

Abstract
Background
Intestinal parasitic infections are major public health problems worldwide, with high prevalence in low income countries where substandard food hygiene practices are common. Asymptomatic food handlers with poor personal hygiene could be potential sources of parasitic infections. This study was aimed to assess the prevalence of intestinal parasitic infections and associated factors among asymptomatic food handlers working at Haramaya University cafeterias, eastern Ethiopia.
Methods
A cross-sectional study was conducted among asymptomatic food handlers working at Haramaya University cafeterias from August 2015 to January 2016. Population proportion to size allocation and systematic random sampling techniques were used to identify the study participants. Stool samples were collected and examined simultaneouly using direct and modified formol ether concentration wet smear techniques. Data were entered and analyzed using SPSS version 20.0 software. Logistic regressions were applied to assess association between independent variable and intestinal parasitic infections. Statistical significance was declared at a p-value less than 0.05.
Results
A total of 417 asymptomatic food handlers were enrolled in this study. Of these, females comprised 79.4%. Large proportion (39.3%) of food handlers were in the age group of 31–40 years. The overall prevalence of intestinal parasitic infections was 25.2% (95% CI: 18.3, 29.6). Entamoeba histolytica/ dispar (46.7%) and A. lumbricoides (14.3%) were the most frequent isolates. Having no formal education [AOR: 2.13, 95% CI: 1.24, 3.67], monthly income of less than 45.7 USD [AOR: 3.86, 95% CI: 1.62, 9.20], lack of hand washing after the use of the toilet with soap [AOR: 2.43, 95% CI: 1.22, 4.86] and untrimmed fingernails [AOR: 3.31, 95% CI: 1.99, 5.49] have significant association with intestinal parasitic infections.
Conclusions
The high prevalence of intestinal parasitic infections in this study highlights the importance of food handlers as probable sources of parasitic infections. Public health measures and sanitation programs should be strengthened to control the spread of intestinal parasitic infections.
Keywords: Intestinal protozoa, Helminth, Food handler, Sanitation, University, Cafeteria
Background
Intestinal parasitic infections (IPIs), caused either by intestinal protozoans or helminths or both, remain a major public health problem across the globe, particularly in low income countries due to difficulties in securing optimal hygienic food handling practices [1]. Centers for Disease Control and Prevention (CDC) estimates that each year, 48 million people get sick, 128,000 are hospitalized and 3000 dies from a foodborne disease [2]. Ethiopia has ranked the second highest burden of ascariasis, the third highest burden of hookworm and the fourth highest burden of trichuriasis in Sub-Saharan Africa [3].
The most prevalent intestinal protozoan parasites in Ethiopia are Giardia lamblia and Entamoeba histolytica/ dispar. Helminthic infection includes Ascaris lumbricoides, Trichuris trichuria and Taenia saginata [4, 5]. Many of these intestinal parasites usually cause asymptomatic infections or produce only mild symptoms, leading to difficulties in eradication and control [6].
Asymptomatic food handlers contribute significantly to the spread of infection to susceptible hosts, given that they are unaware of their potential to transmit, and therefore may not be practicing safe food handling [7]. Particularly, foods prepared in large quantities in high risk establishments such as University cafeterias are more liable to contamination when food handlers are shedding egg or cysts of parasite or food is cultivated in faeces-contaminated soils, fertilizer or water, and subsequently lead to outbreaks of food borne diseases [8]. The transmission could be effected from contaminated hand to the food prepared and finally, to healthy individuals through the chain of infection [2].
For the past two decades, Haramaya University (HU) has been experiencing rapid growth in student intake capacity and cafeteria facilities throughout its campuses. This dictates the need to ensure hygienic food handling and preparation practices in such cafeterias to safeguard the health and wellbeing of the customers. Moreover, the burden of IPIs and predisposing factors among food handlers is unknown. This study was designed to assess the prevalence of IPIs and associated factors among asymptomatic food handlers working at HU cafeterias.
