

Abstract
Background:
The Malignant Hyperthermia Association of the United States recommends that dantrolene be available for administration within 10 minutes. One approach to dantrolene availability is a malignant hyperthermia cart, stocked with dantrolene, other drugs and supplies. However, this may not be of cost-benefit for maternity units, where triggering agents are rarely used.
Methods:
We performed a cost-benefit analysis of maintaining a malignant hyperthermia cart vs an initial dantrolene dose of 250 mg on every maternity unit in the United States. We used a decision tree model to estimate the expected number of lives saved and compared this benefit against the expected costs of the policy.
Results:
We found that maintaining a malignant hyperthermia cart in every maternity unit in the United States would reduce morbidity and mortality costs by $3,304,641 per year nationally but would cost $5,927,040 annually. Sensitivity analyses showed that our results were largely driven by the extremely low incidence of general anesthesia. If cesarean delivery rates in the United States remained at 32% of all births, the general anesthetic rate would have to be greater than 11% to achieve cost-benefit. The only cost effective strategy is to keep a 250 mg dose of dantrolene on the unit for starting therapy.
Conclusions:
It is not of cost-benefit to maintain a fully stocked malignant hyperthermia cart with a full supply of dantrolene within 10 minutes of maternity units. We recommend that hospitals institute alternative strategies (e.g. maintain a small supply of dantrolene on the maternity unit for starting treatment).
Keywords: Malignant hyperthermia, Dantrolene, cost-effective, cost-benefit, obstetrics, maternity units
Introduction
One crucial aspect of anesthesiology is finding clinical and systems-based solutions to address rare but potentially catastrophic events. Malignant hyperthermia (MH), a rare autosomal dominant condition that manifests as a hypermetabolic response when exposed to volatile anesthetics and/or depolarizing muscle relaxants, provides a special example. The treatment for MH is well known, and dantrolene treatment has lowered mortality rates from roughly 80% over 40 years ago to 10% in current practice.1 Additionally, complications from MH (disseminated intravascular coagulation, renal dysfunction, cardiac dysfunction, coma, compartment syndrome, and pulmonary edema), which occurs in 20 to 35% of patients, increase markedly for each 10-minute delay in dantrolene administration. If dantrolene administration is delayed beyond 50 minutes, complication rates increase to 100%.2,3 However from a systems perspective, the correct approach towards preparing for MH is uncertain. While there are slight variations on the incidence of MH reported, the generally accepted incidence rate is 5.85 MH cases per 1,000,000 cases using general anesthesia, or 1 in every 170,698 general anesthetic cases.4–8 Because MH is so uncommon, it is possible that the costs of having immediately available dantrolene may exceed the benefits at the population level, particularly for operating rooms and procedure areas where general anesthesia is uncommonly provided.
Understanding the cost-benefit trade-off of providing dantrolene has important policy implications. Indeed, the Malignant Hyperthermia Association of the United States (MHAUS) recommends that dantrolene be made immediately available (for administration within 10 minutes) in operating room areas.9 This recommendation is cost-effective for sites with a significant number of general anesthetics (e.g., hospitals and stand-alone surgery centers). 4 However, maternity units uncommonly use MH-triggering agents. For example, an institution that delivers 6000 babies a year and has a 30% cesarean delivery rate and a 5% general anesthesia rate will use general anesthesia less than 100 times a year. With the expected MH incidence of 1 case per 170,698 anesthetics, that maternity unit would expect to have a MH case every 1,700 years. Such a low incidence prompts the question of whether the standard proposed by MHAUS is necessary for maternity units, since, to meet this standard, many maternity units should have their own MH cart. While well-intentioned, if the costs of maintaining an MH cart exceed its benefits at the population level, the MHAUS standard diverts resources from other initiatives (e.g., the provision of difficult airway equipment) that may have a larger impact in patient safety and reducing maternal mortality or mortality.
To examine this issue, we conducted a cost-benefit analysis to evaluate whether, at the population level, the benefits of maintaining an MH cart in or near maternity units (and therefore available within 10 minutes) in the United States (instead of relying on MH carts available in other areas of the hospital) exceed the costs associated with this practice. We also evaluated the cost effectiveness of other alternatives such as keeping just the initial dose of the dantrolene on the unit.
Methods
Cost-Benefit Analysis
We used a cost-benefit analysis to estimate the practicality of providing an MH cart for every maternity unit in the United States. Cost-benefit analysis is often used by policymakers and regulators to understand the economics and population-level suitability of a given intervention (e.g., environmental regulations or vehicle safety regulations).10–12 With a cost-benefit analysis, the mortality benefits of the given intervention are compared against its costs. Since mortality benefits are typically calculated as the number of lives saved while costs are estimated in dollars, regulatory agencies use a parameter known as the Value of a Statistical Life (VSL) to convert mortality benefits (in terms of lives saved) to dollar terms. The VSL has been estimated to range from $4 million to $10 million per statistical life.11 Thus, assuming a VSL of $10 million, a given intervention that would save 100 lives per year would only be worthwhile if it cost less than $1 billion (i.e., $10 million times 100) annually.
In our case, we used a cost-benefit analysis to analyze whether the reduced mortality from a policy requiring that every maternity unit in the United States have an MH cart for dantrolene administration would be worth the costs of implementing such a policy. Below, we describe the methods we used to estimate the benefits and costs of this policy.
Policy Benefits
Having an MH cart present in a maternity unit benefits patients to the degree it reduces mortality and morbidity by facilitating earlier administration of dantrolene. Intuitively, the benefits to patients will be larger to the extent (a) more general anesthetics are performed and (b) earlier administration decreases complications and improves survival. To evaluate this hypothesis, we used a decision tree model. These models use probability of events occurring at each point and give estimates for all possible outcomes. We developed a decision tree model to estimate the reduction in morbidity and mortality from having an MH cart present in each maternity unit in the United States (Figure 1).
Figure 1.

