

Abstract
Objective
To determine whether cardiac mortality is abnormally high on days considered unlucky: Chinese and Japanese people consider the number 4 unlucky, white Americans do not.
Design
Examination of cardiac and non-cardiac mortality on and around the fourth of each month in Chinese and Japanese subjects and white controls.
Setting
United States.
Subjects
All Chinese and Japanese (n=209 908) and white (n=47 328 762) Americans whose computerised death certificates were recorded between the beginning of January 1973 and the end of December 1998.
Main outcome measures
Ratio of observed to expected numbers of deaths on the fourth day of the month (expected number was estimated from mortality on other days of the month).
Results
Cardiac mortality in Chinese and Japanese people peaked on the fourth of the month. The peak was particularly large for deaths from chronic heart disease (ratio of observed to expected deaths = 1.13, 95% confidence interval 1.06 to 1.21) and still larger for deaths from chronic heart disease in California (1.27, 1.15 to 1.39). Within this group, inpatients showed a particularly large peak on the fourth day(1.45, 1.19 to 1.81). The peak was not followed by a compensatory drop in number of deaths. White controls, matched on age, sex, marital status, hospital status, location, and cause of death, showed no similar peak in cardiac mortality.
Conclusions
Our findings of excess cardiac mortality on “unlucky” days are consistent with the hypothesis that cardiac mortality increases on psychologically stressful occasions. The results are inconsistent with nine other possible explanations for the findings—for example, the fourth day peak does not seem to occur because of changes in the patient's diet, alcohol intake, exercise, or drug regimens.
What is already known on this topic
Laboratory studies show that cardiovascular changes occur after mild psychological stress, but it is unclear whether fatal heart attacks increase after psychological stress
Previous non-laboratory studies were unable to control for physical and medical changes associated with most stressful occasions
What this study adds
Unlike white people, Chinese and Japanese associate the number 4 with death.
Cardiac mortality in Chinese and Japanese Americans peaks on the fourth day of the month, even though this date is not consistently associated with changes in the physical or medical environment
In The Hound of the Baskervilles, Charles Baskerville died from a heart attack induced by stress; this “Baskerville effect” seems to exist in fact as well as in fiction
Introduction
In The Hound of the Baskervilles, by Sir Arthur Conan Doyle,1 Charles Baskerville has a fatal heart attack resulting from extreme psychological stress. Conan Doyle was a doctor as well as an author—was his story based on medical intuition or literary licence? Are fatal heart attacks and stress linked in fact as well as in fiction? Conan Doyle's intuition is consistent with many laboratory studies which show cardiovascular changes after psychological stress.2–4 For ethical reasons, however, only non-fatal stressors can be studied in the laboratory, and one may not be able to generalise beyond these relatively mild stressors to determine whether, in the real world, fatal heart attacks increase immediately after psychological stress.5
One way to circumvent the ethical problems of the laboratory experiment and yet retain some of its rigour is to use a natural experiment—one that looks for psychological effects of a real world event occurring simultaneously in a study group that is stressed by the event and in a control group that is not.6 To separate the effects of psychological factors from physical changes in the environment, the event under study should not coincide with destruction of the physical environment (as in disasters) or with disruption of medical services.7 In addition, the event should occur on several occasions, because it is easier to correct for chance confounding factors when studying recurring events. We found no previous studies of real life stressors linked to fatal events that met all these criteria.3–5,7,8
We approached the problem by identifying a cultural phenomenon with unpleasant associations for one group (Chinese and Japanese) and neutral associations for another (white Americans and Europeans). In Mandarin, Cantonese, and Japanese, the words “death” and “four” are pronounced almost identically.9,10 Extensive participant observation by three of our authors (GCL, KK, and WZ) indicates that the number 4 evokes discomfort and apprehension in some Chinese and Japanese people. Consequently, some Chinese and Japanese hospitals do not list a fourth floor or number any rooms 4.10,11 Mainland Chinese omit the number 4 in designating military aircraft—an omission said to result from the link between “four” and “death.”12 Some Japanese people avoid travel on the fourth of the month, and some Chinese patients are apprehensive about this date (these reports are based on participant observation). Aversion to the number 4 is also evidenced by Chinese and Japanese restaurants, which avoid this number (see below).