Methods
Study design, period and area
A quantitative, cross-sectional study was conducted among asymptomatic food handlers at HU from August 2015 to January 2016. HU is located in East Hararghe zone at a distance of 510 kms from Addis Ababa, 17 kms from Harar town, and almost 5 kms off the main road from the nearby Haramaya town. The University comprises three campuses: Main, Harar and Chiro campus and consists of fifteen cafeterias (9 in Main, 4 in Harar and 2 in Chiro campus). During the study period, 1274 individuals were serving as food handlers throughout HU cafeterias.
Study population
Study population consisted of asymptomatic food handlers working at HU cafeterias.
Inclusion and exclusion criteria
All asymptomatic food handlers who had a direct contact with foods and drinks were included in this study. Those participants who took antiparasitic drugs in the last three weeks or during data collection were excluded.
Sample size determination
The sample size was calculated using single population proportion formula considering 95% confidence level (CL), 5% margin of error, and a 52.4% prevalence of IPIs [9]. An initial sample size was 384. After considering 10% non-response, the final sample size was determined to be 422.
Sampling techniques
Food handlers were stratified into two strata based on the ownership of cafeteria (HU and private cafeteria). Food handlers working at HU cafeterias were further stratified by their working place (Main, Harar and Chiro campus). Food handlers from private cafeterias were also stratified similarly. Then, the sample size was proportionally allocated based on the size of food handlers working in each cafeteria. Finally, a sample size of 422 from a total population size of 1274 was selected using systematic random sampling technique (Fig. 1). A payroll of food handlers was used for sampling frame.
Fig. 1.
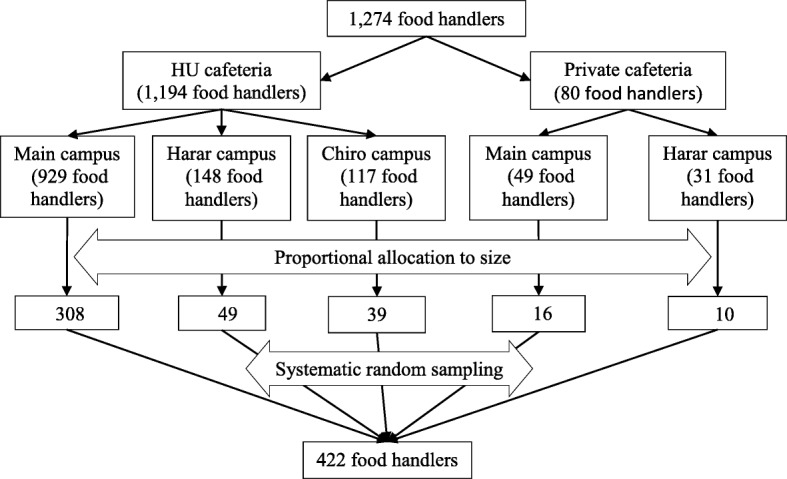
Flow chart showing sampling techniques
Data and specimen collection
Data related to socio-economic factors, food handling practices and other related factors were collected using a pretested structured questionnaire administered by trained nurses. The questionnaire was adopted from the World Health Organization (WHO) food safety checklist and literatures [4, 10, 11]. Data on fingernail trimming was recorded by a simple observation. After interviewing and observation, respondents were asked to bring a small amount of fresh stool sample (2–3 g/pea-size if formed, or 4 ml if watery diarrhea) into a clean, tight-lid sample container after orienting on how to collect the stool specimen by attending laboratory technologist. All specimens were immediately transported using cold box to the Parasitology Laboratory of the College of Health and Medical Sciences of HU for analysis.
Specimen processing and examination
Each stool sample was smeared and tested in triplicate. A saline and Lugol’s direct smears were performed by emulsifying small amount of stool (0.25 mg) uniformly in a drop of normal saline (0.85% NaCl) on one end of a glass slide, and Lugol’s iodine on the other end of the same slide. A saline direct stool smear was used for detection of motility of protozoan trophozoites, which were seen in semisolid/diarrheic specimens. Iodine direct smears showed the characteristic feature of the diagnostic stages in more details. Smear prepared from a sedimented stool was also examined to detect parasites that where too low to be seen in the direct wet smear and exclude false negative result in case of light infections, thus increasing the sensitivity of copromicroscopic techniques. Sedimentation technique was performed using Ridley modified formol ether sedimentation technique. In brief, 1 g of stool was placed in 15 ml conical tube containing 7 ml of 10% formol water, gently emulsified and sieved using 65 mm plastic strainer. The sieved sample was transferred into another conical tube containing 9 ml of 10% formol water and 3 ml of ethyl acetate and centrifuged at 3000 rpm. The supernatant was decanted by inverting the tube and the last drop allowed to sediment by gravity for 15 min. The sediment was then poured on slide, covered with cover glass (22 mm × 22 mm) and examined microscopically under low (10×) with the condenser iris closed sufficiently to give good contrast, and high (40×) objective lenses. Eggs and larvae of helminths, and cysts and trophozoites of protozoan were assessed by propagule size, shape, cell wall width and distinctive internal characteristics [12].
