

I. Introduction
Aging of populations in low to middle income countries is taking place at an unprecedented speed but under economic, political, and institutional conditions that are in stark contrast with those associated with aging processes in high income countries. This is the case in countries of the Latin American and Caribbean (LAC) region where rapid changes of the fertility and mortality regimes, weakening of familial norms and values, and radical reforms of publicly funded safety nets, is rapidly eroding the foundation of traditional support for the elderly.
In this highly descriptive paper we identify conditions affecting the demand and supply of elderly support in LAC and, for the first time, estimate existing patterns of elderly support in seven countries of LAC using a new and as yet unexplored source of information. The first section introduces basic concepts and terminology. The second section describes unique features of LAC countries that exert large a influence on patterns of intergenerational transfers by constraining the supply of elderly support and expanding the demand for it. In the third section we analyze data on intra-family transfers using a set of surveys of elderly adult living in seven large cities in LAC countries. We focus on two dimensions of elderly support: the availability of actors to provide support and the propensity of these actors to supply support. We show evidence of distinct patterns of family support, the result of different combinations of kin-availability and kin propensities to support. The final section concludes.
II. Intra-family transfers and elderly support
Support for the elderly results from transactions that involve three elements: agents, goods (or materials transacted) and socio-political and socio-cultural contexts. Participating agents are an ‘ego’ , a target elderly person, and ‘alters’ who, for the most part but not always, have close kinship ties to ego. Although to varying degrees the bulk of elderly support involves agents’s close kin such as children, children-in-law and non kin, such as spouses, the public sector through several agencies and programs and private markets may also perform an important role. The currency or materials transacted are generally, albeit not restricted to, money, goods, time supplied in the form of services and assistance, and co-residence (Bianchi et al., 2008). Transactions involving elderly support do not occur in a vacuum but within well-defined socio-political and cultural contexts that determine individual preferences, expectations and rules to effect the transactions. Who participates in the transactions, what is transacted or transferred, the timing of transactions, how much is transacted and for how long, are all matters that depend on two set of characteristics. The first is associated with actors themselves (ego and alter) and includes individual traits such as education, wealth, marital status, gender and health status all of which influence actors’ propensities to engage in transactions. The second set includes characteristics that determine explicit or implicit rules that govern type, timing, and duration of transactions but that emanate from the socio-cultural context and the constraints and possibilities created by the public and private sector (Billari and Liefbroer, 2008).
Three remarks are in order. First, a vexing problem in the study of elderly support is that it is unquestionably part of more general system of intergenerational transfers that stretch over the life time of individuals and involve negotiations and bargaining among two or more generations over extended periods of time. Yet, we are frequently constrained to study transactions that occur over a very short period of time and involve at most two generations. Needless to say, testing theories about the nature of elderly support with this massive observational limitation is a difficult task.
Second, elderly support is frequently drawn from close kin (and non-kin), particularly children, children-in-law, and spouses. Who is involved in the allocation of support, what type of support is supplied, and its duration are not matters decided by single individuals according to their own preferences but rather depend on implicit or explicit bargaining among potential participants in these transactions. For the most part we only observe realized transactions and we rarely, if ever, get a glimpse of the negotiating process between siblings, siblings-in-law and other alters, on the one hand, and the target individuals, on the other, that results in an observed pattern of support, one among many other possible realizations. This is a glaring observational shortcoming that limits our ability to understand the processes of interest.
Third, depending on the residential arrangement itself, nature of household headship and household property ownership rights, coresidence could indeed constitute itself a good transacted . However, it is clearly something more than an additional good since coresidence of elderly and kin augments the opportunity for and reduces the costsm of other transactions. For this reason we do not consider coresidence separately but include it among goods transacted.
Below we identify demographic changes that constrain the supply of kin for elderly support, identify changes in elderly health status and institutional reforms that will increase the demand for elderly care, and argue that shifts in cultural expectations will reduce the propensity of family members and close kin to support the elderly.
III. Conditions that influence the demand and supply of elderly support in LAC
The pressure on traditional regimes of elderly support in LAC originates in past demographic changes, changes in institutions that contract the supply of public support, and new cultural norms and expectations that reduce the propensity of kin and close family members to supply elderly support.
a. Demographic changes: the speed of aging and the contracting supply of kin
Although the demographic regimes experienced by low and middle income countries display significant heterogeneity, there are two common features with large implications for the aging of these societies. The first is that in most cases the period between 1930 and 1970 was characterized by massive mortality declines, the combined product of large public health interventions that succeeded in decreasing exposure to diseases, augmenting resistance (vaccines) and reinforcing the ability to recover (chemotherapy such as antibiotics, sulfa drugs, etc...). The bulk of these changes are concentrated among children younger than 10. The second feature is that the traditional fertility regimes characterized by TFR’s exceeding 5, begin to crumble rapidly after 1975–1980. As a result of these two trends the speed of population aging accelerates with an unprecedented pace: aging begins to occur in a much more compressed period of time that it ever did in high-income countries.
We use four indicators of aging: the fraction of the population above age 60,C(t); the mean age of the population at time t, A(t) ;the rate of growth of the population 60 and over at time t, R(t); and L(t) an indicator of kin availability, the ratio of adult kin who are potentially available to provide care and services to elderly. Although A(t) has been largely ignored in the literature it is a useful metric to understand the underlying demographic dynamics of aging (Preston and Lahiri, 1991; Grushka and Preston, 1995; Horiuchi and Preston, 1988). It correlates highly with more conventional indicators of aging such as the proportion of the population who is over 60. L(t) has been used before with slightly different definitions (Wolf, 1994). Here we compute L(t) as the sum, for all five-year age groups, (x,x+5) above age 60, of the products F(x,t)*W(x,t), where F(x,t) is the ratio of the population in the age group (x-25,x-20) to the population in the age group x,x+5 in year t, and W(x,t) is the fraction of the population 60 and older in the age group x,x+5 in year t. The assumption is that, on average, the children of the elderly are to be found among the population born 25 years before year t (Wolf, 1994). More precise fine-tuning of the measure of generational length introduces only trifle changes in the value of the indicator.
Table 1 displays all four indicators for 1950, 1990 and projected values for 2020. For comparative purposes, the table includes estimates for the US and Japan as well. Figure 1 displays the frequency distributions of C(t), L(t), and A(t) for three years in the time interval between 1950 and 2020.
