

Abstract
This study examined changes in speech motor control across a movement transition between sounds within a motor learning task in children with apraxia of speech (CAS) and typical development (TD). It was investigated whether oral articulator movement was refined with practice and whether practice gains generalized to words not included in the practice session. A total of 16 children (ages 5–6) with CAS (n = 8) and TD (n = 8) participated in this study. Novel and real word tokens were produced at three time points. Kinematic data was collected using facial motion tracking at each time point. Children completed a practice session following baseline data collection session that integrated motor learning principles. Three tokens were included in the practice session and the remaining stimuli assessed carryover of practice gains. Kinematic data was then collected immediately following practice and three days later. Kinematic analyses were conducted on the movement gesture for the first syllable of each word. Narrow transcription analyses examined speech production accuracy. Children in the CAS group displayed increased consonant and vowel accuracy only for the practiced tokens. Adjustments to spatial control and movement variability were observed in the CAS group, though only for practiced words. Children in the TD group altered spatial and temporal domains of movement and variability across both practiced and non-practiced tokens. Interestingly, the CAS group displayed a pattern of increased displacement along with decreased variability, which was not observed in the TD group. The degree to which these findings reflect facilitative or maladaptive changes are discussed. Results are also interpreted in relation to vowel properties, novel/real word status, and variable practice of novel and real words.
Keywords: Movement transitions, childhood apraxia of speech, speech motor learning
Researchers and clinicians have had a longstanding interest in determining the degree to which speech motor patterns change with practice in children diagnosed with childhood apraxia of speech (CAS), an impairment characterized by motor planning and/or programming deficits (ASHA, 2007; Grigos & Kolenda, 2010; Grigos, Moss & Lu, 2015; Moss & Grigos, 2012; Nijland, Maassen, & Van Der Meulen, 2003a; Nijland et al., 2003b; Terband, Maassen, Van Lieshout, & Nijland, 2011). While children with CAS may learn to produce speech sounds accurately during treatment, the underlying motor skill may continue to be deficient, hindering generalization. The extent to which speech motor skill must be refined with practice for children with CAS to acquire, generalize and retain speech skills is not known. The current work aims to explore this problem by quantifying changes in speech motor control for a movement transition across a practice period and then exploring generalization to unpracticed speech targets. A better understanding of speech motor changes associated with movement transitions that are seen as a result of practice can inform improved therapeutic strategies for facilitating and retaining accurate movement sequences in children with CAS.
Movement transitions
Movement transitions can be defined as the change in articulatory configuration between segments and/or syllables. The spatial and temporal parameters of such transitions are described as being impaired in children with CAS (e.g., Grigos et al., 2015; Nijland et al., 2003a, 2003b). There is little empirical evidence, however, that quantifies how movement transitions are deficient in this population. Difficulty moving between articulatory positions for segments and syllables may contribute to a number of the characteristics commonly associated with CAS, such as impaired coarticulatory transitions, inconsistent errors, prosodic errors, vowel errors, timing errors, articulatory groping and phoneme distortions (see ASHA, 2007; Davis, et al., 1998; Shriberg, Aram, & Kwiatkowski, 1997a; 1997b; 1997c; Velleman & Strand, 1994). Impaired transitions between words may also underlie inappropriate pausing, which has recently been identified as a diagnostic marker for CAS (_Shriberg et al., 2017a, b, c, d). Further, impaired movement transitions may hinder treatment progress as children with CAS often have difficulty generalizing newly acquired sounds to novel speaking contexts (Ballard et al., 2010; Davis et al., 1998; Forrest, 2003; Grigos & Kolenda, 2010; Maas, Butalla, and Farinella, 2012; Strand & Debertine, 2000; Strand, Stoeckel, & Baas, 2006). This is evident when, for instance, segments produced accurately within treatment stimuli may not remain accurate when combined with other segments in different words. Studying articulatory control associated with movement transitions, even within accurate productions, provides an opportunity to quantify spatial and temporal patterns of movement that are believed to underlie speech production difficulties in children with CAS.
The movement involved in a consonant-vowel (CV) sequence is interesting to explore in children with CAS. Moving from a more distinct (most consonants) to a less distinct (vowel) articulatory contact may pose a motoric challenge for children with CAS. Therefore, studying this sequence may offer insight into the motor control underlying vowel errors, which are prevalent in this population. Children with typical speech and language development children demonstrate accurate vowel production (with the exception of rhotics) by three years of age (Davis & MacNeilage, 1990; Pollock, 2002). In contrast, children with CAS have been reported to have reduced vowel inventories (Davis et al., 1998) and produce a range of vowel errors including diphthong reduction (Pollock & Hall, 1991; Davis et al., 1998), reduced distinction between tense and lax vowels (Davis, Jacks & Marquardt, 2005; Pollock & Hall, 1991), rhotic errors (Davis et al., 1998; 2005; Pollock & Hall, 1991) and vowel substitutions that do not follow a systematic pattern (Davis et al., 2005; Pollock & Hall, 1991). One of the challenges clinicians face when targeting vowel production is that children with CAS may produce vowels accurately in one context but struggle to achieve that same production across varied contexts. This claim is supported by evidence that children with CAS who have complete vowel inventories continue to produce a range of vowel errors over time (Davis et al., 2005). Thus, motor planning and/or programming deficits that are associated with CAS may impact the movement transition into vowels. By studying the movement from consonant into vowel, we aim to characterize the speech motor skill that underlies vowel production that could be contributing to the vowel errors described above in CAS.
Articulatory Control
Typically developing children refine their speech motor skills throughout childhood and adolescence which includes changes in articulator movement duration, displacement, velocity and variability (e.g., Goffman & Smith, 1999; Green, Moore, Higashikawa, & Steeve, 2000; Grigos & Patel, 2007; Grigos, Saxman, & Gordon, 2005; Grigos, 2009; Nip, Green & Marx, 2009; Sharkey & Folkins, 1985; Smith & Gartenberg, 1984; Smith & Goffman, 1998; Walsh & Smith, 2002). They have also been shown to display decreases in movement duration and variability across the practice of nonwords (Heisler, Goffman, & Younger, 2010; Sasisekaran, Smith, Sadagopan, & Weber-Fox, 2010; Walsh, Smith, & Weber-Fox, 2006).
Children with CAS have been reported to display longer movement duration (Case & Grigos, 2016; Grigos et al., 2015; Moss & Grigos, 2012), larger displacement (Terband et al., 2011) and more variable movements (Grigos et al., 2015; Moss & Grigos, 2012) as compared to typically developing children. There is also evidence that children with CAS produce more variable articulator movements than children with other speech sound disorders (Grigos et al., 2015; Moss & Grigos, 2012). Two studies have built upon past research to examine the impact of practice on sound production and articulatory control in children with CAS (Case & Grigos, 2016; Vuolo & Goffman, 2016). Vuolo and Goffman (2016) examined changes in speech production and movement variability in nine children (5–6 years of age), two of which were diagnosed with CAS, within the context of an imitation and retrieval task. Children tended to demonstrate an increase in spatial and temporal variability across a period of five practice periods. In Case and Grigos (2016), children with CAS (n=8, 5–6 years of age) displayed improved consonant accuracy immediately following practice and retained these gains following a three-day interval. The study of movement kinematics at the whole word level revealed longer word duration in children with CAS than in their typically developing peers. Movement duration did not change with practice and variability remained high for accurate productions. These results suggested that high movement variability and longer movement duration (even in the context of accurate productions) may contribute to poor generalization of skills to varied speaking contexts in CAS. The present work is a follow-up study to explore a finer level of articulatory control captured by the transition between segments that can be masked by whole word analyses, in children with CAS and those with typical speech and language development (TD).
One approach to quantifying articulatory control associated with the transition between segments is to measure the transition from oral closing to opening. Movement into oral opening may be particularly challenging for children with speech motor deficits as vowels do not have a specific articulatory contact and require less precision than most consonants. To our knowledge, no published research has quantified the movement transition from oral closing to opening in children with CAS or TD or has explored how such transitions may change over a practice period.
Motor Schema Theory
Motor schema theory (Schmidt, 1975; 2003) provides an interesting framework from which speech motor skill learning can be explored in children with CAS. The concept of the generalized motor program (GMP), which specifies that movements are pre-programmed, is at the core of motor schema theory (Schmidt, 1975). The GMP is the abstract plan that defines the shape of the action. With respect to motor learning, an individual acquires the GMP for a movement through practice and learns the schemata, or rules, necessary to refine parameters to tailor the movement to the environment, which occurs through additional practice and experience (Schmidt, 2003). This has been described as a “reconstruction process” in which practice and feedback conditions can influence the way movements are refined (Schmidt, 2003, p.371). In contrast to limb movement associated with motor skill learning (such as in a golf swing), elements of GMPs and parameters that are involved in speech production are less clearly defined. The GMP may involve the motor commands associated with syllable production where parameters, such as articulator movement timing and amplitude, can be applied to the GMP to appropriately scale the movement to the environment (Maas et al., 2008). The speaker can then compare somatosensory feedback to the schemata and the movement outcome (Schmidt, 2003). Parameters would continue to be adjusted through practice if the desired outcome were not achieved. In speech motor disorders, such as CAS, there are many potential areas of breakdown in this process (see Maas et al, 2008 for a review). The focus of the current work is to study the articulatory adjustments that may be seen with practice in children with CAS and TD, which could shed light on the manner in which parameters are refined in the motor learning process.
A variety of factors are central to the discussion of practice effects in CAS, including the amount of practice, structure of practice sessions, complexity of practice stimuli, and type/frequency of feedback. Practice conditions have a significant impact on motor learning outcomes (Edeal & Gildersleeve-Neumann, 2011; Knock, Ballard, Robin, Schmidt, 2000). Blocked practice (i.e. trials are grouped) is viewed as more effective in the initial learning stage for a novel skill than random practice (i.e. trials presented in a random order) (Knock et al., 2000). The latter may result in greater generalization (Hall & Magill, 1995) as it prevents individuals from using the same pattern across tokens and forces them to reconstruct the actions on each production attempt (Schmidt, 2003).
