

Abstract
Aim:
The aim of this study was to compare the rate of canine retraction, the anchorage loss, and the change in the inclination of the first molars between molar and mini-implant anchorage.
Objective:
(1) To compare the rate of canine retraction between conventional molar anchorage and mini-implant anchorage in the maxilla and mandible. (2) To compare the amount of anchor loss between mini-implant-anchored and molar-anchored sides during canine retraction in the maxilla and mandible.
Materials and Methods:
Ten patients were included in the study. The implants were loaded immediately by applying a force of 100 g. Measurements were made in the pre-retraction and post-retraction lateral cephalograms. A line drawn vertically from the sella-nasion plane through the distal pterygomaxillary point was used as a reference line.
Results:
The mean rates of canine retraction were 0.95 and 0.82 mm/month in maxilla on the implant and molar sides, respectively, and were 0.81 and 0.76 mm/month in mandible on the implant and molar sides, respectively. The mean anchorage loss was 0.1 mm on the implant side and 1.3 mm on the molar side of the maxilla and 0.06 mm on the implant side and 1.3 mm on the molar side of the mandible. The mean change in molar inclination was 0.3° on implant side and 2.45° on molar side of the maxilla and was 0.19° on implant side and 2.69° on molar side of the mandible.
Conclusions:
Implant anchorage is an efficient alternative to molar anchorage.
Keywords: Anchorage, canine retraction, mini-implant
Introduction
The goal of any orthodontic treatment is to achieve the desired tooth movement with minimal side effects. Proffit and Fields[1] define the anchorage as the resistance to unwanted tooth movement. In planning the biomechanical aspects of orthodontic treatment for a specific patient, it is imperative that the orthodontist considers not only the forces required for the necessary tooth movement to achieve the patient's objectives but also the undesired tooth movement that may occur in response to these forces. Anchorage has long been one of the greatest problems in the field of orthodontics because teeth, even molars, move in response to orthodontic forces.[2]
Implant anchorage has burst onto the clinical orthodontic scene to assist the orthodontists in controlling tooth movement. The primary advantage is that implants provide absolute anchorage, which is undoubtedly a more predictable and stable than method requiring patient compliance. Various authors[3] have suggested temporary anchorage for tooth movements that could not otherwise be achieved, such as in patients with insufficient number of teeth for the application of conventional anchorage, where the forces on the reactive unit would generate adverse side effects, in patients with a need for asymmetrical tooth movements in all planes of space, and as an alternative to orthognathic surgery.
Even though temporary anchorage devices (TADs) have been utilized for conserving anchorage, the exact amount of anchor loss produced along with its use has not been studied extensively. Therefore, the purpose of this in vivo study is to evaluate and compare the amount of anchor loss produced by conventional and TAD-supported canine retraction. This study also compared the rate of canine retraction between the two groups. The results of the study can help prove whether TADs can be more efficient alternative for orthodontic space closure.
In this study, a split-mouth design was used having the advantage of removing patient-related bias such as bone morphology and physiology. Since en mass retraction is not supported by a split-mouth design, canine retraction was evaluated. Five of them received TADs and five of them served as control.
This study was to test the hypothesis that the use of mini-implants as a source of anchorage for canine retraction can be an efficient alternative to conventional molar anchorage and to compare the rate of canine retraction and anchorage loss.
Materials and Methods
Ten patients who reported to the Department of Orthodontics, SRM Dental College, Chennai, India, for orthodontic treatment who fulfilled the inclusion criteria were included in the study after obtaining informed consent. The study design was reviewed and approved by the Institutional Review Board (SRMU/M and HS/SRMDC/2011/101). The patients selected had a mean age of 17.3 years (range: 13–22 years), of which six were females and four were males.
The inclusion criteria are as follows:
Cases requiring therapeutic extraction of first premolars as a part of fixed orthodontic treatment
Patients with Angle's Class I malocclusion and ANB between 2° and 4° were selected for implant placement in both maxilla and mandible
Patients with Angle's Class II malocclusion with an ANB between 5° and 7° implant placement were restricted to maxilla as a part of camouflage treatment
Patients requiring maximum anchorage, with 75%–100% of space closure used for retraction of the anterior segment
Patients treated with 0.022” Roth prescription
Aligning and leveling phase should have been completed
No other anchorage preservation methods were used throughout the study.
