kaur R, et al. ‘Not by bread alone’: Impact of a structured ninety-minute play session on development of children in an orphanage. Child: Care, Health, and Development. 2002;28:95–100. doi: 10.1046/j.1365-2214.2002.00246.x. [DOI] [PubMed] [Google Scholar]
- UNICEF. Progress for children: A report card on child protection. New York: Author; 2009. No.8. [Google Scholar]
- van der Sluis S, de Jong PF, van der Leij A. Executive functioning in children, and its relations with reasoning, reading, and arithmetic. Intelligence. 2008;35:427–449. [Google Scholar]
- Van IJzendoorn MH, Palacios J, Sonuga-Barke EJS, Gunnar MR, Vorria P, Juffer F. Children in institutional care: Delayed development and resilience. Monographs of the Society for Research in Child Development. 2011;76:8–30. doi: 10.1111/j.1540-5834.2011.00626.x. Serial No. 301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinfield NS, Sroufe LA, Egeland B, Carlson EA. The nature of individual differences in infant-caregiver attachment. In: Cassidy Jude, Shaver Phillip R., editors. Handbook of attachment: Theory, research, and clinical applications. New York: Guilford Press; 1999. pp. 68–88. [Google Scholar]
- Zeanah CH, Smyke AT, Koga SF, Carlson E. Attachment in institutionalized and community children in Romania. Child Development. 2005;76:1015–1028. doi: 10.1111/j.1467-8624.2005.00894.x. [DOI] [PubMed] [Google Scholar]