The decision tree analysis of the various outcomes related to possible exposure to a malignant hyperthermia-triggering anesthetic for a parturient on a maternity unit. The square indicates a decision under evaluation. The circle represents a chance node with a particular probability of that event happening. The triangle represents the terminal node, or the final event in the evaluation. The asterisk (*) indicates a value obtained from Stanford University Hospital. CD=cesarean delivery; VD=vaginal delivery; GA=general anesthesia; NA=neuraxial anesthesia; MH=malignant hyperthermia; Tx=treatment.
The key parameters for this model were: (1) number of women entering a labor and delivery unit, (2) incidence of births, (3) incidence of non-cesarean delivery obstetric procedures (e.g. post-partum tubal ligations), (4) incidence of cesarean deliveries, (5) incidence of general anesthesia for cesarean deliveries, (6) incidence of general anesthesia for non-cesarean delivery obstetric procedures, (7) incidence of MH for general anesthetic procedures, (8) MH mortality with no delay in dantrolene treatment, (9) MH mortality with no treatment, (10) MH morbidity with no delay in dantrolene treatment, (11) and MH morbidity with no treatment. In general, where there was a range of estimates in the literature, we chose values that would provide the highest reduction in mortality. In converting the benefits of maintaining a cart to dollar amounts, we used a VSL of $10 million per life, the upper end of the range typically used by regulators.10
Policy Costs
We determined the costs of maintaining an MH cart by considering three sources of potential cost: 1) the treatment drug (dantrolene); 2) the physical cart and all other non-dantrolene cart drug and disposable items; and 3) maintenance of the MH cart. In regards to the costs of dantrolene, MHAUS recommends stocking either 36 20-mg vials of the older, less concentrated formulation of dantrolene or 3 250-mg vials of the newer, more concentrated formulation of dantrolene.9 We estimated that a vial of dantrolene costs $84. With a shelf-life of three years, this means that the annualized cost of stocking an MH cart with dantrolene is $1,008 ($84 per vial multiplied by 36 vials, divided by the shelf-life of three years). We used the older formulation of dantrolene for this analysis because it is less expensive.
For the cost of the MH cart, we obtained quotes from suppliers, ranging from $1,400 to $3,200. Since an MH cart is expected to last 10–16 years, we converted these total costs into an annualized cost by assuming an equal depreciation rate over 16 years, resulting in an annual cost of $87.50 (equals $1,400/16). Other MH cart items as recommended by MHAUS include general supplies, monitoring equipment, nursing supplies, lab test supplies, and other drugs that may be useful during resuscitation (including furosemide, sodium bicarbonate, calcium chloride, insulin, and lidocaine).9 Each individual item in the cart has a shelf life between 1 to 5 years and was adjusted accordingly to obtain an annual cost (Table 1).
Table 1.
Abbreviated malignant hyperpyrexia (MH) cart supply costs (excluding the cost of dantrolene)
| MH Cart Items | Annualized Costs |
|---|---|
| Other Drugs | $66.35 |
| General Equipment | $57.72 |
| Monitoring Equipment | $15.33 |
| Nursing Supplies | $10.48 |
| Lab Test Supplies | $0.24 |
| MH Cart | $87.50 |
| Total | $237.62a |
We used cost data from our institution, which obtained the lowest prices of all cart supplies quoted from at least three different vendors.
Other drugs included furosemide, sodium bicarbonate, calcium chloride, insulin, and lidocaine; general equipment included vial spikes, angiocaths, “T” connectors, 500ml bag Lactated Ringer’s solution, 500l bag saline solution, sterile injectable water, luer-lock syringes, radial artery catheters, 3-way stopcocks, primary IV solution sets with drip chambers, 60’ micro-volume IV extension tubing, pediatric armboards, salem pump tubes, non-latex Robinson catheters, catheter-tip syringe, 5-in-1 connectors, Y connectors, , 2-way silicone urinary catheters, 3-way silicone urinary catheters, peritoneal lavage tray, soda lime canister refill, ambu bag with mask; monitoring equipment included arterial line monitoring kit, central venous pressure line kit; nursing supplies included alcohol prep pads, sterile gauze pads 2×2/4×4, iodine prep solution, chlorhexidine prep solution, adhesive IV dressings, 1’ micropore tape, latex-free tourniquets, urinary catheter insertion kit and drainage bag with urimeter; lab supplies included heparinized arterial blood gas syringes, blood tube kits
The maintenance of MH carts was considered as a cost variable. We assumed that weekly checks of the MH cart is $555 of a registered nurse’s (RN) time (i.e. 15 minutes per week times 52 weeks times $42.68 RN hourly wage with benefits as 25% of salary).13 We estimated that a pharmacist performs, at minimum, monthly checks of MH cart drugs, which has an annual cost of $215 (i.e. 15 minutes per month times 12 months times $71.68 pharmacist hourly wage with benefits as 25% of salary).14 The total cost for cart maintenance was therefore estimated to be $770 ($555 + $215).
The cost of a single MH cart was the total of the three costs (cost of dantrolene, cost of MH cart and non-dantrolene cart items, and MH cart maintenance cost) described above. To ensure compliance with MHAUS recommendation without ambiguity, we assume all maternity units in each hospital should have an MH cart, and therefore multiplied the total estimated cost of a single MH cart by the number of maternity units in the United States. According to data from the FY2013 American Hospital Association annual survey published in American Hospital Association Hospital Statistics 2015, there are 2,471 hospitals out of a total of 4,780 reporting hospitals in the United States that indicated the availability of obstetrics services. The United States has 5,686 registered hospitals.15 If we assume the rate of obstetric services are the same for the hospitals that did not respond to the American Hospital Association survey, we can reasonably calculate the number of obstetric care hospitals in the United States to be 2,940.
We performed analyses on alternative strategies for maintaining a supply of dantrolene on the maternity unit. Firstly, we eliminated the other supplies (and their costs) from the MH cart except for the dantrolene and analyzed this in the same manner as we did for the complete MH cart. Second, we redid the dantrolene only analysis without the maintenance costs. Third, we assumed only an initial dose of dantrolene (250 mg) would be kept on the maternity unit and the MH cart from a central location would be brought in to complete the MH therapy. We then reanalyzed this scenario for cost effectiveness using both formulations of dantrolene.