Type and amount of feedback is another key topic addressed in motor learning theories (Schmidt, 2003). Knowledge of Results (KR) includes feedback regarding the accuracy of production (e.g. “correct”), whereas Knowledge of Performance (KP) offers information regarding mechanics of how a sound is produced (e.g., “close the lips more tightly”). KP feedback is believed to be most effective in novel skill learning, as it provides explicit information regarding the targeted movement pattern and is often used when establishing production of a stimulus (Schmidt & Lee, 1988). KR feedback can facilitate long-term retention of practice gains, particularly when provided on a reduced schedule (Maas et al., 2008; Schmidt, 2003). The current study involves practice sessions that were designed to reflect this past work on practice and feedback conditions by using blocked practice followed by randomized practice to promote generalization and by integrating a gradually reduced KR feedback schedule.
Purpose
There is a strong need to quantify how skill acquisition is refined across a practice period in children with CAS. The present study aims to address this need by measuring changes in speech production and articulatory control across the transition from consonant to vowel production within the context of a motor learning task. We also examine changes in speech performance with practice in a group of children with typical development, as speech motor control is still developing and movement parameters in this group could be refined with practice. This work integrates perceptual (i.e., narrow transcription and error analysis) and kinematic (i.e., facial tracking) methods to study speech sound production across a movement transition from oral closing to oral opening over a practice period in children with CAS. In the CAS group, we predict that the movement from consonant to vowel will be refined with practice and characterized by decreased movement duration, displacement and variability over time. These kinematic parameters are selected as prior research involving children with CAS has shown that they are sensitive to change (Grigos et al., 2015; Terband et al., 2011; Vuolo & Goffman, 2016). Further, we hypothesize that changes seen in practiced tokens will not generalize to unpracticed tokens given the speech motor deficits associated with CAS. In the TD group, we predict that the movement transition will not change over the practice period. This prediction is based upon our prior research (Case & Grigos, 2016) that did not reveal changes in articulatory control in this group (through whole word analyses), which may have stemmed from the stimuli not being complex enough to challenge the unimpaired speaker. A greater understanding of how practice impacts movement transitions in children with CAS can inform improved therapeutic strategies for facilitating and retaining accurate sound production in this population, which can have a significant impact on the effectiveness and efficiency of therapeutic intervention.
Method
Participants
A total of sixteen children participated in this study (12 male, 4 female). Children were between five and six years of age and divided into the TD (n=8) and CAS (n=8) groups. Mean age was 5;8 years (SD = 8 months) for the TD group and 5;8 years (SD = 5 months) for the CAS group. Table 1 shows characteristics by individual participant. A subset of the transcription and kinematic data for these children were reported in Case & Grigos (2016) which centered on whole-word analyses. All children were monolingual speakers of English who lived in the United States. Children in both the TD and CAS groups demonstrated age-appropriate nonverbal cognition on the Columbia Mental Maturity Scales (CMMS; Burgmeister, Blum, & Lorge, 1972) and appropriate expressive and receptive language skills according to the Test of Early Language Development, 3rd edition (TELD-3; Hresko, Reid, & Hammill, 2007). All participants demonstrated normal structure of the oral-peripheral mechanism and passed a hearing screening at 20dB SPL at 500, 1000, 2000 and 4000Hz.
Table 1:
Participant Characteristics
| TELD-3 | CMMS | VMPAC | GFTA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| REC | EXP | ADS | GMC | FOMC | SEQ | Conn Speech | Speech Char | %ile | |||||||
| Participant | Age | Q | Q | % | rating | % | rating | % | rating | % | rating | % | rating | ||
| CAS1 | 5;4 | 110 | 88 | 120 | 85 | SEV | 93 | WNL | 87 | WNL | 87 | MOD | 71 | SEV | 13 |
| CAS2 | 5;0 | 110 | 102 | 93 | 95 | WNL | 83 | MOD | 74 | WNL | 87 | MOD | 71 | SEV | 27 |
| CAS3 | 6;9 | 97 | 94 | 89 | 90 | SEV | 70.15 | SEV | 73.9 | MILD | 80 | SEV | 57.14 | SEV | <1 |
| CAS4 | 5;11 | 110 | 94 | 106 | 90 | SEV | 73 | SEV | 50 | SEV | 71 | SEV | 71 | SEV | <1 |
| CAS5 | 6;4 | 89 | 88 | 89 | 75 | SEV | 72.01 | SEV | 69.57 | MOD | 88.89 | MILD | 71.43 | SEV | 24 |
| CAS6 | 5;11 | 118 | 118 | 116 | 100 | WNL | 91 | WNL | 84.8 | WNL | 86.7 | MILD | 71.4 | SEV | 9 |
| CAS7 | 5;8 | 118 | 100 | 113 | 95 | MOD | 75 | SEV | 69.5 | MILD | 87 | MOD | 86 | MOD | 5 |
| CAS8 | 5;7 | 118 | 82 | 109 | 100 | WNL | 85.1 | MOD | 78.3 | WNL | 57.8 | SEV | 57.1 | SEV | <1 |
| mean | 5;8 years | 108.75 | 96.38 | 104.38 | 91.25 | 80.29 | 73.37 | 80.6 | 69.61 | 15.6 | |||||
| SD | 5.28 months | 10.62 | 11.66 | 12.48 | 8.35 | 8.93 | 11.44 | 10.91 | 9.23 | 9.53 | |||||
| TD1 | 5;0 | 109 | 94 | 103 | 100 | WNL | 97 | WNL | 87 | WNL | 100 | WNL | 100 | WNL | 68 |
| TD2 | 6;10 | 105 | 118 | 96 | 100 | WNL | 98.5 | WNL | 97.8 | WNL | 100 | WNL | 100 | WNL | 56 |
| TD3 | 6;0 | 121 | 115 | 111 | 100 | WNL | 99.2 | WNL | 91.3 | WNL | 100 | WNL | 100 | WNL | >75 |
| TD4 | 5;4 | 130 | 115 | 128 | 100 | WNL | 100 | WNL | 100 | WNL | 100 | WNL | 86 | MOD | >83 |
| TD5 | 5;7 | 121 | 100 | 133 | 100 | WNL | 99.2 | WNL | 91.3 | WNL | 100 | WNL | 100 | WNL | 78 |
| TD6 | 5;3 | 124 | 112 | 144 | 100 | WNL | 96.6 | WNL | 84.8 | WNL | 93.3 | WNL | 100 | WNL | 31 |
| TD7 | 6;10 | 121 | 112 | 150+ | 100 | WNL | 99.63 | WNL | 95.65 | WNL | 100 | WNL | 100 | WNL | 56 |
| TD8 | 5;7 | 118 | 115 | 142 | 100 | WNL | 100 | WNL | 80.4 | WNL | 100 | WNL | 100 | WNL | 76 |
| mean | 5;8 years | 118.63 | 110.5 | 122.43 | 100 | 98.77 | 91.02 | 99.29 | 98.38 | 60.83 | |||||
| SD | 8.4 months | 8.05 | 8.78 | 19.14 | 0 | 1.31 | 6.73 | 2.44 | 5.01 | 17.39 | |||||
TELD-3: Test of Early Language Development - 3rd Edition (REC = Receptive Language; EXP = Expressive Language; Q = Quotient); CMMS: Columbia Mental Maturi Scales (ADS = Age Deviation Score); VMPAC: Verbal Motor Production Assessment for Children (GMC = Gross Motor Control, FOMC = Focal Oromotor Control, SEC Sequencing; Conn Speech = Connected Speech; Speech Char = Speech Characteristics); GFTA: Goldman Fristoe Test of Articulation
A comprehensive assessment of speech production skills was conducted on all children across three speaking contexts: single word production [Goldman Fristoe Test of Articulation-2 (GFTA-2, Goldman & Fristoe, 2000)], connected speech (100-word narrative of a wordless picture book, Pancakes for Breakfast by Tomie DePaola), syllable & single word sequences [Verbal Motor Production Assessment for Children (VMPAC; Hayden & Square, 1999)]. Phonetic inventory, percent word consistency (PWC; Case, Moss, & Grigos, 2012), percent consonant correct (PCC; Shriberg, Austin, Lewis, McSweeney, & Wilson, 1997), percent vowel correct (PVC; Shriberg et al., 1997), error patterns (additions, omissions, distortions, substitutions), and prosody were examined across each context. Movement transitioning in speech and non-speech sequences was also examined.
Children in the TD group displayed age-appropriate speech production skills across all examined contexts. Differential diagnosis (ASHA, 2007; Davis et al., 1998) was used to identify children with CAS and rule out children who presented with articulation/phonological disorders, dysarthria, or fluency disorders. The diagnostic framework, including operational definitions and criteria, is provided in Appendix A. The diagnosis of CAS was made independently by both authors who are ASHA certified speech-language pathologists. In connected speech, decreased consonant (PCC = 69.69%) and vowel accuracy (PVC = 86.15%) were observed, in addition to poor speech consistency (PWC = 68.43%). Children with CAS displayed the three consensus features identified by ASHA (2007) in more than one speaking context: inconsistent errors, inappropriate prosody, and disrupted coarticulatory transitions. At least four additional characteristics associated with CAS were also identified in more than one speaking context (see ASHA, 2007; Davis et al., 1998; Forrest, 2003; Hall et al., 1993; Odell & Shriberg, 2001; Shriberg et al., 1997a; 1997b; 1997c; Shriberg et al., 2009; Shriberg et al., 2012; Velleman & Strand, 1994): vowel errors, timing errors related to voicing and nasality, speech sound distortions, articulatory groping, increased errors with increased utterance length and complexity, atypical errors, and a reduced phonetic inventory (see Table 2 for individual characteristics of CAS). Consistent with our past work (Case & Grigos, 2016; Grigos et al., 2015), features were determined to be present when they were seen at least three times in at least two different speaking contexts with the exception of phonetic inventory which could not be judged in this manner. Three children were excluded from the study, as they did not meet the above criteria.
