

Abstract
BACKGROUND
Visibility of the periodontal ligament of mandibular third molars (M3) has been suggested as a method to estimate age.
AIM
To assess the accuracy of this method and compare the visibility of the periodontal ligament in the left M3 with the right M3. The sample was archived panoramic dental radiographs of 163 individuals (75 males, 88 females, age 16-53 years) with mature M3’s.
MATERIALS AND METHODS
Reliability was assessed using Kappa. Accuracy was assessed by subtracting chronological age from estimated age for males and females. Stages were cross-tabulated against age stages younger than and at least 18 and 21 years of age. Stages were compared in the left M3 and right M3.
RESULTS
Analysis showed excellent intra-observer reliability. Mean difference between estimated and chronological ages was 7.21 years (SD 5.16) for left M3 and 7.69 (SD 6.08) for right M3 in males and 6.87 (SD 5.83) for left M3 and 8.61 (SD 6.58) for right M3 in females. Minimum ages of stages 0 to 2 were younger than previously reported, despite a small sample of individuals younger than 18. The left and right M3 stage differed in 46% of the 85 individuals with readings from both side and estimated age differed from -10.5 to 12.2 years between left and right.
CONCLUSION
Accuracy of this method was between 6 and 8 years with an error of 5 to 6 years. The number of individuals with mature M3 apices younger than 18 years was small. The stage of visibility of the periodontal ligament differed between left and right in almost half of our sample with both teeth present. Our findings question the use of this method to estimate age or to discriminate between age younger and at least 18 years.
Keywords: periodontal ligament, age estimation, third molars, mandibular
INTRODUCTION
Olze et al. (2010) described a method of dental age estimation by visualisation of the periodontal ligament of the mandibular third molars (M3) from dental radiographs. (1) Their study was based on a large sample of dental radiographs in Germany aged 15-40 years. The method classifies the visualisation of periodontal ligament width into 4 stage from zero (entirely visible in both roots) to three (visible in only part of one root). This study reported the chronological age for each periodontal ligament visibility (PLV) grade including the minimum age, and suggested PLV was useful to distinguish between individuals younger than and at least 18 and 21 years of age.Another study described the chronological age of these PLV stages in a sample of dental radiographs in Portugal. (2) This second studyreported chronological age for each stage, and noted that the minimum age of PLV stages could not discriminate age at the 18 year threshold but was appropriate for the 21 year threshold in males but not females.
Methods of age estimation need to be tested, and their accuracy and error recorded. (3, 4) The aims of this study were to describe the accuracy estimating age by the periodontal ligament width visibility as described by Olze et al. and assess the suitability in assessing the age thresholds of 18 and 21 years. We also compared periodontal ligament width visibility stage in the left and right mandibular third molars if both were present, and assessed the impact of this on estimated age.
MATERIALS AND METHODS
Ethical approval by Queen Mary Ethics of Research Committee number QMERC2016/06.
The archived panoramic radiographic films were of dental patients of mixed ethnic groups attending the Dental Institute. Radiographs were selected by the second author if the mandibular left and/or right third molars (M3) were clearly visible, roots apices mature and teeth fully erupted. Exclusion criteria were incomplete root formation, caries, restorations and impacted/partially erupted M3’s. The sample was radiographs of 163 individuals consisting of 75 males (mean age 23.33, standard deviation (SD) 5.11, minimum 16.76, maximum 45.03) and 88 females (mean age 22.45, SD 5.36, minimum 16.32, maximum 53.94) shown in Figure 1.
Figure 1.