The number of maternal lives saved per year was calculated by multiplying the incidence of MH cases per year by the incremental difference in mortality rate with dantrolene treatment within 10 minutes. Incidence of MH cases per year equals the number of cesarean deliveries with general anesthetic and non-cesarean obstetric general anesthetic cases (e.g. bilateral tubal ligations or cerclages) multiplied by the probability of MH per general anesthetic case. The probability of MH per general anesthetic case is 1/170958,7 and the total number of annual obstetric cases is 80,427 as calculated by CDC and institutional data (Figure 1). Estimated maternal mortality with no dantrolene treatment is 80% and with dantrolene treatment available within 10 minutes is 10%.4 The calculated number of annual lives saved is 0.33 (80427/170968 times (80%–10%)).
Sensitivity Analysis
We ran a sensitivity analysis to determine how different independent cost variables impact the dependent variable of case fatality rate. We calculated initial cost-benefits based on point values for all variables determined from literature and institutional data. With the sensitivity analysis, we determined a range of possible values for each variable to account for clinical plausibility. More specifically, we allowed for a range of values for one variable while keeping all other variables fixed at the base value to determine the cost-benefit. In addition to the variables used in the decision tree model, we included neonatal morbidity and mortality as additional variables in the sensitivity analysis. We used Microsoft Excel Solver to determine hypothetical values to achieve cost-benefit.
To complement the sensitivity analysis, we ran a Monte Carlo simulation. This method randomly chooses a set of numbers for each variable given parameters and plausible distribution of values to determine hypothetical costs while allowing all variables to change simultaneously. We ran 1000 iterations using the statistical software R, and each variable was set to have a normal or uniform distribution of possible values based on clinical probability (Appendix A). For example, in our model, dantrolene had a uniform distribution between $700 and $1100; and pharmacist salary and benefits had a normally distributed mean of $72 and a standard deviation (SD) of $15. Upper and lower limits were applied, and in this case, the pharmacist salary and benefits value could go no lower than $30 and no higher than $100. If the annual cost of the intervention was less than the value of annual lives saved, we would achieve cost-benefit.
Results
Figure 1 presents the decision tree model and parameters we used to estimate the benefit of having an MH cart present in each maternity unit. Overall, our results suggest that having an MH cart present in each maternity unit in the United States would be expected to reduce maternal mortality from 80% to 10%. Stated differently, an MH cart on every maternity unit (available within 10 minutes) would save 0.33 maternal lives nationally per year. Using a VSL of $10 million per life, this mortality benefit would be worth $3,300,000 per year. MH morbidity has been well-studied with complications seen in 35% of patients who have an MH crisis2, and the risk of MH-related complications increase 2.27 times (or 79%) when the time from the first MH sign and dantrolene administration increases from 10 minutes to 40 minutes.16 Costs associated with MH complications would likely require intensive care stays with ventilation, and were estimated to be on average $75,000 per stay.17,18 The cost associated with an increase in maternal morbidity was calculated by subtracting the MH mortality assuming no treatment from the incidence of MH (80427/170968 – 0.33 = 0.14) and multiplying that number by the increase in morbidity costs (79%−35% times $75,000 = $33,147) which equaled $4,641. Therefore, placing an MH cart in each maternity unit would only be of cost-benefit if the cost of doing so nationally was less than the sum of MH morbidity and mortality costs, or $3,304,641 per year.
Our results found that the annual total cost of placing an MH cart in a maternity unit is $2,016: $1,008 for the dantrolene itself, $238 for the cart and non-dantrolene items, and $770 for MH cart maintenance. Multiplied by 2,940, the total number of maternity units in the United States would result in a total cost of $5,927,040, which is significantly larger than the $3,304,461 cost-benefit threshold value we calculated.
Neonatal mortality and morbidity were included in the sensitivity analysis and Monte Carlo simulation. Neonatal mortality was calculated by multiplying the probability of maternal mortality or morbidity assuming no treatment, the probable range of values that neonatal death occurs, and the value of a statistical life ((0.33+0.06) times 0–40% times $10,000,000). Neonatal morbidity was calculated by multiplying the probability of maternal mortality or morbidity occurring assuming no dantrolene treatment, the probable range of values of neonatal lives not ending in death, the probable range of values of requiring an ICU stay, and the cost of the intensive care unit stay ((0.33+0.06) times (1-(0–40%)) times 10–50% times $75,000).19
The sensitivity analyses are shown in Table 2. The analysis found no mortality benefit in all but two categories within clinically plausible variations in our base values. In comparison to the lowest plausible cost of the MH cart, we would achieve cost-benefit if general anesthesia rates were nearly doubled or if the incidence of MH in general anesthetic cases was twice as high, i.e. 1 in every 85,484 general anesthetic cases. Neonatal mortality and morbidity were not key drivers of the cost-benefit analysis. Additionally, a more sophisticated analysis with the Monte Carlo simulation, which included both maternal and neonatal morbidity and mortality, found that we did not achieve cost-benefit in 93% of the 1000 iterations, i.e. the annual cost of maternal and neonatal lives saved is less than the cost of having the MH carts in maternity units in 93% of the iterations (Table 3 and Appendix A).
Table 2.