Table 2:
Diagnostic criteria met by children with CAS
| CAS1 | CAS2 | CAS3 | CAS4 | CAS5 | CAS6 | CAS7 | CAS8 | |
|---|---|---|---|---|---|---|---|---|
| ASHA Technical Paper: | ||||||||
| Impaired co-articulatory transitions | X | X | X | X | X | X | X | X |
| Inappropriate Prosody | X | X | X | X | X | X | X | X |
| Inconsistent Errors | X | X | X | X | X | X | X | X |
| Additional Features: | ||||||||
| Vowel Errors | X | X | X | X | X | X | X | X |
| Timing Errors | X | X | X | X | X | X | X | X |
| Speech Sound Distortions | X | X | X | X | X | X | X | X |
| Articulatory Groping | X | X | X | X | X | |||
| Errors increase with length and complexity | X | X | X | X | X | X | X | X |
| Atypical errors | X | X | X | X | X | X | X | X |
| Reduced Phonetic Inventory | X | X | X | X | X | X | ||
Procedure
Instruments.
Lip and jaw movement was tracked in three dimensions using a facial capture system (Vicon 460; Vicon Motion Systems, 2001). Twelve 3 mm reflective markers were placed on the lips, jaw, nasion and forehead (Figure 1). Movement of the reflective markers was tracked at a sampling rate of 120 frames per second. A Sony digital camera (Model DSC-T1) was used to collect both audio and video recordings. Custom MATLAB algorithms were used to analyze kinematic data (Mathworks, 2013). Data collection was conducted in a sound attenuated audiometric booth in the Department of Communicative Sciences and Disorders at New York University.
Figure 1.

Twelve reflective markers placed on the lips, jaw, nose and forehead.
Stimuli.
Practiced stimuli (PR) consisted of two novel words, PR1 (badabap, /ˈba.ɾə. bap/) and PR2 (madeepoom, /ˈma.ɾi. pum/), and one real word, PR3 (bubblegum, /ˈbʌ.bəl. gʌm/). The non-practiced stimuli (NPR) consisted of two real words, NPR1 (buttercup, /ˈbʌ.ɾɚ. kʌp/), and NPR2 (bunnyhop, /ˈbʌ.ni. hap/). Novel word stimuli were used to examine how speech performance would change with practice for words with no pre-existing linguistic representation, or habituated error patterns. The term “novel word” is used in the current study (as opposed to nonword), as the stimuli were assigned a lexical referent. This approach is well established as a means to directly examine motor planning skills for speakers with motor planning disorders (Ballard et al., 2010; Case & Grigos, 2016; Murray, McCabe, & Ballard, 2015; Schneider & Frens, 2005; Van der Merwe, 2011). Real word stimuli were incorporated to see if practice that involved novel word tokens would carryover to unpracticed real words, as would be the aim for therapeutic intervention. We also wanted to examine whether changes observed in a practiced real word would generalize to non-practiced words. We chose not to include novel words into the non-practiced set of stimuli as we anticipated it would have been too challenging for children with CAS to produce these tokens in the absence of additional practice and feedback.
There were several considerations when designing these stimuli. Real word and novel word stimuli all contained early developing phonemes with the exception of the rhotic vowel in PR3 (i.e., buttercup). All tokens began and ended with a bilabial consonant to facilitate movement tracking across each word. Direction of articulator movement across vowel sequences was also considered when selecting stimuli. Each syllable of PR1 (badabap), PR3 (bubblegum), and NPR1 (buttercup) contained similar vowels that were all within a vertical plane of movement (/a, ʌ, ə, a/). PR2 (madeepoom) and NPR2 (bunnyhop) contained three differing vowels (/a, i, u/) and were designed to introduce a greater level of complexity when transitioning between syllables.
Design.
Children were seen over three separate days. On Day 1, the diagnostic testing battery was administered to determine group membership. On Day 2, baseline data collection (T1) occurred, followed by a structured practice session, and post-practice data collection (T2). On Day 3, a final data collection session (T3) was conducted to examine retention of practice effects following a 3-day interval. In each data collection session, production of all 5 words was elicited. The structured practice session, however, only included 3 of the 5 words (PR1, PR2, PR3). The non-practiced words (NPR1, NPR2) were not included in the practice session and served as control words to examine carryover of practice effects to a non-practiced target.
Day 1.
All children received a comprehensive assessment to examine oromotor structure and function, articulation skills, speech/non-speech movement sequencing skills, prosody, expressive-receptive language skills, and nonverbal cognition.
Day 2.
Children were first familiarized to the experimental stimuli. They were shown puppets which represented the novel word stimuli, PR1 (Badabap), and PR2 (Madeepoom) and pictures of real word stimuli, PR3 (Bubblegum), NPR1 (Buttercup), and NPR2 (Bunnyhop). The examiner produced five repetitions of each word within a narrative and asked the children to remain quiet and listen carefully to the examiner. This procedure was used to not only familiarize children to the tokens, but also to ensure that they did not produce novel word tokens until data collection began.
Baseline data collection (T1) was initiated following familiarization. Productions of stimuli were elicited in a randomized order in the context of a story retell task. The examiner created stories using the stimuli and children were asked to answer questions or complete sentences according to these stories (e.g., Badabap was walking through a field and came across a beautiful buttercup. Who found a buttercup? What did Badabap find?). Tokens were repeated throughout elicitation to facilitate recall of target words and reduce the cognitive demand of learning novel words. Children did not receive feedback regarding accuracy during this portion.
Following baseline data collection, children were engaged in a structured practice session that took place in a clinic treatment room and lasted approximately 20 minutes. During this session, children practiced the novel word tokens (PR1 & PR2) and one real word token (PR3). Practice incorporated principles of motor learning to facilitate learning of selected tokens. Each token was produced 30 times during this session, resulting in a total of 90 productions within practice.
The practice session was divided into three blocks (10 trials each) where each token was practiced 30 times, for a total of 90 productions (3 blocks X 10 trials each X 3 words). Targets were elicited within a structured, play-based session. In the first block, tokens were practiced in a blocked order. Knowledge of results (KR) and knowledge of performance (KP) feedback was provided on 100% of productions to support initial learning and accuracy of productions. KR feedback indicated whether or not each production was accurate (e.g., “That was right,” “Almost. Let’s try again next time”). KP feedback provided information regarding how the child’s performance differed from the target, in addition to verbal, visual and tactile cues to achieve accurate production (e.g., “Your lips are not closing at the end of the word. Watch my lips close. Be sure to close your lips too”). This included information about the movement associated with sound production, as well as segmental and prosodic accuracy. In the second block of the practice session, tokens were practiced in a randomized order and KP and KR feedback was provided on 50% of productions. In the final block of the practice session, tokens continued to be practiced in a randomized order with KP and KR feedback on 20% of tokens. Throughout practice, the examiner followed a written schedule to control for the order in which tokens were practiced and the feedback schedule for each practice block.
A second data collection session (T2) was conducted immediately following the practice session. During this session, participants produced both the practiced and non-practiced words in a randomized order. The aim of this session was to examine how articulator movement and speech production accuracy differed for those tokens included in a practice session where children received feedback and additional practice as compared to the non-practiced tokens. Data were collected using the same procedure described during baseline data collection.
Day 3.
Participants returned three days later for the final data collection session (T3) to examine whether practice effects were maintained following a brief interval. A three-day interval between sessions was selected as it represents a typical amount of time between treatment sessions. Prior to initiating data collection, children were refamiliarized to the stimuli following the same procedure described above. Production of all practiced and non-practiced tokens was then elicited using a story-telling format, also described above.
Analyses
Transcription analysis.
Two levels of transcription analyses were conducted using narrow transcription. First, production accuracy was calculated for the initial consonant (C1) and initial vowel (V1) for the first syllable of each token given our interest in the coarticulatory transition for this syllable. Second, consonant and vowel accuracy was calculated across the word as an overall index of production accuracy using Percent Consonant Correct (PCC; Shriberg et al., 1997) and Percent Vowel Correct (PVC; Shriberg et al., 1997), respectively. A production was judged to be accurate if it did not contain distortions, omissions, substitutions, or additions. Two ASHA certified speech-language pathologists performed reliability testing on 10% of productions. Across the sample, an inter-rater reliability agreement of 93.75% was achieved based on the novel word tokens. A third listener was used to resolve disagreements.
Kinematic analysis.
Kinematic analyses were performed on the sequence from oral closing to opening associated with the first syllable of each token. The nasion and forehead markers were used to determine the orientation and to account for vertical head movement and rotation. Movement of the upper lip and jaw were calculated by subtracting their y coordinates from stationary points on the forehead (i.e. forehead - upper lip; forehead - jaw). Movement of the lower lip was calculated by subtracting lower lip from jaw (i.e. lower lip – jaw). Lip aperture was calculated as the vertical distance between the upper and lower lips.
The acoustic signal for each token was compared with each kinematic trajectory. Movement onset and offset was determined using the jaw displacement trajectory. Onset was taken as the point ten frames (0.083s) prior to initial peak closing displacement for the first consonant (C1) and offset was measured as the point ten frames following the peak opening displacement (0.083s) associated with the first vowel (V1). Analyses focused on single point measures (Figure 2). Jaw movement duration was measured as the time between the point of oral closure to the point of oral opening. Displacement was measured to examine the excursion of movement from oral closing to opening. Changes in displacement were calculated as the peak to trough (jaw) or trough to peak (lip aperture) displacement. To examine variability of articulator movement across each time period, the coefficient of variation (standard deviation/mean) was calculated for single point measures of jaw duration (duration COV), jaw displacement (displacement COV), and lip aperture (lip aperture COV).
Figure 2.