If the number 4 evokes superstitious stress in some Chinese and Japanese people, and if Conan Doyle's medical intuition was correct, cardiac mortality in Chinese and Japanese people should peak on the fourth of each month. Conan Doyle indicated that Sir Charles Baskerville was susceptible to a heart attack induced by stress because he had chronic heart disease. If so, deaths from chronic heart disease should show a particularly large peak on the fourth day of the month. Sir Charles's superstitious fear of an avenging, spectral hound was shared and reinforced by his neighbours; similarly, Chinese and Japanese superstitious fears are likely to be stronger where they are reinforced by large Chinese and Japanese populations. Hence, the fourth day peak is likely to be stronger in California, which accounts for 42.6% of the Chinese and Japanese deaths in the United States.
We found evidence that the number 4 was considered unlucky by Chinese and Japanese people and examined whether cardiac deaths peaked on the fourth of the month.
Methods
Firstly, we found evidence for avoidance of the number 4 among Chinese and Japanese Americans. New telephone subscribers in California have some choice of the last four digits in their telephone numbers. We searched the California Yellow Pages (via http://altavista.com) for the telephone numbers of California restaurants listed as Chinese or Japanese and those listed as American and found that the Chinese and Japanese had significantly fewer fours in this last section than expected (observed=366; expected=4748/10 [digits 0-9]=474.8; P<0.0001, binomial test). Restaurants listed as American showed no such pattern (observed=219; expected=2036/10=203.6; P=0.879, binomial test).
Having established this, we examined computerised daily national mortality figures for Chinese and Japanese Americans (n=209 908) and white Americans (n=47 328 762) from 1973 (when daily mortality was first recorded) to 1998 (the latest available data).13,14 Chinese, Japanese, and white people were identified from the racial coding on death certificates. The matching of white controls to Chinese and Japanese cases (see figure ) began in 1989 because, before that date, inpatient status was seldom recorded on California death certificates. Deaths from chronic heart disease are those coded 410-414 in the international classification of diseases, 9th revision.15 We matched deaths for white controls to deaths of Chinese and Japanese people, using state and cause of death, inpatient status, age, sex, and marital status. For each Chinese and Japanese death we randomly selected 12 white controls who matched this deceased person on all of these variables. Twelve matches were selected because it was possible to find at most 12 matches for some of the Chinese or Japanese deaths.
As American Asians use the Gregorian calendar in everyday life, we used the Gregorian calendar, rather than the ceremonial lunar calendar.16 There is no correlation between day of the month in one calendar and in the other, so the effects of day of the month in the two calendars are not confounded.
Because mortality in Americans is slightly higher in the first week of each month,17 we used average daily mortality in the first week (days 1-3, 5-7) to estimate the expected mortality on day 4, given the null hypothesis. Subsidiary analyses using days 1-3 and 5-28 to estimate expected mortality on day 4 yielded estimates nearly identical to those obtained using days 1-3 and 5-7.
We measured the size of the fourth day peak (R) by R=X/(Y/6), where X is the number of deaths on the fourth of the month and Y is the total number of deaths in the rest of the first week of the month. The variance of R was determined from table 3 in Gardner and Altman's Statistics with Confidence.18 As in previous studies,17,19–21 we followed recommendations in Vital Statistics of the United States,22 which justifies calculation of confidence limits for complete population data.
Results
On the fourth of the month, cardiac deaths were significantly more frequent than on any other day of the month, and were 7% higher than the average for the rest of the week (ratio of observed to expected deaths=1.07, 95% confidence interval 1.03 to 1.12). This percentage increase is larger for deaths due to chronic heart disease (13%;1.13, 1.06 to 1.21) and still larger (27%; 1.27, 1.15 to 1.39) for chronic heart deaths in California. We call this mortality peak “the Baskerville effect.”
This effect is not evident in white Americans, nor is it evident in Chinese and Japanese Americans who die from causes other than chronic heart disease (ratio=1.02 (0.99 to1.05) for non-heart diseases; 1.04 (0.98 to 1.09) for heart diseases other than chronic heart disease). Thus, Conan Doyle's medical intuition is confirmed: in our dataset the fourth day peak occurs only in people with pre-existing heart conditions.
Because mortality in America peaks in the first week of the month (data not shown), we used a six day comparison period (days 1-3 and 5-7). In case the Baskerville effect was somehow an artefact of this comparison period, we also did a regression analysis, using days 1-3 and 5-28, to generate a substitute for the six day average. The six day and 27 day approaches always yielded similar ratios and all findings are statistically significant whichever approach is used.
Perhaps the Baskerville effect occurs because superstitious relatives attribute the death to the fourth of the month when it actually occurred on the third. Given this hypothesis, deaths of inpatients should show a small or non-existent peak on the fourth day, because the death dates of inpatients are accurately recorded. However, among California Chinese and Japanese dying from chronic heart disease, more inpatient deaths occurred on the fourth day (1.47, 1.19 to 1.81) than on others (1.16, 0.95 to 1.39) (figure).