Sensitivity analyses to determine the independent cost variables’ impact on the dependent variable of mortality and morbidity benefit
| Cost Categories | Base Value | Lower Limit | Upper Limit | *Cost Lower Range | *Cost Upper Range |
| Dantrolene | $1,008.00 | $700.00 | $1,100.00 | $5,019,859 | $6,195,859 |
| Other Cart Supplies | $237.62 | $100.00 | $400.00 | $5,520,776 | $6,402,776 |
| Pharmacist Time | 3 | 1 | 5 | $5,503,901 | $6,346,857 |
| RN Time | 13 | 10 | 20 | $5,548,985 | $6,803,630 |
| Pharmacist Salary + Benefits (25%) | $71.68 | $30.00 | $100.00 | $5,557,761 | $6,175,161 |
| RN Salary + Benefits (25%) | $42.68 | $25.00 | $75.00 | $5,249,840 | $7,160,840 |
| Number of Hospitals | 2940 | 2471 | 3377 | $4,980,140 | $6,806,124 |
| Effectiveness Categories | Base Value | Lower Limit | Upper Limit | **VSL Lower Range | **VSL Upper Range |
| Dantrolene Intervention MH Mortality | 10% | 1.40% | 11.70% | $3,700,857 | $3,217,928 |
| 30 Minute Dantrolene Treatment Delay | 80% | 50% | 100% | $1,891,045 | $4,235,360 |
| GA rate for CD | 5.80% | 3.00% | 10.00% | $1,823,364 | $5,509,039 |
| GA rate for Non-CD Procedures | 4.51% | 2% | 8% | $3,161,956 | $3,486,287 |
| Rate of Non-CD Procedures | 3.20% | 2% | 4% | $3,204,348 | $3,361,121 |
| Number of Births | 3988076 | 3988076 | 3988076 | $3,297,634 | $3,297,634 |
| Rate of CD of all L&D visits | 32.20% | 15.00% | 42.00% | $1,666,388 | $4,227,065 |
| Number of GA Cases per MH Case | 170968 | 341936 | 85484 | $1,648,817 | $6,595,269 |
| Fetal mortality | 0% | 40% | $3,297,634 | $4,864,306 | |
| Fetal morbidity | 10% | 50% | $3,298,880 | $3,303,862 |
Cost = Estimated yearly cost per maternal and fetal lives saved by maintaining a malignant hyperthermia cart on a maternity ward
VSL = Estimated yearly maternal and fetal value of statistical lives
Cost-benefit is achieved when VSL is greater than lowest cost value.
RN=registered nurse; CD=cesarean delivery; GA=general anesthesia; MH=malignant hyperthermia; L&D=labor and delivery
Table 3.
Distribution of cost per annual life saved under different assumptions
| Cost in Dollars per Annual Life Saved | ||||
|---|---|---|---|---|
| 1st Percentile | 25th Percentile | 50th Percentile | 75th Percentile | 99th Percentile |
| $1,305,711 | $2,568,546 | $3,366,010 | $4,314,678 | $7,076,445 |
| Category | Mean Annual Cost | Percentile |
|---|---|---|
| MH Cart + Maintenance | $5,946,891 | 93rd |
| Dantrolene + Maintenance | $4,865,075 | 85th |
| Dantrolene Only (Newer Formulation) | $3,382,355 | 50th |
| Dantrolene Only (Older Formulation) | $2,599,472 | 26th |
| Starter Pack (Older Formulation) Only | $938,698 | 0th |
MH = malignant hyperthermia
Assumptions for this simulation study were normal distributions for salaries and general anesthesia rates, and uniform distributions for cost of dantrolene, cost of cart and supplies, number of hospitals, rates of MH mortality with dantrolene and delay in dantrolene treatment, rates of cesarean and non-cesarean delivery procedures, incidence of MH cases per year, fetal morbidity and fetal mortality. Upper and lower bounds are shown in Appendix A. 1000 iterations of the simulation were conducted. The mean annual cost for the MH cart, 36 dantrolene vials, and 13 20-mg vials for a starter pack for the simulation was calculated. Percentiles for cost per annual life saved were determined and indicates the value below which a percentage of simulated costs fall. Values of cost per annual life saved that cross the cost-benefit threshold for the intervention would make the intervention optimal (e.g. mean annual cost for the MH cart intervention falls in the 93rd percentile, which makes it not optimal 93% of the time and mean annual cost for the starter pack falls in the 0th percentile, which makes it optimal 100% of the time).
We analyzed the general anesthetic rates of cesarean deliveries to determine the rate required to achieve cost-benefit. If cesarean delivery rates in the United States remained at 32% of all births, the general anesthetic rate would have to be greater than 11% to achieve cost-benefit (Figure 2). In addition to general anesthetic rates, cesarean delivery rates and number of deliveries per hospital were potential drivers in the model, therefore we also determined possible scenarios which would achieve cost-benefit by changing three variables: cesarean delivery incidences, general anesthetic rates, and number of deliveries per hospital (Figure 2). For example, if a unit has 5000 deliveries and a cesarean delivery incidence of 40%, general anesthetic rate of at least 2% would be required to achieve cost-benefit.
Figure 2.
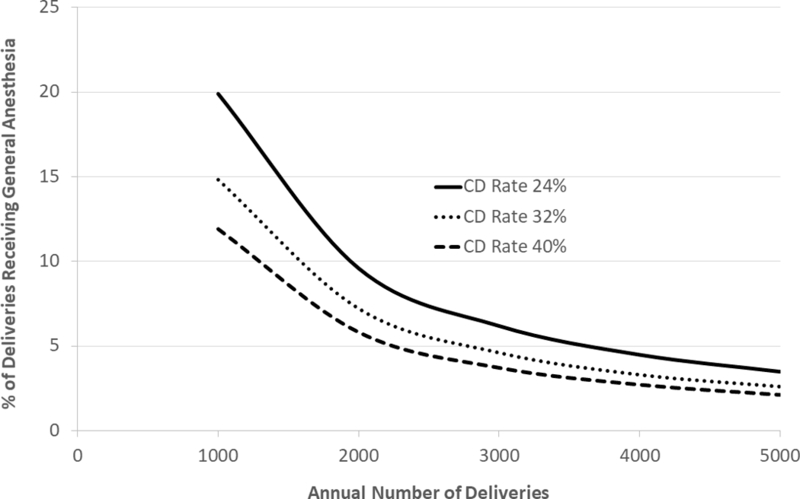
The lines on the graph show the points at which the cost of maintaining a malignant hyperthermia (MH) cart on a maternity unit equals the value of a statistical life. The x-axis is the number of deliveries per year and the y-axis is the percentage of deliveries that have a general anesthetic (GA). Each line represents different cesarean delivery (CD) rates. Points below the lines are cost ineffective.
