

Abstract
Objectives:
The purpose of this paper is to systematically review the various studies and case reports on the morphology and prevalence of middle canals in the mandibular molars.
Methodology:
Electronic databases such as MEDLINE, PubMed, EBSCOhost, ScienceDirect and various journals were screened to identify published literature till March 2017 and earlier for articles related to middle canals in the human permanent mandibular molars. Obtained articles were categorized as original researches, case reports and review articles. Well-defined review questions were developed using the patient population, intervention, comparison and outcome framework to summarize the objectives: “Does middle canal vary in morphology and anatomic location? What is the prevalence of middle canals in mandibular molars? Does ethnicity affect the prevalence of middle canals in mandibular molars?” Morphology was studied and prevalence rates were determined from the evaluation of data extracted from the articles.
Results:
The search strategy resulted in 87 articles, of which 36 were original research papers and 51 were case reports. The prevalence of middle canals in the various populations ranged from 0.26% to 53.8%. Middle canals were reported in Europeans, Asians, Africans and South and North American populations. The prevalence of middle mesial canal and middle distal canal in various races was reported as up to 53.8% and 10%, respectively. The orifice of middle canal exists below a dentinal projection in the groove between the two main canals. They were observed in fin, confluent and independent configuration. Out of these, confluent configuration was more prevalent.
Conclusion:
Middle canal varies in morphology and anatomic location. Ethnicity affects the prevalence of middle canals in the mandibular molars.
Keywords: Mandibular molars, middle distal canal, middle mesial canal, root canal
INTRODUCTION
Mandibular molars requiring endodontic therapy are frequently encountered in dental practice. The mesial root of a mandibular molar commonly presents a mesiobuccal (MB) and a mesiolingual (ML) canal, while the distal root more often contains one canal rather than two. A narrow connection which also contains pulp tissue, the isthmus, is present between two mesial/distal canals. This isthmus area leads to anatomical variations such as middle canals.[1]
Barker et al.[1] and Vertucci and Williams[2] were the first researchers to demonstrate the presence of an extra and independent canal in this region of the mesial root of mandibular molars. Later, Martinez-Berna and Badanelli[3] reported a middle canal in the distal root also. Since then, several researchers have reported middle canals in the mesial/distal root of mandibular molars. While this middle canal has been variously referred to as the intermediate canal,[4] mesio-central canal,[5] third mesial canal,[6] accessory mesial canal[7] and middle mesial canal (MMC).[8,9] Apparently, the term MMC/middle distal canal (MDC) has found its common usage.
For root canal treatment to be successful, it is necessary to locate all root canals, debride them thoroughly and seal them completely with an inert root filling material. Thus, knowledge of the morphology of this middle canal in the mandibular molars is important. A number of studies have reported that root canal systems vary according to race.[10] From the consistency of certain anatomical features in tooth type in different races, it is apparent that such features are genetically determined.[11] With the evolution of dental operating microscope (DOM) and three-dimensional (3D) imaging technique, detailed information is available on the morphology of middle canal.[7]
A systematic review uses defined methods to search, critically appraise and synthesize the available literature pertaining to a clinical question. The purpose of this systematic review was to study the morphology and prevalence of middle canals in the mandibular molars of different populations and whether ethnicity can influence the prevalence of middle canal.
METHODOLOGY
Formulation of review questions
This systematic review was conducted according to the Preferred Reporting Items for Systematic Review statement.[12] Well-defined review questions were developed using the patient population, intervention, comparison and outcome framework to summarize the objectives as follows:
Does MMC/MDC vary in morphology and anatomic location?
What is the prevalence of MMC/MDC in mandibular molars?
Does ethnicity affect the prevalence of MMC/MDC in mandibular molars?
Selection criteria
Studies included in the systematic review were only those published in English and original articles and case reports that reported on the morphology or prevalence of middle canals in mandibular molars, in which the sample size, population studied and technique for evaluation were mentioned.
Literature search and data extraction
An exhaustive search was undertaken through MEDLINE, PubMed, EBSCOhost and ScienceDirect research databases and various journals to identify published literature dated March 2017 and earlier for articles related to MMC/MDC in human permanent mandibular molars. Keywords used were middle mesial/distal canal and mandibular first/second molar, alone or in combination. The references of all selected articles were further scanned for potentially relevant articles. Obtained articles were categorized as original research articles and case reports.
Data pertaining to the morphology and prevalence of the middle canal were analyzed according to the population ethnicity, method of tooth analysis (clearing, radiographic, scanning electron microscope or 3D imaging such as computed tomography [CT], cone beam CT [CBCT], micro CT or clinical examination under DOM), sample size, prevalence of middle canal in the mesial/distal root, the number of root canals and root canal configuration.
RESULTS
Seventy-nine articles were selected, of which 34 were original research papers and 45 were case reports. Depending on methodology, original research articles were separately tabulated with mention of the population ethnicity, technique of evaluation, number of teeth examined and occurrence of MMC and MDC [Tables 1 and 2].
Table 1.
Prevalence of middle mesial and middle distal canals in mandibular first and second molars before introduction of three-dimensional imaging technique
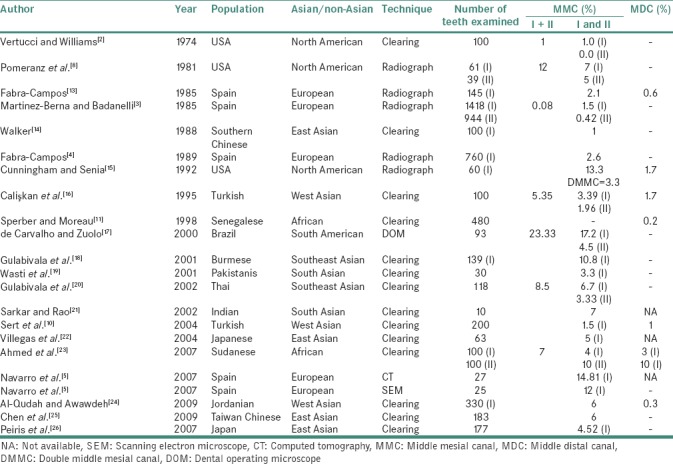
Table 2.
