

Abstract
Introduction:
In this study, we undertook a retrospective analysis of the epidemiological aspects and risk factors of murine typhus (MT) in Korea in the last decade (2006–2015).
Materials and Methods:
MT infections in Korea using a total of 411 cases obtained from the Diseases Web Statistical System of the Korea Center for Disease Control and Prevention.
Results:
In a total of 411 MT infection cases, the cumulative incidence rate was 0.08/100,000 populations. Men were slightly more infected by MT as compared to women (51.3% vs. 48.7%), and a higher incidence of MT was observed in people aged over 40 years (93.4%; P < 0.01). The seasonal pattern of outbreaks revealed that most infections occurred from October to November (69.1% of the total cases) (P < 0.01). Significantly more outbreaks occurred in the southern part (53.5%) of the Korean peninsula as compared to its northern (33.3%) and central (10.7%) parts, as well as the Jeju Island (1.0%) (P < 0.01). In addition, the number of MT infections was significantly higher in rural and sea-village (87.6%) than in urban areas (12.4%; P < 0.01).
Conclusion:
In conclusion, the rapid reemergence of MT outbreaks can be minimized through health education, and a strong enforcement of control measures against rats and their ectoparasites could markedly reduce the transmission of this infection to humans in high-risk areas.
Keywords: Epidemiological aspects, murine typhus, surveillance, The Republic of Korea
INTRODUCTION
Murine typhus (MT) is a widely spread arthropod-borne infectious zoonotic disease caused by Rickettsia typhi of the family Rickettsiaceae and maintained in nature through a cycle involving mainly commensal rodents (Rattus norvegicus and Rattus rattus) and their ectoparasites.[1,2,3,4] This disease occurs on every continent, except for Antarctica, and is observed in a variety of environments, ranging from hot and humid to cold and montane or semi-arid.[1] The classical transmission cycle for MT is rat–flea–rat and accidentally rat–flea–man.[1,2,3,4] Even today, the identities of all the vectors and reservoirs of MT, as well as the precise mode of transmission, remain unknown. For over 50 years, the consensus was that the flea Xenopsylla cheopis is the main vector and that transmission is affected not by bite, but only by contact with the rickettsia-containing feces, the tissue of infected fleas or lice.[1] It was also generally accepted that the fleas acquire their infection from rickettsemic commensal rats. However, recent reports demonstrate that rickettsia can also be transmitted by flea bites and maintained by transversal transmission.[1,5,6] Moreover, while MT is widely spread worldwide, it occurs primarily in ports and coastal towns where commensal rodents are prevalent.[1,2,3,4] In the case of the Republic of Korea, only several reports of MT were available until 1959.[7,8] However, there was a confirmed serological test of MT, for the first time in Korea, even though the occurrences of MT had been suspected (though not officially reported) before 1959.[8] Thereafter, MT occurred sporadically until the 1980s and the 1990s, and the emerged outbreaks were reported.[9,10] In Korea, MT has been classified as a Type III notifiable infectious disease by the Communicable Disease Prevention Act of the Korea Center for Disease Control and Prevention (KCDC), the Ministry of Health and Welfare.[9]
Between 2006 and 2015, a total of 411 cases of MT were the officially reported in South Korea by the national infectious disease surveillance system of the KCDC. However, there is scarce or no information concerning the prevention of and control measures for the epidemiological aspects and risk factors of MT in Korea. Therefore, to facilitate a more effectively planning of future strategies, the present study provides an investigative analysis of the epidemiological aspects and related risk factors of MT in Korea.
MATERIALS AND METHODS
This study sought to investigate the epidemiological aspects and related risk factors of MT infections in Korea using a total of 411 cases obtained from the Diseases Web Statistical System of the KCDC spanning the years from 2006 to 2015[9] under the following seven headings: (1) cumulative incidence rate (CIR) per 100,000 population; epidemiological aspects and risk factors including (2) gender; (3) male-to-female morbidity ratio (MFMR); (4) age of those affected; (5) seasonality; (6) geography; and (7) habitat of MT infections.