We also evaluated the mean annual costs of maintaining less than a fully stocked MH cart and ran Monte Carlo simulations on the various configurations (Table 3). Reducing the cart content to just dantrolene without the other supplies needed in an MH resuscitation reduced the mean annual costs by less than 20% and was still cost ineffective 85% of the time. Eliminating the maintenance costs from the analysis reduced the cost by over 50% and made stocking dantrolene cost effective 74% of the time. However, this scenario ignores the true costs of maintaining the supply. Keeping a single vial of the new formulation of dantrolene20 on the maternity unit (this vial contains enough dantrolene to start the treatment of a 100 kg patient) without adding maintenance costs, is more expensive than keeping a full supply of the older formulation and was cost effective 50% of the time in the Monte Carlo simulations. The only cost effective plan when considering maintenance of the supply, was to keep a “starter pack” of the older formulation on the maternity unit (13 20-mg vials; enough for the first dose of a 100 kg patient). This plan was cost effective 100% of the time in the Monte Carlo simulation.
Discussion
In this study, we performed a cost-benefit analysis to determine the value of maintaining a separate MH cart on the maternity unit within hospitals in the United States. Using conservative assumptions of costs, rates of general anesthesia, incidence of MH, and expected mortality and morbidity from MH, we found that the cost of a life saved is significantly greater than what is considered of cost-benefit. Only by assuming an unreasonably high case fatality rate, general anesthetic incidences or cesarean delivery rates does it become of cost-benefit to maintain a fully stocked MH cart on a maternity unit. Our results are primarily driven by the low number of general anesthetics, and therefore the extremely low likelihood of an MH incident amongst parturients. For example, a previous study found that stocking dantrolene is of cost-benefit in a small ambulatory surgical center that performs 10 triggering anesthetics a day (i.e. 2000–3000 anesthetics per year).4 However, the number of triggering anesthetics is at least an order of magnitude lower in maternity units. For example, even a maternity unit with 10,000 deliveries per year would be expected to perform at most two to three hundred general anesthetics per year.
Our assumption that mortality per MH case will increase from 10% to 80% if dantrolene is not stocked on the maternity unit is conservative and the resultant increased mortality rate estimate is probably excessive. The 80% value is the same as no dantrolene treatment, not delayed treatment (i.e. greater than 10 minutes from diagnosis). We assumed the same mortality rate as no dantrolene treatment since we do not know how much mortality is affected by delayed treatment of unknown duration. We cannot make a data-based recommendation for the maximal allowable time to deliver dantrolene to the maternity unit.
In calculating the costs, we have included labor costs to maintain the MH carts, which were not included in a prior dantrolene cost-benefit study.4 However, labor costs fall under the category of opportunity costs (costs associated with opportunities forgone due to the use of resources) which are widely accepted to be included in cost-benefit analyses.21 We believe it is necessary to depict all costs related to stocking the cart in the maternity unit.
In calculating the benefits, we used the highest VSL that is typically used for cost-benefit analysis. The sensitivity analyses and Monte Carlo simulations further demonstrated no cost-benefit in all cases when considering maternal morbidity and mortality alone despite conservative ranges of general anesthesia and cesarean deliveries. General anesthetic rates for cesarean delivery have declined significantly over the years, with the most recently reported national rate to be 6%.22 Lower general anesthetic rates are encouraged, and should optimally should be <1% for scheduled cases. Additionally, national bodies emphasize bringing cesarean delivery rates lower, ideally below the current national levels of 32%.23,24 Therefore, we doubt there are any maternity units that perform enough cesarean deliveries with general anesthesia in the United States to justify the presence of an MH cart on the unit. However, maternity units with extremely high cesarean delivery rates (e.g. 50%) combined with unacceptably high general anesthesia rates (e.g. 50%) will have an MH incidence an order of magnitude higher than the average unit, and it is likely of cost-benefit for them to have an MH cart in their maternity unit.
We did not do include the more concentrated dantrolene formulation (Ryanodex) in our cost-benefit analysis of a complete MH cart, but given the additional cost of these drugs over dantrolene, they would be expected to be of even less cost-benefit. Our assumption is that most maternity units that perform cesarean deliveries are proximate to a central supply of dantrolene that can be brought to the unit within 30 minutes of a decision to treat MH. We acknowledge that some maternity units may be remote from a central supply location for dantrolene. In these situations, a unit should have their own MH cart. We also assumed the incidence of MH in obstetric patients receiving general anesthesia is the same as general surgical patients. It may be that with the more dynamic nature of a maternity unit, a family history of MH may be missed more frequently than in other settings.
There is a paucity of data on the risks to the fetus, and no reported cases of neonatal harm after maternal exposure. We could only find three case reports of MH associated with cesarean deliveries in which there was information on the fetus.25–27 In only one case was there possible evidence that MH had been triggered in the baby, and we could find no case reports of neonates requiring treatment with dantrolene. In all likelihood, if a neonate ever presented with MH triggered from in utero exposure, treatment would likely take place in the neonatal intensive care unit and the presence of dantrolene on the maternity unit would not affect neonatal outcome. Additionally, detrimental effects of maternal hemodynamic instability on the neonate before delivery would be unaffected by the presence of dantrolene on the unit since the baby would likely be delivered before dantrolene could be administered. Nonetheless, we included neonatal mortality and morbidity in the sensitivity analyses and Monte Carlo simulations. Despite applying conservatively high estimates of neonatal mortality (estimates of up to 40% of neonates dying) and morbidity (including up to 50% of neonates would incur intensive care unit costs), no cost-benefit was achieved in 93% of the simulated cases.
Our analysis shows that maintaining an MH cart on the maternity unit, versus readily available within the hospital is not of cost-benefit. The MH cart also requires storage space in maternity units that may impact access and workflow in patient care areas. The money saved from not maintaining a separate and complete MH cart in a maternity unit could be used to purchase more expensive formulations of dantrolene that can be reconstituted faster and potentially make up for the time it takes to retrieve dantrolene from a centralized supply location within the hospital but remote from the maternity unit.20
It may be more cost-effective to rely on a centralized MH cart for managing a case of MH, but to keep enough dantrolene on the maternity unit for the initial dose. MHAUS recommends an initial dose of dantrolene of 2.5 mg/kg, therefore 250 mg will be needed to treat a 100 kg patient. One vial of the newer, more concentrated formulation is 250 mg. Alternatively, a vial of the older version of dantrolene contains 20 mg and 13 vials are required to supply enough for the initial dose for a 100 kg patient. This alternative plan would eliminate the costs of maintaining a cart and reduce the necessary dantrolene stocked on the obstetric unit. Our analysis of this option was found to be cost-effective with the older formulation of dantrolene and was only cost effective 50% of the time with the newer dantrolene formulation (Ryanodex™) (Table 3). We did not include maintenance in this option because the drug could be added to the stock of other emergency supplies kept on the unit (e.g. intralipid for treatment of local anesthetic systemic toxicity) and maintaining the small stock of dantrolene would not add much to the cost of maintaining the other emergency supplies. This option lowers the costs substantially, reduces storage space, and reduces labor.