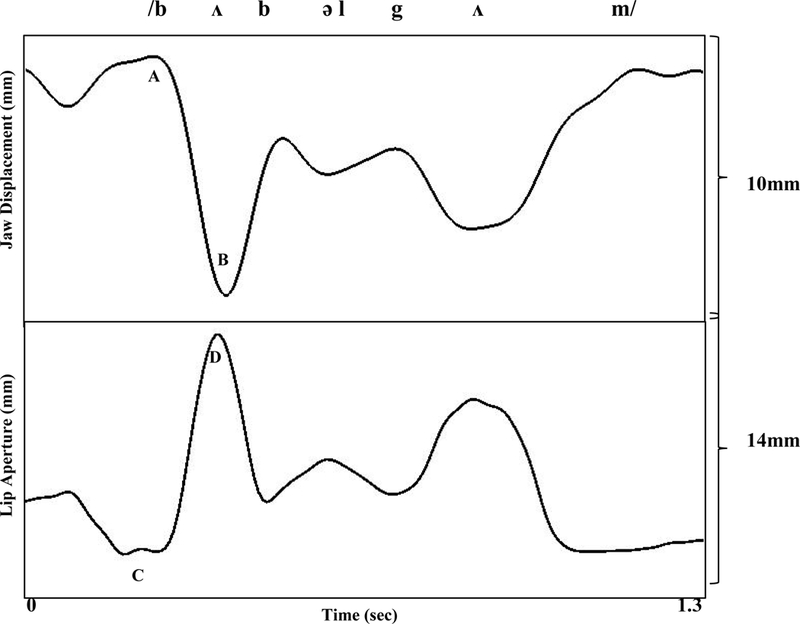
Kinematic traces of jaw displacement and lip aperture corresponding to the utterance “bubblegum.” Displacement measures were based on maximum displacement points. Displacement into oral opening for the first vowel was measured from the point of maximum closing displacement for the initial consonant (Point A) to the point of maximum opening displacement for the following vowel (Point B). The lip aperture trajectory reflects the distance between the upper and lower lips. Lip aperture into oral opening was measured from lip closing (Point C) to lip opening (Point D).
Tokens were included in analyses if production of the first syllable was accurate. When there were errors in other parts of the token, these productions were included if the syllable number was maintained (i.e., 3 syllables) and the consonant following the first vowel was accurate. Analyses on accurate productions is common in studies of articulator movement to ensure that kinematic differences are due to changes in speech motor control that were independent from articulation errors (e.g., Green et al., 2000, 2002; Grigos et al., 2015; Moss & Grigos, 2012; Sasisekaran et al., 2010).
Statistical Analysis.
Linear mixed-effects modeling was used for data analysis due to the small sample size and high degree of variability within participants. The lme4 and lmerTest packages (Baayen, Davidson, & Bates, 2008; Bates, Maechler, Bolker, & Walker, 2010; Kuznetsova, Brockhoff, & Christensen, 2013) in R (http://www.r-project.org) were used to perform statistical analyses. Our prior research (Case & Grigos, 2016) showed that the TD children were highly accurate at baseline and displayed no changes in consonant and vowel accuracy over time. In contrast, the children with CAS were significantly less accurate. Therefore, in this follow up study, the CAS and TD groups were analyzed separately to capture the trajectory of change for each group of children. Within each group, two different sets of analyses were performed for the practiced (PR1, PR2, PR3) and non-practiced words (NPR1, NPR2). The following dependent measures were analyzed: (1) PCC; (2) PVC; (3) C1 accuracy; (4) V1 accuracy; (5) jaw duration; (6) jaw duration COV; (7) jaw displacement; (8) jaw displacement COV; (9) lip aperture; (10) lip aperture displacement COV. When visual inspection indicated data to be skewed, a logit transformation (PCC, PVC, C1, V1) or log transformation (duration, displacement) was performed to decrease skewness and create more normally distributed data. For proportionate data (PCC, PVC, C1, V1), transformation of data was also required to create a continuous variable, as proportional values are bound by zero and one, for the purpose of linear regression analyses.
Time was entered as a fixed effect with three levels for baseline (T1), short-term acquisition (T2), and long-term retention (T3). Random effects of participant and word were also included to account for token- and child-specific variation. For each model, log likelihood comparisons were then performed to determine which random effects significantly contributed to the model. Linear mixed-effects regressions were then conducted using random effects that significantly contributed to the final model for each dependent variable. Results were interpreted as statistically significant when the p-value was less than p = 0.05. If multiple pairwise comparisons were performed following a significant interaction, Bonferroni adjustments were made to the p-value to control for type I error.
Results
Fifteen productions of practiced and non-practiced tokens were elicited at each of the three time periods. Transcription analyses were conducted on the first 13 tokens (correct and incorrect) to ensure an equal number of productions per child. A total of 3120 tokens were included in the transcription analyses (16 participants X 5 tokens X 13 productions X 3 time periods [T1, T2, T3]). Kinematic analyses were completed using tokens in which all markers were visible for analyses and the first syllable was accurately produced. Participants varied in the number of productions that could be included in the analysis. To account for this, each child was required to achieve a minimum of three correct productions of a given token for their data from that token to be included in the kinematic analysis. For those children who produced all tokens accurately, a maximum of eight correct productions were included. The percentage of tokens that were not included in the analyses due to error (i.e. errors in the first syllable, reduced syllable number, inaccurate consonant following the first syllable) was 7% for the CAS group and 0.7% for the TD group. This resulted in a total of 862 tokens for the kinematic analyses in the CAS group (530 practiced (T1: 177, T2: 174, T3: 179) and 332 non-practiced (T1: 109, T2: 111, T3: 112)). There were a total of 952 analyzable tokens in the TD group (568 practiced (T1: 186; T2: 191; T3: 191) and 384 non-practiced (K1: 128, K2: 128, K3: 128)). If a participant did not meet this minimum requirement, their data for that token was not included in the analysis at any of the time points (i.e., PR3: S5; PR4: S5, S6). Transcription and kinematic results are described below.
PCC
There were no significant effects of time on consonant accuracy in practiced tokens in the TD group, F(2, 60) = 0.08, p = 0.92. In the CAS group, mixed effects analyses revealed that time had a significant effect on consonant accuracy in practiced tokens, F(2, 60) = 16.21, p < 0.001 with a significant increase in PCC from T1 to T2 (B = 0.89, SE = 0.21, p < 0.001) and from T1 to T3 (B = 1.14, SE = 0.21, p < 0.001). Analyses showed no significant change in PCC from T2 to T3 (B = 0.25, SE = 0.21, p = 0.25), indicating that accuracy levels were maintained following a 3-day interval (Table 3). Post-hoc analyses did not reveal significant differences for consonant accuracy between novel and real words, F(2, 59) = 1.21, p = 0.31. In the non-practiced tokens, there was no significant effect of time on PCC in the TD, F(2, 38)=1.14, p=0.33, or CAS group, F(2, 37)=2.31, p=0.11.
Table 3:
Mean (Standard Deviation) of Consonant Accuracy (PCC), Vowel Accuracy (PVC), Initial Consonant Accuracy (C1), and Initial Vowel Accuracy (V1) for children with CAS and TD at baseline (T1), immediately following practice (T2), and following a three-day interval (T3)
| TD | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| PCC | 96.89 (4.47) | 97.49 (2.42) | 97.29 (3.69) | 98.83 (2.15) | 99.63 (0.81) | 99.20 (1.25) |
| PVC | 97.08 (3.41) | 98.00 (2.89) | 96.96 (4.67) | 98.36 (2.72) | 99.22 (1.65) | 98.46 (3.71) |
| C1 | 96.79 (8.15) | 99.36 (2.17) | 99.04 (2.60) | 99.52 (1.92) | 100 (0) | 99.52 (1.92) |
| V1 | 98.72 (3.70) | 98.40 (3.19) | 97.44 (3.70) | 99.52 (1.92) | 100 (0) | 99.04 (3.85) |
| CAS | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| PCC | 74.48 (16.88) | 87.85 (10.75) | 89.60 (10.41) | 84.42 (13.85) | 88.56 (13.83) | 90.73 (11.32) |
| PVC | 78.62 (21.37) | 86.75 (12.82) | 86.11 (14.06) | 78.20 (22.96) | 80.77 (21.47) | 81.25 (23.38) |
| C1 | 92.95 (12.81) | 94.23 (11.84) | 97.76 (6.98) | 97.60 (3.68) | 99.52 (1.92) | 98.56 (3.10) |
| V1 | 83.65 (14.04) | 84.94 (25.71) | 90.06 (18.07) | 81.25 (28.78) | 83.65 (28.63) | 78.85 (32.94) |
PVC
There was no significant effect of time on vowel accuracy in the TD group for practiced tokens, F(2, 60), p = 0.50. In the CAS group, analyses revealed time to have a significant effect on vowel accuracy in practiced tokens, F(2, 60) = 6.43, p = 0.003. A significant increase in PVC was seen from T1 to T2 (B = 0.70, SE = 0.24, p = 0.005) and from T1 to T3 (B = 0.61, SE = 0.24, p = 0.014). No significant difference was observed from T2 to T3 (B = −0.09, SE = 0.21, p = 0.68) (Table 3). Post-hoc analyses revealed no significant change in vowel accuracy for novel versus real word tokens in the CAS group, F(2, 59) = 0.796, p = 0.46. For non-practiced tokens, there were no significant effects of time on vowel accuracy in either the TD, F(2, 37) = 0.60, p = 0.56, or CAS groups, F(2, 37) = 1.23, p = 0.30.
C1 Accuracy
Production accuracy was examined for the first consonant (C1) of each token. Mixed effects analyses revealed no significant change in C1 accuracy over time in practiced tokens for either the TD, F(2, 67) = 1.85, p = 0.17, or CAS group, F(2, 60) = 1.75, p = 0.18 (Table 3). For non-practiced tokens, analyses also revealed no significant effect of time on C1 accuracy for children with TD, F(2, 38) = 0.61, p = 0.55, or CAS, F(2, 37) = 1.69, p = 0.20.
V1 Accuracy
Accuracy of the initial vowel (V1) was examined across all three sessions. V1 accuracy did not change with time for the practiced tokens for either the TD, F(2, 60) = 1.43, p = 0.25, or CAS group, F(2, 60) = 2.45, p = 0.10. Similarly, there was no effect of time on V1 accuracy in non-practiced tokens for children with TD, F(2, 44) = 0.54, p = 0.59, or CAS, F(2, 37) = 0.27, p = 0.77 (Table 3).