In this study, the CIR of MT was estimated by the World Health Organization established criteria, and the upper and lower limits of the 95% confirmed interval (CI) were calculated. Statistically significant differences between the epidemiological aspects and risk factors were determined using the Chi-square test and the paired t-test. All data analyses were performed in Excel 2007 (Microsoft Co., Redmond, WA, USA). The results were considered statistically significant at P < 0.05 and P < 0.01, respectively.
RESULTS
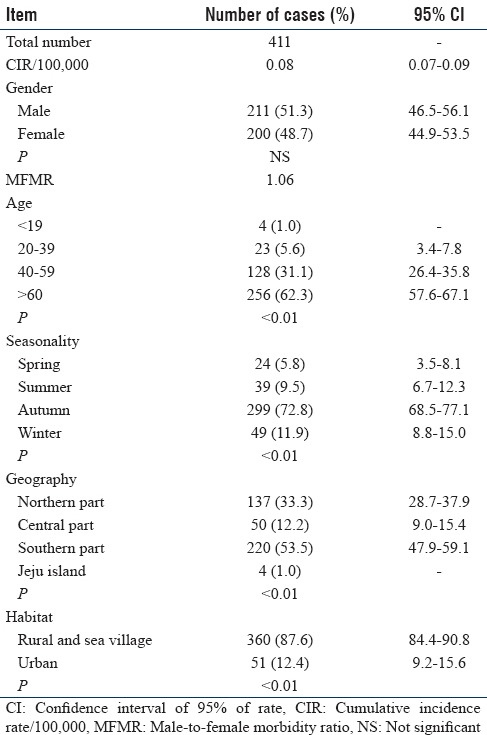
Table 1 summarizes the epidemiological aspects of MT cases reported in Korea in the last decade (2006 and 2015) which were analyzed by the association with CIR, as well as gender, age, seasonality, geography, and habitat risks of the affected individuals. There were a total of 411 MT infections from 2006 to 2015, and the CIR was 0.08 (95% CI, 0.07–0.09) per 100,000 population. Differences between men and women in response to infectious diseases are an overlooked public health concern. In Korea, a slightly higher number of men are infected (51.3%) as compared to women (48.7%). However, this difference does not reach statistical significance.
Table 1.
Epidemiological aspects and risk factors of murine typhus surveillance in Korea, in the years 2004-2015
The percentage distribution of MT infections of the total 411 cases by age was as follows: In the groups aged under 19, 20–39, 40–59, and over 60 years, the rates were 1.0%, 5.6%, 31.1%, and 62.3%, respectively (P < 0.01). The distribution by age group showed that over 93.4% of the cases occurred in the older-than-40-year age bracket, clearly showing a higher incidence rate in the elderly [Figure 1].
Figure 1.
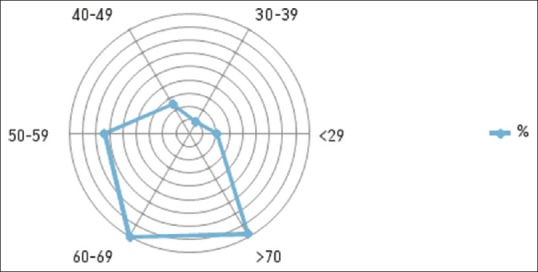
Distribution rate (%) of murine typhus outbreaks by age in Korea, in the years 2006–2015
With regard to the seasonal pattern, incidence cases among MT patients were 5.8%, 9.5%, 72.8%, and 11.9% in spring, summer, autumn, and winter, respectively (P < 0.01) [Figure 2].
Figure 2.