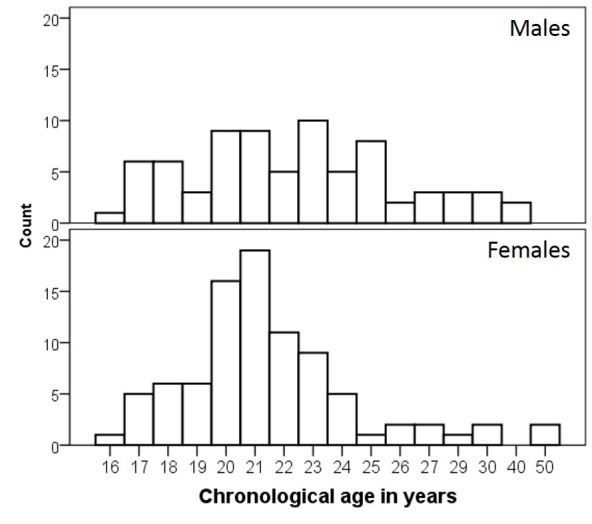
Age and sex distribution of radiographic sample of 75 males and 88 females.
The number of M3’s assessed on the left side was 128, right side 120 and both left and right M3 were present and included in the study in 85 individuals (total number of M3’s 248).
The periodontal ligament of M3’s was assessed by the first author on a light box after training and calibration. Each M3 was assigned into one of the four stages of periodontal ligament visibility (PLV) described by Olze et al. (2010). (1) This is illustrated in Figure 2;stage zero is defined as the periodontal ligament visible along the full length of all roots; stage 1 the periodontal ligament is invisible in one root from apex to more than half root; stage 2 is the invisible along almost the full length of one root or along part if the root in two roots or both; stage 3 the periodontal ligament is invisible along almost the full length of two roots.
Figure 2.
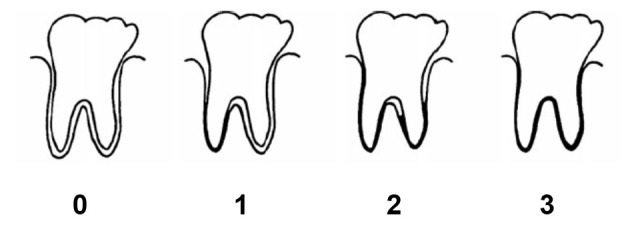
Periodontal ligament visibility stages adapted from Olze et al. (1)
To assess reliability, 40 teeth were selected from the sample (10 of each stage)and re-examined by the first author and examined by the second author. Intra- and inter-observer reliability were calculated using Cohen’s Kappa.
The mean chronological age, SD, minimum and maximum age of each PLV stage was calculated in males and females for left and right side M3.PLV and chronological age were cross tabulated into age stages less than 18, at least 18, less than 21 and at least 21 years of age to assess how well PLV stage discriminated at these age thresholds.
The accuracy of PLV as a method of age estimation was calculated by using the reference mean age of each stage (from Olze et al. 2010) to calculate dental age for left and right M3 in males in females. (1) The difference and absolute difference between dental and chronological ages was calculated and a t-test was used to assess the significance of the mean difference between dental and chronological ages.
The PLV stage was compared in the left and right side M3 if both were present in an individual and both were included in the selection criteria (N=85). The percentage agreement and Cohen’s Kappa calculated. The difference in dental age between the left and right M3’s was calculated for the individuals where PLV stage differed.
RESULTS
Intra-observer reliability value for Kappa was 0.898 (N=40). Inter-reliability Kappa value was 0.586.
Results of mean chronological age, SD, minimum and maximum age of each PLV stage in males and females for left and right side M3 are shown in Table 1. Results of mean age for the left M3 are illustrated in Figure 3 (dashed line is age 18 years). A notable finding is the large age range for all stages including zero (evident prior to 18 up to the late-twenties in this tooth). Most stages included individuals who were younger than 18 years of age. The minimum age of stages 1, 2 and 3 were in some cases younger than the minimum age of stage zero. The age range overlapped considerably between stages.