Jaw Duration
Results of mixed effects analyses indicated no significant change in jaw opening duration over time for the practiced tokens in the TD, F(2, 558.21) = 0.37, p = 0.69, or CAS groups, F(2, 518.28) = 1.36, p = 0.26 (Table 4). For the non-practiced tokens, analyses revealed a significant change in jaw opening duration over time in the TD group, F(2, 374) = 4.25, p = 0.02. Jaw duration was significantly longer from T2 to T3, B = 0.06, SE = 0.05, p = 0.004. Analyses found no significant change in jaw duration from T1 to T2 (B = −0.08, SE = 0.05, p = 0.11) or from T1 to T3 (B = 0.06, SE = 0.05, p = 0.19). In contrast, for children with CAS, jaw opening duration was similar across each time period for the non-practiced tokens, F(2, 321.24) = 2.73, p = 0.07.
Table 4:
Mean (Standard Deviation) of opening jaw duration (seconds) and the variability of jaw duration (coefficient of variation) for children with CAS and TD at baseline (T1), immediately following practice (T2), and following a three-day interval (T3)
| TD | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Duration | 0.19 (0.06) | 0.19 (0.10) | 0.19 (0.07) | 0.20 (0.08) | 0.18 (0.07) | 0.22 (0.11) |
| Duration COV | 0.26 (0.11) | 0.35 (0.19) | 0.27 (0.10) | 0.29 (0.16) | 0.35 (0.14) | 0.33 (0.11) |
| CAS | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Duration | 0.20 (0.06) | 0.19 (0.04) | 0.20 (0.03) | 0.20 (0.03) | 0.20 (0.03) | 0.22 (0.04) |
| Duration COV | 0.33 (0.19) | 0.31 (0.13) | 0.31 (0.13) | 0.31 (0.09) | 0.33 (0.09) | 0.33 (0.14) |
Duration COV
The coefficient of variation (standard deviation/mean) was calculated for duration values (duration COV) to examine changes in variability of jaw opening duration over time. In the TD group, mixed effects analyses revealed a significant change in duration COV over time for practiced tokens, F(2, 60) = 3.59, p = 0.03). Analyses indicated that variability increased from T1 to T2 (B = 0.27, SE = 0.10, p = 0.01) and did not change from T1 to T3 (B = 0.07, SE = 0.10, p = 0.50) or from T2 to T3 (B = −0.20, SE = 0.10, p = 0.06). Post-hoc analyses indicated no significant change in duration COV over time for novel as compared to real words, F(2, 58) = 1.00, p = 0.37. In the CAS group, analyses indicated no significant effect of time on duration COV for practiced tokens, F(2, 59.01) = 0.15, p = 0.86 (Table 4). For the non-practiced tokens, mixed effects analyses found no significant change over time for duration COV for either the TD, F(2, 38) = 1.94, p = 0.16, or CAS group, F(2, 32.76) = 0.12, p = 0.89.
Jaw Displacement
The jaw displacement measure captured the vertical movement from the point of oral closing to oral opening. In the TD group, there were no significant changes in jaw displacement over time for practiced tokens, F(2, 555.02) = 1.18, p = 0.31. In the CAS group, analyses indicated jaw displacement to significantly change over time for the practiced tokens, F(2, 518.32) = 3.38, p = 0.04. Regression analyses indicated no significant difference in jaw displacement from T1 to T2 (B = −0.53, SE = 0.35, p = 0.13) or from T1 to T3 (B = 0.37, SE = 0.35, p = 0.287). However, a significant increase in displacement was observed from T2 to T3 (B = 0.91, SE = 0.35, p = 0.01) (Table 5). Post-hoc analyses did not indicate changes in jaw displacement to differ between novel and real word tokens, F (2, 517.04) = 0.24, p = 0.79 (Figure 3). For non practiced tokens, there were no significant change over time for jaw displacement in the TD, F(2, 368.03) = 0.06, p = 0.94, or CAS group, F(2, 321.35) = 0.48, p = 0.62.
Table 5:
Mean (Standard Deviation) of opening jaw displacement (millimeters) and the variability of jaw displacement (coefficient of variation) for children with CAS and TD at baseline (T1), immediately following practice (T2), and following a three-day interval (T3)
| TD | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Displacement | 9.32 (3.77) | 9.06 (3.89) | 8.97 (3.42) | 7.49 (2.28) | 7.38 (2.87) | 7.44 (2.64) |
| Displacement COV | 0.27 (0.09) | 0.34 (0.17) | 0.26 (0.08) | 0.26 (0.09) | 0.29 (0.10) | 0.33 (0.08) |
| CAS | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Displacement | 10.34 (3.47) | 9.92 (3.18) | 10.84 (3.66) | 9.33 (2.92) | 9.46 (3.37) | 9.73 (3.10) |
| Displacement COV | 0.29 (0.13) | 0.34 (0.10) | 0.25 (0.10) | 0.25 (0.08) | 0.28 (0.11) | 0.26 (0.07) |
Figure 3.
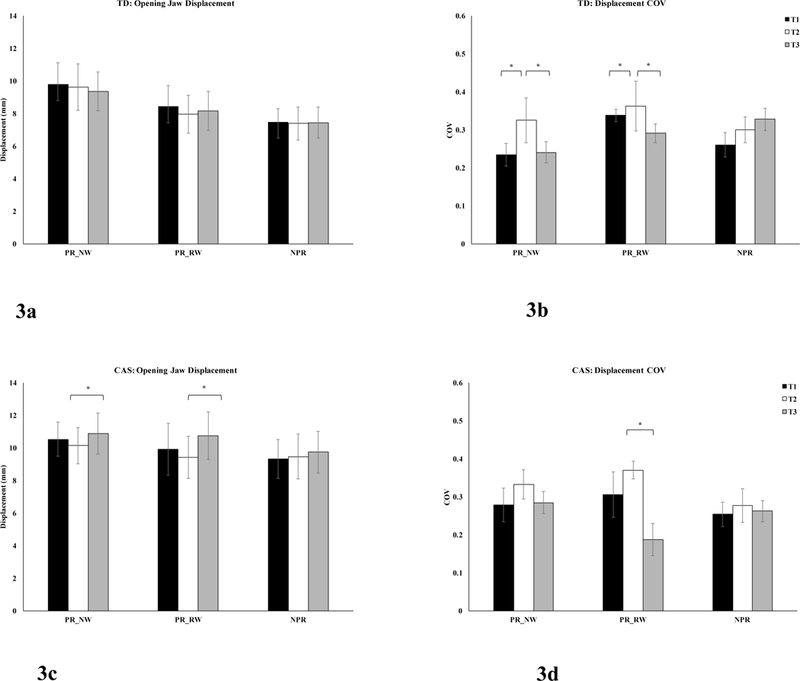
The mean and standard error jaw displacement and jaw displacement variability as measured by the coefficient of variation (COV) for the practiced novel words (PR_RW), practiced real word (PR_RW), and non-practiced words (NPR) at baseline (T1), immediately following practice (T2), and following a three-day interval (T3) in children with TD (a, b) and CAS (c, d).
Jaw Displacement COV
Variability of jaw opening displacement was examined over time using COV values (displacement COV). In the TD group, mixed effects analyses revealed a significant change in displacement COV over time in the practiced tokens, F(2, 62) = 3.41, p = 0.04. Analyses further revealed a significant increase in displacement COV from T1 to T2 (B = 0.07, SE = 0.03, p = 0.04) and a significant decrease from T2 to T3 (B = −0.08, SE = 0.03, p = 0.019). There was no significant change in the displacement COV from T1 to T3, B = −0.01, SE = 0.03, p = 0.72 (Table 5). Post-hoc analyses revealed no significant differences over time for displacement COV in the TD group for novel as compared to real word tokens, F(2, 64) = 0.55, p = 0.58.
In the CAS group, the fixed effect of time was found to have a significant impact on displacement COV for the practiced tokens, F(2, 59.095) = 6.11, p = 0.004. Analyses revealed that displacement COV significantly increased from T1 to T2 (B = 0.06, SE = 0.03, p = 0.03) and decreased from T2 to T3 (B = −0.09, SE = 0.03, p = 0.001). There were no differences from T1 to T3 (B = −0.03, SE = 0.03, p = 0.218). Post-hoc analyses revealed a significant difference in displacement COV over time for novel versus real word tokens, F(2, 56.104) = 3.86, p = 0.03. To explore this significant interaction, the data were subset into novel word (PR1, PR2) and real word (PR3) tokens to examine changes in displacement COV over time separately for novel and real words (Figure 3). The p-value was adjusted to p = 0.02 to account for multiple comparisons. No significant change in displacement COV over time was observed for the novel word tokens, F(2, 38) = 2.09, p = 0.14. However, displacement COV was found to change over time for the real word token, F(2, 12) = 7.18, p = 0.009. Analyses indicated a significant decrease in displacement COV from T1 to T3 (B = −0.12, SE = 0.05, p = 0.03) and from T2 to T3 (B = −0.18, SE = 0.05, p = 0.003). Thus, decreased jaw displacement variability was only seen in the real word token at the final time period. In the non-practiced tokens, displacement COV was similar across all time points for children in both the TD, F(2, 38) = 2.75; p = 0.08, and CAS groups, F(2, 29.30) = 0.35, p = 0.71.
Lip Aperture
Mixed effects analyses indicated no significant change in lip aperture over time in practiced tokens for children with TD, F(2, 557.02) = 0.88, p = 0.42, or CAS F(2, 56.72) = 0.14, p = 0.87 (Table 6). In the non-practiced tokens, lip aperture significantly changed over time for children in the TD group, F(2, 369.05) = 6.32, p = 0.002. Regression analyses indicated a significant increase in lip aperture from T2 to T3, B = 1.65, SE = 0.47, p = 0.0004 with no significant changes from T1 to T2 (B = −0.92, SE = 0.47, p = 0.052) or from T1 to T3 (B = 0.74, SE = 0.47, p = 0.12). In the CAS group, no significant differences in lip aperture were observed for non-practiced tokens, F(2, 31.81) = 0.03, p = 0.97.