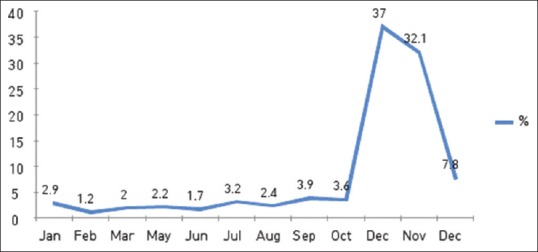
Distribution rate (%) of murine typhus outbreaks by month in Korea, in the years 2006–2015
These cases occurred predominantly from October to the end of November (69.1% of the total number of cases) of each year.
A summary of the incidence of MT infections in relation to geography revealed a significantly higher number of outbreaks in the southern part of the Korean Peninsula (53.5%) as compared to the northern (34.0%) and central parts (10.7%), as well as the Jeju Island (P < 0.01). Moreover, the distribution of MT cases was significantly higher in rural and sea-village (87.6%) than in urban areas (12.4%) (P < 0.01).
DISCUSSION
MT is an arthropod-borne infectious disease caused by R. typhi which is not spread from person to person. Clinically, the disease is characterized by high fever, headache, generalized pain, weakness, and a rash that, if present, is usually centrally distributed on the trunk.[1,4,10] In the case of Korea, MT occurred sporadically until the 1980s, when outbreaks were the first reported. However, the number of reported MT outbreaks in Korea rapidly increased after the 1990s to present.[9,10] Specifically, the number of MT cases sharply increased from nine cases in 2003 to 87 cases in 2008, when the disease was at its peak. However, in recent years, the number of MT cases fell from 41 in 2012 to 15 in 2015. In the present study, we analyzed a total of 411 MT cases with the CIR of 0.08/100,000 population between 2006 and 2015. On the other hand, in Japan, for example, MT may have reemerged due to the recent increase of black rats, R. rattus. This patient mentioned that they had captured a rat and disposed of carcass about a week before the onset of symptoms of MT.[2] Differences between men and women in response to in factious disease are an overlooked public health concern. In Korea, a slightly higher number of men are infected (51.3%) as compared to women (48.7%) although the difference is not statistically significant (MFMR was 1.06). However, this remarkable in gender distribution is believed to be due to cultural differences in terms of life types, clothing, and ornamentation.[8,10,11]
The percentage distribution by age group showed that over 93.4% of the cases occurred in the older-than-40-year age bracket, clearly showing a higher incidence rate in the elderly [Figure 1]. Moreover, a recent tendency in South Korea is that most young people move to cities for work and that elderly people are left behind to work as farmers and fishery on their own land.[10,11] Thus, the higher incidence in the elderly may be caused by an increased risk of infection due to their engagement in activities in rural and sea-village and urban areas, which are prone to MT outbreaks.[1,3,10,11]
It is well known that epidemic diseases, including MT infections, are affected by season and climate changes.
The observed seasonal pattern of incidence cases among MT patients was 5.8%, 9.5%, 72.8%, and 11.9% in spring, summer, autumn, and winter, respectively (P < 0.01) [Figure 2].
These cases occurred predominantly from October to the end of November of each year (69.1% of the total cases) [Figure 2]; this is the favored period for the ectoparasites, such as X. cheopis, of a vector where warm and humid climates prevail for most time of the year.[1,2,3,4,5,6] These findings strongly support the hypothesis that MT is a household infection due to its intimate association with commensal rats and their fleas and ectoparasites. Nearly all human cases have occurred indoors where commensal rats have been present.[1,2,3,4]
Furthermore, none of recent studies have thoroughly evaluated the reasons for the outbreaks of MT in relation to the inhabitants. Possible related factors include improvements in the standard living and housing in both rural and urban areas, ecological changes in rodent populations, and other nature-related factors.[1,2,3,4,5,9,10,12]
Consequently, counteractive measures against a possible increase in the number of MT cases in the future should be prioritized. Since commensal rats and their fleas are the key factors in the life cycle of MT, control measures against rats and their ectoparasites could markedly reduce the transmission of this infection to humans.[1,2,3,4]
Finally, the incidence of MT has significantly increased over the last decade in Korea. MT is one of the most widely speared arthropod-borne infections endemic in many coastal areas and ports throughout the world. Despite the widespread endemicity of MT, the focal transmission of the disease allows for highly targeted prevention in high-risk areas.[1,6,9,10,11]
CONCLUSION
The rapid reemergence of MT outbreaks can be minimized through health education; furthermore, well-informed recommendation for control measures against rats and their ectoparasites could considerably reduce the transmission of this infection to humans in high-risk areas. Therefore, this study provides a quantitative analysis of MT surveillance in Korea and contributes to better planning of future control strategies. We hope that this information will be a useful reference in further studies of MT in the public health service sector.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
This work was supported by Korea Institute of Planning and Evaluation for Technology in Food, Agriculture, Forest, and Fisheries (IPET) through Animal Disease Management Technology Development Program funded by Ministry of Agriculture, Food, and Rural Affairs (MAFRA), No. 316045-3.