Table 1. Mean age, standard deviation (SD), minimum and maximum age of PLV category in left M3 and right M3 in males and females.
| Side | PLV | N | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
| Males | left | 0 | 5 | 20.28 | 3.86 | 17.38 | 26.89 |
| 1 | 7 | 20.77 | 3.11 | 16.76 | 25.06 | ||
| 2 | 25 | 21.98 | 3.48 | 17.79 | 31.18 | ||
| 3 | 22 | 25.70 | 5.34 | 20.86 | 45.03 | ||
| right | 0 | 3 | 22.50 | 5.85 | 18.04 | 29.13 | |
| 1 | 4 | 18.37 | 0.89 | 17.38 | 19.41 | ||
| 2 | 26 | 23.50 | 6.87 | 16.76 | 45.03 | ||
| 3 | 23 | 24.61 | 4.32 | 18.93 | 34.85 | ||
| Females | left | 0 | 11 | 21.59 | 2.66 | 17.70 | 27.10 |
| 1 | 12 | 20.05 | 2.21 | 17.64 | 24.19 | ||
| 2 | 33 | 21.56 | 2.59 | 16.32 | 29.41 | ||
| 3 | 13 | 26.42 | 8.22 | 18.16 | 50.37 | ||
| right | 0 | 3 | 18.70 | 1.10 | 17.70 | 19.88 | |
| 1 | 11 | 19.81 | 1.33 | 17.86 | 21.55 | ||
| 2 | 30 | 22.93 | 6.31 | 17.46 | 53.94 | ||
| 3 | 20 | 23.31 | 7.03 | 16.32 | 50.37 |
Figure 3.
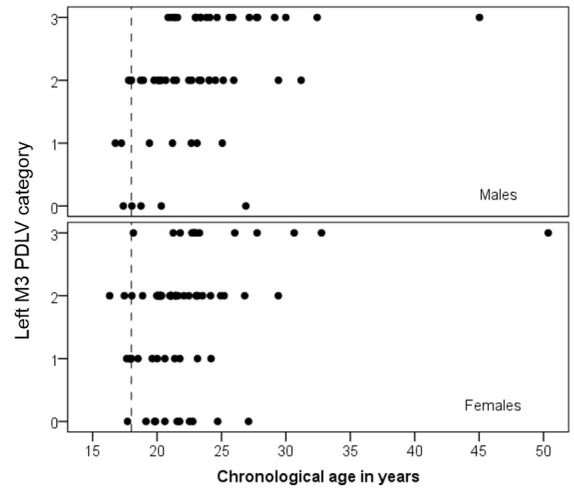
Periodontal ligament visibility stages and chronological age of left mandibular third molar (M3) in males and females. Dotted line is 18 years of age.
Results on the cross tabulation of age thresholds younger than or at least 18 and 21 years of age by PLV are shown in Table 2. No male in stage 3 was younger than 18 years of age (0/22 left M3 and 0/23 right M3). No females presented with left M3 in stage 3 but this differed to the right side where 1/20 was aged younger than 18.
Table 2. Cross tabulation of PLV category and age thresholds in years.
| Side | PLV | N | <18 | 18+ | <21 | 21+ | |
|---|---|---|---|---|---|---|---|
| Males | left | 0 | 5 | 1 | 4 | 4 | 1 |
| 1 | 7 | 2 | 5 | 3 | 4 | ||
| 2 | 25 | 3 | 22 | 12 | 13 | ||
| 3 | 22 | 0 | 22 | 1 | 21 | ||
| right | 0 | 3 | 0 | 3 | 2 | 1 | |
| 1 | 4 | 2 | 2 | 4 | 0 | ||
| 2 | 26 | 4 | 22 | 10 | 16 | ||
| 3 | 23 | 0 | 23 | 6 | 17 | ||
| Females | left | 0 | 11 | 1 | 10 | 5 | 6 |
| 1 | 12 | 3 | 9 | 8 | 4 | ||
| 2 | 33 | 2 | 31 | 13 | 20 | ||
| 3 | 13 | 0 | 13 | 1 | 12 | ||
| right | 0 | 3 | 1 | 2 | 3 | 0 | |
| 1 | 11 | 1 | 10 | 8 | 3 | ||
| 2 | 30 | 2 | 28 | 11 | 19 | ||
| 3 | 20 | 1 | 19 | 7 | 13 |
Results of the accuracy of estimating using PLV (Olze et al. 2010) (1) including the mean difference between dental and chronological ages, standard deviation, absolute mean difference, minimum and maximum age are shown in Table 3 (pooled stages) and Table 4 (by PLV stage). The mean difference between dental and chronological ages ranged from 6 to 8 years with a standard deviation of 5 or 6 years. In general terms, the mean difference between dental and chronological ages increased with PLV stage and most comparisons were statistically highly significant.