Table 1:
Values of C(t), R(t), A(t) and L(t) for 1950 – 2020
| 1950 | 1990 | 2020 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C(t) | R(t) | L(t) | A(t) | C(t) | R(t) | L(t) | A(t) | C(t) | R(t) | L(t) | A(t) | |
| Argentina | 7.0 | .11 | 4.95 | 25.5 | 12.9 | .23 | 3.03 | 31.3 | 16.6 | .27 | 2.89 | 35.6 |
| Bolivia | 5.6 | .11 | 4.65 | 24.2 | 5.8 | .11 | 4.34 | 23.9 | 8.9 | .14 | 3.97 | 29.3 |
| Brazil | 4.9 | .09 | 5.16 | 23.5 | 6.7 | .12 | 4.31 | 27.4 | 15.3 | .25 | 3.24 | 35.0 |
| Chile | 6.9 | .12 | 4.52 | 25.4 | 9.0 | .15 | 3.72 | 29.6 | 18.2 | .31 | 2.69 | 36.2 |
| Colombia | 5.6 | .11 | 5.02 | 24.2 | 6.2 | .11 | 4.19 | 26.1 | 9.7 | .23 | 3.28 | 33.4 |
| Costa Rica | 5.7 | .11 | 4.22 | 24.3 | 6.4 | .11 | 4.27 | 26.4 | 14.3 | .22 | 3.09 | 33.8 |
| Cuba | 7.3 | .13 | 4.51 | 25.8 | 11.7 | .18 | 3.30 | 33.1 | 25.0 | .30 | 2.44 | 42.2 |
| Dominican Republic | 5.2 | .10 | 4.59 | 23.8 | 5.6 | .09 | 4.50 | 25.7 | 14.2 | .23 | 3.25 | 34.2 |
| Ecuador | 8.1 | .16 | 3.65 | 26.6 | 6.1 | .11 | 4.16 | 26.9 | 12.6 | .20 | 3.53 | 36.5 |
| El Salvador | 4.8 | .09 | 4.71 | 23.4 | 6.0 | .12 | 3.73 | 24.9 | 10.1 | .16 | 3.88 | 31.7 |
| Guatemala | 4.3 | .08 | 5.19 | 22.9 | 5.1 | .10 | 4.29 | 22.1 | 7.4 | .12 | 4.54 | 27.2 |
| Honduras | 3.9 | .08 | 5.40 | 22.5 | 4.5 | .09 | 4.57 | 22.3 | 8.6 | .14 | 4.17 | 29.4 |
| Mexico | 7.1 | .14 | 3.89 | 25.6 | 5.9 | .11 | 4.21 | 25.4 | 13.5 | .21 | 3.43 | 34.2 |
| Nicaragua | 4.1 | .08 | 5.15 | 22.7 | 4.3 | .09 | 4.61 | 21.7 | 8.4 | .13 | 4.35 | 28.4 |
| Panama | 6.5 | .12 | 4.34 | 25.0 | 7.3 | .14 | 3.89 | 27.1 | 10.5 | .25 | 3.13 | 35.2 |
| Paraguay | 8.9 | .17 | 3.54 | 27.4 | 5.4 | .10 | 4.32 | 24.7 | 9.4 | .16 | 3.79 | 29.9 |
| Peru | 5.7 | .11 | 4.66 | 24.3 | 6.1 | .11 | 4.29 | 27.0 | 12.6 | .20 | 3.56 | 36.8 |
| Uruguay | 11.8 | .20 | 3.37 | 30.2 | 16.5 | .29 | 2.69 | 34.2 | 18.4 | .31 | 2.57 | 37.3 |
| Venezuela | 3.4 | .06 | 7.00 | 22.0 | 5.7 | .10 | 4.61 | 25.6 | 13.2 | .21 | 3.32 | 33.2 |
| Barbados | 8.5 | .15 | 4.06 | 27.0 | 15.3 | .25 | 2.49 | 33.3 | 23.2 | .39 | 2.49 | 41.5 |
| Jamaica | 5.8 | .10 | 5.16 | 24.4 | 9.2 | .16 | 2.87 | 27.6 | 14.9 | .24 | 3.21 | 35.1 |
| Trinidad | 6.1 | .11 | 4.67 | 24.6 | 8.7 | .15 | 3.61 | 29.0 | 17.4 | .28 | 2.91 | 38.7 |
| Puerto Rico | 6.1 | .12 | 4.10 | 24.6 | 13.2 | .23 | 3.06 | 32.7 | 20.5 | .35 | 2.60 | 38.2 |
| United States | 12.5 | .21 | 30.8 | 16.6 | .27 | 35.6 | 24.7 | .44 | 40.6 | |||
| Japan | 7.7 | .24 | 26.2 | 17.4 | .27 | 39.6 | 32.1 | .59 | 46.6 | |||
Sources: Calculation using the United Nations Data Base (1999)
Figure 1:
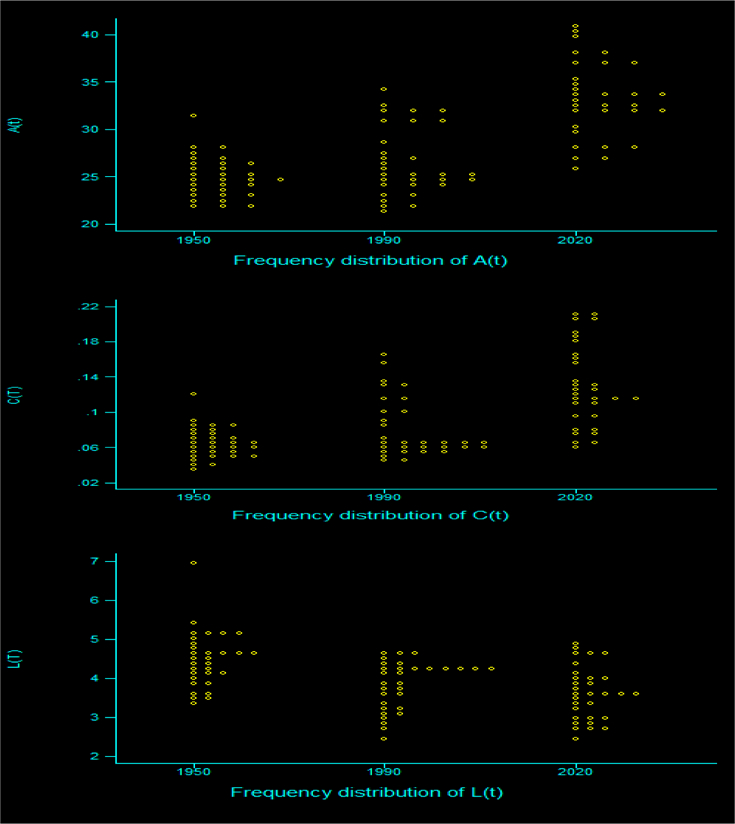
Frequency distribution of A(t), R(t) and L(t) for three years over four decades
Figure 1 reveals the momentum of aging in the region: the modes of all three empirical distributions converge toward values typical of aging societies. Simultaneously, there is an increase in variance, a result of heterogeneous timing of the mortality and fertility transitions in the region. A(t) is highly sensitive to the specific trajectory toward older age distributions: whereas in 1950 most countries in the region attained values below 25 years, by 2020 all of them are expected to exceed 25 years, and most of them will attain values surpassing 30 years. During the period 1990–2020 A(t) will increase on average from 27.2 years to 33.3 years, a rate of increase of about 22 percent. A comparison of trajectories of A(t) in the region with those in the Northern Europe, US and Japan reveals that countries in the region will experience higher rates of changes in A(t) than what would be expected given their absolute values of A(t). Over long periods of time--long enough to cancel out irregularities due to transient phenomena-- the rate of change in A (t) is an indicator of the intrinsic speed of aging in a demographic regime. In LAC countries, where mortality and fertility decline are packed in a few years, the speed of aging is much higher than in areas such as Western Europe and North America, where mortality and fertility decline took place more gradually, over extended periods of time. We show elsewhere (Palloni et al., 2002) that the rate of change in A(t) in LAC is 30 to 50 per cent higher than it was in Europe and North America at an equivalent period in the demographic transitions. The main implication of this feature is somewhat paradoxical: the transition toward an older population in countries of LAC this region is gaining speed when their age distributions are still very young.
