

Abstract
Cochlear implants are highly efficient devices that can restore hearing in subjects with profound hearing loss. Due to improved speech perception outcomes, candidacy criteria have been expanded over the last few decades. This includes patients with substantial residual hearing that benefit from electrical and acoustical stimulation of the same ear, which makes hearing preservation during cochlear implantation an important issue. Electrode impedances and the related issue of energy consumption is another major research field, as progress in this area could pave the way for fully implantable auditory prostheses. To address these issues in a systematic way, adequate animal models are essential. Therefore, the goal of this protocol is to provide an animal model of cochlear implantation, which can be used to address various research questions. Due to its large tympanic bulla, which allows easy surgical access to the inner ear, as well as its hearing range which is relatively similar to the hearing range of humans, the guinea pig is a commonly used species in auditory research. Cochlear implantation in the guinea pig is performed via a retroauricular approach. Through the bullostomy a cochleostomy is drilled and the cochlear implant electrode is inserted into the scala tympani. This electrode can then be used for electrical stimulation, determination of electrode impedances and the measurement of compound action potentials of the auditory nerve. In addition to these applications, cochlear implant electrodes can also be used as drug delivery devices, if a topical delivery of pharmaceutical agents to the cells or fluids of the inner ear is intended.
Keywords: Medicine, Issue 136, Guinea Pig, Cochlear Implantation, Animal Model, Hearing Loss, Electrophysiology, Hearing Preservation
Introduction
More than 500 million people worldwide suffer from hearing loss.1 Impaired hearing has been linked to a higher rate of depression, lower self-esteem and lower feelings of self-worth, which all lead to reduced quality of life.2 While hearing aids are an adequate way to restore sensory function in cases of moderate hearing loss, the most effective treatment modality for patients suffering from profound hearing loss is the cochlear implant (CI). Due to the excellent outcomes with respect to speech perception, candidacy criteria for cochlear implantation now also includes patients who have substantial residual hearing in the low frequency region, but do not benefit from hearing aids.3 Since these patients can use combined electric and acoustic stimulation in the implanted ear, hearing preservation has become a major issue for CI surgeons. During cochlear implantation, an electrode array is inserted into the scala tympani of the cochlea, where it electrically stimulates the auditory nerve.4 The electrode insertion trauma poses a risk to residual hearing and induces fibrosis, which increases electrode impedances and battery consumption of the implant. Thus, models to study pharmaceutical interventions that can reduce the hearing loss and fibrosis caused by the insertion of the electrode are essential.
The guinea pig is a suitable and convenient animal model for CIs, because of the easier and more reproducible surgical access to the inner ear as compared to gerbils, rats or mice.5,6,7,8 Furthermore, the hearing range of this species is relatively comparable to human hearing.9 Larger species like cats or monkeys, which have been used to address specific research questions related to CIs, do not represent a reasonable choice for most CI studies due to both ethical and financial considerations.10,11
In summary, the guinea pig is a reliable and relatively cost-efficient model to evaluate the effects of pharmacological interventions in the setting of cochlear implantation.
Protocol
All animal experiments were approved by the local animal welfare committee and the Austrian Federal Ministry for Science, Research and Economy.
1. Prepare the Equipment and Setup Required for Surgery
Position the surgical microscope, drill, heating plate and pulse oximeter to allow easy and efficient handling during surgery. Check the function of the devices based on the manufacturer's manual. Make sure that the heating plate is set at 38 °C in order to protect the animal from hypothermia during the surgery.
Put on a hood and a mask.
Perform surgical hand disinfection. Wash hands meticulously with soap. Dry hands and then use an alcoholic hand sanitizer to disinfect hands. Put on gloves after the hands are dry.
Prepare the sterilized surgical instruments and the equipment required for cochlear implantation. See the Table of Materials for the surgical instruments and equipment used for guinea pig CI implantation in this protocol.