Exclusion criteria
Patients with systemic illness
Compromised periodontium
Patients who are allergic to titanium
Missing tooth anterior to the first molars
Local bone pathology as detected in the orthopantomogram.
Methods
All the ten selected patients were treated with preadjusted edgewise appliance system (Roth 0.022” slot). After leveling and aligning was completed with nickel-titanium (NiTi) archwires, a 19” × 25” SS archwire was placed. The titanium mini-implants, Absoanchor (Dentos Inc., Daegu City, Korea), were placed in both maxilla and mandible for eight patients and only in maxilla for two patients. A single-experienced operator placed the implants for all the ten patients using a computer-generated random allocation of sides. All the implants had a diameter of 1.3 mm and were 8 mm in length. The mini-implants were positioned at the maximum thickness of interdental bone between the roots of the second premolar and first molar in the patients' right side. In the maxilla, the mini-implant was inserted at an angle of 30°–40°, and in the mandible, it was inserted at 10°–20° angulation to the long axis of the teeth to increase the surface contact between the mini-implant and the bone [Figure 1].
Figure 1.

Mini implants placed in maxilla and mandible
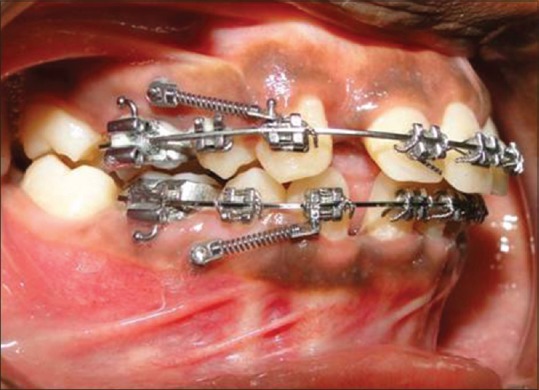
All the implants were loaded immediately. Orthodontic forces were applied with a NiTi-closed coil spring to deliver a force of 100 g (measured with the Dontrix gauge; American Orthodontics) by stretching it between the implant and the canine on the implant-anchored side and between the molar and the canine on the molar-anchored side [Figures 2 and 3]. The period of the study ranged from 4 to 7 months.
Figure 2.

Nickel-titanium closed coil spring stretched between the implant and the canine on the implant-anchored (right) side
Figure 3.
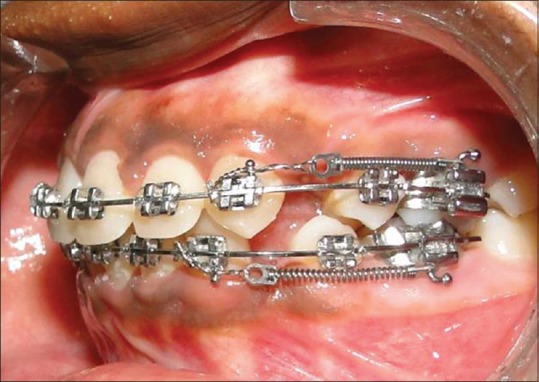
Nickel-titanium closed coil spring stretched between the molar and the canine on the molar-anchored (left) side
Two sets of records were taken; the first was before the implant placement and other when canine retraction was completed in accordance with the patient's treatment plan. Records include (1) study models made from alginate impressions of the maxillary and mandibular dental arches and (2) cephalometric radiographs.
To differentiate the right and left sides on the lateral cephalograms, guides made of 19” × 25” SS wires were placed in the molar buccal tubes and canine brackets. The guides were square shaped on the right side and triangular shaped on the left side. These reference wires prepared for each patient were kept during the investigation period, and the same wires were used for each patient for the other radiographs[4] [Figures 4 and 5].
Figure 4.

Guides placed in canine brackets and molar buccal tubes on the right side
Figure 5.

Guides placed in canine brackets and molar buccal tubes on the left side
Care was taken to make the vertical segment of the guides about the mesial ends of the buccal tubes on molars and distal ends of the canine brackets. The guides were placed at right angles to the occlusal plane. The amount of canine retraction and anchorage loss were measured using a stable landmark in the cranium as a reference. A line drawn vertically from the sella-nasion (SN) plane through the distal pterygomaxillary point was used as a reference line.[4]
The horizontal distance was measured from the reference line to the guide on the canine bracket on both sides at the beginning and end of canine retraction. The amount of canine retraction was calculated by the difference between the preretraction and postretraction values. The rate of canine retraction was calculated by dividing the amount of canine retraction by time is taken for the retraction[5] [Figure 6].