Prevalence of middle mesial and middle distal canals in mandibular first and second molars after introduction of three-dimensional imaging
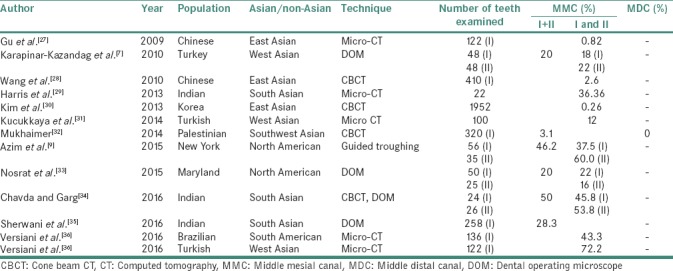
The prevalence of MMC in various populations ranged from 0.26% to 53.8%, whereas MDC was reported in eight studies only, with the prevalence ranging from 0.0% to 10%. The prevalence of double MMC (DMMC) was reported in one study to be 3.3%.
Few studies have drawn a distinction between the prevalence of the middle canal in the mandibular first and second molars. Pomeranz et al.[8] reported an equal incidence of MMC in both mandibular first and second molars, while in most of the other studies, the prevalence was higher in the first than in the second molar. Only four studies reported a higher prevalence of MMC in the mandibular second molar.[7,9,23,34]
Twenty-two research articles reported on the prevalence of the different configuration types (fin/confluent/independent) of the middle canal [Table 3].
Table 3.
Prevalence of configuration types in the middle canal
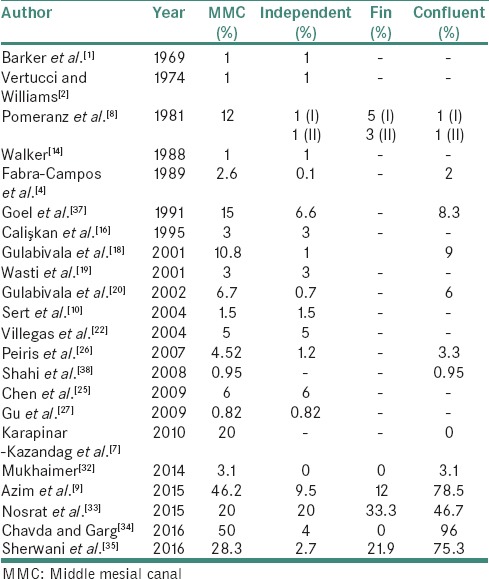
Earlier studies have reported an increased occurrence of the independent configuration.[1,2,14] With the introduction of the DOM and 3D imaging, the fin and confluent configurations were also identified.[33,34,35] Hence, in contemporary studies, a greater prevalence of the confluent configuration compared to fin and independent configurations has been reported.[9,33,34,35]
In addition to research articles, 47 case reports were also reviewed in the present study, with mentions of populations, tooth number, number of root and canals and configuration type (independent/fin/confluent) in each root. These case reports were divided into two groups: non-Asian versus Asian population [Tables 4 and 5].
Table 4.
Case reports on middle canals in non-Asian countries
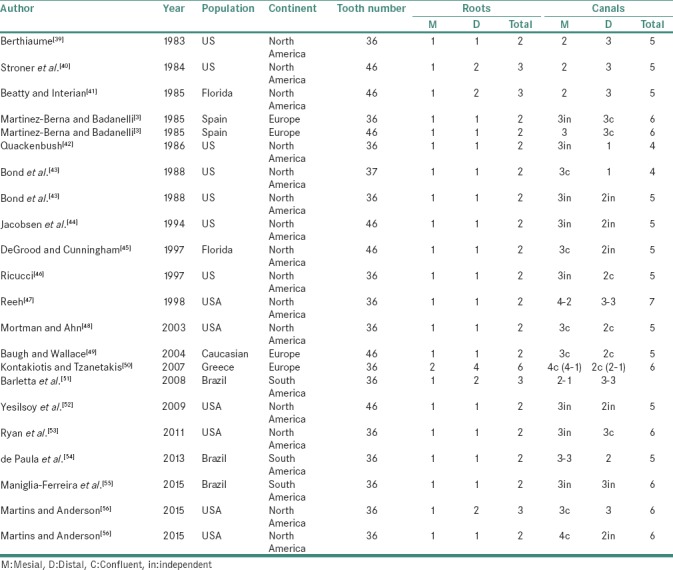
Table 5.
Case reports on middle canals in Asian countries
DISCUSSION
Location of the middle canal orifice
The middle canal orifice exists below a dentinal projection in the groove between the two main canals. The layer of dentin in this groove is lighter in color than adjacent dentin. Studies have reported the average length of the groove in mandibular first and second molars to be 1.07–2.81 mm[36] and the average depth to be 1.05 mm[52] and 0.17–7.66 mm.[36] The difference in the observations between studies may be attributed to differences in the method of study, sample sizes and populations studied.
Diameter and volume of the middle canal orifice
Since extra canals are formed between two main canals, their diameter is less than that of the main canals. The mean minor diameter of the MMC orifice is reported to be 0.16 mm, which is three times less than the diameter of the two main orifices (0.50 mm).[36] This also results in less mean volume of the MMCs. In mesial roots, the mean volume of the MMC and MB and ML canals is reported to be 0.20 ± 0.10, 0.75 ± 0.20 and 0.88 ± 0.19 mm3 respectively.[36] Hence, overzealous preparation of middle canals may lead to perforation.
Middle canal configuration types
Pomeranz et al.[8] classified MMCs into three types [Figure 1a–d]. According to these authors, (i) this canal can run independently from the orifice to the apex (independent), (ii) the canal can join the MB or ML canals before exiting from the apex (confluent) or (iii) an isthmus may be present between the MMC/MDC and the MB or ML canal during any stage of its course from the orifice to the apex (fin). Thus, independent canals originated as a separate orifice and terminated from a separate foramen. Confluent canals originated as a separate orifice but joined the MB or ML canal before leaving the apex, while the fin type did not have a separate orifice and was usually a small linear extension between the MB and ML canals of very small length allowing free movement of the file between the main canal and the fin.