Table 3. Mean difference in years between estimated dental age and chronological age.
| Side | N | Mean | SD | significance | Absolute mean | |
|---|---|---|---|---|---|---|
| Males | left | 59 | 7.21 | 5.16 | 0.000 | 7.91 |
| right | 56 | 7.69 | 6.08 | 0.000 | 8.93 | |
| Females | left | 69 | 6.87 | 5.83 | 0.000 | 7.74 |
| right | 64 | 8.61 | 6.58 | 0.000 | 9.77 |
Table 4. Mean difference in years between estimated dental age and chronological ages by periodontal ligament visibility category.
| Side | PLV | Mean | SD | Significance | Absolute mean | N | |
|---|---|---|---|---|---|---|---|
| Males | left | 0 | 1.02 | 3.86 | NS | 3.26 | 5 |
| 1 | 1.63 | 3.11 | NS | 2.66 | 7 | ||
| 2 | 9.32 | 3.48 | 0.000 | 9.32 | 25 | ||
| 3 | 8.01 | 5.34 | 0.000 | 9.03 | 22 | ||
| right | 0 | -1.00 | 5.85 | NS | 4.09 | 3 | |
| 1 | 3.83 | 0.89 | 0.003 | 3.83 | 4 | ||
| 2 | 7.60 | 6.87 | 0.000 | 9.64 | 26 | ||
| 3 | 9.58 | 4.32 | 0.000 | 9.64 | 23 | ||
| Females | left | 0 | -0.49 | 2.66 | NS | 2.07 | 11 |
| 1 | 2.85 | 2.21 | 0.001 | 3.10 | 12 | ||
| 2 | 9.84 | 2.59 | 0.000 | 9.84 | 33 | ||
| 3 | 9.28 | 8.22 | 0.002 | 11.53 | 13 | ||
| right | 0 | 2.80 | 1.10 | 0.048 | 2.80 | 3 | |
| 1 | 3.69 | 1.33 | 0.000 | 3.69 | 11 | ||
| 2 | 8.67 | 6.31 | 0.000 | 10.16 | 30 | ||
| 3 | 12.09 | 7.03 | 0.000 | 13.59 | 20 |
The results of estimated age (dental age) plotted against chronological ages for males and females are illustrated in Figure 4.The diagonal line shows estimated age equal to chronological age. It is clear that only a few individuals are close to this line and age was over-estimated for most individuals.
Figure 4.

Scatter plot of dental age versus chronological age in years.Markers show periodontal ligament visibility stages 0 to 3. Diagonal line is dental age equal to chronological age.
Results comparing PLV stage of left M3 and right M3 in the 85 individuals with both teeth included in the study are shown in Table 5. Agreement in stage between left M3 and right M3 was evident in 46 out of the 85 individuals (54%). Differences between the left and right M3’s (N=39) were evident across all PLV stages. Kappa was 0.33. The difference in estimated age in years when the PLV differed between left and right side plotted against chronological age is illustrated in Figure 5. Estimated age differed as much as -10.5 to 12.2 years.
Table 5. Comparison of PLV categories of left M3 versus right M3 within the same individual.
| Right M3 | ||||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | Total | ||
| Left M3 | 0 | 4 | 4 | 3 | 0 | 11 |
| 1 | 3 | 6 | 8 | 0 | 15 | |
| 2 | 0 | 1 | 20 | 15 | 36 | |
| 3 | 1 | 0 | 6 | 16 | 23 | |
| Total | 6 | 11 | 37 | 31 | 85 | |
Figure 5.