The question remains whether the higher cost of the newer dantrolene formulation is offset by the lower footprint of storing one vial versus 13 vials of the older dantrolene formulation on the maternity unit. Each vial of the older dantrolene formulation is 60 ml and almost one liter of sterile water is required to reconstitute the 13 vials. The newer dantrolene formulation requires just 5 ml of water for reconstitution. Clearly, it would be easier to keep a supply of the new version of dantrolene in an emergency kit on labor and delivery. However, each vial of the new version costs $3000 and has a shelf life of 33 months. The older version costs $84 for vial and has 36-month shelf life. Therefore, the cost of the first dose of the older dantrolene formulation is one third of the cost of the new dantrolene formulation. The only scenario that is 100% cost effective is to keep a starter kit of the old version.
There are likely to be some maternity units that have a dantrolene supply close enough to their operating room suite so that they meet MHAUS recommendations, or they may perform their cesarean deliveries in the main operating rooms of the hospital. The existence of these situations does not change our results. If we remove a maternity unit because it is capable of using a nearby dantrolene supply, we must reduce a proportionate probability that a general anesthesia related delivery would occur, and thus it would cause a similar reduction of MH occurrence. While there are variations of general anesthetic rates among different maternity units, we do not anticipate a reduction that favors maternity units that use main operating room MH carts as opposed to maternity units who should have their own MH cart. Total costs will decrease, but this also results in a proportional decrease in number of lives saved due to the reduction in MH cases and general anesthetics in the maternity units. The results of the analysis and its interpretation stays the same.
The number of maternity units in the United States would only affect the analysis if it was much lower than our derived number of 2,940, and would therefore result in lower associated costs. We performed a sensitivity analysis where we accounted for the variability of the number of maternity units in the United States. According to the AHA Hospital Statistics, there were a total of 2,471 registered hospitals that responded to the survey and stated that they had obstetric services. In our sensitivity analysis, we set a lower limit of plausibility and assumed that the additional 906 hospitals that did not respond to the survey did not have obstetric services. We found that maintaining MH carts on a fewer number of maternity units was still not cost-effective.
In conclusion, maintaining a fully stocked MH cart with dantrolene in a maternity unit is not of cost-benefit. If general anesthesia rates remain relatively low on maternity units, MH treatment plans that rely on a centralized MH cart are the most cost-benefit solution in the labor and peripartum setting. We believe that the standards set by MHAUS can be fulfilled if a hospital demonstrates the ability to rapidly deliver an MH cart to the maternity unit within 30 minutes of a decision to treat MH and the maternity unit maintains an initial dantrolene treatment dose of 250 mg.
Acknowledgments
Funding: PH was supported by the Foundation for Anesthesia Education and Research’s 2015 Medical Student Anesthesia Research Fellowship program. None of the other authors have any financial interests to disclose.
Appendix A. R Program Code for Monte Carlo Simulation
# 1000 data points for each variable are randomly assigned in a normal or uniform distribution. Variables with normal distributions that have a lower and upper bound will contain 1200 data points initially. Then, the first 1000 data points within the lower and upper bounds will be selected for the simulation.
# 1. VARIABLES TO CALCULATE COST
# d = total cost of 36 dantrolene IV mg vials
# MHcart = malignant hyperthermia cart cost
# PT = pharmacist’s time in hours required for MH cart maintenance
# PS = pharmacist’s salary and benefits
# PS2 = dummy variable of PS, which satisfies specified constraints
# RT = registered nurse’s time in hours required for MH cart maintenance
# RS = registered nurse’s salary and benefits
# RS2 = dummy variable of RS, which satisfies specified constraints
# H_num = number of hospitals in the U.S. that has an L&D suite
# Tot_Cost = total annual cost of MH cart, MH cart maintenance, and L&D nurse training
# Dantrolene IV 20 mg
# uniform distribution within limits
# lower bound = $700, upper bound = $1100
> d <- runif(1000, 700, 1100)
# MH Cart Supplies
# uniform distribution
# lower bound $300, upper bound = $450
> MHcart <- runif(1000, 300, 450)
# Pharmacist’s Time for Cart Maintenance
# uniform distribution with bounds
# lower bound = 1, upper bound = 5
> PT <- runif(1000, 1, 5)
# Pharmacist’s Salary + Benefits
# normal distribution
# mean = $71.68, SD = $15
> PS <- rnorm(1200, 71.68, 15)
> PS2 <- PS[PS >=30 & PS <= 100][1:1000]
# RN’s Time for Cart Maintenance
# uniform distribution with bounds
# lower bound = 10, upper bound = 20
> RT <- runif(1000, 10, 20)
# RN Salary + Benefits
# normal distribution
# mean = $42.68, SD = $10, lower bound = 25, upper bound 75
> RS <- rnorm(1500, 42.68, 10)
> RS2 <- RS[RS >=25 & RS <=75][1:1000]
# Number of Hospitals
# uniform distribution
# lower bound = 2471, upper bound = 3377
> H_num <- runif(1000, 2471, 3377)
# Calculating the total annual cost in the U.S.
> Tot_Cost = ((d+MHcart)+PT*PS2+RT*RS2)*H_num
# 2. VARIABLES TO CALCULATE EFFECTIVENESS
# MH_mort_wd = mortality rate of MH patients who were administered dantrolene immediately
# MH_mort_ddelay = mortality rate of MH patients who have a delay in dantrolene treatment, variable as multiplier of MH_mort_wd
# Mmorb_wd = maternal morbidity with dantrolene treatment
# Mmorb_ddelay = maternal morbidity due to delay in treatment
# FMorb = fetal morbidity due to delay in maternal MH treatment
# FMort = fetal mortality due to delay in maternal MH treatment
# GA_CS = rate of triggering general anesthetics used for cesarean sections in the U.S.
# GA_CS2 = dummy variable for GA_CS, which satisfies specified constraints
# GA_nonCS = rate of triggering general anesthetics used for admitted L&D patients undergoing non-cesarean section procedures in the U.S.