Table 6:
Mean (Standard Deviation) of opening lip aperture (millimeters) and the variability of lip aperture (coefficient of variation) for children with CAS and TD at baseline (T1), immediately following practice (T2), and following a three-day interval (T3)
| TD | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Lip Aperture | 11.84 (4.55) | 11.68 (5.86) | 11.61 (4.32) | 11.42 (3.53) | 10.51 (4.73) | 12.15 (3.45) |
| Lip Aperture COV | 0.23 (0.09) | 0.31 (0.21) | 0.23 (0.09) | 0.27 (0.14) | 0.27 (0.11) | 0.25 (0.10) |
| CAS | Practiced Words | Non-Practiced Words | ||||
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Lip Aperture | 12.87 (4.68) | 12.93 (3.78) | 12.51 (4.85) | 12.89 (3.96) | 12.10 (4.97) | 12.35 (3.91) |
| Lip Aperture COV | 0.22 (0.13) | 0.26 (0.06) | 0.20 (0.09) | 0.21 (0.10) | 0.23 (0.08) | 0.25 (0.16) |
Lip Aperture COV
The variability of lip aperture was examined across each time period using the COV values (lip aperture COV). For practiced tokens, mixed effects analyses did not indicate a significant effect of time on lip aperture COV for children in the TD, F(2, 60) = 3.05, p = 0.06, or CAS groups, F(2, 31.80), = 0.82, p = 0.45 (Table 6). For non-practiced tokens, analyses indicated that lip aperture COV did not change over time for children in the TD, F(2, 38) = 0.17, p = 0.84, or CAS groups, F(2, 57.06) = 2.42, p = 0.10.
Discussion
The purpose of this work was to explore changes in speech motor control associated with a movement transition between a consonant-vowel sequence across a practice period in children with CAS and in children with typical speech and language development. In the CAS group, jaw movement displacement increased in all practiced words (real and novel word) from T2 to T3. Displacement variability increased from T1 to T2 for all practiced words, then decreased from T2 to T3 for the practiced real word only. There were no significant changes in movement duration or lip aperture displacement. While our results revealed several changes in movement kinematics, the only evidence that supported our initial predictions was a decrease in displacement variability from T2 to T3. Practice effects were also evident in the TD group, which included changes in movement variability in the practiced word and duration/lip aperture in the non-practiced word. Movement changes were not anticipated in the TD group, however, based on prior whole word analyses involving these same TD children (Case & Grigos, 2016). Though the CAS and TD groups were analyzed separately to capture the trajectory of change for each group of children, it was noted qualitatively that by the final session (Time 3) there was a tendency for jaw opening displacement to be larger and displacement COV to be smaller in the CAS than TD groups. Taken together, these findings provide insight into the manner in which children refine their articulator movements during structured practice, which will be expanded upon below.
Refined movement transitions
One focus of this research was to examine properties of speech motor control that underlie a movement transition. Movement from oral closing to oral opening may be challenging because vowels require less precision than consonants and do not have a specific articulatory contact. Children in both the TD and CAS groups refined this movement transition over a practice period by reducing variability, which was consistent with past research (Heisler et al., 2010; Sasisekaran et al., 2010; Walsh et al., 2006). Thus, reduced movement variability appeared to be a positive outcome of practice. Additionally, children with CAS adjusted spatial control to achieve such variability changes in the practiced words, which was not seen in the TD children. Increased amplitude may have helped stabilize their articulatory systems, therefore driving the reduction in variability (Terband, et al., 2011). Greater stability in the production of the initial syllable could have facilitated improved motor control for subsequent phonemes in the words, thus contributing to the significant gains in word accuracy with practice. Lastly, evidence of change in jaw displacement but not lip aperture suggests that the jaw may have been easier to stabilize that the lips, which is consistent with developmental findings that jaw stability is achieved before lip stability in young children (Green et al., 2002). Research conducted over a longer practice period is needed to elucidate whether changes in jaw movement displacement and variability are maintained in order to fully determine whether these patterns are facilitative or maladaptive in nature. Further, the possible relationships between variables, such as displacement and variability, must be explored in finer detail to understand if and how change in one may influence the other within a practice paradigm.
Changes in both displacement and variability were observed in the practiced real word, bubblegum, but not in the practiced novel words, in the CAS group. Differences in vowel type between tokens offer one explanation for this result. The initial vowel /ʌ/ in bubblegum is a central vowel as compared to the low back vowel /a/ in the novel words badabap and madeepoom. The transition into a neutral vowel pattern may be easier than the movement into a back vowel (that involves more lingual movement), particularly in the context of an anterior consonant. The same biomechanical constraints that influence babbling where anterior consonants are likely to be paired with central vowels (Davis & MacNeilage, 1990) may be evident in older children with speech impairment. Thus, patterns that are more likely to occur in early development may be easier to refine with practice in children with CAS. This result encourages us to consider how the transition between segments may be differentially impacted by consonant and vowel characteristics. This can have important implications for the design of treatment stimuli, which warrants further study.
A second explanation for changes in variability over time is that variability may be differentially influenced by word status (i.e. real vs. novel word). One could argue that novel words pose greater linguistic and motoric challenge for speakers (e.g., Sasisekaran et al., 2010), which would result in greater movement variability for novel than real word tokens. This explanation seems less plausible, however, as there were no significant differences in consonant/vowel accuracy between real and novel words when examined at the level of the movement transition (i.e. C1 and V1) in the CAS and TD groups. Further, similar improvements in consonant and vowel accuracy were observed at the word level even though familiarity with the real word token was likely to have varied between children (i.e. some five-year-olds will have had some exposure to the word bubblegum while others will have had none). Our findings were consistent with past research that did not show differences in speech accuracy in the production of real versus nonword stimuli in children with CAS (Thoonen, Maasen, Gabreels, Schreuder, & Swart, 1997). That same work, however, did reveal greater accuracy for real vs. nonwords in typically developing children. Given that use of nonword vs. real word stimuli during treatment is a debated topic in the field (e.g., Maas, Gildersleeve-Neumann, Jakielski, & Stoeckel, 2014) further research is warranted to explore whether long-term maintenance of practice gains would be influenced by lexical status and word familiarity. One additional consideration is that language ability may influence performance on a nonword vs. a real word task. Therefore, similar performance in terms of speech accuracy between nonword and real word stimuli in the present work may have been supported by the typical language skills displayed by all participants.
Reconstructing motor schemas with practice
Articulator movement changes across this practice period were consistent with a “reconstruction process” described within schema theory (Schmidt, 2003, p.371). When reconstructing an existing motor schema, a series of modifications are made to movement parameters across successive attempts of a target. In the present investigation, changes in movement displacement and variability indicated that adjustments were being made to these schemas with practice in the TD children and children with CAS. Of note, motor schemas were refined in the CAS group through changes in variability and spatial control, but not through adjustments in the temporal domain. Lack of change in temporal control was surprising given that longer movement duration has been reported in children with CAS (Case & Grigos, 2016; Grigos et al., 2015; Moss & Grigos, 2012) and in children with specific language impairment (Goffman, 1999; Goffman, 2004), as compared to children with typical speech and language development. It is plausible that temporal patterns may be less flexible to change with practice and/or that a longer practice period was required to elicit changes in the temporal domain in children with CAS. Decreased variability in the practiced, real word token combined with maintained gains in consonant and vowel accuracy at the final time period suggested that motor learning was occurring. However, one could question these gains, as they did not generalize to stimuli not included in the practice session, in the CAS group. It is likely that the practice period for the current experiment was insufficient to elicit more widespread change in both practiced and non-practiced tokens over time. Further research is needed to explore whether additional time engaged in structured practice would result in carryover to non-practiced tokens. In contrast to the children with CAS, the TD children displayed movement changes in the non-practiced tokens between T2 and T3. Lip aperture decreased and duration increased (in the absence of variability changes) suggesting that the TD children have flexibility to alter both spatial and temporal aspects of movement to achieve a speech goal. As parallel gains were not observed in the practiced tokens, we do not interpret these changes as generalization of practice effects. Rather these changes reflect flexibility in TD children to alter both spatial and temporal aspects of movement to achieve a speech goal in the absence of direct practice.
An additional consideration is whether practice gains were supported by variable practice of combined real and novel word tokens. Variable practice is believed to result in greater stability for a targeted movement schema, as it provides a range of practice conditions which results in greater flexibility and control to modify movement parameters (Ballard, Maas, & Robin, 2007). Variable practice that involves both real and novel word stimuli may simultaneously address motor planning skills and carryover of these skills to other stimuli. As supported by a number of researchers (Ballard et al., 2010; Van der Merwe, 2011), novel word stimuli could be used to directly address underlying motor planning deficits. Nonwords allow practice of the movement sequences within consonant-vowel combinations that do not have pre-existing linguistic representation. One challenge, however, involves the generalization of these skills to real words or novel contexts. Incorporating real word stimuli into the same practice sets that include novel word targets may facilitate a child’s ability to immediately apply skills to linguistically meaningful words. Further, the degree of practice and structure of targeted real words (i.e., consonant vowel combinations within a word) should be carefully considered to facilitate generalization of practice gains. Our findings highlight the need to explore this element of treatment design and whether variable practice may lead to more robust speech motor learning.
Clinical Implications
Our motivation for examining how children with CAS respond to practice is driven by the notions that poor generalization and slow treatment progress are characteristic of this impairment. Prior studies identified movement variability as the one parameter that distinguished children with CAS from children with other speech sound disorders (Moss & Grigos, 2012; Grigos et al., 2015), a result that encouraged us to explore whether articulatory control is refined with practice. Case & Grigos (2016) addressed this question, but did not find changes in movement variability when measured at the whole-word level. In the current work, however, changes in articulatory control were found when using single point measures to examine movement parameters at a finer level (i.e., close-open gesture). This level of detail may be necessary to capture nuanced adjustments to motor control in children with CAS following practice, particularly those associated with movements between segments.
One clinical implication of these findings is that a movement transition between a consonant and vowel can be modified even though the sound sequence is judged to be accurate by a trained listener. Both PCC and PVC improved across all phonemes for practiced words, although there were no significant improvements in accuracy for the consonant and vowel of the first syllable. Nonetheless, the movements associated with the movement transition in the first syllable were refined with practice as children worked towards improved word accuracy. The disparity between transcription and kinematic results highlight the value of tools such as kinematic analysis that allow us to capture aspects of speech output that may not be perceivable. Such subtle articulatory changes may lay the foundation for improved consonant and vowel production across syllables and words that could be achieved with additional practice. Our results raise the possibility that children with CAS require ongoing practice that strengthens already established movement sequences. Building speech motor skill in this way could result in improved generalization and maintenance.