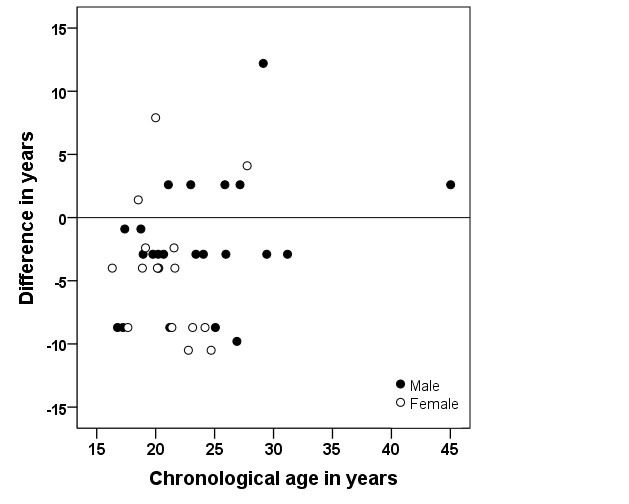
Accuracy of estimating age from PVL stage of left M3 plotted against right M3 in years. Line is accuracy left M3 equal to right M3.
DISCUSSION
The accuracy of PLV as an estimate of age has not previously been reported. The average difference between estimated age from PLV and chronological age ranged from 6 to 8 years with SD values as much as six years. Absolute mean values were from 7 to almost 10 years.
Our results show that there is considerable overlap in age between PLV categories and that there is poor discrimination when age is cross-tabulated into younger than 18 and at least 18 years of age. The minimum ages of PLV stages have been used to exclude individuals as being under 18 or 21 years of age by virtue of their PLV stage. Olze et al. concluded that an individual can be excluded as being under 18 if stages 1, 2 or 3 have been attained and stage 2 can be used to predict the age of 21. (1) Sequeira et al. report that stage 3 rather than stage 2 was a better predictor of the age of 21 years. (2) They report a lower minimum age of stage 2 than stage 1. Lucas et al. also report a lower minimum age of the second stage than the first stage. (5) It is clear from the studies reporting chronological age of PLV stages, that the number of individuals with mature apices of M3 younger than 18 years of age is not large and that the minimum age of PLV stages varies considerably. Our results illustrated in Figures 1 and 3, show that firstly, any sample that includes individuals with mature M3 apices is by its very nature small and secondly, the minimum age of PLV stages was younger than 18 for all stages in females and all but stage 3 in males. These findings demonstrate that the use of the minimum age of PLV stages is inappropriate to include or exclude individuals under 18 or 21 years of age.
The main inclusion criteria for our radiographic sample was mature apices of M3 and our sample of dental radiographs was small, particularly for individuals with mature M3 apices who were younger than 18 years of age. This lack of individuals younger than 18 with mature M3 root apices is of major importance particularly when PLV is used to estimate the likelihood of being younger than, or at least 18 years of age. None of the studies reporting chronological age of PLV stages (1, 2) or modifications thereof (5)detail the number of individuals below the age of 18 with mature M3 apices in their samples. The small number of individuals with mature apices younger than 18 has a bearing on the minimum age of PLV stages. Although Olze et al. (1) lists the number of males and females in one-year age stages, they do not report how many of the 17 year olds presented with mature M3 apices. They report a minimum age of stage 0 as 17.6 years in males and 17.2 years in females, suggesting that none of the 15 and 16 year olds presented with mature M3 apices. Sequira et al. (2) state that their inclusion criteria as the presence of mature M3 apices, however, confusingly, their results report the minimum age of M3 stage 0 in males as 18.2. This suggests that either the tables contain a typographical error or none of the 8 males aged 17 years of age had mature apices. Lucas et al. (5) modified the original definitions of PLV stages and assessed a large sample consisting of 100 males and 100 females per year of age from age 16. It can be deduced from their illustration that only 11 out of 200 females and 7 out of 200 males under 18 years of age have mature apices.
Exclusion criteria of any radiographic study are also important and are not always detailed. Two large radiographic studies (1, 5) appear to exclude a large proportion of individuals in their total sample (36% and 46% respectively). The reason for this in unclear. Sequira et al. (2) excluded impacted M3 or those with caries or endodontic treatment.