Discussion
To assess the effects of psychological stress on cardiac mortality, we identified a recurring occasion which, firstly, induces stress in study groups but not in controls, and, secondly, is not objectively hazardous. We showed that Chinese and Japanese cardiac deaths peak on the fourth of the month. White controls display no such peak. At present, the only explanation consistent with the findings is that psychological stress linked to the number four elicits additional deaths among Chinese and Japanese patients. 
There is no linguistic link in English between the number 13 and death.This may help to explain why white mortality shows no peak on the thirteenth of the month, despite the Chinese and Japanese peak on the fourth.
Alternative explanations
On the fourth of the month, patients might change diets, increase alcohol consumption, refuse medicines, or overstrain themselves. These behavioural changes are much less likely for inpatients, who are closely controlled and monitored, than for others. The large inpatient effect undermines all these explanations.
Perhaps the fourth day peak in inpatient deaths occurs because patients refuse to leave hospital on this unlucky day, thus dying as inpatients rather than outpatients. This “discharge hypothesis” implies a compensatory drop in outpatient deaths on the fourth day, and no such drop was seen.
If the fourth day peak occurred because deaths occurred a day or two earlier than they otherwise would have, then this peak should have been followed immediately by a compensatory drop in deaths. No such drop was seen (figure).
Perhaps the Baskerville effect appears because the study and control groups differ demographically. However, our control group of white subjects matched to each member of the study group on state and cause of death, inpatient status, age, sex, and marital status did not show the Baskerville effect (figure).
It is unlikely that the fourth day is objectively more hazardous than the six days surrounding it because no increased mortality on the fourth was found in white controls.
Conclusion
The debate on whether there are fatal psychosomatic processes is unresolved. The question deserves further investigation using rigorous methods, careful controls, and large samples. The natural experiment presented here seems to have met these criteria, and it has provided a new technique for examining fatal psychosomatic effects.
Our findings are consistent with the scientific literature and with a famous, non-scientific story. The Baskerville effect exists both in fact and in fiction and suggests that Conan Doyle was not only a great writer but a remarkably intuitive physician as well.
Figure.

Extreme psychological stress hastened Charles Baskerville's death
Figure.
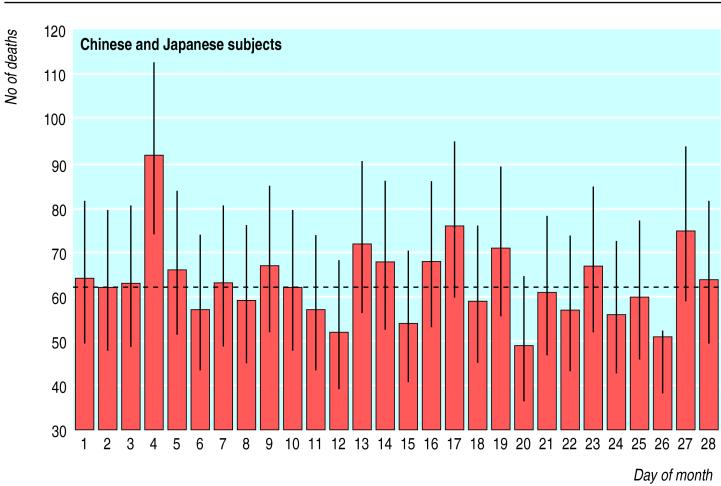
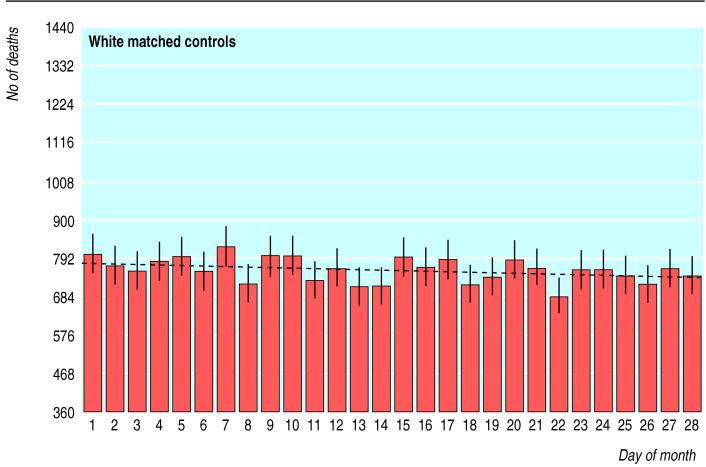
Number of deaths from chronic heart disease, by day of month, in (top) Chinese and Japanese and (bottom) white inpatients (12 matched controls per subject), California, 1989-98 (before 1989, inpatient status was rarely recorded on death certificates in California). Error bars show 95% confidence intervals; dotted line is a regression line fitted to days 1-3 and 5-28
Acknowledgments
We thank Peter H T Liu, Lien-Fen S Chu, Rachel Phillips, Chen Ruzhen, Daniel Smith, Elvira R Strasser, and Li Xianghui for helpful comments.