Operational definition
Asymptomatic infections defined by the absence of acute gastrointestinal symptoms such as abdominal discomfort, vomiting, nausea and diarrhea [13].
Food handler is a person performing under contractual agreement or permanent employee who handles, prepares, serves, or sells food and drink, or who comes in contact with eating or cooking utensils or other equipment used in the handling, preparation, service, or sale of food.
Data quality control
The questionnaire was initially prepared in English and translated into the local language (Amharic and Afan Oromo) by language experts and translated back into English by another expert and pretested on 5% asymptomatic food handlers working in Dire Dawa University, Eastern Ethiopia to ensure its consistency. The reliability of the questionnaire was validated using Cronbach’s alpha, and the result was 0.80, indicating a high level of internal consistency [14]. Data collectors and supervisors were trained for two days on method of data collection, specimen collection and examination techniques. The stool specimen examination was conducted in triplicate by trained Medical Parasitologists. The final result was determined through inter-examiners agreement. Moreover, investigators were involved in the decision in case of disagreement. Completion, accuracy and clarity of the collected data were checked every day.
Methods of data analysis
Data were double entered into epidemiological information software (EPI Info™ version 3.5.1) to ensure accuracy of the data. The data were cleaned and exported to statistical package for social sciences (SPSS) software version 20.0 (SPSS Inc., Chicago, IL) for further analysis. Descriptive statistics were calculated for all variables. Bivariate and multivariable logistic regression models were used to assess the association between independent variables and IPIs. Variables that had a p-value < 0.25 in bivariate analysis were run in multivariable logistic regression at 95% CL to determine independent predictors of the outcome. A p-value < 0.05 was considered to indicate statistical significance association.
Results
Participant characteristics
This study included 417 asymptomatic food handlers (331 females and 86 males) with a response rate of 98.9%. The mean age of participants was 36.1 ± 8.7 standard deviation. Large proportion (39.3%) of food handlers were found in the age group of 31–40 years and had formal education (76.3%). Nearly half (47%) of the participants had more than 10 years of work experiences (Table 1).
Table 1.
Characteristics of asymptomatic food handlers working at HU, eastern Ethiopia from August 2015 to January 2016 (n = 417)
| Characteristics | Frequency | % | |
|---|---|---|---|
| Sex | Female | 331 | 79.4 |
| Male | 86 | 20.6 | |
| Age (in year) | > 40 | 145 | 34.8 |
| 31–40 | 165 | 39.3 | |
| 21–30 | 91 | 21.8 | |
| < 21 | 17 | 4.1 | |
| Formal education | No | 99 | 23.7 |
| Yes | 318 | 76.3 | |
| Year of service (in year) | > 10 | 196 | 47.0 |
| 5–10 | 93 | 22.3 | |
| < 5 | 128 | 30.7 | |
| Average monthly income (in USD) | < 45.7 | 291 | 69.8 |
| 45.7–91.3 | 27 | 6.5 | |
| 91.4–137 | 29 | 7.0 | |
| > 137 | 70 | 16.8 | |
| Ownership of cafeteria | Private | 77 | 18.5 |
| HU owned | 340 | 81.5 | |
Prevalence of intestinal parasites
Of 417 stool specimens, 25.2% (95% CI: 18.3, 29.6) were found to be positive for one or more parasite species: comprising protozoa (61%) and helminths (39%). The most prevalent parasite was E. histolytica/ dispar (46.7%) followed by A. lumbricoides (14.3%) and then G. lamblia (13.3%). Less frequent identified intestinal parasite spp. were T. trichuria, Schistosoma mansoni and Dientamoeba fragilis; accounted for 2.9% of the total isolates (Table 2). Mixed intestinal parasites (E. histolotica/dispar, G. lamblia and H. nana) were detected in 2.6% of the participants.
