

Abstract
Many hamstring injuries that occur during physical activity occur while the muscles are lengthening, during eccentric hamstring muscle actions. Opposite of these eccentric hamstring actions are concentric quadriceps actions, where the larger and likely stronger quadriceps straighten the knee. Therefore, to stabilize the lower limbs during movement, the hamstrings must eccentrically combat against the strong knee-straightening torque of the quadriceps. As such, eccentric hamstring strength expressed relative to concentric quadricep strength is commonly referred to as the "functional ratio" as most movements in sports require simultaneous concentric knee extension and eccentric knee flexion. To increase the strength, resiliency, and functional performance of the hamstrings, it is necessary to test and train the hamstrings at different eccentric speeds. The main purpose of this work is to provide instructions for measuring and interpreting eccentric hamstring strength. Techniques for measuring the functional ratio using isokinetic dynamometry are provided and sample data will be compared. Additionally, we briefly describe how to address hamstring strength deficiencies or unilateral strength differences using exercises that specifically focus on increasing eccentric hamstring strength.
Keywords: Medicine, Issue 135, Sport science, preventive intervention, quadriceps, isokinetic, eccentric exercises, bilateral ratio, ipsilateral ratio, lower limb, resistance training, conditioning, muscle weakness, injuries
Introduction
The relationship between knee flexor and extensor strength has been identified as an important parameter in assessing a person's risk of incurring a lower limb injury1. Specifically, there is an increased probability of hamstring injury when ipsilateral or bilateral imbalances in hamstring strength are present when compared to quadricep strength2. Therefore, many sport scientists and practitioners test knee flexor and extensor strength to determine whether an athlete is at risk of incurring a hamstring injury. However, various testing methods are used that do not allow for direct comparisons to be made between methods (e.g., different contraction speeds, different muscle actions, and field testing vs. laboratory testing)3,4,5,6,7,8,9. Although different testing methods provide different bits of valuable information regarding strength levels, the methodological approach for thigh muscle isokinetic strength testing should be unified to enable comparisons across individuals, populations, and time.
Although the evaluation of ipsilateral imbalances between knee flexors and extensors have been often described using the conventional concentric hamstring to concentric quadriceps ratio (H/QCONV)10,11, co-activation of the knee flexors and extensors is known to occur during all movements and takes place through opposing contraction modes. To explain, the knee extensors are primarily involved in propulsion during jumping and running, whereas the knee flexors primarily stabilize the knee during landing and running by decelerating the lower limb and counteracting the rapid and forceful concentric contractions of the extensors. As most movements in sports require simultaneous concentric knee extension and eccentric knee flexion, a relative strength comparison between the two would be appropriate. Therefore, eccentric knee flexor strength relative to concentric knee extensor strength is commonly tested and is known as the "functional ratio" (H/QFUNC)12.
Compared to the H/QCONV ratio where values can range from 0.43 to 0.9012, the H/QFUNC ratio can range from 0.4 to 1.413, indicating that data from different protocols should not be compared to each other. Although maximal concentric torque decreases as concentric speed increases14,15,16, eccentric torque is greater than concentric torque as speed increases16,17. As such, the H/QFUNC ratio can approach a value of 1.0 as the speed of testing contraction increases13,18. Since most sport movements occur at high velocities, knee extensor and flexor strength testing are likely more ecologically valid at higher speeds. Therefore, such strength testing protocols should include progressively increased speeds in a stepwise progression.
If isokinetic testing reveals a large discrepancy between eccentric hamstring and concentric quadricep strength, the discrepancy should be narrowed through training. For this purpose, decreasing knee extensor strength should never compensate for weak knee flexors at the expense of a more favorable H/QFUNC ratios, especially in sporting environments. The other option would be to progressively and intensively increase knee flexor strength so that the hamstrings become stronger, especially in relation to the quadriceps, at higher speeds. Therefore, if isokinetic testing reveals some degree of hamstring weakness, a training intervention will likely be necessary to increase hamstring strength, especially during eccentric muscle actions. As with all training interventions, follow-up testing should be performed to determine the efficacy of the eccentrically-focused hamstring strength training program, and further adjustments may need to be made. The objective of this paper is to describe how to test isokinetic functional eccentric hamstring strength, reveal potential hamstring weakness, and suggest how to resolve a functional hamstring weakness.