Figure 6.
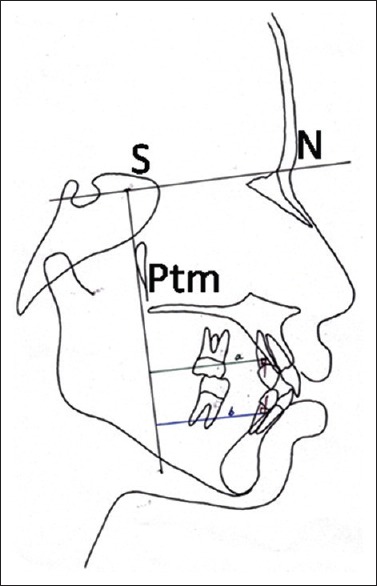
Measurement of the canine position (a - maxilla, b - mandible)
For measuring the amount of anchorage loss, the horizontal distance from the reference line to the guide on the molar buccal tube on both sides was calculated, at the beginning and end of canine retraction.[6] The difference between the two values is the amount of anchorage loss [Figure 7].
Figure 7.
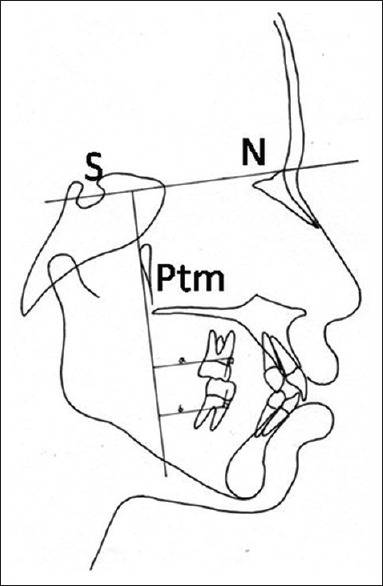
Measurement of the molar position (a - maxilla, b - mandible)
The angle between the long axis of the guide on the molars and SN plane was used to calculate the inclination of the maxillary and mandibular first molars before and after canine retraction[6] [Figure 8].
Figure 8.
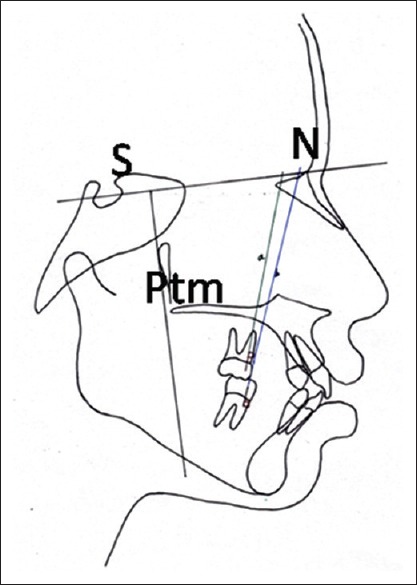
Measurement of the inclination of the first molars (a - maxilla, b - mandible)
Results
As per the objectives of the study, all the canines were retracted successfully on both implant and nonimplant sides in all subjects [Figures 9 and 10]. All the implants remained stable throughout the study.
Figure 9.
Canine retraction completed in the implant-anchored side
Figure 10.

Canine retraction completed in the molar-anchored side
Statistical analysis
The data obtained were entered in the excel sheet and subjected to statistical analysis using SPSS Software version 15.0 (IBM, Armonk, NY, USA). The mean, standard error, and standard deviation were tabulated. The Student's t-test/Mann–Whitney test was used to determine the level of significance.
The amount of anchorage loss in this study ranged from 0 to 2 mm, with a mean of 0.1 mm in implant side and 1.3 mm in molar side in the maxilla. In mandible, anchorage loss ranged from 0 to 2 mm with a mean of 0.6 mm on the implant side and 1.3 mm on the molar side [Table 1]. The difference in anchorage loss between implant and molar side is highly statistically significant P < 0.05 in both maxilla and mandible. The mean amount of distal movement of canines with implant as anchorage was 4.4 mm in maxilla and 3.5 mm in mandible; the mean distal movement of canines with conventional molar anchorage was 4.2 mm in maxilla and 3.5 mm in mandible. Table 2 shows the amount of canine retraction in maxilla and mandible.