Table 2.
Percent of intestinal parasitic spp. isolated from the stools of the study participants at HU, eastern Ethiopia from August 2015 to January 2016 (n = 105)
| Types of parasitic isolates | Frequency | % |
|---|---|---|
| E. histolytica/ dispar | 49 | 46.7 |
| A. lumbricoides | 15 | 14.3 |
| G. lamblia | 14 | 13.3 |
| H. nana | 11 | 10.4 |
| Hookworms | 8 | 7.6 |
| Taenia species | 5 | 4.7 |
| Others (T. trichuria, S. mansoni, D. fragilis) | 3 | 2.9 |
Factors associated with intestinal parasitic infections
Among the total variables included in the bivariate logistic analysis, ten variables (age, educational status, years of service, monthly income, hand washing after touching body parts, use of the apron when cooking, hand washing after the use of the toilet, fingernail trimming, hand washing before eating foods and medical check-up) were associated with IPIs at a p-value < 0.25. These variables were then computed in a multivariable logistic regression analysis. The results of multivariable logistic analysis showed that not attending formal education [AOR: 2.13, 95% CI: 1.24, 3.67], earning of a monthly income of less than 45.7 USD [AOR: 3.86, 95% CI: 1.62, 9.20], lack of hand washing after the use of the toilet with soap [AOR: 2.43, 95% CI: 1.22, 4.86] and untrimmed fingernails [AOR: 3.31, 95% CI: 1.99, 5.49] were significantly associated with IPIs (Table 3).
Table 3.
Bivariate and multivariable logistic regression analysis on factors associated with IPIs among asymptomatic food handlers at HU, eastern Ethiopia from August 2015 to January 2016
| Characteristics | Negative (%) | Posetive (%) | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|---|
| Sex | Female | 248 (74.9) | 83 (25.1) | 0.97 [0.57, 1.68] 1 |
– |
| Male | 64 (74.4) | 22 (25.6) | |||
| Age (in years) | > 40 | 98 (67.6) | 47 (32.4) | 2.11 [0.54, 7.00] 1.79 [0.97, 3.31] 1.05 [0.57, 1.93] 1 |
1.61 [0.44, 5.88] 1.77 [0.89, 3.51] 0.92 [0.48, 1.79] 1 |
| 31–40 | 131 (79.9) | 33 (20.1) | |||
| 21–30 | 69 (75.8) | 22 (24.2) | |||
| < 21 | 14 (82.2) | 3 (17.6) | |||
| Formal education | No | 63 (63.6) | 36 (36.4) | 2.11 [1.29, 3.43] 1 |
2.13 [1.24, 3.67]* 1 |
| Yes | 249 (78.3) | 69 (21.7) | |||
| Years of service (in years) | > 10 | 136 (69.4) | 60 (30.6) | 2.01 [1.17, 3.47] 1.42 [0.73, 2.73] 1 |
1.66 [0.91, 3.03] 1.57 [0.78, 3.20] 1 |
| 5–10 | 71 (76.3) | 22 (23.7) | |||
| < 5 | 105 (82.0) | 23 (18.0) | |||
| Average monthly income (in USD) | < 45.7 | 205 (70.4) | 86 (29.6) | 3.78 [1.66, 8.58] 3.15 [0.99, 10.07] 1.88 [0.54, 6.48] 1 |
3.86 [1.62, 9.20]* 3.22 [0.91, 11.43] 1.87 [0.50, 6.99] 1 |
| 45.7–91.3 | 20 (74.1) | 7 (25.9) | |||
| 91.4–137 | 24 (82.8) | 5 (17.2) | |||
| > 137 | 63 (90.0) | 7 (10.0) | |||
| Ownership of cafeteria | Private | 61 (79.2) | 16 (20.8) | 0.74 [0.41, 1.35] | – |
| HU | 251 (73.8) | 89 (26.2) | |||
| Hand washing before food preparing with a soap | No | 79 (71.2) | 32 (28.8) | 1.29 [0.79, 2.11] 1 |
– |
| Yes | 233 (76.1) | 73 (23.9) | |||
| Hand washing after touching body parts | No | 150 (70.4) | 63 (29.6) | 1.62 [1.03, 2.54] 1 |
1.33 [0.81, 2.18] 1 |
| Yes | 162 (79.4) | 42 (20.6) | |||
| Use of apron when handling food | No | 109 (69.9) | 47 (30.1) | 1.51 [0.96, 2.37] 1 |
1.37 [0.83, 2.27] 1 |
| Yes | 203 (77.8) | 58 (22.2) | |||
| Hand washing after toilet with a soap | No | 231 (71.5) | 92 (28.5) | 2.48 [1.32, 4.68] 1 |
2.43 [1.22, 4.86] * 1 |
| Yes | 81 (86.2) | 13 (13.8) | |||