Protocol
The presented protocol follows the guidelines of human research ethics committee at Charles University, Faculty of Physical Education in Sport and has been previously approved as part of research.
1. Familiarize All Subjects Before Isokinetic Testing by Following Steps
Ensure that the subjects have not had any recent musculoskeletal injuries or pain in the lower limbs in the previous 6 months. If a subject reports recent knee pain, or has knee pain during testing, exclude the subject.
As eccentric isokinetic testing is likely a novel stimulus for many individuals, familiarize the subject with the protocols on a valid isokinetic dynamometer19,20 (steps 1.3 to 1.7.6, below) at least twice before participating in official testing. Instruct the subjects to not perform any lower body resistance training, or other strenuous exercises, 72 h before testing.
- To begin, guide the subjects through a general warm up.
- Instruct the subjects to jog for 5-10 min or cycle for 5-10 min on an ergometer with a resistance of 1.5-2 W/kg of body mass with a cadence between 60-90 rpm.
- After cycling, instruct the subjects to perform two sets of 8-10 body weight lunges and 8-10 hamstring curls on a Swiss ball with each leg with 1 min of rest between sets.
- Next, guide the subjects through dynamic stretching of the lower limbs including the quadriceps and hamstrings21.
Show the subject an example of the isokinetic torque-angle curve and explain that live visual feedback will be provided during the test.
Explain that the subject should "kick out as hard and fast as possible" for concentric knee extension and "pull back as hard as fast as possible" for concentric knee flexion. Also explain that the machine will move on its own during eccentric actions, but that the subject should try to "push as hard as possible" during eccentric knee flexion (eccentric action of the quadriceps) and "pull as hard as possible" during eccentric knee extension (eccentric actions of the hamstrings).
Allow the subject to ask any questions and make sure they understand what will happen during the test. Clearly state that if the subject experiences any pain or discomfort during the test that makes the subject wish to terminate the test at any time, the subject should inform the researcher immediately, and the test can be safely aborted.
- Start the pre-set protocol listed in Table 1, and continually guide the subject through the protocol.
- Using the recommendations of Brown22, position the subject on the dynamometer in a sitting position with a hip angle of 100° of extension. Adjust the settings of the dynamometer to ensure that the subject's hips are all the way back and in contact with the chair and the dynamometer's axis of rotation axis is in-line with the axis of rotation of the subject's tested knee.
- Instruct the subject to hold a deep breath while fixing the shoulders, pelvis, and thigh of the tested leg using the pads and straps on the dynamometer. Fix the lever arm of the dynamometer to the distal part of the shin with the pad placed 2.5 cm over the apex of the medial malleolus, but do not support the non-exercised lower limb.
- Allow the subject to passively and actively go through the full extension and flexion range of motion while readjusting the straps, dynamometer settings, or both if needed.
- Ensure that the subjects can see a screen that shows the torque-angle curve and provide a verbal countdown to begin the test. Instruct the subjects to hold the handgrips located at the side of the seat during all testing efforts.
- Start the test and verbally encourage the subject by using phrases such as "go", "push harder", "pull, pull, pull", etc. During the rest intervals, provide the subject with short instructions about the upcoming task.
- After completing the protocol, allow the subject to get out of the dynamometer chair, and adjust the dynamometer to test the other limb.
- After repositioning the subject and adjusting the machine accordingly, perform the gravity correction measurement again and start the test for the untested lower limb.
- Open the test results that show the angle-torque curve and check whether the subject achieved the selected speed of contraction for the whole movement.
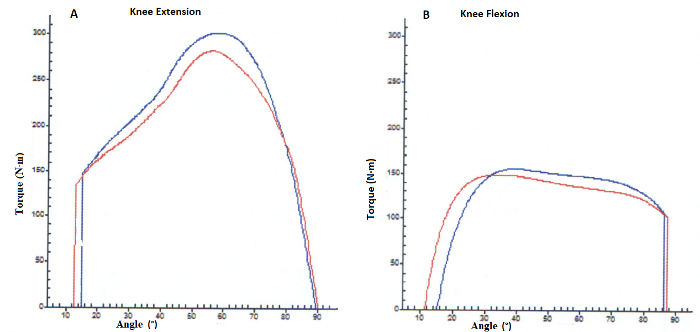
- To determine if the desired speed was accomplished, ensure that the angle-torque curve does not appear to be interrupted (Figure 1).