L(t) is a telling indicator for it reflects availability of members of younger generations to elderly people. Residential arrangements of the elderly and the quality and quantity of intrafamily transfers toward the elderly are influenced by the magnitude of L(t). During the period 1950–2020 the (unweighted) median value of L(t) in the region drops from about 4.8 to 3.1 while its variance increases, reflecting intercountry demographic heterogeneity. Barring reversals of fertility trends, the value of L(t) will continue its steep decline and will attain levels close to 2.5 or less before 2020. As in the case of other indicators of aging, relatively large changes in L(t) are packed in a short period of time. The declining trend of L(t) is much faster and implies changes of higher magnitudes than the trend in Northern Europe and North America: in the most rapid phase of the transition in these societies L(t) changes from values that do not exceed 3.5 to values around 1.5. Instead, countries of LAC experience more massive changes, as the reduction in the absolute value of L(t) is twice as large, from values around 5 to about 2.5. If future trends conform to projections, the change from levels of L(t) of about 5 to values around 2.5 will occur over a period of time that is nearly half as long as the period of time within which the same transition took in North America and Northern Europe. The differences are striking and suggest that the impact of aging on kin availability in the region will be felt more suddenly than ever before.
b. Demographic regimes and increasing demand for elderly support
Past demographic trends left footprints in the composition of the elderly population by frailty that could be consequential for future demand for health and disability care. The initial acceleration of the process of aging during the period 1990–2020 is, to a large extent, due to the momentum rooted in the mortality decline of the period 1940–1970, unlikely to be malleable or responsive to future policies (Palloni et al, 2002). The nature and timing of the mortality decline will mark the elderly population along two dimensions. First, the initial acceleration of the rate of increase of the elderly population during the period 2000–2020 is almost entirely due to large increases in survival among members of birth cohorts born after 1940. Cohorts that attain their 60th birthday between 2000 and 2020 are the beneficiaries of unusually large improvements in survival, particularly during early childhood, that took place in the absence of significant improvements in standards of living. In fact, one can show that the relatively compressed schedule of the aging process in LAC can be traced to the medical and public health revolution that triggered the mortality decline nearly half a century ago. This legacy of the past has an important implication for the health and disability status of the elderly after the year 2000.
Second, it is well-known that there is a close connection between health and disability conditions at older ages and early life experiences with illnesses, nutritional insufficiency, and deprivations (Barker, 1998). It is then likely that the main beneficiaries of the secular mortality decline, the birth cohorts who enter older ages after the year 2000 and perhaps until 2020, will be marked by higher risks of some chronic conditions and disability than it was the case among elderly in high income countries at similar stages of the aging process (Palloni et al., 2002)
The effects of these two dimension of LAC aging will only be augmented by an unusual characteristic of the epidemiological regimes in the region, namely, one with an unprecedented coexistence between modern chronic conditions and sustained high prevalence of infectious diseases.
In summary, the demography of the initial phase of the aging process in LAC will translate into an accelerated rate of increase of the elderly population. The conditions that account for the acceleration also imply an unfavorable health and disability distributions of elderly cohorts. This feature, in combination with an unusual ecology of diseases, will expand morbidity (Fries, 1980; Singer and Manton, 1994; Manton, 1982) and could lead to a significant upsurge in the demand for elderly care precisely during a period of rapid decline of kin availability.
c. Institutional contexts: the decline of safety nets
Intrafamily support for the elderly is just one part of a larger set of transfers involving several generations and agents. In pre-industrial societies, the bulk of these transfers originated within the family though a significant part of elderly support, particularly for the poor, infirm and destitute came from charity and non government institutions (Lee, 1997; Lesthaeghe, 1980, 1983). In modern societies the public and private sector begins to play a major role, managing transfers from the younger to the older generations. The nature of the institutional environment matters for the existence, quantity and timing of elderly support rooted within the family, mostly involving their children and grand children. When the institutional context is strong and the public sector assumes a dominant role, routine intrafamily transfers to older people are weakened and the motive that supports them languishes (Lee, 1994). But in societies where such institutional context does not exist, is primitive and underdeveloped, covers only a small fraction of the elderly, and has been weakened by political transformations, macro economic stresses or a take over from the private sector, then elderly support becomes critically dependent on intra family exchanges.
c.1.The public sector and the economic environment
Countries in LAC have a relatively long historical tradition of a strong role of the state and the public sector. However, under pressure from recurrent economic crises, shifts in ideological paradigms and pressure from international institutions and donors, many of these systems have begun to dissolve and massive reforms have placed a larger part of the responsibility for elderly support on individuals themselves (through private sector and present investments) or on their families. This sudden redirection of systems of intergenerational transfers occurs at a bad time, when the aging process is accelerating and in the absence of sustained macroeconomic performance, high sensitivity to recurrent recessions and high levels of poverty and inequality. Unlike high-income countries, aging precedes by a long time the establishment of economies with high income per capita, lower levels of inequality and reduced poverty.