Table 1.
Comparison of amount of canine retraction between sides in the maxilla and mandible

Table 2.
Comparison of rate of canine retraction between sides in the maxilla and mandible

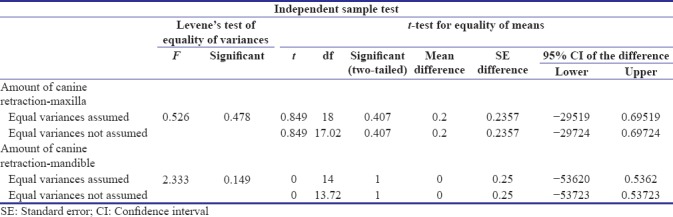
The mean rates of canine retraction were 0.95 mm/month in maxilla and 0.81 mm/month in mandible on the implant-anchored side and were 0.82 mm/month in maxilla and 0.76 mm/month in mandible on the molar-anchored side. The difference in rate of canine retraction was statistically significant (P = 0.012) only in the maxilla. Table 3 shows that mean change in the inclination of molars was 0.3° on the implant-anchored side and 2.45° on the molar-anchored side of the maxilla, whereas the mean change in molar inclination was 0.19° on implant-anchored side and 2.69° on molar-anchored side of the mandible. These values were found to be highly significant both in maxilla (P = 0.000) and mandible (P = 0.001). Independent sample test for the amount of canine retraction in maxilla and mandible at 95% confidence interval is illustrated in Table 4.
Table 3.
Comparison of change of molar inclination in maxilla and mandible
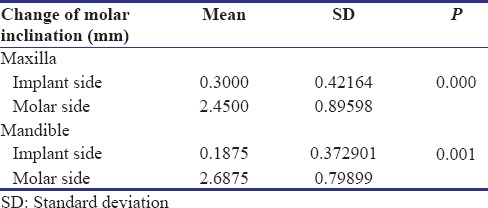
Table 4.
Independent samples test for the amount of canine retraction in maxilla and mandible
Discussion
Successful orthodontic treatment has always required intraoral anchorage with a high resistance to displacement. Typically, orthodontic movement of a tooth is anchored by a large group of teeth so as to minimize undesired displacements of anchoring teeth. Intraoral and extraoral auxiliary devices can be used to prevent unwanted movement, but the effectiveness of these measures is dependent upon the level of patient cooperation.
Storey and Smith[7] have shown that as much as 5%–55% of the total extraction space can be taken up by an anchor unit made up of the first molar and second bicuspid when used for the retraction of a cuspid tooth. Various animal and human studies have shown that immediate loading of orthodontic mini-implants does not affect osseointegration and anchorage potential.[8,9]
Glaucio Serra et al.[10] found that the bone deposition rate was higher in the immediately loaded group than in the unloaded group.
In 2003, Park et al.[11] noted considerably fewer failures when the implants are placed in the areas of attached gingiva rather than movable soft tissue. The best sites for mini-implant placement for retraction are the interdental spaces between the second premolars and first molars.
Relatively few studies have measured the amount of anchorage loss and the rate of canine retraction during canine retraction in humans.
One reason is that it is difficult to find stable landmarks from which to measure tooth movement. In the present study, an attempt was made to overcome this problem using a stable landmark in the cranium as a reference. A line drawn vertically from the SN plane through the distal pterygomaxillary point is used as a reference line.[7]
In our study, the mean rates of canine retraction were 0.95 mm/month in the maxilla and 0.81 mm/month in mandible on the implant-anchored side and were 0.82 mm/month in the maxilla and 0.76 mm/month in mandible on the molar-anchored side.
The difference in the rate of canine retraction was statistically significant in the maxilla. These results were similar to that of another study by Thiruvenkatachari et al.[9]
Anchorage loss in this study ranged from 0 to 2 mm with mean of 0.1 mm on implant side and 1.3 mm on the molar side in the maxilla. In the mandible, anchorage loss ranged from 0 to 2 mm with mean of 0.06 mm on the implant side and 1.3 mm on the molar side. The difference in anchorage loss between implant and molar side is highly significant statistically both in maxilla and mandible.