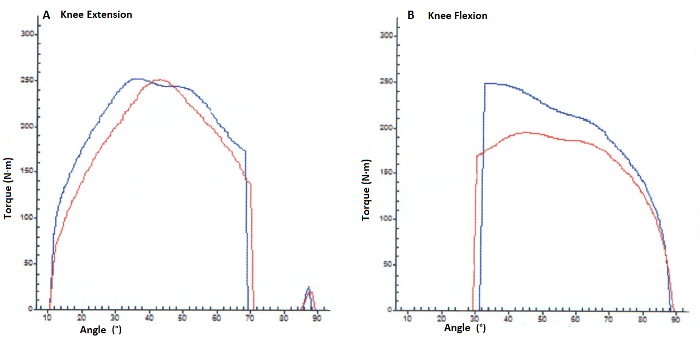
- If the curve looks interrupted (Figure 2), it is likely that the subject did not push or pull against the lever arm fast enough for the dynamometer to register torque. If the subject was not able to reach the required angular velocity and register torque, continue with additional familiarization or exclude the subject from the study and check the possibility of an articular knee lesion23.
2. Isokinetic Strength Measurement After Two Familiarization Visits
Set up the dynamometer's software to perform the tests according to Table 1, and complete the protocol as described in steps 1.3 to 1.7.6.
After the end of the protocol, allow the subject out of the chair and begin analyzing the data.
3. Hamstrings to Quadriceps Functional Ratio Calculation
Use the best peak torque values from all three trials at each given speed and type of muscle action. Insert the peak torque data and resultant ratios into a data organizing software that can graphically depict data such as Microsoft Excel.
Calculate the H/QFUNC60 ratio by dividing the hamstring eccentric peak torque at 60°·s-1 by the quadriceps concentric peak torque at 60°·s-1.
Calculate the H/QFUNC180 ratio by dividing the hamstring eccentric peak torque at 180°·s-1 by the quadriceps concentric peak torque at 180°·s-1.
Calculate the H/QFUNC240 ratio by dividing the hamstring eccentric peak torque at 240°·s-1 by the quadriceps concentric peak torque at 240°·s-1.
- After creating a table similar to Table 2, compare the H/QFUNC ratios across different speeds and between the right and left limbs.
- Compare the measured peak values with normative data of a similar athletic group of the same age and gender.
- Determine if bilateral imbalances are present by comparing the right and left limbs at each tested speed.
- Determine if the ipsilateral H/Qconv ratio at the same speed is above or below 0.624. If the values are below 0.6, the ipsilateral hamstring weakness is present compared to the quadriceps; design a specific hamstring strengthening intervention (Section 4).
- Determine if the ipsilateral H/Qfunc ratio increases along with increased speed and reaches the desired value of 1.012,18, preferably in the speed of 180°·s-1. If the HQfunc does not increase with the increased speed, implement hamstring training to resolve the reciprocal function of the hamstrings (Section 4).
4. Eccentric Hamstring Strength Training Examples
- Consult with a trained exercise professional25, such as Certified Strength and Conditioning Specialist, to select various exercises that target the hamstrings across a variety of muscle lengths, speeds, and movement patterns.
- Consult the exercise professional for advice regarding exercises that improve neuromuscular control during landing and jumping in addition to exercises reported to decrease hamstring injury risk.
- Under the professional's guidance, use complex exercises to strengthen both the hamstrings and quadriceps during "triple extension" exercises where the hips, knees, and ankle simultaneously flex and extend such as the squat, deadlift, and lunge.
- Under the professional's guidance, use exercises such as drop jumps or other repeated jumps to train proprioception in the lower limbs.
Under the professional's guidance, progressively increase the number of sets and repetitions in bodyweight exercises such as the Nordic curl and unilateral hamstring curl on the Swiss ball32, while also progressively increasing the external resistance and decreasing the number of repetitions in complex exercises (for an example, see Table 3).