| Fingernail trimming | No | 81 (58.7) | 57 (41.3) | 3.39 [2.14, 5.36] 1 |
3.31 [1.99, 5.49] * 1 |
| Yes | 231 (82.8) | 48 (17.2) | |||
| Hand washing before eating food with a soap | No | 75 (72.8) | 28 (27.2) | 0.59 [0.69, 1.90] 1 |
– |
| Yes | 237 (75.5) | 77 (24.5) | |||
| Medical check-up (in the last 6 months) | No | 223 (72.6) | 84 (27.4) | 1.59 [0.93, 2.73] 1 |
1.43 [0.79, 2.57] 1 |
| Yes | 89 (80.9) | 21 (19.1) | |||
| Food safety training | No | 219 (74.7) | 74 (25.3) | 1.10 [0.62, 1.64] 1 |
– |
| Yes | 93 (75.0) | 31 (25.0) | |||
Note: *P < 0.05, COR Crude odds ratio, AOR Adjusted odds ratio, CI Confidence interval
Discussion
The prevalence of IPIs in the present study was 25.2%. The finding was in agreement with a study report (25%) from Gonder University, Ethiopia [15], lower compared to previous studies conducted elsewhere in Ethiopia: Bahir Dar town (41.1%) [16], Yebu town (44.1%) [17], Addis Ababa (45.3%) [5] and Mekelle (52.4%) [9], but higher than a report (10.3%) in Sai-Yok, Thailand [18]. The existence of such variations may be explained by the differences in practices of personal hygiene, environmental sanitation, health promotion practices, geographical location and type of diagnostic sensitivity.
The most frequently isolated intestinal parasite in this study was E. histolytica/ dispar (46.7%). The finding was in line with two studies (32.3%) [9] and (36.6%) [10] conducted in different time period in Mekelle University, Ethiopia. But, it was in disagreement with a study report in Gonder University [15], in which G. lamblia (11%) was most predominantly isolated. The variations in the frequency and type of parasites might be due to differences in sample size (small sample size might overestimate the proportion), geographical location and environmental conditions.
The odds of being positive for atleast one IPIs was two times higher among food handlers who had no formal education than those who attended formal eduaction. This was supported by studies conducted elsewhere in Ethiopia [15, 19]. This may be explained in terms of lack of knowledge that made food handlers unaware of food safety guidelines and hence, may have reduced their understanding of the risks of parasitic contamination as well as protocols to mitigate these risks.
In this study, the odds of being infected with IPIs was four fold higher among food handlers who earned a monthly income of < 45.7 USD than those who earned > 134.0 USD. Similar findings were documented in other studies [19, 20]. The effect of low income on risk of parasitic infections is complex in nature and could be attributed to the sources of drinking water and food, environment sanitation, access to education and living conditions of individuals [21].
Food handlers who did not wash their hands after the use of the toilet had two time higher odds having IPIs compared to food handlers who did. This was supported by another study [10]. Not washing hands after the use of the toilet might have been affected by the availability of sanitary materials, level of education and lack of personal hygiene training, which highlight the need for future sanitation interventions. Conversely, lack of apron uses during food preparation, hand washing before food preparation, hand washing after touching body parts and lack of hand washing before eating food with a soap were not statistically associated with IPIs. These could be influenced by social desirability bias.