When compound action potential (CAP) measurements are intended, prepare an approximately 3.5 cm-long piece of Teflon-insulated gold wire by carefully removing parts of the insulation from both ends using a micro forceps (approximately 3 mm from one end and 5 mm from the other end). Prepare a second piece of gold wire (approximately 2.5 cm) with uninsulated ends of approximately 5 mm. Place the prepared wires in alcohol or disinfectant.
2. Anesthesia, Medication and Animal Preparation
Weigh the animal. NOTE: Animals used are female Dunkin-Hartley albino guinea pigs. The weight of the animals used, which are approximately 4-6 weeks old, ranges from 300 to 400 g.
Prepare the anesthetics and medication required for surgery based on the weight of the animal. Prepare 0.72 mL of the anesthetic mixture, consisting of 0.06 mL ketamine (100 mg/mL), 0.18 mL medetomidine (1 mg/mL), 0.12 mL of midazolam (5 mg/mL) and 0.36 mL of fentanyl (50 µg/mL) for surgery on a 400 g guinea pig. See Table 1 for weight-based doses of the anesthetics.
Inject the mixture of ketamine, medetomidine, midazolam and fentanyl subcutaneously to the fat pad in the neck of the animal using a 27 G needle. See Table 1 for weight based doses of the anesthetics. Cover the cage and leave the animal in a quiet place for 10 min before proceeding.
Lubricate the eyes of the animal and keep them lubricated during the whole procedure. Shave the head of the animal, focusing on the retroauricular region to allow for a sufficient surgical access to the bulla.
Position the animal on the heating plate in prone position and make sure that the animal is not in direct contact with the heating plate to prevent thermal burns. Place the pulse oximeter probe on a foot of the animal. Then carefully open the mouth of the animal with a small laryngoscope and clean the entire oral cavity from food rests by using a sucker.
- Keep the mouth of the animal opened with the laryngoscope. Carefully insert a stomach tube into the esophagus of the animal and slowly push it in the direction of the stomach until a resistance is felt.
- Monitor the O2-saturation of the animal to make sure that the stomach tube is not in the trachea. Remove the stomach tube if there is a decrease in O2 saturation and try again after the animal is completely oxygenated.
Inject a mixture of physiological saline, 5% glucose and enrofloxacin into the fat pad in the neck of the animal using a 23 G needle.
Use alcoholic hand sanitizer to disinfect hands again. Put on new clean gloves.
Prepare the surgical field with alternating scrubs of povidone iodine and 70% ethanol and cover the animal. Use self-adhesive drapes or towel clamps to make sure that only the surgical field stays uncovered during the procedure.
Subcutaneously inject 0.1 mL of 2% lidocaine solution into the area of the planned incision for sufficient local anesthesia and position the animal sideways.
Re-dose the animal with ¼ of the initial dose of the anesthetic mixture every 30 min after the first injection to maintain sufficient anesthesia.
3. Cochlear Implantation
Perform an approximately 2-3 cm skin incision 3-5 mm posterior to the pinna using a scalpel. Use bipolar cautery when necessary to minimize bleeding. Note: Anesthetic depth should be confirmed by the lack of pedal withdrawal prior to the first incision. This test should be repeated every 15-20 minutes to monitor anesthetic depth throughout the procedure.
Carefully cut the muscles in the retroauricular area after palpating the auditory bulla using a 15 scalpel or surgical scissors. NOTE: Palpate the auditory bulla as a prominence under the muscles.
Dissect the muscles from the bulla by pushing them gently aside using a raspatory or a cotton bud. Use a retractor to expose the full length of the incision and have unhindered access to the bulla.
Use the tip of a 15 scalpel to drill a hole into the bulla. Carefully rotate the scalpel until the bone is perforated to allow for inspection of the middle ear structures.
Enlarge the bullostomy as needed to make sure that the basal turn of the cochlea and the round window niche can be adequately visualized. Position the head of the animal in an inflected position in order to access these structures. Cover the area of the bullostomy with a small piece of a compress to prevent blood and extracellular fluid from running in to the middle ear. NOTE: The inflected position of the head may obstruct the airway of the animal. Therefore, the oxygen saturation of the animal needs to be checked frequently.