Representative Results
The examples below show the differences between young elite soccer athletes (age 15.4 ± 0.5 years, body mass 62.7 ± 8.2 kg, height 175 ± 9.1, training experience more than 8 years) performing eccentric hamstring training (EHT, n = 18) and without EHT (n = 15) for 12 weeks (Figure 3). The group performing EHT included this exercise two times per week, while the group without EHT performed core training and a general lower limb program instead. Both groups participated in their program for four months.
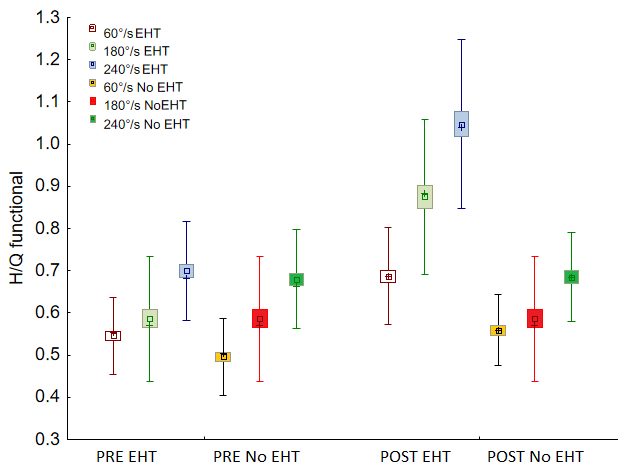
Before the training program, neither group increased their H/Qfunc as the tested speed increased (Figure 3). After 12 weeks of training, EHT players had significantly greater H/Qfunc at each tested speed. Moreover, the EHT group showed increased H/Qfunc between the speeds 60°·s-1, 180°·s-1, and 240°·s-1, while the core training group (without EHT) showed H/Qfunc increase only between the speed 60°·s-1 and 240°·s-1.
Figure 1: Apropriate knee flexors and extensor torque during 10-90° knee flexion range of motion. (A) Torque/angle strength curve for knee extension, (B) torque/angle strength curve for knee flexion. Please click here to view a larger version of this figure.
Figure 2:. Interrupted knee flexors and extensor torque during 10-90° knee flexion range of motion. (A) Torque/angle strength curve for knee extension, (B) torque/angle strength curve for knee flexion. Please click here to view a larger version of this figure.
Figure 3: The representative results of H/Qfunc with and without specific hamstring training. H: hamstrings, Q: quadriceps, EHT: eccentric hamstrings training, PRE: test before specific training, POST: test after 12 weeks specific training. Data are presented as the mean ± standard deviation. The error bars represent the standard deviation.
| Test phase | Task | Rest |
| Pre-test | Gravity correction, set knee flexion to 90°, set range of motion from 90° to 10° (where 0° = full extension) | |
| Trial at 60°·s-1 | Concentric knee extension/flexion 1 repetition | 15 s |
| Test at 60°·s-1 | Concentric knee extension/flexion 3 repetitions | 60 s |
| Trial at 60°·s-1 | Eccentric knee extension/flexion 1 repetition | 15 s |
| Test at 60°·s-1 | Eccentric knee extension/flexion 3 repetitions | 60 s |
| Trial at 180°·s-1 | Concentric knee extension/flexion 1 repetition | 15 s |
| Test at 180°·s-1 | Concentric knee extension/flexion 3 repetitions | 60 s |
| Trial at 180°·s-1 | Eccentric knee extension/flexion 1 repetition | 15 s |
| Test at 180°·s-1 | Eccentric knee extension/flexion 3 repetitions | 60 s |
| Trial at 240°·s-1 | Concentric knee extension/flexion 1 repetition | 15 s |
| Test at 240°·s-1 | Concentric knee extension/flexion 3 repetitions | 60 s |
| Trial at 240°·s-1 | Eccentric knee extension/flexion 1 repetition | 15 s |
| Test at 240°·s-1 | Eccentric knee extension/flexion 3 repetitions | 60 s |
Table 1: Isokinetic testing protocol.