In a bleak overview of conditions in the region, Kliksberg (2000) presents evidence suggesting that (a) levels of poverty have increased drastically since 1985 and so have levels of economic inequality; (b) unemployment rates have increased, particularly among the most youthful and poorest segment of the population; (c) deficits in budgets associated with public health have ballooned; (d) the informal sector of the economy has expanded considerably. As a real income shrinks, access to health services weakens and transfers from the public sector in the form of retirement pensions and welfare spiral downwards (Marichal, 1989; Altimir, 1984). Additional moves toward draconian fiscal policies and a shrinkage of the contribution of publicly funded programs will erode further safety nets and reduce protection to the weakest members of societies.
c.2. Pension systems
In a pay-as-you-go system, there are several sources of tension that need to be neutralized. The first is associated with the sheer increase in the older population relative to the economically active population. As we showed before all countries in the region will surely experience a drastic increase in the ratio of pensioners to workers as a result of past demographic trends. The second source of tension is associated with improvements of survival of the elderly population. Gains in survival will increase the expected length of time to be spent as a pensioner, and will be manifested numerically in an increase in the rate of increase of the elderly population and as an increase in the proportion of the total population aged 60+. Unlike the previous source of tension, this one will depend on future rather than on past trends in mortality. The third source of tension is related to the health and disability status of the elderly. Demand for health care services will certainly go up simply as a result of the increase in the population 60+. But the rate of increases can spike substantially if, in addition, the composition of the elderly population by health and frailty is unfavorable.
The imbalance generated by excess demand for pension payments and health care services generated by these three sources of tension will require measures with adverse effects on one or more sub-populations: benefits to the elderly could be reduced, age at retirement can be gradually increased so that pension expenditures (and associated health benefits) balance out tax receipts and, finally, tax receipts on the economically active population can be increased. In most cases a combination of these solutions produces temporary relief in a relatively equitable manner.
Privatization (or capitalization schemes) has been hailed as a full or partial solution to existing cracks in the public pension systems (Barrientos, 1997; Barrientos and Firinguetti, 1995). But these schemes are unlikely to resolve the problems posed by the peculiar demographic profile of the elderly in the region. The author of a recent evaluation of conditions in LAC concludes “Pension reform has contributed to make the labour market the main source of social insurance for the majority of households in Latin America. Given the record of the Latin American economies in the past few decades, and the current changes under way in their labor markets, it is at least doubtful that the growing ranks of the old will find the future more secure” (Barrientos, 1997: 351).
There are two and only two offsetting mechanisms that can be deployed to maintain or increase quality of life of the elderly. One of them is to reinforce support from families and kin either through shared residential arrangements or through persistent flow of goods and services. The other mechanism is an increase in the labor force participation of the elderly. If these mechanisms are not fully utilized or if they are inefficiently implemented, there will be deterioration of well being, particularly among elderly women. The first mechanism is already being used actively and there are attempts to prop its continued implementation. We will show later that in a sample of countries of the region, intra family transfers are almost universal though they are dependent on a number of individual characteristics. It is telling that in other low to middle income countries increasingly weary governments are warning that it will be necessary to reinforce family and kin sources of support (Knodel et al., 1997). The mounting financial pressure exerted by the growth of the elderly population appears impossible to arrest with conventional instruments involving fiscal expenditures only.
The second mechanism is feasible solution provided that, as is thought to occur in other social and economic contexts, increased labor force participation of the elderly is a likely response to economic considerations. We suspect, however, that this solution will not be very effective in LAC. First, labor force participation rates among the elderly in the region are already far higher than elsewhere and is likely that the segment of the labor market to which most elderly can contribute effectively is already saturated. Second, the idea that labor force participation responds only to economic incentives neglects evidence indicating that it is also a function of health and disability status. To the extent that this is so and that elderly health and disability status in the region may actually worsen, further increases in labor force participation are not likely to occur. Finally, the areas of the economy where current and future elderly can contribute are those with low productivity, low human capital requirements and low wages.
d. The ideological context and kin’ s propensity to support the elderly
Paradoxically, the same shifts in values and ideology that undercut traditional fertility regimes will also erode the cultural fabric on which traditional elderly support rests.
Transactions between generations are not just constrained and shaped by demographics, economics or political factors. They also depend on normative contexts, largely determined by shared beliefs and cultural values and by the institutional context that regulates exchanges via redistribution of income and goods and services. In most societies intergenerational transfers rest on an implicit contract between members of different generations. Although there are other determinants that affect both the direction and magnitude of these transfers, they depend on motivation and incentives to maintain intergenerational solidarity. Transfers from the younger to the older generations that occur within the family—as opposed to those that originate in private markets and in the public sector-- are particularly dependent on the strength of this motive. It can acquire a variety of forms, including coresidence with older parents, financial aid, provision of goods and supply of services in the form of time spent caring for infirm or disabled parents, company and leisure, security, etc.
Industrialization and urbanization caused a sharp fertility decline and, simultaneously, a weakening of the moral sense of obligation toward the older generation. The younger generation became more preoccupied with their own well-being and the quality of their own (reduced number of) children than with the well being of their parents. The ethic of filial piety is thought to crumble under industrialization, commercialization, and the emergence of large urban centers (Ruggles, 2009). The onset of the second demographic transition, the passage from a “modern” to a “post modern” ethics (Van der Kaa 2002), and the emergence of a hedonistic culture increases the pressure on individuals to withdraw from intergenerational exchanges that favor the elderly. This transition in value systems regarding intergenerational transfers is at least implicit in various theories of fertility decline, including those that attribute the passage from a high to a low fertility regime to a reversal of intergenerational wealth flows (Caldwell, 1976;1982) as well as to the adoption of a ‘Western (individualistic) ideology’ (Caldwell, 1982), and to the diffusion of ideas and preferences that emphasize individual aspirations and investments that enhance the quality of children at the expense or in lieu of investments on parents (Cleland and Wilson, 1987).
If these conjectures are borne out by the facts and if the linkage between value systems and shifting fertility regimes remains strong, low and middle income countries in general and LAC in particular will experience a devaluation of the intergenerational contract that acted as a prop for elderly support
In summary, countries in LAC will experience rapid and compressed aging under institutional constraints that allocate only a weak role to public transfers, where important fractions of elderly individuals’ needs will go unsatisfied, or partially satisfied via intra family support and, much less so, through increases in private income from reentry in the labor market. These demographic and institutional conditions affecting the demand and supply of support may not have had enough time to operate to alter the nature of entrenched patterns of old-age support. But since countries in the region are at different stages of the demographic transition, we should be able to exploit the resulting heterogeneity to understand the transformations, if any, forced by demographic, cultural and institutional changes. The following table summarizes the main points
IV. Intergenerational transfers in LAC: recent patterns and trends
The foregoing description highlights the potential fragility of intrafamily and institutional transfers to the elderly in AC countries. Constrains in the supply of support and simultaneous increases in the size of the demand may threaten the future well being of the most vulnerable segment of the population.