Position the animal in the prone position. Expose the vertex of the animal by performing a rectangular incision and removing the skin. Dissect the periosteum and clean the bone from any other kind of tissue or blood by using a scalpel.
When CAP measurements are intended, finish the preparation of the 3.5 cm teflon insulated gold wire by forming a small hook with a micro forceps at the end of the wire, which has been uninsulated for 3 mm.
When CAP measurements are intended, guide the end of the gold wire, which has been uninsulated for 5 mm, subcutaneously to the vertex through an 18 G peripheral venous catheter using a micro forceps. Use another micro forceps with the other hand to guide the hooked end of the wire carefully in to the middle ear.
When CAP measurements are intended, inflect the head of the animal to visualize the area of the round window niche through the bullostomy. Use the other hand to hook the gold wire to the bony prominence of the round window niche by using a micro forceps.
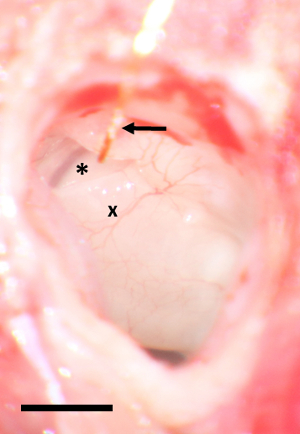
Maintain gentle tension at the gold wire and fix it to the cranial verge of the bullostomy with 10 - 15 µL of tissue glue by using a 1 mL syringe with a 27 G needle. Avoid displacement of glue into the middle ear. See Figure 1 for an intraoperative picture of the round window area with the gold wire in situ.
When CAP measurements are intended, connect the uninsulated end of the gold wire to the equipment used to measure auditory potentials and perform baseline CAP measurements. See Honeder et al., 2016, for a detailed description of the CAP measurements routinely performed in our laboratory.12
Position the animal in prone position. Drill 2 holes 1 mm anterior to the lambda suture using a 1-mm burr without causing damage to the dura. Implant 2 stainless steel screws 2mm into the skull. NOTE: The screws serve as fixation points for the connector of the electrode. Adapt the distance between the screws with respect to the size of the connector.
Use an 18 G peripheral venous catheter to guide the electrode from the connector to the bulla in a tissue layer as close to the skull as possible.
Mix the dental cement powder with the fluid for dental cement powder using a spatula according to the manufacturer's manual.
Place 0.5 - 0.7 mL of semifluid dental cement between the screws by using a spatula. Position the connector of the electrode between the screws.
Keep the connector in position until the dental cement is hardened. Make sure that the screws are encased by the cement to allow for stable fixation of the connector.
Position the animal sideways. Carefully drill the cochleostomy 1 mm from the round window niche using a 0.5 mm diamond burr at a rotation rate of 5000 rounds per minute.
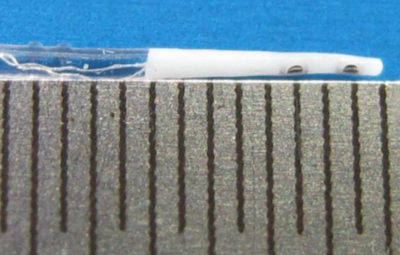
Carefully insert the electrode in to the scala tympani to a depth of 4 mm.Withdraw the electrode and repeat the insertion. See Figure 2 for the electrode used for guinea pig cochlear implantation.
Using a straight needle, seal the cochleostomy area with a small piece of muscle. Fix the electrode to the cranial verge of the bullostomy with 10 µL of tissue glue by using a 1 mL syringe with a 27 G needle.
Prepare the dental cement as mentioned in 3.14. Carefully close the bullostomy with approximately 0.3 mL of dental cement by using a spatula. Close the retroauricular incision using 5-0 absorbable sutures.
Turn the animal to the prone position.