| Right lower limb | Hamstrings peak torque (N∙m) | Quadriceps peak torque (N∙m) | H/Q conventional | H/Q functional |
| 60°·s-1 concentric | 117 | 243 | 0.48 | 0.7 |
| 60°·s-1 eccentric | 171 | 327 | 0.52 | |
| 180°·s-1 concentric | 123 | 168 | 0.73 | 0.95 |
| 180°·s-1 eccentric | 159 | 327 | 0.59 | |
| 240°·s-1 concentric | 98 | 137 | 0.71 | 1.21 |
| 240°·s-1 eccentric | 167 | 297 | 0.56 | |
| Left lower limb | ||||
| 60°·s-1 concentric | 118 | 245 | 0.48 | 0.62 |
| 60°·s-1 eccentric | 152 | 282 | 0.54 | |
| 180°·s-1 concentric | 113 | 151 | 0.75 | 0.99 |
| 180°·s-1 eccentric | 149 | 286 | 0.52 | |
| 240°·s-1 concentric | 114 | 134 | 0.85 | 1.14 |
| 240°·s-1 eccentric | 153 | 298 | 0.51 |
Table 2: Organized table with test outcome values. H: hamstrings, Q: quadriceps.
| Week | Sessions per week | Sets | Repetitions |
| 1 | 1 | 1 | 5 |
| 2 | 2 | 2 | 6 |
| 3 | 2 | 3 | 6-8 |
| 4 | 2 | 3 | 8-10 |
| 5 | 3 | 3 | 8-10 |
| 6-12 | 3 | 3 | 12,10,8 |
Table 3: Nordic curl exercise volume progression according to Mjølsnes 32 .
Discussion
The first critical step in the aforementioned protocol is the athlete's familiarization, especially for the eccentric tests. Subjects may have to be familiarized two or three times to ensure reliable data during such isokinetic testing. Furthermore, it may be a good idea to re-familiarize subjects if testing sessions are more than two months apart. The second critical step is properly setting up the athlete in the dynamometer, ensuring that the knee axis is in-line with the axis of the dynamometer; it is also important to note that stronger individuals may push or pull so hard against the lever arm that the seat pad becomes depressed or the knee joint may move slightly forward or backward. These possibilities should be considered during positioning the athlete and during testing. Another critical point is the ability of the athlete to produce maximal torque production at all tested speed conditions and load range data reduction across increasing velocities. The maximal attainable torque is highly dependent on the speed of contraction, meaning that it is crucial to check whether an athlete can generate torque against the lever arm throughout the whole range of motion (ROM) during high-speed protocols (240°·s-1). Along these lines, the load range data should be reduced by eliminating the first and last 10° of measured range of motion22 to avoid artificial spikes in the torque output signal that may occur at the beginning and end of the ROM.
After completing a successful test, it is also important to interpret the data correctly. If the H/Qconv values (e.g., at 60° m∙s-1) are below 0.6, ipsilateral hamstring weakness is present compared to the quadriceps. However, assessing this ratio alone is not enough for predicting a possible hamstring strain or anterior cruciate ligament injury33,34. More important is to assess whether the H/Qfunc ratio increases along with the tested speed. The minimal recommended H/Qfunc increase between different tested speeds is not sufficiently established. However, we are suggesting optimal H/Qfunc increase between the speed of 60°, 180°, and 240°·s-1 from above 0.6, to above 0.8, to above 0.113,18. The H/QFUNC should be also evaluated in relation to specific athlete groups, where uninjured elite sprinters tested at 60°∙s-1 were reported for H/QFUNC 0. 83 ± 0.17 and injured sprinters 0.73 ± 0.1235. Between-leg comparisons may be valuable information as well. For example, a bilateral strength difference greater than 15% (measured in the same speed) is considered to increase an athlete's risk of knee injury36 and a difference over 20% indicates that an athlete is predisposed to injury37. On the other hand, a bilateral deficit less than 10% is not considered a significant imbalance and is interpreted as a target for athletes with previous imbalances or athletes reconditioning after injury2.