In this section we describe for the first time patterns of intrafamily transfers in seven countries of the region. In the almost absolute absence of previous knowledge about general patterns of intrafamily transfers, the description that follows is useful to illustrate regularities that may be foretelling responses to stresses identified above.
a. Data
We use data from the survey SABE (Salud, Bienestar y Envejecimiento), a multicenter survey to investigate the health and well-being of older people in various Latin American and Caribbean cities. The SABE study provides a unique opportunity to carry out a comparable cross-national survey of older persons in selected urban areas of the region. The populations studied are adults aged 60 and older residing in private households occupied by permanent dwellers in each of the seven selected cities (Buenos Aires (Argentina), Bridgetown (Barbados), Sao Paulo (Brazil), Santiago (Chile), Havana (Cuba), Mexico City (Mexico), and Montevideo (Uruguay)).
Table 2 displays basic information from the survey. The individual response rates are up to international standards even in the cases of Argentina and Uruguay, the two countries with the highest rates of non response.The survey includes information on key demographic, socioeconomic and health characteristics of the target and coresident and non resident children, siblings, other relatives and friends, and other persons, during the last 12 months. It includes information on age, sex, education, marital status, working condition, self-reported health, chronic conditions, functionality, and health coverage, and transfers received from and provided to coresident and non resident relatives, friends, and other persons including institutions or organizations in the community.
Table 2:
Variables in Latin American Elderly in Seven Cities (percent)
| Characteristic | Pooled | BA | BT | SP | SG | HV | MX | MV |
|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||
| Females | 61.6 | 63.3 | 59.7 | 58.9 | 65.7 | 62.8 | 59.3 | 63.4 |
| Males | 38.4 | 36.7 | 40.3 | 41.1 | 34.3 | 37.2 | 40.7 | 36.6 |
| Age | ||||||||
| 60–69 | 45.2 | 47.3 | 41.7 | 37.6 | 47.5 | 46.5 | 55.6 | 47.1 |
| 70–79 | 36.0 | 39.5 | 38.4 | 37.7 | 34.5 | 31.8 | 31.0 | 39.5 |
| 80–84 | 10.5 | 8.1 | 11.0 | 14.3 | 9.8 | 10.9 | 7.9 | 8.6 |
| 85 + | 8.2 | 5.2 | 8.9 | 10.4 | 8.1 | 10.9 | 5.6 | 4.9 |
| Marital status | ||||||||
| Married | 46.2 | 43.0 | 44.9 | 52.3 | 43.6 | 37.4 | 53.9 | 48.7 |
| Widowed | 33.9 | 41.8 | 23.6 | 35.5 | 35.8 | 35.0 | 32.0 | 36.7 |
| No unión | 19.9 | 15.2 | 31.5 | 12.2 | 20.6 | 27.6 | 14.1 | 14.6 |
| Education | ||||||||
| No schooling | 10.2 | 3.5 | 0.8 | 24.5 | 11.3 | 4.7 | 19.1 | 4.3 |
| Elementary | 62.7 | 68.2 | 75.8 | 63.1 | 60.0 | 52.1 | 58.5 | 61.4 |
| Secondary + | 26.7 | 28.4 | 22.9 | 11.5 | 28.6 | 43.2 | 20.9 | 33.9 |
| Head of household | 69.5 | 69.0 | 81.2 | 62.5 | 64.6 | 72.7 | 61.4 | 73.0 |
| Currently employed | 20.9 | 24.2 | 16.2 | 20.4 | 24.1 | 18.5 | 30.6 | 17.0 |
| Home Owner | 74.3 | 88.2 | 60.2 | 81.2 | 86.7 | 59.6 | 84.8 | 71.2 |
| With health coverage | 79.0 | 82.7 | 15.0 | 97.4 | 88.5 | 100 | 73.0 | 97.9 |
| Self-rated health | ||||||||
| Good/very good/excellent | 46.9 | 65.1 | 50.2 | 44.7 | 35.4 | 43.1 | 30.3 | 63.2 |
| Fair/bad | 53.1 | 34.9 | 49.8 | 55.3 | 64.6 | 56.9 | 69.7 | 36.8 |
| Disability | 19.9 | 18.6 | 13.8 | 23.7 | 25.6 | 20.5 | 19.4 | 17.0 |
| At least one ADL | ||||||||
| At least one IADL | 23.8 | 19.1 | 20.2 | 35.2 | 27.0 | 23.0 | 23.5 | 13.2 |
| At least 1 chronic condition | 77.5 | 81.6 | 76.6 | 76.8 | 80.7 | 81.0 | 68.6 | 76.8 |
| Sample size | 1043 | 1812 | 2143 | 1306 | 1905 | 1247 | 1450 | 1096 |
| Response rates | --- | 62.5 | 80.3 | 84.6 | 84.0 | 95.3 | 85.0 | 65.3 |
BA: Buenos Aires, BT: Bridgetown, SP; Sao Paulo, SG: Santiago, HV: Havana; MX: Mexico City, MV: Montevideo
Table 2 summarizes targets’ socioeconomic and health characteristics in all seven cities and in the pooled data. Around 60 % of the population being studied are females and over 40 % is aged 60 to 69 years. Most elderly in all seven cities are married or in a consensual union, while more than one-third are widow(er)s. The majority of respondents have no more than elementary education (a minimum of 52% in Havana and 75.8% in Bridgetown). Working condition at the time of the interview varies greatly across cities: the largest percentage is in Mexico City (31%) while the lowest is in Bridgetown (16%). The largest fraction who are household heads is in Bridgetown (81%), while the lowest is in Mexico City (61%). Home ownership varies from 61% (Mexico City) to 81% (Buenos Aires). Health characteristics display important variation across cities. Levels of health coverage vary from a low 15% who have some kind of insurance in Bridgetown to being universal in Havana. Second, elderly health status varies greatly among cities when measured by self-reported health, number of ADLs and IADLs, and chronic conditions. The proportion of people with at least one ADL ranges from 14% in Bridgetown to 26% in Santiago and the levels of IADL range from 13% in Montevideo to 35% in Sao Paulo. With the exception of Buenos Aires and Montevideo, the fraction that self-reports fair or bad health exceeds 50%. The prevalence of chronic conditions exceeds 60% everywhere.
b. Determinants of elderly support
We start from the premise that elderly support depends on two conditions: availability of alters and propensity of alter to engage in transactions. The observed value of the prevalence of transactions of any arbitrary currency is simply the product of the probability that an elderly person has alters available to effect a transaction and the conditional probability that these alters supply the currency. We focus first on transactions involving money, goods, and services and then on patterns of coresidence. We first describe measures of availability and propensity and then estimate logit models to generate predicted probabilities of transaction of a given type.
b.1. Definitions and notation
We use the term ‘ego’ to refer to the target elderly and indexed by k. We use the term ‘alter’ to refer to those who can provide support. They are indexed by j. These include spouses, children (living or not at home), and others (including siblings, other relatives and friends). We use the term ‘currency’ or ‘product’ to refer to the materials that are transacted and are indexed by r. These include income, goods, and services/others (including time). The expression for the probability of receiving help by k from j, Pjk, is as follows
where Pjk is the probability that alter j gives support to k, pjk is the propensity of alter j to provide support for k and Qjk is the probability of elderly k to have and alter j available. To simplify description we define the following subpopulations of egos:
Population 1: composed of targets who live alone and have no surviving children; Population 2: composed of targets who live alone but who have surviving children;
Population 3: composed of targets who have no spouse but live with at least one child;
Population 4: composed of targets who live with a spouse but have no surviving children;
Population 5: composed of targets who live with a spouse and have surviving children;
Population 6: composed of targets who live with spouse and at least one surviving child
Population 7: a residual population including rarely found coresidential patterns.