An important finding in our study was the lack of similarity between the left and right side M3 PLV stages (Table 5) and how this impacts on estimated age (Figure 5). A large percentage of individuals differed in PLV stage where both sides were included and this can result in a considerable difference in the estimated age. Few studies compare contra-lateral root shape of third molars from radiographs, however a recent 3D study showed similar M3 root morphology contra-laterally in 81% of a Korean sample i.e. 19% had dissimilar root morphology. (6) A limitation of our study was the small sample and the sequence of scoring. Ideally all left M3’s should have been scored and then all right side M3’s.
We report results on the accuracy and precision of estimating age using PLV. Reasons for this inaccuracy relates to the anatomy of the periodontal ligament, third molar root variation and difficulties visualising the ligament space. Coolidge (7)measured the periodontal ligament thickness from histological sections summarising findings to show that thickness varied between alveolar crest, mid-root and apex. This paper illustrates some individual results as bar charts and from these raw data, it is possible to calculate average thickness of the periodontal ligament (in hundredths of millimetres) at the alveolar crest in 166 individuals aged 11-16 years was 22.04 (SD 8.59) and in 73 individuals aged 32-50 years was 19.99 (SD 7.29). The mean value in the younger age group is smaller than the older group, however, this is not significantly different. They excluded one outlier, aged 25 with a considerably thinner periodontal ligament width. A study of periodontal ligament thickness from radiographs showed no clear pattern in measurements between erupted, un-erupted, functional or non-functional teeth. (8) The dimensions of the periodontal ligament varied between 259 and 267 microns for erupted M3 and 217 and 341 microns in un-erupted M3, with the maximum thickness seen in impacted M3. (8) The effect of other factors such as the presence of caries, restorations and endodontic treatment on the width of the periodontal ligament is unknown. Third molars with restorations are included in the illustrated examples of stages by Olze et al. (1) and an impacted M3 by Lucas et al. (5)
Factors that affect visualisation include the anatomic variation in third molar root morphology and the definition of PLV stages. The anatomy of third molar roots can affect the quality of the radiographic image. The ability of the radiograph to show fine detail (resolution) is measured in line pairs per millimetre and is the ability to discern the boundaries of two objects that are close together. The resolution of a panoramic radiograph is best at the centre of the focal trough but third molar roots may not be favourable placed for high resolution.
Third molars vary considerably in the number, shape and curvature of the roots as well as the separation or fusion of the roots, length of root trunk, bifurcation shape and apical curvature. This is particularly important in three dimensions for endodontics and surgical removal of M3, but also affect the visibility of PLV viewed in two dimensions seen radiographically. The line drawings in Olze et al. (1) depict a typical mandibular molar with two separate roots where the periodontal ligament is clearly visible outlining the mesial and distal root with a clear bifurcation between the roots. Root morphology of M3 is reviewed by Ahmed et al. (9)who reports that the M3 pattern of two separate roots is the most frequent with a prevalence in different studies of 82% (10), 77% (11), 74% (9), 73% (12), 69% (13), 68% (14), 57% (6), 46% (15) and 44% (16). The roots of M3 can curve towards each other with converging apices with no clear periodontal ligament space (illustrated in Figure 6a and b). If the roots are in close proximity for their entire length, the periodontal ligament space between the roots and at the furcation is not clearly visible (Figure 6c). The prevalence of fused roots of M3 is reported as 19% (14) and 24%. (17) Prevalence of C-shaped roots in cross-section is reported as 11%.14The prevalence of the pattern of a single rooted M3 ranges from 56% (16), 52% (15), 42% (6), 24% (13), 21% (12), 17% (11) to 12% (18). Other factors influencing the clarity of visualising the periodontal ligament of M3includes the proximity of the root apices to the inferior alveolar nerve or the mesial root of M3 being in close proximity to the distal root of the mandibular second molar (see Figure 6b).
Figure 6.