Figure 1.

Pomeranz et al., medial mesial canal classification showing independent configuration (a), fin configuration (b), confluent configuration to mesiobuccal canal (c) and to mesiolingual canal (d)
Versiani et al.[36] described the confluent and fin variations further by evaluating CBCT images of extracted mandibular molars. According to them, in the confluent configuration, the MMC joins the MB and/or ML canal by transverse anastomoses, intercanal connections or isthmus during its trajectory to the apical foramen. Thus, the confluent type can be either without [Figure 2a] or with an isthmus [Figure 2b]. Further, the location of the union of two canals varied from mid-root to the apex.
Figure 2.
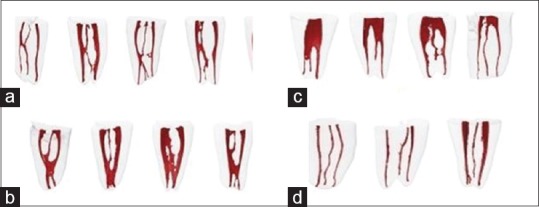
Versiani et al., middle mesial canal configuration showing confluent anatomy without isthmus (a), with isthmus (b), fin configuration (c), and independent configuration (d)
In the fin configuration, the MMC orifice was connected in the coronal third to the MB and/or ML canal orifices by a groove, but the mesial canals left the root via three separate foramina [Figure 2c].
In the independent configuration, three independent canals extended from the pulp chamber to the apex [Figure 2d].
A classification similar to the one used for MMC has been used for MDC by replacing mesial with distal. Later, an additional configuration – double middle mesial/distal, i.e., four canals in one root, was also reported.[37,47,50,56,63,66,75,76,77,78,79] These four canals can be independent, exiting from four separate foramina[63] or confluent with one middle canal joining the ML and the other joining the MB and exiting as two canals from two foramina[66,76,77,78,79] or all four joining and exiting from one foramen.[50]
Location of the middle canal with respect to the main canal
Some research articles report the third canal to be located equidistant to both the main canals, while others report it to be closer to one of the main canals. Sherwani et al.[35] observed that, in 67% of cases from an Indian population, the MMC orifice was located in the middle of the MB and ML orifice and 20% had the orifice closer to the ML canal, while the remaining 12% had the orifices located closer to the MB canal. In contrast, Karapinar-Kazandag et al.[7] reported a higher number of canals closer to either the ML or the MB canal in their study which employed magnifying loupes. Nosrat et al.,[33] in a study on a population from the USA, demonstrated that the MMC was located closer to the ML canal in a majority of the cases, followed by in the middle of the MB and ML canals. In a study by de Toubes et al.,[81] more number of MMC was identified close to the MB (46%) than to the ML (31%) canal, while 23% were located at the center.
There are case reports also of variations in the location of the middle canal orifice. Deepalakshmi et al.[70] reported four cases of MMC in mandibular first molars in which the middle canal was present at equidistance between the two mesial canals. De Moor RJ et al.,[60] presented two cases of MMC, one located almost equidistant from the two main canals of a left mandibular first molar and the other located very close to the MB canal of a right mandibular first molar.
Geographical distribution of middle mesial canal
Middle canals have been reported in Europeans, Asians, Africans and South and North Americans. The findings of studies have also pointed to geographical difference [Figure 3]. Nosrat et al.[33] and Versiani et al.[36] found significant differences in the incidence of MMC between White (12.2%) and non-White (29.4%) patients and Brazilian and Turkish populations, respectively.
Figure 3.

Geographic distribution of prevalence of middle mesial canal
Relation of prevalence of middle mesial canal to number of distal canals
Sherwani et al.[35] observed that MMC is more prevalent in mandibular first molars which have two distal canals (45.4%) than in those with one distal canal (13.7%). In contrast, Nosrat et al.[33] found no significant association between MMC and the presence of separate distal canals.
Prevalence of configuration types
The early studies reported only independent configurations of middle canals.[1,2] However, with the introduction of the classification of configuration types by Pomeranz et al.,[8] the other types were also observed. De Pablo et al.,[82] reported an equal incidence of independent and confluent MMC at the apical third. In contrast, Pomeranz et al.[8] identified more numbers of fin configuration (two MB fins and six ML fins) than confluent configuration. Fabra-Campos[13] reported an increased frequency of confluent configuration compared to fin or independent configurations. Confluence to MB canal in the apical third was more prevalent (65%) than to ML canal in the same area. Prevalence of confluent configuration has also been reported by other researchers[9,33,34,35] to lie between 46.7% and 96%. Furri[83] observed a greater prevalence of confluent canals in teeth with MMC than in those with DMMC in both first and second mandibular molars.
Karapinar-Kazandag et al.[7] reported all MMC to have confluent anatomy with no incidence of independent or fin anatomy, but with the confluency pattern differing between the first and second molars. In the former, the middle canal frequently crossed the midline and merged with the MB canal, whereas in the latter, it more frequently merged with the ML canal. de Toubes et al.[81] reported that a higher number of MMC connected to the MB (54%) than to the ML (38%) canal.
Confluence configuration in MDC has also been reported. In this case, the distobuccal and mid-distal canals joined at the middle third of the root and exited through a single apical foramen while the distolingual canal had a separate orifice and foramen. A case of MMC and MDC confluence configuration in both mesial and distal roots of a mandibular first molar has also been reported.[68]
Location of confluence of the main and middle canals
Beatty and Interian[41] reported a case of confluence of MDC with the distolingual canal in its apical third and with the distobuccal canal in its coronal third in a mandibular first molar. Gupta et al.[71] reported that MMC and MDC were found confluent with their respective mesial/distal buccal canals at the junction of the middle and apical one-thirds, indicating the presence of three orifices and two apical foramina in each root. Versiani et al.[36] reported the MMC to be more frequently confluent with the MB (16.7%) than the ML (8.3%) canal in their Brazilian population.