These 7 subpopulations consist of sets of elderly according to available (supply of) alters (including spouses and children). The main distinction between subpopulations 1 and 2, for example, is one of availability of surviving children whereas the distinction between 2 and 3 is the residential arrangement. The same applies to subpopulations 4 and 5 and 5 and 6 respectively.
We calculate quantities Qjk’s as the fraction of target elderly in each of the subpopulations defined above. Qjk’s are the outcome of past demographic regimes, the result of individuals’ fertility, migration, mortality and, more generally, family history. Aggregate differences in Qjk across countries reflect the influence of both demographic regimes and cultural norms regarding co-residence. Throughout we will take them as given.
The quantities pjk refer to the proportion of elderly in a given subpopulation who receive some type of support from the available alters. Unlike the Qjk these quantities can be modeled as follows:
where φ(pjk) is a linearizing transform (such as logit), Zj is a vector of characteristics for alter j and Xk is a vector of characteristics for ego k. We can define pjk for each of the currencies or products involved in transactions (money, goods, and services and other). If there are three products we will have pjkr for r =1,2, 3. But we can also have pjk for ANY one combination of the r’s. We will consider the following combinations and contrasts: No transactions vs any; transactions including money and goods only; transactions involving services only. We will label these combinations r =1, 2, and 3 respectively and denote pjkr the probability of combination r.
The classification of elderly into seevn subpopulations is a simplifying device to ease the discussion of availability and propensities. It also enables us to lighten the notation. In what follows we will refer to availability Qs (s=1,2…7) to mean the fraction of elderly in subpopulation s (with an implicit availability of alters defined by the nature of s) and to prs as the probability that an elder in subpopulation s receives support of type r from among some of the alters included (permissible) in subpopulation s.
The predicted (via logit models) values of psr combined with the observed (sample) values of Qs yield the following:
where P r (Z) is the proportion of elders with vector of characteristics Z who receive support of type r and ps r is the predicted (via logit models) propensity to provide support of type r in subpopulation s and with characteristic X. The summation is over all subpopulations distinguished above, and P r(Z) can be interpreted as the predicted prevalence of support of type r among elderly with characteristic Z. Note that the operation above is analogous to the calculation of a crude rate with Qs (X) performing the role of age composition and psr standing in for rates.
b.2. Descriptive results: summary measures
Table 3 displays the main quantities of interest in all seven cities and in the pooled sample for each currency defined above. The least common subpopulations are those with no available surviving children (1 and 4) whereas the most common are those with surviving children either not living with the target elderly (2 and 5) or living in with an elderly couple (6) or with the target elderly alone (3). There is sizeable intercountry variability in the distribution of elderly by subpopulations. Cities in countries with the heaviest aging (Argentina, Barbados, Cuba and Uruguay) exhibit higher prevalence of the least common subpopulations, those where surviving children are either not available (2 and 4) or where they live apart (5). The second panel of Table 2 table displays observed propensities of alter(s) to provide elderly support in each subpopulation. With the exception of subpopulation 1, propensities are high, in most cases exceeding .60 or .70. Thus a majority of elders receives some kind of support from alters regardless of subpopulation. There is only modest diversity in propensities across all 7 cities. First, in countries where aging is more advanced, elderly whose population of alters is reduced are more likely to receive support than in countries where aging is least advanced. Second, there is high propensity of support in subpopulations that include a spouse, irrespective of whether or not there are children surviving available. It is likely that in these cases the provider of support is the spouse herself. The last panel displays the product of the values in each of the other two panels. The sum of these values is the average prevalence of support in each sample(including the pooled sample in the last row of last panel).
Table 3.
Observed values of kin availability and propensity to support Eldery
| A. Percents of targets having available alters (Qjk) | ||||||||
| Population | Pooled | BA | BT | SP | SG | HV | MX | MV |
| Alone,NOchild(1) | 4.7 | 7.8 | 6.0 | 3.5 | 2.3 | 4.2 | 2.8 | 7.8 |
| Alone,SURVchild(2) | 14.0 | 20.9 | 17.2 | 13.5 | 11.7 | 8.2 | 8.1 | 22.7 |
| NOSpouse,CORESchild(3) | 34.4 | 27.2 | 29.0 | 29.1 | 43.7 | 49.6 | 34.6 | 23.0 |
| SpouseNOSURVchildren(4) | 2.2 | 2.1 | 4.1 | 1.9 | 1.0 | 1.6 | 1.2 | 2.9 |
| SpouseSURVNOCORESchild(5) | 16.7 | 21.3 | 19.7 | 20.8 | 10.9 | 10.1 | 13.0 | 21.9 |
| SpouseCORESchild(6) | 28.1 | 20.7 | 24.1 | 31.1 | 30.5 | 26.4 | 40.4 | 21.7 |
| Residual(R=7) | 8.5 | 6.6 | 8.8 | 8.7 | 8.7 | 10.0 | 6.7 | 8.4 |
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| B. Propensity (in percents) of alters to support(pjk) | ||||||||
| Population | Pooled | BA | BT | SP | SG | HV | MX | MV |
| AloneNOchild(1) | 44.67 | 43.42 | 41.41 | 53.62 | 40.74 | 41.67 | 25.00 | 54.67 |
| AloneSURVchild(2) | 68.02 | 72.55 | 56.34 | 80.75 | 71.94 | 72.34 | 67.02 | 58.72 |