When CAP measurements are intended, grab the posterior edge of the rectangular incision at the vertex of the animal by using a tissue forceps. Use a scissor with the other hand to make a subcutaneous tunnel of approximately 2 cm length in the neck of the animal.
When CAP measurements are intended, implant the 2.5 cm gold wire subcutaneously into the neck of the animal using a forceps. Solder the shorter uninsulated end to the designated pin of the connector on the vertex of the animal.
When CAP measurements are intended, solder the round window niche electrode (gold wire) to the appropriate pin of the connector on the vertex of the animal.
Apply an additional amount of dental cement on the top of the connector to fully cover the insulated pins and the electrode.
When CAP measurements are intended, perform postoperative measurements according to the research protocol.
4. Postoperative Care
Apply atipamezole and flumazenil subcutaneously after the surgery and measurements in order to antagonize the anesthesia.
Apply physiologic saline as fluid substitution to support the recovery of the animal from the surgery.
- Place the animal under a heating lamp until it has fully recovered from anesthesia and starts to move within the cage.
- Prevent hyperthermia or burn by placing the heating lamp approximately 50 cm to the animal. Make sure that the body temperature of the animal is always between 37.5 °C and 39 °C.
Check the animal for symptoms of vestibular injury like nystagmus, circling or rolling over.13,14
Apply buprenorphine for analgesia twice a day for two more days post-surgery. NOTE: Before the first application of buprenorphine post-surgery make sure that the animal has completely recovered and has stable respiration. Application of this medication while the animal is still under anesthesia may lead to respiratory depression.
Weigh the animal during the first 3 days post-surgery to detect possible weight loss as a surrogate marker of distress during this time. NOTE: Weight loss of approximately 10% during the first 3 days post-surgery can be expected and should be considered common. This weight loss is temporary and will recover within a few days.
Representative Results
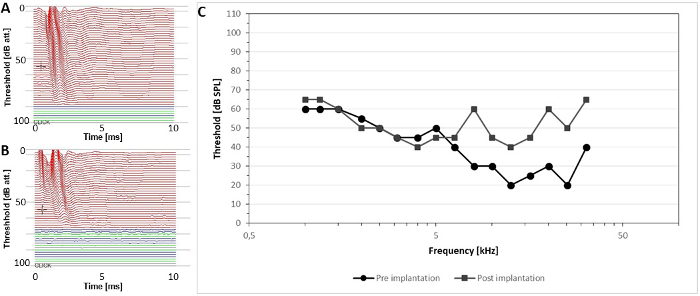
Usually surgical wounds heal fast and without complications in the guinea pig model and the contacts for postoperative electrophysiological measurements remain easily accessible at the vertex of the animal (Figure 3). Figure 4 shows the pre- and postoperative click-CAP measurement of a representative animal. Electrode insertion resulted in a threshold shift of 16 decibels (dB) (Figures 4A and 4B). Figure 4C illustrates the pre- and postoperative frequency-specific CAP thresholds of the same animal. CAP thresholds are almost unchanged in the low frequencies, whereas a threshold shift of approximately 25 to 30 dB is achieved in the high frequency area, starting at 8 kHz.

Electrode insertion can cause trauma to the inner ear. In addition to the acute surgical trauma, the foreign body reaction to the electrode negatively impacts cochlear implant performance. Figure 5 demonstrates the cochleae of guinea pigs after CI insertion and different histological procedures. In Figure 5A the electrode, which is positioned correctly in the scala tympani, was left in situ, whereas in Figure 5B the electrode was removed before histological workup. In Figure 5A almost no foreign body reaction is visible, whereas in Figure 5B a large area of the scala tympani is filled with fibrotic tissue. Figure 5C depicts the fracture of the osseous spiral lamina due to CI electrode insertion, which also caused a loss of spiral ganglion cells in this animal. Such fractures can explain higher than expected threshold shifts in some animals.