# GA_nonCS2 = dummy variable for GA_nonCS, which satisfies specified constraints
# nonCS = rate of admitted L&D patients who undergo non-cesarean section procedures
# rate_birth = rate of births as a proportion of total procedures done at the hospital
# total_births = total number of births in the U.S.
# rate_CS = rate of cesarean sections in the U.S.
# Num_GA_CS = total number of triggering general anesthetic cases in cesarean sections seen in the U.S.
# Num_GA_nonCS = total number of triggering general anesthetic cases in admitted L&D patients’ non-cesarean section procedures seen in the U.S.
# Tot_GA = total number of triggering general anesthetic cases in all admitted L&D patient procedures
# MH_incidence = the incidence rate of MH in patients who are exposed to a triggering general anesthetic
# Tot_MH = total number of MH cases per year
# MH Mortality with Dantrolene
# uniform distribution within 1.4% to 11.7%
# lower bound 1.4%, upper bound 11.7%
> MH_mort_wd <- runif(1000, 0.014,0.117)
# MH Mortality with Delay in Dantrolene Treatment
# uniform distribution between 50%−100%
# lower bound .5, upper bound 1
> MH_mort_ddelay <- runif(1000, 0.5, 1)
# Maternal morbidity with dantrolene treatment
# uniform distribution between 30% and 40%
> Mmorb_wd <-runif(1000, 0.3, 0.4)
# Maternal morbidity due to delay in treatment
# uniform distribution between 60% and 100%
> Mmorb_ddelay <-runif(1000, 0.6, 1)
# Fetal morbidity due to delay in maternal MH treatment
# uniform distribution between 10% and 50%
> FMorb <-runif(1000,0.10,0.50)
# Fetal mortality due to delay in maternal MH treatment
# uniform distribution between 10% and 40%
> FMort <- runif(1000,0.10,0.40)
# GA Rate for CS
# normal distribution
# mean = 5.8%, SD = 1%, lower bound = 3%, upper bound = 10%
> GA_CS <- rnorm(1200, 0.058, 0.01)
> GA_CS2 <- GA_CS[GA_CS >=0.03 & RS <=0.1][1:1000]
# GA Rate for Non CS Procedures
# normal distribution
# mean = 4.51%, SD = 1%, lower bound = 2%, upper bound = 8%
> GA_nonCS <- rnorm(1200, 0.0451, 0.01)
> GA_nonCS2 <- GA_nonCS[GA_nonCS >=0.02 & GA_nonCS<=0.08][1:1000]
# Rate of Non CS Procedures
# uniform distribution
# lower bound = 2%, upper bound = 4%
> non_CS <- runif(1000, 0.02, 0.04)
# Rate of Birth as a Proportion of Total Procedures Performed on Admitted L&D Patients
# (vaginal birth + birth via cesarean section) / total admitted L&D patient procedures
> rate_birth <- 1-non_CS[1:1000]
# Number of Births in the U.S.
# taken from CDC data
> total_births = 3988076
# Rate of CS
# uniform distribution
# lower limit 15%, upper limit 42%
> rate_CS <- runif(1000, 0.15, 0.42)
# Determining the number of GA cases per year
> Num_GA_CS = total_births*rate_CS*GA_CS2
> Num_GA_nonCS = (non_CS/(rate_birth/total_births))*GA_nonCS2
> Tot_GA = Num_GA_CS + Num_GA_nonCS
# Incidence of MH Per Year
> MH_incidence = 1/170968
> Tot_MH = Tot_GA * MH_incidence
# 3. VARIABLES TO CALCULATE COST BENEFIT
# Yearly_Maternal_Life_Saved = the incremental number of lives saved per year by having the dantrolene immediately available in the L&D suite
# Yearly_Maternal_Mortality_Value = yearly value of maternal life saved
# Yearly_Maternal_Morbidity_Value = yearly value of maternal morbidity cost saved
# Yearly_Fetal_Mortality_Value = yearly value of fetal life saved
# Yearly_Fetal_Morbidity_Value = yearly value of fetal morbidity cost saved
# Total_Annual_Values_Lives_Saved = yearly value of maternal and fetal lives saved by having dantrolene immediately available
> Yearly_Life_Saved = Tot_MH*(MH_mort_ddelay – MH_mort_wd)
> Yearly_Maternal_Mortality_Value = Yearly_Life_Saved*10000000
> Yearly_Maternal_Morbidity_Value = (Tot_MH- Yearly_Life_Saved)*(Mmorb_ddelay – Mmorb_wd)*75000
> Yearly_Fetal_Mortality_Value = (Yearly_Life_Saved + Mmorb_ddelay – Mmorb_wd)*FMort*10000000
> Yearly_Fetal_Morbidity_Value = (Yearly_Life_Saved + Mmorb_ddelay – Mmorb_wd)*(1-FMort)*FMorb*75000
> Total_Yearly_Value_Lives_Saved = Yearly_Maternal_Mortality_Value + Yearly_Maternal_Morbidity_Value + Yearly_Fetal_Mortality_Value + Yearly_Fetal_Morbidity_Value
# Cost-benefit is achieved if Total_Yearly_Value_Lives_Saved > Tot_Cost
# Results of Monte Carlo Simulation:
# Tot_Cost
# Mean $5,946,891
# Min $3,896,981
# Max $9,216,903
# Total_Yearly_Value_Lives_Saved
# 1st percentile: $1,446,511
# 25th percentile: $3,117,773
# 50th percentile: $4,093,143
# 75th percentile: $5,361,656
# 85th percentile: $5,928,065
# 99th percentile: $8,470,213
Footnotes
Conflict of Interest: The authors declare no competing interests
Prior Presentations: Not applicable
References:
- 1.Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB: Malignant hyperthermia deaths related to inadequate temperature monitoring, 2007–2012: a report from the North American malignant hyperthermia registry of the malignant hyperthermia association of the United States. Anesth Analg 2014; 119: 1359–66 [DOI] [PubMed] [Google Scholar]