The odds IPIs was three fold higher among food handlars who had untrimmed fingernails compared to those who trimmed fingernails. Other studies have also shown untrimmed fingernails to be a determinant for IPIs among food handlers [17, 19]. Untrimmed fingernails could serve as a vehicle for transport of organisms from the source to the food due to the area beneath a fingernail harbors most organisms and is difficult to clean [22]. However, the present study did not attempt to assess the parasite carriage of the fingernail contents.
There were some limitations in this study. Firstly, the fingernail contents examination was not performed for ova/cyst of parasites. Examination of fingernail contents is one way to indicate cross-contamination and transferring of parasites from infected food handlers to actual food, and then to healthy individuals. Social desirability bias, which may cause weak association of hand washing habits with IPIs is another concern. In spite of these limitations, the use of sensitive diagnostic techniques and combination of methods with triplicate examination applied in this study would help to recover greater rate of intestinal parasites that would indicate the ‘true prevalence’.
Conclusion
The prevalence of IPIs in this study is high. E. histolytica/dispar and G. lamblia are the most prevalent intestinal parasites. Not attending formal education, low monthly income, lack of hand washing after the use of the toilet with soap and untrimmed fingernails are independent predictors of IPIs. Preventive programs on awareness of the infectious diseases, improving hygiene and environmental sanitation should be strengthened to reduce IPIs. Large scale longitudinal study is recommended to robustly capture the burden of IPIs and its health effect on food handlers and customers.
Acknowledgements
This research work was financed by the Haramaya University, which is gratefully acknowledged. We are also sincerely grateful to all study participants.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- AOR
Adjusted Odds Ratio
- CDC
Centers for Disease Control and Prevention
- CL
Confidence Level
- COR
Crude Odds Ratio
- HU
Haramaya University
- IPIs
Intestinal Parasitic Infections
- WHO
World Health Organization
Authors’ contributions
DM, KH and MT: participated from conception of research questions to laboratory sample analysis, statistical analysis, preparation and reviewing of the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethical clearance was obtained from Institutional Health Research Ethics Review Committee of the Haramaya University. Signed consent was obtained from the participants. Infected individuals were treated freely based on their laboratory findings according to national standard treatment guideline.
Consent for publication
Not applicable.
Competing interests
All the authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Dadi Marami, Email: dmarami4@gmail.com.
Konjit Hailu, Email: konjit27@gmail.com.
Moti Tolera, Email: motitolera@gmail.com.
References
- 1.World Health Organisation (WHO). Prevention and control of intestinal parasitic infections. Geneva: World Health Organisation; 1987. p. 7-18. [cited 2018 August 05]. Available from: http://www.who.int/neglected_diseases/resources/who_trs_749/en/.
- 2.Centers for Disease Control and Prevention (CDC). Foodborne illnesses and germs. [cited 2018 May 25]. Available from: https://www.cdc.gov/foodsafety/foodborne-germs.html.
- 3.Hotez P, Fenwick A, Savioli L, Molyneux D. Rescuing the “bottom billion” through neglected tropical disease control. Lancet. 2009;373:1570–1576. doi: 10.1016/S0140-6736(09)60233-6. [DOI] [PubMed] [Google Scholar]
- 4.Girma H, Getenet B, Zeleke M. Prevalence of intestinal parasites among food handlers at cafeteria of Jimma University specialized hospital, Southwest Ethiopia. Asian Pac J Trop Dis. 2017;7(8):930–933. doi: 10.12980/apjtd.7.2017D7-20. [DOI] [Google Scholar]
- 5.Aklilu A, Kahase D, Dessalegn M, Tarekegn N, Gebremichael S, Zenebe S, Desta K, Mulugeta G, Mamuye Y, Mama M. Prevalence of intestinal parasites, salmonella and shigella among apparently health food handlers of Addis Ababa university student’s cafeteria, Addis Ababa. Ethiopia BMC Res Notes. 2015;8(1):4–9. doi: 10.1186/s13104-015-0972-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization (WHO). Prevention and control of intestinal parasitic infections. [Technical report series no. 749]. Geneva: 1987. [PubMed]
- 7.Anjum W, Kalasker P, Bhaskar K. Prevalence of intestinal parasites and its associated socio-demographic factors among the food handlers of Bagalkot city, Karnataka, India. Int J Community Med Public Heal. 2017;44(1):1–4. [Google Scholar]
- 8.Charles R. Mass catering. 70 Seiten, 8 Abb. World Health Organization regional publications, European series no. 15, Copenhagen 1983, Preis: 13,- SFr.