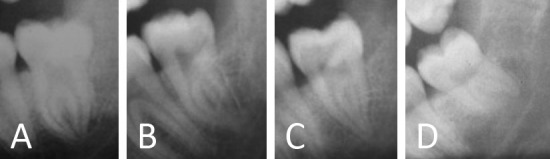
Examples of root morphology of M3 where PVL stage is difficult to visualise. (A) Root apices in close proximity. (B) Root apices overlapping. (C) Apical third of roots in close proximity (D) Mesial root curved and out of focal trough.
The PLV stage definitions have limitations. The drawing in Olze et al. (1) suggest that region of unclear PLV extends from the root apex towards the root trunk. In our experience, we noted areas where the PLV was not visible at the bifurcation while the rest of the ligament was visible. We also noted cases where an area of unclear ligament occurred on the lateral surface of a root with clear ligament space around the apex of that and the entire other root. Stage assessment defined by Olze et al. (1) requires training and calibration and the stages are not always easy to identify. Although intra-observer reliability of PLV stage was good, inter-observer reliability was less so, possibly due to the subjective nature of identifying grey levels that distinguish small visual differences that represent the edge of a ligament space adjacent to a curved root surface. (19) Future research on digital radiographs and image analysis software may help to quantify PLV stage.
An attempt to simplify PLV was made by Lucas et al. who adapted the four PLV stages into various percentages of the entire periodontal ligament. (5) Their categories A to D are defined as PLV as 100% visible, 75-50% visible, 50-25% visible and 0% visible respectively. These definitions omit a large proportion of cases (99-76% and 24-1%) and it is unclear how to assign a third molar with 50% of the periodontal ligament visible is it is both stage B and C.
Results of chronological age of each PLV stage in our study (Figure 3) shows that PLV is a poor maturity marker for several reasons. All PLV stages have a large age range with stage zero observed prior to 18 up to the late-twenties. Most PLV stages were present prior to 18 years of age and the age range overlapped considerably between PLV stages. In addition, the minimum age of PLV stages 1, 2 and 3 were in some cases younger than the minimum age of stage zero. The maximum age of PLV stages is also of interest. Both Olze et al. (1) and Sequira et al. (2) report a maximum age of stage 0 as 30 years (females left M3, males right M3). The considerable age overlap of each of the stages suggests that PLV varies considerably and is not an age related change that can reliably estimate age.
A limitation in our understanding of the rate of PLV is that all studies to date are based on cross-sectional radiographs. Quantifying the rate and severity of age related changes such as PLV of mandibular third molars in the same individual over time is possible from longitudinal radiographs. In the absence of such longitudinal data, we postulate that the nature and rate of increasing PLV stage with age is too variable to be of much practical use to estimate age accurately and is unsuitable to assess if an individual is below or at least 18 or 21 years of age.
CONCLUSION
Accuracy of PLV stage was between 6 and 8 years with an error of 5 to 6 years.
The number of individuals with mature M3 apices younger than 18 years was small.
The stage of visibility of the periodontal ligament differed between left and right in almost half of our sample with both teeth present.
Our findings question the use of this method to estimate age or to discriminate between age younger and at least 18 years.