| NOSpouseCORESchild(3) | 95.10 | 92.83 | 91.02 | 97.36 | 96.74 | 96.47 | 95.02 | 91.86 |
| SpouseNOSURVchildren(4) | 90.34 | 70.00 | 86.76 | 94.74 | 100.00 | 100.00 | 78.57 | 100.00 |
| SpouseSURVNOCORESchild(5) | 94.38 | 88.89 | 92.92 | 96.80 | 99.23 | 95.95 | 90.07 | 96.19 |
| SpouseCORESchild(6) | 96.67 | 93.56 | 95.73 | 97.87 | 97.25 | 98.89 | 95.53 | 94.71 |
| Residual(7) | 91.93 | 88.41 | 85.53 | 95.19 | 93.91 | 94.74 | 88.10 | 94.32 |
| Total | 89.40 | 83.89 | 83.61 | 93.70 | 93.11 | 93.02 | 90.06 | 84.16 |
| C. Probability (in percents) of support (pjk*Qjk) | ||||||||
| Population available | Pooled | BA | BT | SP | SG | HV | MX | MV |
| AloneNOchild(1) | 2.10 | 3.39 | 2.48 | 1.88 | 0.94 | 1.75 | 0.70 | 4.26 |
| AloneSURVchild(2) | 9.52 | 15.16 | 9.69 | 10.90 | 8.42 | 5.93 | 5.43 | 13.33 |
| NOspouseCORESchild(3) | 32.71 | 25.25 | 26.40 | 28.33 | 42.28 | 47.85 | 32.88 | 21.13 |
| SpouseNOSURVchild(4) | 1.99 | 1.47 | 3.56 | 1.80 | 1.00 | 1.60 | 0.94 | 2.90 |
| SpouseSURVNOCORESchild(5) | 15.76 | 18.93 | 18.31 | 20.13 | 10.82 | 9.69 | 11.71 | 21.07 |
| SpouseCORESchild(6) | 27.16 | 19.37 | 23.07 | 30.44 | 29.66 | 26.11 | 38.59 | 20.55 |
| Residual(7) | 7.81 | 5.84 | 7.53 | 8.28 | 8.17 | 9.47 | 5.90 | 7.92 |
| Total | 89.40 | 83.89 | 83.61 | 93.70 | 93.11 | 93.02 | 90.06 | 84.16 |
Figure 2 displays (a) the proportion of elderly receiving any support whatsoever (any-support) and (b) the proportion whose support consists of a bundle that includes money and goods only, and those that include services only. The proportion receiving support is close to .9 and varies little by age or gender. The fraction receiving money as part of a bundle of currencies is higher among females than among males and in both cases drops off with age.
Figure 2:
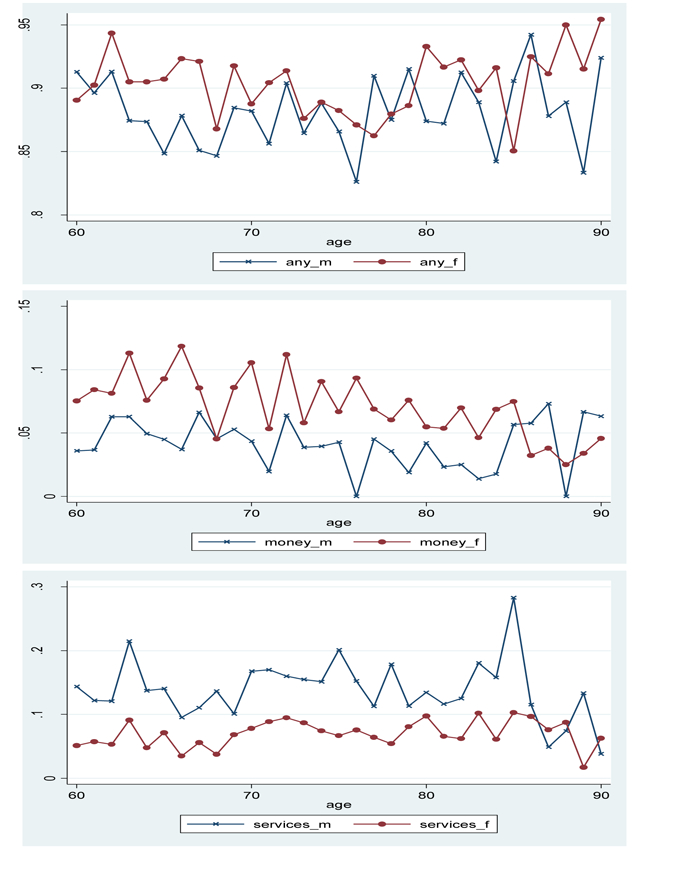
Observed prevalence of elderly support: any support, money, and goods and services
Legends: xxxx_m refers to males; xxx_f refers to females
b.3 Iso-transfer curves
For any type of currency r (including any type of help) we can construct curves representing combinations of different values of Qs and prs that yield the same value of the product ϑrs= Qs*prs. We can let Qs vary from .10 to 1 in jumps of .25 and, for each one of these values, we calculate the prs that produce any arbitrarily chosen value of ϑrs.. The result is a set of hyperbolae showing different combination of availability of alter and propensities that yield the same values of ϑrs for any given r. Plots of these curves by r leads to r-specific iso-transfers surfaces. These iso-transfer curves and surfaces are useful to understand contrasts between different countries as well as trajectories followed by different societies. For example, according to some theories prevalence of transfers of any type should diminish simply because demographic availability of alters shrinks (demographic constraints influencing supply). If so, a society in a transfer surface would drop from a high level curve to a low level one by moving only along the Qs’ axis. Alternatively, if the shift is associated with changes in propensities, the point in the graph will drop along the ps axis. Figure 3 displays an example of inso-transfers and illustrates these two types of shifts
Figure 3:

Iso-transfer surfaces for populations 3 and 6 (propensity to support, pjk; availability of support, Qjk)
Figure 3 displays iso-transfers curves and locates each country in the space of possible contours. We do this for the two most commonly found subpopulations, namely, 3 and 6 and for only one currency, namely, any support. Expectations are that cities in countries with least advanced aging (Mexico City, San Paolo, Santiago) should be located on the upper part of the diagram (higher propensities) and leaning toward the right quadrant. By contrast, cities in countries with more advanced ageing (Buenos Aires, Montevideo, Havana) should be located on the lower part of the diagram (lower propensities) and in the left quadrant of the diagram (lower propensities)
b.4 Decomposition of differences of prevalence of elderly support
Differences in prevalence of elderly support associated with any currency can be decomposed into those associated with differences in the elderly distribution by subpopulation and differences in propensities. Indeed, for any two populations
where s refers to subpopulation type, P’s are the prevalence of transfers of any type in populations 1 and 2 , and p and Q refer to propensities to transfer and prevalence of subpopulations of type s respectively. The difference between P1 and P2 is like a difference between crude death rates but instead of age distributions we have population composition by type (defined by Q’s) and instead of rates we have propensities, ps r
As an illustration we compare the two cities representing countries at the extreme of the aging process, Buenos Aires and San Paolo respectively. The total difference (see Table 3) is of the order of .10 (.84 for Buenos Aires and .94 for San Paolo). Of this difference, the bulk (.072) is associated with differences in propensities and the residual (.03) is associated with differences in the distribution by subpopulations. Thus, the tug of aging in this particular comparison is felt primarily because of changes in propensities not because of supply constrains due to demographic availability.
c. Modeling transfers
We now attempt to identify the most important determinants associated with transfers to elderly in LAC. While there is a fair amount of research about elderly support in other developing countries, there is little in the LAC region. A notable exception to this is the pioneering work by Wong and colleagues using the MHAS, the Mexican Survey of Aging (Wong, 2008; Wong and Higgins, 2007).