Although the presented protocol can be used in many athletic populations, it is possible to adjust the speed and contraction mode for testing untrained or extremely trained subjects. In the event that maximal strength tests are warranted, isometric tests can be performed on a dynamometer as well and can be used in conjunction with dynamic testing38. If the athletes are highly trained or participate in high velocity sports, speeds nearer to 300°·s-1 39 or more may be appropriate. Regardless of the speeds used, the presented method is limited to isokinetic contractions and single joint movements, neither of which happen during sport. However, in a laboratory setting, isokinetic measurements likely provide the most valid and reliable data for assessing concentric and eccentric strength of the knee flexors and extensors22. One alternative method for assessing muscle net force is by calculating it from reactive force40; however, this method is unable to isolate force or torque generated by a specific group of muscles.
If coaches or practitioners are in search of additional data to create global strength measures for different muscle groups, additional measurements can be performed on the muscles of the lower body35,41,42,43,44,45. Together, the H/QFUNC ratio combined with strength measurements of the hip adductors, abductors, and extensors can provide a wealth of data that can be used to monitor the effectiveness of a resistance training program. The future application of this method might be in its combination to other isolated strength measures, specification of compared knee joint angles for specific purposes13, and combination with multijoint movements such as the leg press46 or squat47.
Disclosures
There are no conflicts of interest to report.
Acknowledgments
The authors would like to thankfully acknowledge all of the subjects in the study. Funding sources A research grant from the Czech Science Foundation GACR NO. 16-13750S, PRIMUS/17/MED/5 and UNCE 032 project.
References
- Hughes G, Watkins J. A risk-factor model for anterior cruciate ligament injury. Sports Med. 2006;36(5):411–428. doi: 10.2165/00007256-200636050-00004. [DOI] [PubMed] [Google Scholar]
- Dauty M, Potiron-Josse M, Rochcongar P. Identification of previous hamstring muscle injury by isokinetic concentric and eccentric torque measurement in elite soccer player. Isokinet Exerc Sci. 2003;11(3):139–144. [Google Scholar]
- Lehnert M, Stastny P, Tufano JJ, Stolfa P. Changes in Isokinetic Muscle Strength in Adolescent Soccer Players after 10 Weeks of Pre-Season Training. The Open Sports Sciences Journal. 2017;10:27–36. [Google Scholar]
- Andersen LL, et al. Changes in the human muscle force-velocity relationship in response to resistance training and subsequent detraining. J Appl Physiol. 2005;99(1):87–94. doi: 10.1152/japplphysiol.00091.2005. [DOI] [PubMed] [Google Scholar]
- Lehnert M, et al. Changes in injury risk mechanisms after soccer specific fatigue in male youth soccer players. J Hum Kinet. 2018;62:1–10. doi: 10.1515/hukin-2017-0157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipinska P, Szwarc A. Laboratory tests and game performance of young soccer players. Trends in Sport Sciences. 2016;23(1) [Google Scholar]
- Stania M, et al. The effect of the training with the different combinations of frequency and peak-to-peak vibration displacement of whole-body vibration on the strength of knee flexors and extensors. Biol Sport. 2017;34(2):127. doi: 10.5114/biolsport.2017.64586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehnert M, et al. Training-induced changes in physical performance can be achieved without body mass reduction after eight week of strength and injury prevention oriented programme in volleyball female players. Biol Sport. 2017;34(2):205–213. doi: 10.5114/biolsport.2017.65995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kabaciński J, Murawa M, Fryzowicz A, Dworak LB. A comparison of isokinetic knee strength and power output ratios between female basketball and volleyball players. Human Movement. 2017;18(3):40–45. [Google Scholar]