REFERENCES
- 1.Olze A, Solheim T, Schulz R, Kupfer M, Pfeiffer H, Schmeling A. Assessment of the radiographic visibility of the periodontal ligament in the lower third molars for the purpose of forensic age estimation in living individuals. Int J Legal Med. 2010;124:445–8. 10.1007/s00414-010-0488-7 [DOI] [PubMed] [Google Scholar]
- 2.Sequeira CD, Teixeira A, Caldas IM, Afonso A, Pérez-Mongiovi D. Age estimation using the radiographic visibility of the periodontal ligament in lower third molars in a Portuguese population. J Clin Exp Dent. 2014;6:e546–50. 10.4317/jced.51813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ritz-Timme S, Cattaneo C, Collins MJ, Waite ER, Schütz HW, Kaatsch HJ, et al. Age estimation: The state of the art in relation to the specific demands of forensic practise. Int J Legal Med. 2000;113:129–36. 10.1007/s004140050283 [DOI] [PubMed] [Google Scholar]
- 4.Christensen AM, Crowder CM. Evidentiary standards for forensic anthropology. J Forensic Sci. 2009;54:1211–6. 10.1111/j.1556-4029.2009.01176.x [DOI] [PubMed] [Google Scholar]
- 5.Lucas VS, McDonald F, Andiappan M, Roberts G. Dental age estimation: periodontal ligament visibility (PLV)—pattern recognition of a conclusive mandibular maturity marker related to the lower left third molar at the 18-year threshold. Int J Legal Med. 2017;131:797–801. 10.1007/s00414-016-1468-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Park JB, Kim NR, Park S, Ko Y. Evaluation of number of roots and root anatomy of permanent mandibular third molars in a Korean population, using cone-beam computed tomography. Eur J Dent. 2013;7:296–301. 10.4103/1305-7456.115413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Coolidge EG. The thickness of the human periodontal membrane. J Am Dent Assoc. 1937;24:1260–70. [Google Scholar]
- 8.Richardson ER. Comparative thickness of the human periodontal membrane of functioning versus non-functioning teeth. J Oral Med. 1967;22:120–6. [PubMed] [Google Scholar]
- 9.Ahmed IA, Azzeh MM, Zwiri AMA, Abu Haija MS, Diab MM. Root and canal morphology of third molars in a Jordanian subpopulation. Saudi Endod J. 2016;6:113–21. 10.4103/1658-5984.189350 [DOI] [Google Scholar]
- 10.Zakhary SY, Fahim OM, Gorgy AA. Morphologic characteristics of lower third molar as related to successful endodontic therapy. Egypt Dent J. 1988;34:323–37. [PubMed] [Google Scholar]
- 11.Sidow SJ, West LA, Liewehr FR, Loushine RJ. Root canal morphology of human maxillary and mandibular third molars. J Endod. 2000;26:675–8. 10.1097/00004770-200011000-00011 [DOI] [PubMed] [Google Scholar]
- 12.Kuzekanani M, Haghani J, Nosrati H. Root and canal morphology of mandibular third molars in an Iranian population. J Dent Res Dent Clin Dent Prospects. 2012;6:85–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sert S, Sahinkesen G, Topcu FT, Eroglu SE, Oktay EA. Root canal configuration of third molar teeth. A comparison with first and second molars in the Turkish population. Aust Endod J. 2011;37:109–17. 10.1111/j.1747-4477.2010.00254.x [DOI] [PubMed] [Google Scholar]
- 14.Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J. 2002;35:56–62. 10.1046/j.1365-2591.2002.00452.x [DOI] [PubMed] [Google Scholar]
- 15.Guerisoli DMZ, De Souza RA, De Sousa Neto MD, Silva RG, Pecora JD. External and internal anatomy of third molars. Braz Dent J. 1998;9:91–4. [PubMed] [Google Scholar]
- 16.Cosić J, Galic N, Vodanovic M, Njemirovskij V, Segovic S, Pavelic B, et al. An in-vitro morphological investigation of the endodontic spaces of third molars. Coll Antropol. 2013;37:437–42. [PubMed] [Google Scholar]
- 17.Ross IF, Evanchik PA. Root fusion in molars: incidence and sex linkage. J Periodontol. 1981;52:663–7. 10.1902/jop.1981.52.11.663 [DOI] [PubMed] [Google Scholar]
- 18.Zakhary SY, Fahim OM, Gorgy AA. Morphologic characteristics of lower third molar as related to successful endodontic therapy. Egypt Dent J. 1988;34:323–37. [PubMed] [Google Scholar]
- 19.Bell GW, Rodgers JM, Grime JR, Edwards KL, Hahn MR, Dorman ML, et al. The accuracy of dental panoramic tomographs in determining the root morphology of mandibular third molar teeth before surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:119–25. 10.1067/moe.2003.16 [DOI] [PubMed] [Google Scholar]