Case reports also report confluence to either the MB[13,48,49] or the ML canal.[44,45]
Case reports of the prevalence of middle canals
Mandibular first molar with MMC[3,42,43,44,45,46,48,49,52,53,54,55,56,59,60,61,67,70,71,72,73,74,80]
Mandibular first molar with MMC and MDC[3,53,55,56,71,73,80]
Mandibular first and second molar with double middle mesial[47,50,66,75,78]
Mandibular first molar with double distal canal[63,76,77,79]
Mandibular first molar with DMMC and MDC[47]
Mandibular second molar with DMMC and MDC[78]
Mandibular first molar with DMMC and double MDC[77]
Mandibular first molar with one distal root with three canals at orifice exiting as two canals[64]
Mandibular first molar with two distal roots, with one canal at the orifice and apex in one root and two canals at the orifice exiting as one canal at the apex in the other root[40,41]
Mandibular first molar with two distal roots with two independent canals in each root[63]
Mandibular first molar with three distal roots with one canal in each root[42,57,62]
Mandibular first molar with four separate distal roots and one canal in each root[62]
Mandibular second molar with one canal each in the distal root and radix paramolaris and three canals in the mesial root, i.e., a total of five canals[84]
Mandibular permanent second molar with four roots (two mesial and two distal) and root canals – mesial roots were separated in the cervical one-third near the cervical margin, while the distal roots were divided at a lower level in the middle one-third of the root.[26]
Isthmus versus middle canal
An isthmus is a narrow connection between two root canals that contains pulp tissue. Harris et al.[29] employed micro CT to detect isthmuses and reported their presence in 100% of their specimens. The extension of the isthmus coronally from the apex has been reported to be up to 3–5 mm[85] and between 4 mm and 6 mm.[86,87] Mannocci et al.,[88] employing micro-CT, found isthmuses at all levels but also reported more prevalence at 3 mm from the apex than at 1 mm. Mortman and Ahn[48] suggested that the middle canal is not an extra canal; rather, it develops due to instrumentation in the isthmus area.
Correlation of middle mesial canals with age
Several authors[89,90,91] have suggested that third canals are more likely to be found in younger patients. This may be attributed to the fact that roots undergo different stages of development with age. The mandibular first molars erupt at 6–7 years of age; apical closure, however, is completed at 8–9 years of age. The completion of canal differentiation commences at about 3–6 years after root completion. Furthermore, ages ranging from 12 to 20 years had mixed patterns of canal morphology; therefore, these periods seem to be a transition period for canal differentiation. Hess[92] explained that differentiation of the root canals appears by deposition of secondary dentine within the canal at the cervical, middle and apical thirds in the mesiodistal direction. This causes canal separation. Hence, when the tooth shows only one mesial root canal in the mandibular molar, it is possible that the differentiation of root canals has not been completed. Peiris et al.[93] also confirmed that canal differentiation is completed at around 30–40 years of age in both first and second molars. At this age, there are more chances for development of middle canal in the mandibular molar. Azim et al.[9] correlated the occurrence of MMCs with patients' ages and concluded that younger patients aged 30–40 years had a significantly higher incidence of an MMC. Nosrat et al.[33] reported that the incidence of negotiable MMCs overall and their frequency of identification were higher in younger patients, i.e., 32.1% in patients ≤30 years old, 23.8% in patients 30–40 years old and 3.8% in patients >40 years. Similar results were reported by Sherwani et al.,[35] who observed that there was a significant decrease in the incidence of MMCs with an increase in age in an Indian population.
Methodologies employed to study morphology and prevalence of middle canals
When comparing methodologies, the clearing technique was the most frequently used in-vitro technique,[1,82] although most contemporary research used 3D imaging systems such as CBCT and micro CTs. Of these, micro CT provided a better assessment of fine anatomical structures because of the possibility of using a higher exposure time and lower voxel sizes than CBCT. Another significant advantage was that a large number of sections were available for each mm.
Of the in-vivo methods, 2D periapical radiography was the most commonly used. The DOM was an important aid in locating additional canals. Karapinar-Kazandag et al.[7] reported that more number of MMC was detected with magnifying loupes or DOM, a finding that was corroborated by de Carvalho and Zuolo.[17] However, the evaluation of root canal systems was most accurate when the investigator explored clinically the interior of a tooth.
Various case reports also support the use of magnification for the detection of extra canals. Deepalakshmi et al.[70] reported four cases of MMC in the mandibular first molar detected using the DOM. They observed that enhanced lighting and visibility allows the identification of subtle color changes, a better understanding of the pulp floor map and fine instrumentation, while the coaxial illumination and magnification improves identification of extra canals. Srinivasan and Ravishanker[60] have described the successful nonsurgical management of two cases of mandibular first molar with MMC under magnification and illumination. Chavda and Garg[34] reported that the sensitivity of magnification in detecting middle canals in mandibular molars is the same as that of CBCT analysis.