A second clinical implication is that the findings support treatment approaches that focus on practice of movement gestures at the level of the syllable (Strand & Skinder, 1999; Strand, Stoeckel & Baas, 2006) rather than on individual sounds in children with CAS. Thus when selecting stimuli within treatment, the clinician may consider how consonant-vowel combinations address movement from closure for an initial consonant to different degrees of oral aperture in subsequent vowels. Practice of stimuli designed accorded to type of movement transition could potentially lead to more longstanding change in the underlying motor control processes.
Limitations
There were several limitations associated with this work. A small group of participants with CAS were studied who displayed age-appropriate receptive language and cognition. While we intentionally controlled for these variables, there is a great deal of heterogeneity in CAS with respect to concomitant deficits in language and cognition, which could impact performance on a practice test. These factors influence the generalizability of the findings. An additional limitation was the analysis unit. While we proposed that studying articulator movement from consonant to vowel captures the movement transition between sounds, speech production involves many different transitions (e.g. vowel to consonant, consonant to consonant, syllable to syllable). Further research is needed to understand how task demands may influence the production of a range of transitions in this population. The findings were also limited by the need to study accurate productions using kinematic analysis. While we are confident that our kinematic findings were not influenced by speech sound errors, there is a great deal that can be learned from the difficulty children with CAS may have transitioning between segments that can only be captured by analyzing speech errors. Lastly, it is important to keep in mind that these findings are specific to children with CAS. Additional research is needed to understand whether children with other speech sound disorders would display similar patterns.
Conclusions
With a greater understanding of the characteristics associated with CAS over recent years comes the need for research that quantifies changes in speech production following practice in this population. The present work addressed this need and revealed that movement transitions were refined with practice in children with CAS through changes in jaw opening displacement and variability. Observations of both increased displacement and decreased variability supported the notion that greater amplitude may have facilitated movement stability. These results leave us questioning whether changes in speech motor control may lay the foundation for segmental changes that may emerge with additional practice. Future research is warranted to explore this notion further.
Acknowledgments
The authors would like to acknowledge Hailey Small, Penelope Elias, Lauren Perry, and Panagiota Tampakis for assistance with data collection and processing. We are grateful to the participants and their families for their dedication to the project.
Funding
This research was supported by funding from National Institute on Deafness and Other Communicative Disorders Grant R03DC009079 and the Childhood Apraxia of Speech Association of North America.
Appendix A: CAS Diagnostic Framework and Criteria
Criteria for CAS Diagnosis:
(Speaking Contexts Assessed = Single words, connected speech, syllable sequencing tasks)
Presence of all three characteristics identified in the ASHA (2007) position statement (I,II,III)1 in more than one speaking context2;
At least four out of the seven characteristics shown below;
| Characteristic | Definition | Criteria |
|---|---|---|
| I. Impaired co-articulatory transitions1, 3, 4, 5 | Difficulties forming articulatory transitions between adjacent sounds and/or syllables, particularly when they included phonemes that were present in the child’s repertoire; | All characteristics must be observed at least three times in more than one speaking context |
| (Example: difficulty combining the phoneme /b/ with different vowels, even though /b/ and the vowels are accurately produced in other contexts). | ||
| II. Inconsistent errors on same word productions1, 5, 6 | Consonant and vowel errors that differ across repeated productions of the same word; | |
| (Example: hot /hat/ → /ha/, /at/, or /ta/ by the same speaker). | ||
| III. Inappropriate prosody1, 3, 4, 5, 6 | Syllable segregation, slow speech rate, equal stress, incorrect lexical and phrasal stress | |
| 1. Vowel errors1, 3, 4, 5, 6, 7, 8 | Vowel substitutions, omissions, distortions, or complexity changes | A characteristic must
be observed at least three times in more than one speaking
context. |
| (Example: reducing a diphthong to a monophthong) | ||
| 2. Timing errors1, 3, 4, 5 | Voicing errors1, 3, 4, 5, errors related to nasality1, 5 | |
| (Example: denasalization, nasalization) | ||
| 3. Speech sound distortions1, 3, 4, 5 | Perceived deviations with respect to the place, manner, or voicing that do not result in the substitution of a different phoneme for the target phoneme | |
| (Example: partially voiced production of /p/, excess aspiration of /k/) | ||
| 4. Articulatory groping1, 3, 4, 5 | Visual struggle of articulator movements that accompany phoneme production | |
| 5. Errors increase with length and complexity1, 3, 4, 5, 6 | Increased errors as syllable number (e.g., monosyllabic vs multisyllabic), phrase, and sentence length increase. | |
| 6. Atypical errors1 | Substitution, omission error patterns
that are not expected in the course of typical development
(Examples: initial consonant deletion, glottal substitution, backing) |
|
| 7. Reduced phonetic inventory6 | A child is not producing phonemes acquired by 90% of same-age children9 | |
Footnotes
Declaration of Interest
The authors report no conflicts of interest.
References
- American Speech-Language-Hearing Association. (2007). Childhood apraxia of speech [Technical Report].
- Baayen RH, Davidson DJ, & Bates DM (2008). Mixed-effects modeling with crossed random effects for subjects and items. Journal of Memory and Language, 59(4), 390–412. doi: 10.1016/j.jml.2007.12.005. [DOI] [Google Scholar]
- Ballard KJ, Robin DA, McCabe P, & McDonald J (2010). A treatment for dysprosody in childhood apraxia of speech. Journal of Speech, Language,&Hearing Research,53, 1227–1245. [DOI] [PubMed] [Google Scholar]
- Ballard KJ, Maas E, & Robin DA (2007). Treating control of voicing in apraxia of speech with variable practice. Aphasiology, 21(12), 1195–1217. [Google Scholar]
- Bates D, Maechler M, Bolker B, & Walker S (2010). Linear mixed-effects models using Eigen and S4 (Version 1.1). Retrieved from http://lme4.r-forge.r-project.org/.
- Burgmeister B, Blum L, & Lorge I (1972). Columbia Mental Maturity Scale. The Psychological Corporation. [Google Scholar]
- Case J, & Grigos MI (2016). Articulatory control in childhood apraxia of speech in a novel word learning task. Journal of Speech, Language, and Hearing Research, 59, 1253–1268. doi: 10.1044/2016_JSLHR-S-14-0261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis BL, Jacks A, & Marquardt TP (2005). Vowel patterns in developmental apraxia of speech: three longitudinal case studies. Clinical linguistics & phonetics, 19(4), 249–274. [DOI] [PubMed] [Google Scholar]
- Davis BL, Jakielski KJ, & Marquardt TP (1998). Developmental apraxia of speech: Determiners of differential diagnosis. Clinical linguistics & phonetics, 12(1), 25–45. [Google Scholar]
- Davis BL, & MacNeilage PF (1990). Acquisition of Correct Vowel Production: A Quantitative Case Study. Journal of Speech, Language, and Hearing Research, 33(1), 16–27. [DOI] [PubMed] [Google Scholar]
- Edeal DM, & Gildersleeve-Neumann CE (2011). The importance of production frequency in therapy for childhood apraxia of speech. American Journal of Speech-Language Pathology, 20(2), 95–110. [DOI] [PubMed] [Google Scholar]
- Forrest K (2003). Diagnostic criteria of developmental apraxia of speech used by clinical speech-language pathologists.American Journal of Speech-Language Pathology, 12(3),376–380. [DOI] [PubMed] [Google Scholar]
- Goffman L (2004). Kinematic differentiation of prosodic categories in normal and disordered language development. Journal of Speech, Language, and Hearing Research, 47(5), 1088–1102. [DOI] [PubMed] [Google Scholar]
- Goffman L, & Smith A (1999). Development and phonetic differentiation of speech movement patterns. Journal of Experimental Psychology: Human perception and performance, 25(3), 649. [DOI] [PubMed] [Google Scholar]
- Goldman, & Fristoe (2000). Goldman Fristoe Test of Articulation (2nd ed). Circle Pines, MN: American Guidance Service, Inc. [Google Scholar]
- Green JR, Moore CA, Higashikawa M, & Steeve RW (2000). The Physiologic Development of Speech Motor Control. Lip and Jaw Coordination. Journal of Speech, Language, and Hearing Research, 43(1), 239–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green JR, Moore CA, & Reilly KJ (2002). The sequential development of jaw and lip control for speech. Journal of Speech, Language, and Hearing Research, 45, 66–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grigos MI (2009). Changes in articulator movement variability during phonemic development: a longitudinal study. Journal of Speech, Language, and Hearing Research, 52(1), 164–177. [DOI] [PubMed] [Google Scholar]
- Grigos MI, & Kolenda N (2010). The relationship between articulatory control and improved phonemic accuracy in childhood apraxia of speech: A longitudinal case study. Clinical linguistics & phonetics, 24(1), 17–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grigos MI, Moss A, & Lu Y (2015). Oral articulatory control in childhood apraxia of speech. Journal of Speech, Language, and Hearing Research, 58(4), 1103–1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grigos MI, & Patel R (2007). Articulator movement associated with the development of prosodic control in children. Journal of Speech, Language& Hearing Research, 50(1), 119–130. [DOI] [PubMed] [Google Scholar]
- Grigos MI, Saxman JH, & Gordon AM (2005). Speech motor development during acquisition of the voicing contrast. Journal of Speech, Language, and Hearing Research, 48(4), 739–752. [DOI] [PubMed] [Google Scholar]
- Hall KG, & Magill RA (1995). Variability of practice and contextual interference in motor skill learning. Journal of motor behavior, 27(4), 299–309. [DOI] [PubMed] [Google Scholar]
- Hayden DA, & Square PA (1999). VMPAC: Verbal Motor Production Assessment for Children. San Antonio: Psychological Association. [Google Scholar]
- Heisler L, Goffman L, & Younger B (2010). Lexical and artic- ulatory interactions in children’s language production. Developmental Science, 13, 722–730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hresko W, Reid D, & Hammill D (2007). Test of Early Language Development (3rd ed.). Austin, TX: Pearson Assessment. [Google Scholar]
- Iuzzini J, & Forrest K (2010). Evaluation of a combined treatment approach for childhood apraxia of speech. Clinical linguistics & phonetics, 24(4–5), 335–345. [DOI] [PubMed] [Google Scholar]
- Knock TR, Ballard KJ, Robin DA, & Schmidt RA (2000). Influence of order of stimulus presentation on speech motor learning: A principled approach to treatment for apraxia of speech. Aphasiology, 14(5–6), 653–668. [Google Scholar]
- Kuznetsova A, Brockhoff PB, & Christensen RH (2013). lmerTest: Tests for random and fixed effects for linear mixed effect models (lmer objects of lme4 package) (Version 2.0). Retrieved from http://lmertest.r-forge.r-project.org/.