Footnotes
Funding: This study was supported by a grant from the Marian E Smith Foundation.
Competing interests: None declared.
References
- 1.Doyle AC. The hound of the Baskervilles. London: John Murray; 1964. . (First published 1901-2.) [Google Scholar]
- 2.Soufer R, Bremner JD, Arrighi JA, Cohen I, Zaret BL, Burg MM, et al. Cerebral cortical hyperactivation in response to mental stress in patients with coronary artery disease. Proc Natl Acad Sci USA. 1998;95:6454–6459. doi: 10.1073/pnas.95.11.6454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Krantz DS, Sheps DS, Carney RM, Natelson BH. Effects of mental stress in patients with coronary artery disease. JAMA. 2000;283:1800–1802. doi: 10.1001/jama.283.14.1800. [DOI] [PubMed] [Google Scholar]
- 4.Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation. 1999;99:2192–2217. doi: 10.1161/01.cir.99.16.2192. [DOI] [PubMed] [Google Scholar]
- 5.Steptoe A, Vogele C. Methodology of mental stress testing in cardiovascular research. Circulation. 1991;83(suppl 2):14–24. [PubMed] [Google Scholar]
- 6.Phillips DP, Glynn L. Field studies. In: Kazdin AE, editor. Encyclopedia of psychology. Oxford: Oxford University Press; 2000. [Google Scholar]
- 7.Phillips DP, Halebsky SC. The epidemiology of found experiments. JAMA. 1995;273:1221. [PubMed] [Google Scholar]
- 8.Witte DR, Bots ML, Hoes AW, Grobbee DE. Cardiovascular mortality in Dutch men during 1996 European football championship: longitudinal population study. BMJ. 2000;321:1552–1554. doi: 10.1136/bmj.321.7276.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Min su shu zi de bing tai yu lao fa [Popular morbid beliefs in numbers and their alleviation]. www.fgs.org.tw/library/3-1/3-1-D-19.htm (accessed 19 Apr 2000).
- 10. Schauwecker's guide to Japan: superstition. www.japan-guide.com/e/e2209.html (accessed 7 Dec 2000).
- 11.Chungshan Hospital. [Visitor' brochure.] Taipei: The Hospital, [nd]. (Available from authors.)
- 12.Subject H11, Chinese aircraft designations. rec.aviation.military FAQ, Part 5. www.hazegray.org/faq/ram5.htm (accessed 14 Oct 2001).
- 13.Mortality detail file. Hyattsville, MD: US National Center for Health Statistics (computer data file).
- 14.Mortality file. Sacramento, CA: California Department of Health Services (computer data file).
- 15.National Center for Health Statistics. Vital statistics of the United States, 1994. 2. Mortality. Part A. Washington, DC: Government Printing Office; 1997. [Google Scholar]
- 16.The Western calendar and calendar reforms. www.britannica.com/eb/article?ev=108734 (accessed 8 Dec 2000).
- 17.Phillips DP, Christenfeld N, Ryan NM. An increase in the number of deaths in the United States in the first week of the month. N Engl J Med. 1999;341:93–98. doi: 10.1056/NEJM199907083410206. [DOI] [PubMed] [Google Scholar]
- 18.Gardner MJ, Altman DG, editors. Statistics with confidence. London: British Medical Journal; 1989. [Google Scholar]
- 19.Phillips DP, Ruth TE, Wagner LM. Psychology and survival. Lancet. 1993;342:1142–1145. doi: 10.1016/0140-6736(93)92124-c. [DOI] [PubMed] [Google Scholar]
- 20.Phillips DP, Smith DG. Postponement of death until symbolically meaningful occasions. JAMA. 1990;263:1947–1951. [PubMed] [Google Scholar]
- 21.Phillips DP, King EW. Death takes a holiday: mortality surrounding major social occasions. Lancet. 1988;ii:728–732. doi: 10.1016/s0140-6736(88)90198-5. [DOI] [PubMed] [Google Scholar]
- 22.National Center for Health Statistics. Vital statistics of the United States, 1973-1994. Vol. 2. Mortality. Part A. Technical Appendix. Washington, DC: Government Printing Office, 1976-1997.