3D imaging such as spiral CT was also used to confirm the presence of middle canal after an extra canal was suspected in conventional radiography.[73] Newer technologies such as 3D digital reconstruction and computer-aided rapid prototyping were used in a case to visualize the bifurcation of the distal root in mandibular first molar.[60] In this technique, a physical model was prepared by selectively solidifying ultraviolet-sensitive liquid resin using a laser beam. Paul and Dube[94] supported the use of 3D imaging with CBCT as an adjunct to digital radiography for the identification of MMC. Nance et al.[95] observed that tuned-aperture CT system of digital imaging was superior to conventional film for the detection of root canals that will probably be missed upon conventional X-ray examination. An advantage of CBCT over DOM was that it allowed the morphologic visualization of the canal trajectory, mainly in the mid- and apical-thirds of the roots, whereas visualization with DOM was limited to the straight portion of the canal.[5]
An innovative technique was used in one study to observe the root canal confluence configuration. In this, after negotiating the root canal system, the “straightest” canal of each root was instrumented. A gutta-percha cone was placed in the canal and a small file (#08 or #10) was inserted to the working length and then removed in all other canals. The gutta-percha cone was removed and inspected for notches indicating the presence of confluence.[83]
Clinically troughing the mesial pulpal groove in a mesio-apical direction away from the furcation is a significant factor in detection and negotiation of MMCs. A recent in-vivo study[13] has demonstrated that 39.6% more MMCs were detected and explored after controlled troughing to within 2 mm depth using a 1 mm diameter round bur head as a depth guide. This observation is in agreement with that of Chavda and Garg,[34] Ricucci[46] and Barletta et al.[58]
A literature search reveals various case reports on MDC with different configurations-one distal root with three canals at the orifice exiting as two canals,[44,63] two distal roots with one canal at the orifice and apex in one root and two canals at the orifice exiting as one canal at the apex in the other root,[36,37] two distal roots with two independent canals in each root[60] and three distal roots with one canal in each root.[38,39,59]
CONCLUSION
According to morphological studies, a complete isthmus between the main canals results in a middle canal. Middle canal varies in morphology and anatomic location. Its orifice is smaller in diameter and may or may not be equidistant from the orifice of the main canals. During its course, it may exist independently or may be confluent with the main canal. A few studies have reported that ethnicity affects the prevalence of the middle canal.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Barker BC, Lockett BC, Parsons KC. The demonstration of root canal anatomy. Aust Dent J. 1969;14:37–41. doi: 10.1111/j.1834-7819.1969.tb03330.x. [DOI] [PubMed] [Google Scholar]
- 2.Vertucci FJ, Williams RG. Root canal anatomy of the mandibular first molar. J N J Dent Assoc. 1974;45:27–8. [PubMed] [Google Scholar]
- 3.Martinez-Berna A, Badanelli P. Mandibular first molars with six root canals. J Endod. 1985;11:348–52. doi: 10.1016/S0099-2399(85)80043-1. [DOI] [PubMed] [Google Scholar]
- 4.Fabra-Campos H. Three canals in the mesial root of mandibular first permanent molars: A clinical study. Int Endod J. 1989;22:39–43. doi: 10.1111/j.1365-2591.1989.tb00503.x. [DOI] [PubMed] [Google Scholar]
- 5.Navarro LF, Luzi A, García AA, García AH. Third canal in the mesial root of permanent mandibular first molars: Review of the literature and presentation of 3 clinical reports and 2 in vitro studies. Med Oral Patol Oral Cir Bucal. 2007;12:E605–9. [PubMed] [Google Scholar]
- 6.Holtzmann L. Root canal treatment of a mandibular first molar with three mesial root canals. Int Endod J. 1997;30:422–3. doi: 10.1046/j.1365-2591.1997.00106.x. [DOI] [PubMed] [Google Scholar]
- 7.Karapinar-Kazandag M, Basrani BR, Friedman S. The operating microscope enhances detection and negotiation of accessory mesial canals in mandibular molars. J Endod. 2010;36:1289–94. doi: 10.1016/j.joen.2010.04.005. [DOI] [PubMed] [Google Scholar]
- 8.Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7:565–8. doi: 10.1016/S0099-2399(81)80216-6. [DOI] [PubMed] [Google Scholar]
- 9.Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification: An in vivo investigation. J Endod. 2015;41:164–8. doi: 10.1016/j.joen.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 10.Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. Int Endod J. 2004;37:494–9. doi: 10.1111/j.1365-2591.2004.00837.x. [DOI] [PubMed] [Google Scholar]
- 11.Sperber GH, Moreau JL. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J. 1998;31:117–22. doi: 10.1046/j.1365-2591.1998.00126.x. [DOI] [PubMed] [Google Scholar]
- 12.Bader JD. Systematic reviews and their implications for dental practice. Tex Dent J. 2004;121:380–7. [PubMed] [Google Scholar]
- 13.Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod. 1985;11:568–72. doi: 10.1016/S0099-2399(85)80204-1. [DOI] [PubMed] [Google Scholar]
- 14.Walker RT. Root form and canal anatomy of mandibular first molars in a Southern Chinese population. Endod Dent Traumatol. 1988;4:19–22. doi: 10.1111/j.1600-9657.1988.tb00287.x. [DOI] [PubMed] [Google Scholar]
- 15.Cunningham CJ, Senia ES. A three-dimensional study of canal curvatures in the mesial roots of mandibular molars. J Endod. 1992;18:294–300. doi: 10.1016/s0099-2399(06)80957-x. [DOI] [PubMed] [Google Scholar]