The results of our study matched the results of another human study by Thiruvenkatachari et al.[6] Upadhyay et al.[10] conducted a study to determine the efficiency of mini-implants as intraoral anchorage units for en masse retraction of the six maxillary anterior teeth. They concluded that mini-implants are efficient for intraoral anchorage reinforcement for en masse retraction and intrusion of the maxillary anterior teeth.
The change in the inclination of molars was 0.3° on the implant-anchored side and 2.45° on the molar-anchored side of the maxilla whereas the change in molar inclination was 0.19° on the implant-anchored side and 2.69° on molar-anchored side of the mandible. These values were highly significant statistically.
Mesial tipping of the first molars was observed in the molar-anchored side both in maxilla and mandible. However, this mesial tipping was not significant in the implant-anchored side. The mesial tipping of the molars can be attributed to the anchorage loss in the molar-anchored side.
In the present clinical trial, the split-mouth study design was used because it offers the advantage of direct comparison between two groups.
Since the implant and molar anchorage were studied in the same subject, the left and right sides were considered to be independent of each other. Hence, a transpalatal arch was not used as it can influence the opposite side since the force on the one side molar may affect the opposite side via transpalatal arch.
The results of the present study showed that mini-implants are an efficient source of anchorage for canine retraction in the maxilla and mandible. Anchorage loss was less and the rate of canine retraction was greater in the implant-anchored side when compared with the molar-anchored side. Mesial tipping of the molar is also less on the implant-anchored side.
In recent years, treatment with orthodontic mini-implants has been added to the existing options for orthodontic therapy. This addition has broken the boundaries of tooth movement possible with conventional fixed appliance therapy. At present, mini-implants are the only available method of absolute intraoral anchorage for all patients.
Mini-implants allow orthodontists to achieve treatment goals that were previously considered extremely difficult, if not impossible. The advent of mini-implants has changed the way treatment strategy is made from anchorage-oriented to problem-oriented diagnosis and treatment planning.
Conclusion
From the present study, it can be concluded that implant anchorage is an efficient alternative to conventional molar anchorage. Mini-implants have provided the clinician with a superior alternative that previously was not possible in orthodontic treatment. Therefore, orthodontic mini-implants can be a powerful aid in resolving challenging malocclusions which require increased anchorage potential.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Proffit WR, Fields HW., Jr . Contemporary Orthodontics. 3rd ed. St. Louis: Mosby Inc; 2000. [Google Scholar]
- 2.Nanda R. Biomechanics and Esthetic Strategies in Clinical Orthodontics. 1st ed. Elsevier Inc; 2005. [Google Scholar]
- 3.Melsen B. Mini-implants: Where are we? J Clin Orthod. 2005;39:539–47. [PubMed] [Google Scholar]
- 4.Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod. 2003;37:321–8. [PubMed] [Google Scholar]
- 5.Onçağ G, Seçkin O, Dinçer B, Arikan F. Osseointegrated implants with pendulum springs for maxillary molar distalization: A cephalometric study. Am J Orthod Dentofacial Orthop. 2007;131:16–26. doi: 10.1016/j.ajodo.2005.02.034. [DOI] [PubMed] [Google Scholar]
- 6.Thiruvenkatachari B, Ammayappan P, Kandaswamy R. Comparison of rate of canine retraction with conventional molar anchorage and titanium implant anchorage. Am J Orthod Dentofacial Orthop. 2008;134:30–5. doi: 10.1016/j.ajodo.2006.05.044. [DOI] [PubMed] [Google Scholar]
- 7.Storey E, Smith R. Force in orthodontics and its relation to tooth movement. Aust J Dent. 1952;56:11–8. [Google Scholar]
- 8.Chen Y, et al. Clinical and histologic analysis of the stability of microimplants with immediate orthodontic loading in dogs. Am J Orthod Dentofacial Orthop. 2009;136:260–7. doi: 10.1016/j.ajodo.2007.10.046. [DOI] [PubMed] [Google Scholar]
- 9.Lisiane, et al. Long-term follow-up of dental single implants under immediate orthodontic load. Angle Orthod. 2010;80:807–811. doi: 10.2319/021010-86.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Serra G, et al. Sequential bone healing of immediately loaded mini-implants: histomorphometric and fluorescence analysis. Am J Orthod Dentofacial Orthop. 2010;137:80–90. doi: 10.1016/j.ajodo.2007.12.035. [DOI] [PubMed] [Google Scholar]
- 11.Park K, et al. Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod. 2003;37:321–8. [PubMed] [Google Scholar]