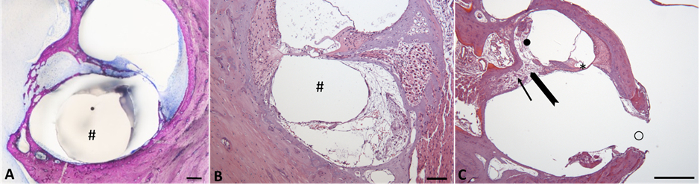
Figure 1: Round window area with gold wire in situ. An asterisk marks the round window, an x the basal turn of the cochlea. The gold wire is marked by an arrow. Scale bar 2 mm. Please click here to view a larger version of this figure.
Figure 2: Guinea pig cochlear implant electrode. The electrode with two contacts is inserted for 4 mm. The diameter of the electrode is tapered from 0.3 mm at the tip to 0.5 mm. Lines indicate 0.5 mm. Please click here to view a larger version of this figure.
Figure 3: Guinea pig approximately two weeks after cochlear implantation. The CI electrode is in situ and the contacts for electrophysiological measurements are easily accessible at the vertex of the animal. Please click here to view a larger version of this figure.
Figure 4: Representative CAP thresholds (A) Preoperative click CAP threshold of a representative animal. (B) Postoperative click CAP threshold of the same animal, exhibiting a threshold shift of 16 dB. Lines indicate 10 dB. (C) Pre- and postoperative frequency-specific CAP thresholds. While low frequencies are almost unchanged, a threshold shift of 25-30 dB can be observed in the frequency range of 8 to 32 kHz. Please click here to view a larger version of this figure.
Figure 5: Potential local consequences of CI electrode insertion. (A) Micrograph of a basal turn of a guinea pig cochlea with the CI electrode in situ (#) and only minimal foreign body reaction. Histological analysis was performed using a grinding and polishing technique after resin embedding and Giemsa staining.15 Scalebar 100 µm (B) Micrograph of the tympanic duct of the upper basal turn of the cochlea with visible tissue response leaving a canal after removal of the CI electrode (#). Scalebar 100 µm (C) Lower basal turn of cochlea with fractured osseous spiral lamina (bold arrow) and adjacent tissue response: (i) loss of spiral ganglion cells (arrow) in Rosenthal`s canal (ii) fibrosis and osteoneogenesis in vestibular duct (●), and (iii) loss of the organ of Corti (*). Drilling-hole for insertion of CI (○) with adjacent osteoneogenesis. Scalebar 500 µm. Figures 5B and 5C were stained with hematoxylin (blue) & eosin (red). Please click here to view a larger version of this figure.
Discussion
The presented protocol describes how to perform cochlear implantation in the guinea pig model. This protocol can be used to evaluate different interventions for their effects on residual hearing and foreign body reaction to the CI electrode. Several precautions should be taken to achieve a high reproducibility and accuracy of the experiments.
Baseline hearing thresholds of all guinea pigs should be measured preoperatively using e.g. auditory brainstem responses. Some of the commercially available guinea pigs exhibit a relevant hearing loss and should therefore not be included in the experimental cohort. Depending on the length of the surgery and protocol this evaluation can be performed either immediately before surgery or a few days before cochlear implantation, giving the animal sufficient time to recover from anesthesia.
When performing surgery under general anesthesia in a spontaneously breathing animal, speed is important. Therefore, meticulous preparation before surgery is essential, as is the choice of the anesthetic protocol. The use of ketamine, medetomidine, midazolam and fentanyl in combination with local anesthesia results in a sufficient anesthesia and analgesia, while at the same time the animal continues to breathe spontaneously. Compared to the often-described use of ketamine and xylazine, this regimen results in better analgesia and reduced perioperative morbidity and mortality. It is important to have all instruments and medications (including a booster of the anesthetics) readily available before putting the animal to sleep.
Due to position changes of the animals during the surgery (changing from prone position to sideward position and back), there is a risk of aspiration of the stomach content in to the lungs. For this reason, the protocol also includes the application of a stomach tube, which is a fast and easy way to protect the animal from aspiration and reduce the perioperative mortality.