- 16.Calişkan MK, Pehlivan Y, Sepetçioǧlu F, Türkün M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995;21:200–4. doi: 10.1016/S0099-2399(06)80566-2. [DOI] [PubMed] [Google Scholar]
- 17.de Carvalho MC, Zuolo ML. Orifice locating with a microscope. J Endod. 2000;26:532–4. doi: 10.1097/00004770-200009000-00012. [DOI] [PubMed] [Google Scholar]
- 18.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34:359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 19.Wasti F, Shearer AC, Wilson NH. Root canal systems of the mandibular and maxillary first permanent molar teeth of South Asian Pakistanis. Int Endod J. 2001;34:263–6. doi: 10.1046/j.1365-2591.2001.00377.x. [DOI] [PubMed] [Google Scholar]
- 20.Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J. 2002;35:56–62. doi: 10.1046/j.1365-2591.2002.00452.x. [DOI] [PubMed] [Google Scholar]
- 21.Sarkar S, Rao AP. Number of root canals, their shape, configuration, accessory root canals in radicular pulp morphology. A preliminary study. J Indian Soc Pedod Prev Dent. 2002;20:93–7. [PubMed] [Google Scholar]
- 22.Villegas JC, Yoshioka T, Kobayashi C, Suda H. Frequency of transverse anastomoses with and without apical communication in Japanese population teeth. Aust Endod J. 2004;30:50–2. doi: 10.1111/j.1747-4477.2004.tb00178.x. [DOI] [PubMed] [Google Scholar]
- 23.Ahmed HA, Abu-bakr NH, Yahia NA, Ibrahim YE. Root and canal morphology of permanent mandibular molars in a Sudanese population. Int Endod J. 2007;40:766–71. doi: 10.1111/j.1365-2591.2007.1283.x. [DOI] [PubMed] [Google Scholar]
- 24.Al-Qudah AA, Awawdeh LA. Root and canal morphology of mandibular first and second molar teeth in a Jordanian population. Int Endod J. 2009;42:775–84. doi: 10.1111/j.1365-2591.2009.01578.x. [DOI] [PubMed] [Google Scholar]
- 25.Chen G, Yao H, Tong C. Investigation of the root canal configuration of mandibular first molars in a Taiwan Chinese population. Int Endod J. 2009;42:1044–9. doi: 10.1111/j.1365-2591.2009.01619.x. [DOI] [PubMed] [Google Scholar]
- 26.Peiris R, Takahashi M, Sasaki K, Kanazawa E. Root and canal morphology of permanent mandibular molars in a Sri Lankan population. Odontology. 2007;95:16–23. doi: 10.1007/s10266-007-0074-8. [DOI] [PubMed] [Google Scholar]
- 27.Gu L, Wei X, Ling J, Huang X. A microcomputed tomographic study of canal isthmuses in the mesial root of mandibular first molars in a Chinese population. J Endod. 2009;35:353–6. doi: 10.1016/j.joen.2008.11.029. [DOI] [PubMed] [Google Scholar]
- 28.Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, et al. Evaluation of the root and canal morphology of mandibular first permanent molars in a Western Chinese population by cone-beam computed tomography. J Endod. 2010;36:1786–9. doi: 10.1016/j.joen.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 29.Harris SP, Bowles WR, Fok A, McClanahan SB. An anatomic investigation of the mandibular first molar using micro-computed tomography. J Endod. 2013;39:1374–8. doi: 10.1016/j.joen.2013.06.034. [DOI] [PubMed] [Google Scholar]
- 30.Kim SY, Kim BS, Woo J, Kim Y. Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population: Variations in the number of roots and canals. J Endod. 2013;39:1516–21. doi: 10.1016/j.joen.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 31.Kucukkaya S, Nagas E, Tatar I, Celik H, Gorduysus MO. Middle mesial canal in mandibular first molar: A micro CT study. ECDS NAL. 2014;1:4–10. [Google Scholar]
- 32.Mukhaimer RH. Evaluation of root canal configuration of mandibular first molars in a Palestinian population by using cone-beam computed tomography: An ex vivo study. Int Sch Res Notices 2014. 2014 doi: 10.1155/2014/583621. 583621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: Incidence and related factors. J Endod. 2015;41:28–32. doi: 10.1016/j.joen.2014.08.004. [DOI] [PubMed] [Google Scholar]
- 34.Chavda SM, Garg SA. Advanced methods for identification of middle mesial canal in mandibular molars: An in vitro study. Endodontology. 2016;28:92–6. [Google Scholar]
- 35.Sherwani OA, Kumar A, Tewari RK, Mishra SK, Andrabi SM, Alam S. Frequency of middle mesial canals in mandibular first molars in North Indian population – An in vivo study. Saudi Endod J. 2016;6:66–70. [Google Scholar]
- 36.Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch Oral Biol. 2016;61:130–7. doi: 10.1016/j.archoralbio.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 37.Goel NK, Gill KS, Taneja JR. Study of root canals configuration in mandibular first permanent molar. J Indian Soc Pedod Prev Dent. 1991;8:12–4. [PubMed] [Google Scholar]
- 38.Shahi S, Yavari HR, Rahimi S, Torkamani R. Root canal morphology of human mandibular first permanent molars in an Iranian population. J Dent Res Dent Clin Dent Prospects. 2008;2:20–3. doi: 10.5681/joddd.2008.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Berthiaume JT. Five canals in a lower first molar. J Mich Dent Assoc. 1983;65:213–4. [PubMed] [Google Scholar]
- 40.Stroner WF, Remeikis NA, Carr GB. Mandibular first molar with three distal canals. Oral Surg Oral Med Oral Pathol. 1984;57:554–7. doi: 10.1016/0030-4220(84)90316-5. [DOI] [PubMed] [Google Scholar]
- 41.Beatty RG, Interian CM. A mandibular first molar with five canals: Report of case. J Am Dent Assoc. 1985;111:769–71. doi: 10.14219/jada.archive.1985.0208. [DOI] [PubMed] [Google Scholar]
- 42.Quackenbush LE. Mandibular molar with three distal root canals. Endod Dent Traumatol. 1986;2:48–9. doi: 10.1111/j.1600-9657.1986.tb00123.x. [DOI] [PubMed] [Google Scholar]
- 43.Bond JL, Hartwell GR, Donnelly JC, Portell FR. Clinical management of middle mesial root canals in mandibular molars. J Endod. 1988;14:312–4. doi: 10.1016/S0099-2399(88)80033-5. [DOI] [PubMed] [Google Scholar]