- Andrade MDS, et al. Isokinetic hamstrings-to-quadriceps peak torque ratio: the influence of sport modality, gender, and angular velocity. J Sports Sci. 2012;30(6):547–553. doi: 10.1080/02640414.2011.644249. [DOI] [PubMed] [Google Scholar]
- Lund-Hanssen H, Gannon J, Engebretsen L, Holen K, Hammer S. Isokinetic muscle performance in healthy female handball players and players with a unilateral anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 1996;6(3):172–175. doi: 10.1111/j.1600-0838.1996.tb00085.x. [DOI] [PubMed] [Google Scholar]
- Coombs R, Garbutt G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med. 2002;1(3):56. [PMC free article] [PubMed] [Google Scholar]
- Aagaard P, Simonsen EB, Magnusson SP, Larsson B, Dyhre-Poulsen P. A new concept for isokinetic hamstring: quadriceps muscle strength ratio. Am J Sports Med. 1998;26(2):231–237. doi: 10.1177/03635465980260021201. [DOI] [PubMed] [Google Scholar]
- Hill AV. The heat of shortening and the dynamic constants of muscle. Proc Roy Soc Lond B Biol Sci. 1938;126(843):136–195. doi: 10.1098/rspb.1949.0019. [DOI] [PubMed] [Google Scholar]
- Hill A. Production and absorption of work by muscle. Science. 1960;131(3404):897–903. doi: 10.1126/science.131.3404.897. [DOI] [PubMed] [Google Scholar]
- Carney KR, Brown LE, Coburn JW, Spiering BA, Bottaro M. Eccentric torque-velocity and power-velocity relationships in men and women. Eur J Sport Sci. 2012;12(2):139–144. [Google Scholar]
- Haeufle D, Günther M, Bayer A, Schmitt S. Hill-type muscle model with serial damping and eccentric force-velocity relation. J Biomech. 2014;47(6):1531–1536. doi: 10.1016/j.jbiomech.2014.02.009. [DOI] [PubMed] [Google Scholar]
- Aagaard P, Simonsen EB, Trolle M, Bangsbo J, Klausen K. Isokinetic hamstring/quadriceps strength ratio: influence from joint angular velocity, gravity correction and contraction mode. Acta Physiologica. 1995;154(4):421–427. doi: 10.1111/j.1748-1716.1995.tb09927.x. [DOI] [PubMed] [Google Scholar]
- Impellizzeri FM, Bizzini M, Rampinini E, Cereda F, Maffiuletti NA. Reliability of isokinetic strength imbalance ratios measured using the Cybex NORM dynamometer. Clin Physiol Funct Imaging. 2008;28(2):113–119. doi: 10.1111/j.1475-097X.2007.00786.x. [DOI] [PubMed] [Google Scholar]
- Alvares JBdAR, et al. Inter-machine reliability of the Biodex and Cybex isokinetic dynamometers for knee flexor/extensor isometric, concentric and eccentric tests. Phys Ther Sport. 2015;16(1):59–65. doi: 10.1016/j.ptsp.2014.04.004. [DOI] [PubMed] [Google Scholar]
- Manoel ME, Harris-Love MO, Danoff JV, Miller TA. Acute effects of static, dynamic, and proprioceptive neuromuscular facilitation stretching on muscle power in women. J Strength Condit Res. 2008;22(5):1528–1534. doi: 10.1519/JSC.0b013e31817b0433. [DOI] [PubMed] [Google Scholar]
- Brown LE. Isokinetics in human performance. Human Kinetics; 2000. [Google Scholar]
- Iacono AD, et al. Isokinetic moment curve abnormalities are associated with articular knee lesions. Biol Sport. 2017. pp. 83–91. [DOI] [PMC free article] [PubMed]
- Hoffman J, Maresh C, Armstrong L. Isokinetic and dynamic constant resistance strength testing: Implications for sport. Physical Therapy Practice. 1992;2:42–53. [Google Scholar]
- Maciaszek J. Muscles training for the stability of the spine. Trends in Sport Sciences. 2017;24(2) [Google Scholar]
- Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Intrinsic risk factors for hamstring injuries among male soccer players: a prospective cohort study. A J Sports Med. 2010;38(6):1147–1153. doi: 10.1177/0363546509358381. [DOI] [PubMed] [Google Scholar]
- Al Attar WSA, Soomro N, Sinclair PJ, Pappas E, Sanders RH. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: A systematic review and meta-analysis. Sports Med. 2017. pp. 1–10. [DOI] [PubMed]