To maintain sterility during re-positioning, the areas where the animal is touched need to be covered by sterile drapes, gloves need to be changed thereafter or re-positioning needs to be done by another individual that is not sterile.
O2-saturation monitoring is also of utmost importance during the surgery. The positioning of the head required for visualization of the promontory and round window niche can cause an obstruction of the airway, which can easily be handled when identified early enough.
Usually the animals lose a great amount of body fluids (e.g. blood, extra cellular fluid, urine) during the surgery. Therefore, the fluid substitution protocol introduced in this manuscript represents a well-tolerated method to stabilize the hemodynamics of the animals and supports their fast recovery from anesthesia.
In order to avoid mistakes when performing audiometrical measurements, it is recommended to connect the same pin of the connector to a specific electrode during each surgery.
One limitation of this method is the relatively high variability in postoperative hearing threshold shifts, which often do not correlate well with the surgeon's perception. Even though this variability in outcomes resembles the situation in human CI recipients with residual hearing, it is not fully understood what the causes of the variable results are.16,17,18 In general, the variability decreases with time and the experience of the surgeon. It is important to avoid excessive forces when inserting the electrode, which can be achieved by a slow insertion speed. Because the careful insertion of a CI electrode can result in only very limited hearing loss, the presented protocol describes a repeated insertion of the electrode, which causes a higher and more predictable hearing loss. This hearing loss is most pronounced in the high frequency area, between 16 and 32 kHz. As the intracochlear trauma depends on the insertion depth, the morphology of the cochlea and the approach (cochleostomy versus round window insertion) need to be taken into account. Insertion of the CI electrode through the round window membrane, usually performed in human hearing preservation cochlear implantation, has also been used in the guinea pig model.19 Because the round window membrane is hidden in the guinea pig and electrode insertion through the round window membrane results in an unfavorable insertion angle, drilling a cochleostomy leads to more predictable hearing threshold shifts. This protocol proposes the use of a scalpel instead of a drill for the opening of the tympanic bulla, because this results in a reduced noise exposure of the ear to be implanted. A histological evaluation of the inner ears addressing the foreign body reaction to the electrode, the amount of hair cells and spiral ganglion cells as well as trauma to structures like the osseous spiral lamina and electrode translocation rates should be performed in all implanted ears, as these results facilitate better understanding of the functional results measured.12,20
Disclosures
Christoph Arnoldner and Clemens Honeder are the holders of a research grant from MED-EL Austria. The electrodes used in this publication were provided by MED-EL Austria. The remaining authors have nothing to disclose.
Acknowledgments
The authors want to thank Sandra Peiritsch for the care of the animals and Noelani Peet for medical writing. The financial support by the Austrian Science Fund (FWF grant P 24260-B19) and MED-EL Austria is gratefully acknowledged.