- 44.Jacobsen EL, Dick K, Bodell R. Mandibular first molars with multiple mesial canals. J Endod. 1994;20:610–3. doi: 10.1016/S0099-2399(06)80088-9. [DOI] [PubMed] [Google Scholar]
- 45.DeGrood ME, Cunningham CJ. Mandibular molar with 5 canals: Report of a case. J Endod. 1997;23:60–2. doi: 10.1016/S0099-2399(97)80211-7. [DOI] [PubMed] [Google Scholar]
- 46.Ricucci D. Three independent canals in the mesial root of a mandibular first molar. Endod Dent Traumatol. 1997;13:47–9. doi: 10.1111/j.1600-9657.1997.tb00010.x. [DOI] [PubMed] [Google Scholar]
- 47.Reeh ES. Seven canals in a lower first molar. J Endod. 1998;24:497–9. doi: 10.1016/S0099-2399(98)80055-1. [DOI] [PubMed] [Google Scholar]
- 48.Mortman RE, Ahn S. Mandibular first molars with three mesial canals. Gen Dent. 2003;51:549–51. [PubMed] [Google Scholar]
- 49.Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: A case report and literature review. J Endod. 2004;30:185–6. doi: 10.1097/00004770-200403000-00015. [DOI] [PubMed] [Google Scholar]
- 50.Kontakiotis EG, Tzanetakis GN. Four canals in the mesial root of a mandibular first molar. A case report under the operating microscope. Aust Endod J. 2007;33:84–8. doi: 10.1111/j.1747-4477.2007.00068.x. [DOI] [PubMed] [Google Scholar]
- 51.Barletta FB, Dotto SR, Reis Mde S, Ferreira R, Travassos RM. Mandibular molar with five root canals. Aust Endod J. 2008;34:129–32. doi: 10.1111/j.1747-4477.2007.00089.x. [DOI] [PubMed] [Google Scholar]
- 52.Yesilsoy C, Porras O, Gordon W. Importance of third mesial canals in mandibular molars: Report of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e55–8. doi: 10.1016/j.tripleo.2009.03.019. [DOI] [PubMed] [Google Scholar]
- 53.Ryan JL, Bowles WR, Baisden MK, McClanahan SB. Mandibular first molar with six separate canals. J Endod. 2011;37:878–80. doi: 10.1016/j.joen.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 54.de Paula AF, Brito-Júnior M, Quintino AC, Camilo CC, Cruz-Filho AM, Sousa-Neto MD, et al. Three independent mesial canals in a mandibular molar: Four-year followup of a case using cone beam computed tomography. Case Rep Dent 2013. 2013 doi: 10.1155/2013/891849. 891849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Maniglia-Ferreira C, Gomes Fde A, Sousa BC. Management of six root canals in mandibular first molar. Case Rep Med 2015. 2015 doi: 10.1155/2015/827070. 827070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Martins JN, Anderson C. Endodontic treatment of the mandibular first molar with six roots canals – Two case reports and literature review. J Clin Diagn Res. 2015;9:ZD06–8. doi: 10.7860/JCDR/2015/11866.5779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Friedman S, Moshonov J, Stabholz A. Five root canals in a mandibular first molar. Dent Traumatol. 1986;2:226–8. doi: 10.1111/j.1600-9657.1986.tb00150.x. [DOI] [PubMed] [Google Scholar]
- 58.Takeda FH, Harashima T, Kimura Y, Matsumoto K. A comparative study of the removal of smear layer by three endodontic irrigants and two types of laser. Int Endod J. 1999;32:32–9. doi: 10.1046/j.1365-2591.1999.00182.x. [DOI] [PubMed] [Google Scholar]
- 59.Min Ks. Clinical management of a mandibular first molar with multiple mesial canals: A case report. J Contemp Dent Pract. 2004;5:142–9. [PubMed] [Google Scholar]
- 60.de Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: An endodontic challenge. Int Endod J. 2004;37:789–99. doi: 10.1111/j.1365-2591.2004.00870.x. [DOI] [PubMed] [Google Scholar]
- 61.Chang SF. Re-treatment of a mandibular first molar with five canals-case report. J Dent Sci. 2006;1:74–8. [Google Scholar]
- 62.Lee SJ, Jang KH, Spangberg LS, Kim E, Jung IY, Lee CY, et al. Three-dimensional visualization of a mandibular first molar with three distal roots using computer-aided rapid prototyping. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:668–74. doi: 10.1016/j.tripleo.2005.06.013. [DOI] [PubMed] [Google Scholar]
- 63.Ghoddusi J, Naghavi N, Zarei M, Rohani E. Mandibular first molar with four distal canals. J Endod. 2007;33:1481–3. doi: 10.1016/j.joen.2007.08.018. [DOI] [PubMed] [Google Scholar]
- 64.Chandra SS, Rajasekaran M, Shankar P, Indira R. Endodontic management of a mandibular first molar with three distal canals confirmed with the aid of spiral computerized tomography: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e77–81. doi: 10.1016/j.tripleo.2009.06.017. [DOI] [PubMed] [Google Scholar]
- 65.Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: A case report and literature review. Int Endod J. 2010;43:714–22. doi: 10.1111/j.1365-2591.2010.01737.x. [DOI] [PubMed] [Google Scholar]
- 66.Aminsobhani M, Bolhari B, Shokouhinejad N, Ghorbanzadeh A, Ghabraei S, Rahmani MB, et al. Mandibular first and second molars with three mesial canals: A case series. Iran Endod J. 2010;5:36–9. [PMC free article] [PubMed] [Google Scholar]
- 67.La SH, Jung DH, Kim EC, Min KS. Identification of independent middle mesial canal in mandibular first molar using cone-beam computed tomography imaging. J Endod. 2010;36:542–5. doi: 10.1016/j.joen.2009.11.008. [DOI] [PubMed] [Google Scholar]