- Maas E, Butalla CE, & Farinella KA (2012). Feedback frequency in treatment for childhood apraxia of speech. American Journal of Speech-Language Pathology, 21(3), 239–257. [DOI] [PubMed] [Google Scholar]
- Maas E, Gildersleeve-Neumann CE, Jakielski KJ, & Stoeckel R (2014). Motor-based intervention protocols in treatment of childhood apraxia of speech (CAS). Current developmental disorders reports, 1(3), 197–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MathWorks, Inc. (2013). MATLAB Version 8.1 [computer software]. Natick, MA: The Mathworks Inc. [Google Scholar]
- Moss A, & Grigos MI (2012). Interarticulatory coordination of the lips and jaw in childhood apraxia of speech. Journal of Medical Speech-Language Pathology, 20(4), 127–132. [PMC free article] [PubMed] [Google Scholar]
- Nijland L, Maassen B, & van der Meulen S (2003a). Evidence of motor programming deficits in children diagnosed with CAS. Journal of Speech, Language, and Hearing Research, 46, 437–450. [DOI] [PubMed] [Google Scholar]
- Nijland L, Maassen B, Van Der Meulen S, Gabreëls F, Kraaimaat FW, & Schreuder R (2003b). Planning of syllables in children with developmental apraxia of speech. Clinical linguistics & phonetics, 17(1), 1–24. [DOI] [PubMed] [Google Scholar]
- Nip ISB, Green JR, & Marx DB (2009). Early speech motor development: Cognitive and linguistic considerations. Journal of Communication Disorders, 42, 286–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollock KE (2002). Identification of vowel errors: Methodological issues and preliminary data from the Memphis Vowel Project. Vowel disorders, 83–113. [Google Scholar]
- Pollock K, & Hall P (1991). An analysis of the vowel misarticulations of five children with developmental apraxia of speech. Clinical linguistics & phonetics, 5(3), 207–224. [Google Scholar]
- Sasisekaran J, Smith A, Sadagopan N, & Weber-Fox C (2010). Nonword repetition in children and adults: Effects on movement coordination. Developmental Science, 13, 521–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt RA (1975). A schema theory of discrete motor skill learning. Psychological review, 82(4), 225. [Google Scholar]
- Schmidt RA (2003). Motor schema theory after 27 years: Reflections and implications for a new theory. Research quarterly for exercise and sport, 74(4), 366–375. [DOI] [PubMed] [Google Scholar]
- Schmidt RA, & Lee T (1988). Motor control and learning. Human kinetics. [Google Scholar]
- Sharkey SG, & Folkins JW (1985). Variability of Lip and Jaw Movements in Children and Adults Implications for the Development of Speech Motor Control. Journal of Speech, Language, and Hearing Research, 28(1), 8–15. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Aram DM, & Kwiatkowski J (1997a). Developmental Apraxia of Speech I. Descriptive and Theoretical Perspectives. Journal of Speech, Language, and Hearing Research, 40(2), 273–285. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Aram DM, & Kwiatkowski J (1997b). Developmental Apraxia of Speech II. Toward a Diagnostic Marker. Journal of Speech, Language& Hearing Research, 40, 286–312. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Aram DM, & Kwiatkowski J (1997c). Developmental Apraxia of Speech III. A Subtype Marked by Inappropriate Stress. Journal of Speech, Language, and Hearing Research, 40(2), 313–337. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Austin D, Lewis BA, McSweeny JL, & Wilson DL (1997d). The Percentage of Consonants Correct (PCC) Metric Extensions and Reliability Data. Journal of Speech, Language, and Hearing Research, 40(4), 708–722. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Strand EA, Fourakis M, Jakielski KJ, Hall SD, Karlsson HB, ... & Wilson DL (2017a). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: I. Development and description of the Pause Marker. Journal of Speech, Language, and Hearing Research, 60(4), S1096–S1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shriberg LD, Strand EA, Fourakis M, Jakielski KJ, Hall SD, Karlsson HB, ... & Wilson DL (2017b). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: II. Validity studies of the Pause Marker. Journal of Speech, Language, and Hearing Research, 60(4), S1118–S1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shriberg LD, Strand EA, Fourakis M, Jakielski KJ, Hall SD, Karlsson HB, ... & Wilson DL (2017c). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: III. Theoretical coherence of the Pause Marker with speech processing deficits in Childhood Apraxia of Speech. Journal of Speech, Language, and Hearing Research, 60(4), S1135–S1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shriberg LD, Strand EA, Fourakis M, Jakielski KJ, Hall SD, Karlsson HB, … & Wilson DL (2017d). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: IV. The Pause Marker Index. Journal of Speech, Language, and Hearing Research, 60(4), S1153–S1169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith BL, & Gartenberg TE (1984). Initial observations concerning developmental characteristics of labio‐mandibular kinematics. J Acoust Soc Am, 75(5), 1599–1605. [DOI] [PubMed] [Google Scholar]
- Smith A, & Goffman L (1998). Stability and patterning of speech movement sequences in children and adults. Journal of Speech, Language, and Hearing Research, 41(1), 18–30. [DOI] [PubMed] [Google Scholar]
- Strand E, & Debertine P (2000). The efficacy of integral stimulation intervention with developmental apraxia of speech. Journal of Medical Speech-Language Pathology, 8(4), 295–300. [Google Scholar]
- Strand EA, Stoeckel R, & Baas B (2006). Treatment of severe childhood apraxia of speech: A treatment efficacy study. Journal of Medical Speech-Language Pathology, 14(4), 297–308. [Google Scholar]
- Terband H, Maassen B, Van Lieshout P, & Nijland L (2011). Stability and composition of functional synergies for speech movements in children with developmental speech disorders. Journal of communication disorders, 44(1), 59–74. [DOI] [PubMed] [Google Scholar]
- Thoonen G, Maassen B, Gabreels F, Schreuder R, & Swart B (1997). Towards a standardised assessment procedure for developmental apraxia of speech. International Journal of Language & Communication Disorders, 32(1), 37–60. [DOI] [PubMed] [Google Scholar]
- Van der Merwe A (2011). A speech motor learning approach to treating apraxia of speech: Rationale and effects of intervention with an adult with acquired apraxia of speech. Aphasiology, 25(10), 1174–1206. [Google Scholar]
- Velleman S, & Strand K (1994). Developmental verbal dyspraxia In Bernthal J & Bankson N (Eds.), Child phonology: Characteristics, assessment, and intervention with special populations (pp. 110–139). New York: Thieme Medical. [Google Scholar]
- Vicon Motion Systems. (2001). Vicon 460 [computer software]. Los Angeles, California.
- Vuolo J, & Goffman L (2016). An exploratory study of the influence of load and practice on segmental and articulatory variability in children with speech sound disorders. Clinical Linguistics & Phonetics, DOI: 10.1080/02699206.2016.1261184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh B, & Smith A (2002). Articulatory Movements in Adolescents Evidence for Protracted Development of Speech Motor Control Processes. Journal of Speech, Language, and Hearing Research, 45(6), 1119–1133. [DOI] [PubMed] [Google Scholar]
- Walsh B, Smith A, & Weber-Fox C (2006). Short-term plasticity in children’s motor speech systems. Developmental Psychobiology, 48, 660–674. [DOI] [PubMed] [Google Scholar]
- 1. American Speech-Language-Hearing Association. (2007). Childhood apraxia of speech [Technical Report].
- 2. Shriberg LD, Fourakis M, Hall SD, Karlsson HB, Lohmeier HL, McSweeny JL, … & Wilson DL (2010). Extensions to the speech disorders classification system (SDCS). Clinical Linguistics & Phonetics, 24(10), 795–824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Shriberg LD, Lohmeier HL, Strand EA, & Jakielski KJ (2012). Encoding, memory, and transcoding deficits in childhood apraxia of speech. Clinical Linguistics & Phonetics, 26(5), 445–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Shriberg LD, Strand EA, Fourakis M, Jakielski KJ, Hall SD, Karlsson HB, … & Wilson DL (2017a). A diagnostic marker to discriminate childhood apraxia of speech from speech delay: I. Development and description of the Pause Marker. Journal of Speech, Language, and Hearing Research, 60(4), S1096–S1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Grigos MI, Moss A, & Lu Y (2015). Oral articulatory control in childhood apraxia of speech. Journal of Speech, Language, and Hearing Research, 58(4), 1103–1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Pollock KE, & Hall PK (1991). An analysis of the vowel misarticulations of five children with developmental apraxia of speech. Clinical Linguistics & Phonetics, 5(3), 207–224. [Google Scholar]
- 7. Davis BL, Jakielski KJ, & Marquardt TP (1998). Developmental apraxia of speech: Determiners of differential diagnosis. Clinical Linguistics & Phonetics, 12(1), 25–45. [Google Scholar]
- 8. Davis BL, Jacks A, & Marquardt TP (2005). Vowel patterns in developmental apraxia of speech: three longitudinal case studies. Clinical linguistics & phonetics, 19(4), 249–274. [DOI] [PubMed] [Google Scholar]
- 9. Smit AB, Hand L, Freilinger JJ, Bernthal JE, & Bird A (1990). The Iowa articulation norms project and its Nebraska replication. Journal of Speech and Hearing Disorders, 55(4), 779–798 [DOI] [PubMed] [Google Scholar]