- Wright GA, Delong TH, Gehlsen G. Electromyographic Activity of the Hamstrings During Performance of the Leg Curl, Stiff-Leg Deadlift, and Back Squat Movements. J Strength Condit Res. 1999;13(2):168–174. [Google Scholar]
- Hedayatpour N, Golestani A, Izanloo Z, Meghdadi m. Unilateral leg resistance training improves time to task failure of the contralateral untrained leg. Acta Gymnica. 2017;47(2):72–77. [Google Scholar]
- Ebben WP. Hamstring activation during lower body resistance training exercises. Int J Sports Physiol Perform. 2009;4(1):84–96. doi: 10.1123/ijspp.4.1.84. [DOI] [PubMed] [Google Scholar]
- Vigotsky AD, Harper EN, Ryan DR, Contreras B. Effects of load on good morning kinematics and EMG activity. PeerJ. 2015;3:e708. doi: 10.7717/peerj.708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mjølsnes R, Arnason A, Raastad T, Bahr R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand J Med Sci Sports. 2004;14(5):311–317. doi: 10.1046/j.1600-0838.2003.367.x. [DOI] [PubMed] [Google Scholar]
- Dyk N, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44(7):1789–1795. doi: 10.1177/0363546516632526. [DOI] [PubMed] [Google Scholar]
- Steffen K, et al. Association between lower extremity muscle strength and noncontact ACL injuries. Med Sci Sports Exerc. 2016;48(11):2082–2089. doi: 10.1249/MSS.0000000000001014. [DOI] [PubMed] [Google Scholar]
- Sugiura Y, Saito T, Sakuraba K, Sakuma K, Suzuki E. Strength deficits identified with concentric action of the hip extensors and eccentric action of the hamstrings predispose to hamstring injury in elite sprinters. J Orthop Sports Phys Ther. 2008;38(8):457–464. doi: 10.2519/jospt.2008.2575. [DOI] [PubMed] [Google Scholar]
- Knapik JJ, Bauman CL, Jones BH, Harris JM, Vaughan L. Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. Am J Sports Med. 1991;19(1):76–81. doi: 10.1177/036354659101900113. [DOI] [PubMed] [Google Scholar]
- Fowler N, Reilly T. Assessment of muscle strength assymetry in soccer players. Contemporary ergonomics. 1993. pp. 327–327.
- Worrell TW, Perrin DH. Hamstring muscle injury: the influence of strength, flexibility, warm-up, and fatigue. J Orthop Sports Phys Ther. 1992;16(1):12–18. doi: 10.2519/jospt.1992.16.1.12. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- Hall S. Basic biomechanics. McGraw-Hill Higher Education; 2014. [Google Scholar]
- Stastny P, et al. Hip abductors and thigh muscles strength ratios and their relation to electromyography amplitude during split squat and walking lunge exercises. Acta Gymnica. 2015;45(2):51–59. doi: 10.1515/hukin-2015-0016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stastny P, et al. The Gluteus Medius Vs. Thigh Muscles Strength Ratio and Their Relation to Electromyography Amplitude During a Farmer's Walk Exercise. J Hum Kinet. 2015;45:157–165. doi: 10.1515/hukin-2015-0016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicholas SJ, Tyler TF. Adductor muscle strains in sport. Sports Med. 2002;32(5):339–344. doi: 10.2165/00007256-200232050-00005. [DOI] [PubMed] [Google Scholar]
- Stastny P, Tufano JJ, Golas A, Petr M. Strengthening the Gluteus Medius Using Various Bodyweight and Resistance Exercises. Strength Condit J. 2016;38(3):91–101. doi: 10.1519/SSC.0000000000000221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khayambashi K, Ghoddosi N, Straub RK, Powers CM. Hip Muscle Strength Predicts Noncontact Anterior Cruciate Ligament Injury in Male and Female Athletes: A Prospective Study. Am J Sports Med. 2016;44(2):355–361. doi: 10.1177/0363546515616237. [DOI] [PubMed] [Google Scholar]
- Cordova ML, Ingersoll CD, Kovaleski JE, Knight KL. A comparison of isokinetic and isotonic predictions of a functional task. J Athl Train. 1995;30(4):319–322. [PMC free article] [PubMed] [Google Scholar]
- Gentil P, Del Vecchio FB, Paoli A, Schoenfeld BJ, Bottaro M. Isokinetic dynamometry and 1RM tests produce conflicting results for assessing alterations in muscle strength. J Hum Kinet. 2017;56(1):19–27. doi: 10.1515/hukin-2017-0019. [DOI] [PMC free article] [PubMed] [Google Scholar]