- 68.Jain S. Mandibular first molar with three distal canals. J Conserv Dent. 2011;14:438–9. doi: 10.4103/0972-0707.87223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Mushtaq M, Farooq R, Rashid A, Robbani I. Spiral computed tomographic evaluation and endodontic management of a mandibular first molar with three distal canals. J Conserv Dent. 2011;14:196–8. doi: 10.4103/0972-0707.82602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Deepalakshmi M, Karumaran CS, Miglani R, Indira R. Independent and confluent middle mesial root canals in mandibular first molars: A report of four cases. Case Rep Dent 2012. 2012 doi: 10.1155/2012/103125. 103125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Gupta S, Jaiswal S, Arora R. Endodontic management of permanent mandibular left first molar with six root canals. Contemp Clin Dent. 2012;3:S130–3. doi: 10.4103/0976-237X.95124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Karunakaran JV, Shobana R, Kumar M, Kumar S, Mankar S. Management of middle mesial canal in mandibular second molar. J Pharm Bioallied Sci. 2012;4:S161–4. doi: 10.4103/0975-7406.100259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Aksel H, Serper A. Mandibular first molars with a medial root canal. J Dent Sci. 2013;8:205–6. [Google Scholar]
- 74.Nayak BG, Singh I. Using spiral computed tomography for endodontic management of a mandibular first molar with a middle mesial canal: A case report. Gen Dent. 2013;61:43–6. [PubMed] [Google Scholar]
- 75.Subbiya A, Kumar KS, Vivekanandhan P, Prakash V. Management of mandibular first molar with four canals in mesial root. J Conserv Dent. 2013;16:471–3. doi: 10.4103/0972-0707.117495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Baziar H, Daneshvar F, Mohammadi A, Jafarzadeh H. Endodontic management of a mandibular first molar with four canals in a distal root by using cone-beam computed tomography: A case report. J Oral Maxillofac Res. 2014;5:e5. doi: 10.5037/jomr.2014.5105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Arora A, Acharya SR, Sharma P. Endodontic treatment of a mandibular first molar with 8 canals: A case report. Restor Dent Endod. 2015;40:75–8. doi: 10.5395/rde.2015.40.1.75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Kottoor J, Paul KK, Mathew J, George S, Mathew J, Roy A, et al. Apermanent mandibular second molar with seven root canal systems. Quintessence Int. 2014;45:381–3. doi: 10.3290/j.qi.a31537. [DOI] [PubMed] [Google Scholar]
- 79.Sinha N, Singh B, Langaliya A, Mirdha N, Huda I, Jain A, et al. Cone beam computed topographic evaluation and endodontic management of a rare mandibular first molar with four distal canals. Case Rep Dent 2014. 2014 doi: 10.1155/2014/306943. 306943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Hasan M, Rahman M, Saad N. Mandibular first molar with six root canals: A rare entity. BMJ Case Rep 2014. 2014:pii: bcr2014205253. doi: 10.1136/bcr-2014-205253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.de Toubes KM, Côrtes MI, Valadares MA, Fonseca LC, Nunes E, Silveira FF, et al. Comparative analysis of accessory mesial canal identification in mandibular first molars by using four different diagnostic methods. J Endod. 2012;38:436–41. doi: 10.1016/j.joen.2011.12.035. [DOI] [PubMed] [Google Scholar]
- 82.De Pablo OV, Estevez R, Sanchez MP, Heilborn C, Cobenca C. Root anatomy and canal configuration of the permanent mandibular first molar: A systematic review. J Endod. 2010;36:1919–31. doi: 10.1016/j.joen.2010.08.055. [DOI] [PubMed] [Google Scholar]
- 83.Furri M. Differences in the confluence of mesial canals in mandibular molar teeth with three or four root canals. Int Endod J. 2008;41:777–80. doi: 10.1111/j.1365-2591.2008.01431.x. [DOI] [PubMed] [Google Scholar]
- 84.Ragavendran N, Bhat GT, Hegde MN. Mandibular second molar with 3 mesial canals and a radix paramolaris. J Pharm Bioallied Sci. 2014;6:S182–4. doi: 10.4103/0975-7406.137461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Teixeira FB, Sano CL, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ, et al. Apreliminary in vitro study of the incidence and position of the root canal isthmus in maxillary and mandibular first molars. Int Endod J. 2003;36:276–80. doi: 10.1046/j.1365-2591.2003.00638.x. [DOI] [PubMed] [Google Scholar]
- 86.Fan B, Pan Y, Gao Y, Fang F, Wu Q, Gutmann JL, et al. Three-dimensional morphologic analysis of isthmuses in the mesial roots of mandibular molars. J Endod. 2010;36:1866–9. doi: 10.1016/j.joen.2010.08.030. [DOI] [PubMed] [Google Scholar]
- 87.von Arx T, Steiner RG, Tay FR. Apical surgery: Endoscopic findings at the resection level of 168 consecutively treated roots. Int Endod J. 2011;44:290–302. doi: 10.1111/j.1365-2591.2010.01811.x. [DOI] [PubMed] [Google Scholar]
- 88.Mannocci F, Peru M, Sherriff M, Cook R, Pitt Ford TR. The isthmuses of the mesial root of mandibular molars: A micro-computed tomographic study. Int Endod J. 2005;38:558–63. doi: 10.1111/j.1365-2591.2005.00994.x. [DOI] [PubMed] [Google Scholar]
- 89.Weine FS. Case report: Three canals in the mesial root of a mandibular first molar. J Endod. 1982;8:517–20. doi: 10.1016/S0099-2399(82)80080-0. [DOI] [PubMed] [Google Scholar]
- 90.Fabra-Campos H. The problem of lower first molars in endodontic treatment. Rev Esp Endodoncia. 1983;1:135–53. [PubMed] [Google Scholar]
- 91.Martínez-Berná A, Ruiz-Badanelli P. Maxillary first molars with six canals. J Endod. 1983;9:375–81. doi: 10.1016/S0099-2399(83)80188-5. [DOI] [PubMed] [Google Scholar]
- 92.Hess W. Formation of Root-Canals in Human Teeth I. J Nat Dent Assoc. 1921;8:704–34. [Google Scholar]
- 93.Peiris HR, Pitakotuwage TN, Takahashi M, Sasaki K, Kanazawa E. Root canal morphology of mandibular permanent molars at different ages. Int Endod J. 2008;41:828–35. doi: 10.1111/j.1365-2591.2008.01428.x. [DOI] [PubMed] [Google Scholar]
- 94.Paul B, Dube K. Identification and endodontic management of middle mesial canal in mandibular second molar using cone beam computed tomography. Case Rep Dent 2015. 2015 doi: 10.1155/2015/867976. 867976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Nance R, Tyndall D, Levin LG, Trope M. Identification of root canals in molars by tuned-aperture computed tomography. Int Endod J. 2000;33:392–6. doi: 10.1046/j.1365-2591.2000.00330.x. [DOI] [PubMed] [Google Scholar]