REFERENCES
- 1.Azad AF. Epidemiology of murine typhus. Annu Rev Entomol. 1990;35:553–69. doi: 10.1146/annurev.en.35.010190.003005. [DOI] [PubMed] [Google Scholar]
- 2.Sakaguchi S, Sato I, Muguruma H, Kawano H, Kusuhara Y, Yano S, et al. Reemerging murine typhus, Japan. Emerg Infect Dis. 2004;10:964–5. doi: 10.3201/eid1005.030697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Adjemian J, Parks S, McElroy K, Campbell J, Eremeeva ME, Nicholson WL, et al. Murine typhus in Austin, Texas, USA, 2008. Emerg Infect Dis. 2010;16:412–7. doi: 10.3201/eid1603.091028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kim HC, Yang YC, Chong ST, Ko SJ, Lee SE, Klein TA, et al. Detection of Rickettsia typhi and seasonal prevalence of fleas collected from small mammals in the republic of Korea. J Wildl Dis. 2010;46:165–72. doi: 10.7589/0090-3558-46.1.165. [DOI] [PubMed] [Google Scholar]
- 5.Farhang-Azad A, Traub R, Baqar S. Transovarial transmission of murine typhus rickettsiae in Xenopsylla cheopis fleas. Science. 1985;227:543–5. doi: 10.1126/science.3966162. [DOI] [PubMed] [Google Scholar]
- 6.Azad AF, Radulovic S, Higgins JA, Noden BH, Troyer JM. Flea-borne rickettsioses: Ecologic considerations. Emerg Infect Dis. 1997;3:319–27. doi: 10.3201/eid0303.970308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Woo JH, Cho JY, Kim YS, Choi DH, Lee NM, Choe KW, et al. A case of laboratory-acquired murine typhus. Korean J Intern Med. 1990;5:118–22. doi: 10.3904/kjim.1990.5.2.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chun CH, Chung HY. Three cases of confirmed murine typhus. Korean J Intern Med. 1959;2:87–90. [Google Scholar]
- 9.Murine Typhus Cases: Web Statistical System of National Notifiable Disease Surveillance System. Republic of Korea: Korea Center for Disease Control and Prevention; 2006-2015. [Last accessed on 2016 Oct 12]. Available from: http://www.cdc.go.kr/
- 10.Korea Center for Disease Control and Prevention. Infectious Diseases Surveillance Yearbook. Republic of Korea: The Ministry of Health and Welfare. Korea Center for Disease Control and Prevention. 2012:97–338. [Google Scholar]
- 11.Bang HA, Lee MJ, Lee WC. Comparative research on epidemiological aspects of tsutsugamushi disease (scrub typhus) between Korea and Japan. Jpn J Infect Dis. 2008;61:148–50. [PubMed] [Google Scholar]
- 12.Lee HW. Hemorrhagic fever with renal syndrome in Korea. Rev Infect Dis. 1989;11(Suppl 4):S864–76. [PubMed] [Google Scholar]