- 9.Gebreyesus A, Adane K, Negash L, Asmelash T, Belay S, Alemu M, Saravanan M. Prevalence of Salmonella typhi and intestinal parasites among food handlers in Mekelle University student cafeteria, Mekelle. Ethiopia Food Control. 2014;44:45–48. doi: 10.1016/j.foodcont.2014.03.040. [DOI] [Google Scholar]
- 10.Nigusse D, Kumie A. Food hygiene practices and prevalence of intestinal parasites among food handlers working in Mekelle University students cafeteria. Mekelle GARJSS. 2012;1(4):65–71. [Google Scholar]
- 11.World Health Organization (WHO). Food safety and HACCP checklist. Geneva: World Health Organization. [cited 2015 May 15]. Available from: https://ncfreshproducesafety.ces.ncsu.edu/wp-content/uploads/2014/03/SOPcklistHACCP.pdf?fwd=no.
- 12.Cheesbrough M. District Laboratory Practice in Tropical Countries, part 2. New York: Cambridge University Press; 2006.
- 13.Garzon M, Pereira-da-Silva L, Seixas J, Papoila A, Alves M, Ferreira F, Reis A. Association of enteric parasitic infections with intestinal inflammation and permeability in asymptomatic infants of Sao Tome Island. Pathog Glob Heal. 2017;111(3):116–127. doi: 10.1080/20477724.2017.1299831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Taber K. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Edu. 2017:1–24.
- 15.Dagnew M, Tiruneh M, Moges F, Tekeste Z. Survey of nasal carriage of Staphylococcus aureus and intestinal parasites among food handlers working at Gondar University, Northwest Ethiopia. BMC Public Health. 2012;12(837). 10.1186/1471-2458-12-837. [DOI] [PMC free article] [PubMed]
- 16.Bayeh A, Fantahun B, Bezabih B. Prevalence of Salmonella typhi and intestinal parasites among food handlers in Bahir Dar town. Northwest Ethiopia Ethiop J Heal Dev. 2010;24(1):46–50. [Google Scholar]
- 17.Tefera T, Mebrie G. Prevalence and predictors of intestinal parasites among food handlers in Yebu town. Southwest Ethiopia PLoS One. 2014;9(10):e110621. doi: 10.1371/journal.pone.0110621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kusolsuk T, Maipanich W, Nuamtanong S, Pubampen S, Sa-nguankiat S, Rojekittikhun W, Lekkla A, Tunyong W, Chettanadee S, Komalamisra C. Parasitic and enteric bacterial infections among food handlers in tourist-area restaurants and educational-institution cafeterias, Sai-yok district, Kanchanaburi province. Thailand Trop Med Parasitol. 2011;34(2):49–53. [Google Scholar]
- 19.Gezehegn D, Abay M, Tetemke D, Zelalem H, Teklay H, Baraki Z, Medhin G. Prevalence and factors associated with intestinal parasites among food handlers of food and drinking establishments in Aksum town. Northern Ethiopia BMC Public Health. 2017;17(1):819. doi: 10.1186/s12889-017-4831-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tessema A, Gelaye K, Chercos D. Factors affecting food handling Practices among food handlers of Dangila town food and drink. BMC Public Health. 2014;14(1). 10.1186/1471-2458-14-571. [DOI] [PMC free article] [PubMed]
- 21.Forson A, Arthur I, Ayeh-Kumi P. The role of family size, employment and education of parents in the prevalence of intestinal parasitic infections in school children in Accra. PLoS One. 2018;13(2):1–10. doi: 10.1371/journal.pone.0192303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lin C, Wu F, Kim H, Doyle M, Michael B, Williams L. A comparison of hand washing techniques to remove Escherichia coli and caliciviruses under natural or artificial fingernails. J Food Prot. 2003;66:2296–2301. doi: 10.4315/0362-028X-66.12.2296. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article [and its supplementary information files].