References
- Stevens G, et al. Global and regional hearing impairment prevalence: an analysis of 42 studies in 29 countries. Eur J Public Health. 2013;23(1):146–152. doi: 10.1093/eurpub/ckr176. [DOI] [PubMed] [Google Scholar]
- Ciorba A, Bianchini C, Pelucchi S, Pastore A. The impact of hearing loss on the quality of life of elderly adults. Clin Interv Aging. 2012;7:159–163. doi: 10.2147/CIA.S26059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnoldner C, et al. Electric acoustic stimulation in patients with postlingual severe high-frequency hearing loss: clinical experience. Adv Otorhinolaryngol. 2010;67:116–124. doi: 10.1159/000262603. [DOI] [PubMed] [Google Scholar]
- Kral A, O'Donoghue GM. Profound deafness in childhood. N Engl J Med. 2010;363(15):1438–1450. doi: 10.1056/NEJMra0911225. [DOI] [PubMed] [Google Scholar]
- DeMason C, et al. Electrophysiological properties of cochlear implantation in the gerbil using a flexible array. Ear Hear. 2012;33(4):534–542. doi: 10.1097/AUD.0b013e3182498c28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eshraghi AA, et al. Pattern of hearing loss in a rat model of cochlear implantation trauma. Otol Neurotol. 2005;26(3):442–447. doi: 10.1097/01.mao.0000169791.53201.e1. discussion 447. [DOI] [PubMed] [Google Scholar]
- Mistry N, Nolan LS, Saeed SR, Forge A, Taylor RR. Cochlear implantation in the mouse via the round window: effects of array insertion. Hear Res. 2014;312:81–90. doi: 10.1016/j.heares.2014.03.005. [DOI] [PubMed] [Google Scholar]
- Wysocki J. Topographical anatomy of the guinea pig temporal bone. Hear Res. 2005;199(1-2):103–110. doi: 10.1016/j.heares.2004.08.008. [DOI] [PubMed] [Google Scholar]
- Heffner HE, Heffner RS. Hearing ranges of laboratory animals. J Am Assoc Lab Anim Sci. 2007;46(1):20–22. [PubMed] [Google Scholar]
- Van Beek-King JM, Bhatti PT, Blake D, Crawford J, McKinnon BJ. Silicone-coated thin film array cochlear implantation in a feline model. Otol Neurotol. 2014;35(1):45–49. doi: 10.1097/MAO.0000000000000186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marx M, et al. Cochlear implantation feasibility in rhesus macaque monkey: anatomic and radiologic results. Otol Neurotol. 2013;34(7):76–81. doi: 10.1097/MAO.0b013e31829411b4. [DOI] [PubMed] [Google Scholar]
- Honeder C, et al. Effects of sustained release dexamethasone hydrogels in hearing preservation cochlear implantation. Hear Res. 2016. [DOI] [PubMed]
- Ris L, Capron B, de Waele C, Vidal PP, Godaux E. Dissociations between behavioural recovery and restoration of vestibular activity in the unilabyrinthectomized guinea-pig. J Physiol. 1997;500:509–522. doi: 10.1113/jphysiol.1997.sp022037. (Pt 2) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jin Z, Mannstrom P, Skjonsberg A, Jarlebark L, Ulfendahl M. Auditory function and cochlear morphology in the German waltzing guinea pig. Hear Res. 2006;219(1-2):74–84. doi: 10.1016/j.heares.2006.06.001. [DOI] [PubMed] [Google Scholar]
- Honeder C, et al. Effects of intraoperatively applied glucocorticoid hydrogels on residual hearing and foreign body reaction in a guinea pig model of cochlear implantation. Acta Otolaryngol. 2015;135(4):313–319. doi: 10.3109/00016489.2014.986758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moteki H, et al. Long-term results of hearing preservation cochlear implant surgery in patients with residual low frequency hearing. Acta Otolaryngol. 2017;137(5):516–521. doi: 10.1080/00016489.2016.1252061. [DOI] [PubMed] [Google Scholar]
- Eshraghi AA, et al. Clinical, surgical, and electrical factors impacting residual hearing in cochlear implant surgery. Acta Otolaryngol. 2017;137(4):384–388. doi: 10.1080/00016489.2016.1256499. [DOI] [PubMed] [Google Scholar]
- Reiss LA, et al. Morphological correlates of hearing loss after cochlear implantation and electro-acoustic stimulation in a hearing-impaired Guinea pig model. Hear Res. 2015;327:163–174. doi: 10.1016/j.heares.2015.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang MY, et al. The Effect of Systemic Steroid on Hearing Preservation After Cochlear Implantation via Round Window Approach: A Guinea Pig Model. Otol Neurotol. 2017;38(7):962–969. doi: 10.1097/MAO.0000000000001453. [DOI] [PubMed] [Google Scholar]
- Eshraghi AA, Yang NW, Balkany TJ. Comparative study of cochlear damage with three perimodiolar electrode designs. Laryngoscope. 2003;113(3):415–419. doi: 10.1097/00005537-200303000-00005. [DOI] [PubMed] [Google Scholar]