- 2.Larach MG, Gronert GA, Allen GC, Brandom BW, Lehman EB: Clinical presentation, treatment, and complications of malignant hyperthermia in North America from 1987 to 2006. Anesth Analg 2010; 110: 498–507 [DOI] [PubMed] [Google Scholar]
- 3.Riazi S, Larach MG, Hu C, Wijeysundera D, Massey C, Kraeva N: Malignant hyperthermia in Canada: characteristics of index anesthetics in 129 malignant hyperthermia susceptible probands. Anesth Analg 2014; 118: 381–7 [DOI] [PubMed] [Google Scholar]
- 4.Aderibigbe T, Lang BH, Rosenberg H, Chen Q, Li G: Cost-effectiveness analysis of stocking dantrolene in ambulatory surgery centers for the treatment of malignant hyperthermia. Anesthesiology 2014; 120: 1333–8 [DOI] [PubMed] [Google Scholar]
- 5.Kim DC: Malignant hyperthermia. Korean J Anesthesiol 2012; 63: 391–401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Larach MG, Dirksen SJ, Belani KG, Brandom BW, Metz KM, Policastro MA, Rosenberg H, Valedon A, Watson CB, Society for Ambulatory A, Malignant Hyperthermia Association of the United S, Ambulatory Surgery F, Society for Academic Emergency M, National Association of Emergency Medical T: Special article: Creation of a guide for the transfer of care of the malignant hyperthermia patient from ambulatory surgery centers to receiving hospital facilities. Anesth Analg 2012; 114: 94–100 [DOI] [PubMed] [Google Scholar]
- 7.Shafer SL, Dexter F, Brull SJ: Deadly heat: economics of continuous temperature monitoring during general anesthesia. Anesth Analg 2014; 119: 1235–7 [DOI] [PubMed] [Google Scholar]
- 8.Strazis KP, Fox AW: Malignant hyperthermia: a review of published cases. Anesth Analg 1993; 77: 297–304 [DOI] [PubMed] [Google Scholar]
- 9.The Malignant Hyperthermia Association of the United States. https://www.mhaus.org/faqs/category/frequently-asked-questions-about/stocking-an-mh-cart/?utm_source=categorizedContentLink. Accessed January 5, 2018,
- 10.Brannon I: What is a life worth? Regulation 2004; 27: 60–3 [Google Scholar]
- 11.Kneiser TV K; Woock C; Ziliak J: The value of statistical life: Evidence from panel data. Rev Econ Stat 2012; 94: 74–87 [Google Scholar]
- 12.Robinson LA: How US Government Agencies Value Mortality Risk Reductions. Review of Environmental Economics and Policy 2007; 1: 283–299 [Google Scholar]
- 13.Occupational Employment and Wages, https://www.bls.gov/oes/current/oes291141.htm. Accessed Oct 12, 2016,
- 14.Occupational Employment and Wages, http://www.bls.gov/oes/current/oes291051.htm. Accessed Oct 12, 2016,
- 15.AHA Hospital Statistics, 2015. edition. Chicago, IL, Health Forum, LLC, 2015 [Google Scholar]
- 16.Brandom BW KA, Sivak EL, Young MC: Update on Dantrolene in the Treatment of Anesthetic Induced Malignant Hyperthermia. SOJ Anesthesiol Pain Manag 2015; 2: 1–6 [Google Scholar]
- 17.Dasta JF, McLaughlin TP, Mody SH, Piech CT: Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med 2005; 33: 1266–71 [DOI] [PubMed] [Google Scholar]
- 18.Graf J, Muhlhoff C, Doig GS, Reinartz S, Bode K, Dujardin R, Koch KC, Roeb E, Janssens U: Health care costs, long-term survival, and quality of life following intensive care unit admission after cardiac arrest. Crit Care 2008; 12: R92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Services NPISQA: Special Care Nursery Admissions. Edited by Services NPISQA. National Perinatal Information System/Quality Analytic Services, March of Dimes Perinatal Data Center, 2011
- 20.Ryanodex--A New Dantrolene Formulation for Malignant Hyperthermia. Med Lett Drugs Ther 2015; 57: 100. [PubMed] [Google Scholar]
- 21.Palmer S, Raftery J: Economic Notes: opportunity cost. BMJ 1999; 318: 1551–2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Juang J, Gabriel RA, Dutton RP, Palanisamy A, Urman RD: Choice of Anesthesia for Cesarean Delivery: An Analysis of the National Anesthesia Clinical Outcomes Registry. Anesth Analg 2017; 124: 1914–1917 [DOI] [PubMed] [Google Scholar]
- 23.Palanisamy A, Mitani AA, Tsen LC: General anesthesia for cesarean delivery at a tertiary care hospital from 2000 to 2005: a retrospective analysis and 10-year update. Int J Obstet Anesth 2011; 20: 10–6 [DOI] [PubMed] [Google Scholar]
- 24.Main EK, Morton CH, Melsop K, Hopkins D, Giuliani G, Gould JB: Creating a public agenda for maternity safety and quality in cesarean delivery. Obstet Gynecol 2012; 120: 1194–8 [DOI] [PubMed] [Google Scholar]
- 25.Lips FJ, Newland M, Dutton G: Malignant hyperthermia triggered by cyclopropane during cesarean section. Anesthesiology 1982; 56: 144–6 [DOI] [PubMed] [Google Scholar]
- 26.Sewall K, Flowerdew RM, Bromberger P: Severe muscular rigidity at birth: malignant hyperthermia syndrome? Can Anaesth Soc J 1980; 27: 279–82 [DOI] [PubMed] [Google Scholar]
- 27.Cupryn JP, Kennedy A, Byrick RJ: Malignant hyperthermia in pregnancy. Am J Obstet Gynecol 1984; 150: 327–8 [DOI] [PubMed] [Google Scholar]