Elderly support can originate in four different sources: (a) unearned income from assets or public sources, (b) pension and welfare receipts, (c) earned income from labor force participation, (d) intergenerational coresidence and (e) direct intergenerational transfers from children to elderly. While (a) and (b) can be considered as exogenously defined, the other three types involve complicated reciprocal relations. Thus, an older adult’s decision to remain or reenter the labor force may depend on the magnitude and stability of children support. This, in turn, could be influenced by the willingness and possibilities that the elderly has to remain or reenter the labor force. Similarly, transfers from children who do not coreside with their parents may depend on whether or not there is intergenerational coresidence. To the extent that there is coresidence, transfers could take the form of coresident children’ help within the household replacing transfers from children living outside the elderly’ household. Thus modeling (e), (c) and (d) independently will lead to inconsistent estimates and results.
One way to approach the problem has been suggested by Cobb-Clark and Cameron (2008) as well as Nguyen (2008) who, following the lead of Lillard and Willis (1997) model simultaneously the elderly supply of labor force, coresidenec and transfers from children not living in the household. To simplify the estimation and because labor force participation of elderly in LAC is rather reduced we opt for a simpler strategy, namely, to model simultaneously intergenerational coresidence and transfers from children not living in the household while ignoring the role of elderly labor force participation. The model contains two equations for two latent variables:
where TR*i is a latent continuous variable for transfers from children living outside the household to individual i, CR*i is intergenerational coresidence (latent continuous variable) for individual i, Xi is a vector of covariates affecting both CR*i and TR*i, Zi is a vector of instruments which influences CR*i but not TR*i, and εTRi and εCRi are correlated normally distributed error terms. We actually observe TRi and CRi that can be defined as follows:
and
By specifying apriori a scaled matrix of variance-covariance of error terms with the variance of εCRi set to 1, the variance of εTRi set to σ2 and covariance of εTRi and εCRi set to ρ*σ, we can estimate the model using a modified iv probit model. Because the endogenous variable is discrete instead of continuous, our estimates may not be consistent. The key assumption is that the vector Z contains truly exogenous variables, that is, determinants of CR that do not affect TR. For this purpose the vector Z includes three variables: (1) elderly’s ownership of the home, (2) whether the elderly is a head of household, and (3) a variable indicating proximity of children not living in the household. Although this choice of Z is not entirely satisfactory since one could argue that any of these covariates can also influence transfers, we surmise that relations are weak and the damage to our estimates is modest.
We then proceed to estimate the equation for coresidence using a simple probit model and, in a second stage, the jointly observed outcomes CR and TR to generate estimated parameters for TR. We use the sample of elderly individuals with surviving children and children living outside the household. This subsample is appropriate since it includes only individuals who have the possibility of experiencing both intergenerational coresidence and transfers from children who do not coreside. Among these, only a subset has children who do not coreside with them and who can provide transfers while living in a different household. While these individuals may contribute to the equation for coresidence they do not contribute to the equation for transfers.
The main results are displayed in Tables 4a, 4b and 4c
Table 4a:
Estimated probit coefficients of demographic, socioeconomic, and health variables on the probability of coresiding with children
| Exogenous variables | Coeff. | p-value |
|---|---|---|
| Parents’ characteristics | ||
| Age | 0.020 | 0.000 |
| Gender | −0.132 | 0.003 |
| Education (Ref. none) | ||
| Elementary | −0.064 | 0.314 |
| Secondary | −0.294 | 0.000 |
| Marital Status (Ref. in union) | ||
| Widows | 0.472 | 0.000 |
| No unión | 0.272 | 0.000 |
| Health status (IADL) | 0.238 | 0.000 |
| Head | −0.341 | 0.000 |
| Proximity | −0.224 | 0.000 |
| Wealth | 0.418 | 0.000 |
| Children’s characteristics (all children) | ||
| Males (number) | −0.076 | 0.782 |
| Females (number) | −0.136 | 0.622 |
| Marital status (number) | ||
| Single | 0.204 | 0.000 |
| Married | −0.439 | 0.000 |
| Other | −0.451 | 0.000 |
| Employment (number) | −0.171 | 0.000 |
| Education (number) | ||
| None | −0.058 | 0.107 |
| Elementary | 0.021 | 0.348 |
| Secondary or more | −0.035 | 0.119 |
| Number of children | 0.801 | 0.004 |
| Children’s median age | −0.035 | 0.000 |
| Country differences | ||
| Argentina | 0.181 | 0.022 |
| Barbados | −0.553 | 0.000 |
| Brazil | 0.433 | 0.000 |
| Chile | 0.566 | 0.000 |
| Cuba | 0.928 | 0.000 |
| Mexico | 0.507 | 0.000 |
| Constant | −1.935 | 0.000 |
| LR chi square | 4850 | 0.000 |
| Pseudo R square | 0.410 | |
| N | 9106 | |
Table 4b.
Estimated effects of demographic, socioeconomic, and health variables on the probability of receiving help, money and goods, and services. Pooled data (AloneNOchild and SpouseNOSURVchild)
| Independent variables | Any Help | Money/Goods | Services | |||
|---|---|---|---|---|---|---|
| Coeff. | p | Coeff. | p | Coeff. | P | |
| Gender (Ref. female) | 0.1783 | 0.445 | −0.3700 | 0.364 | 0.1943 | 0.527 |
| Age (ref. 60–69) | ||||||
| 70 – 79 | 0.2656 | 0.250 | −0.1202 | 0.743 | 0.7028 | 0.019 |
| 80 – 84 | 0.5493 | 0.083 | −0.5885 | 0.298 | 0.4253 | 0.286 |
| 85 + | 0.3403 | 0.364 | 0.5289 | 0.350 | −0.0309 | 0.954 |
| Education (Ref. none) | ||||||
| Elementary | 0.0337 | 0.935 | 0.7935 | 0.312 | 0.3183 | 0.561 |
| Secondary | −0.3578 | 0.417 | 0.0522 | 0.951 | 0.3540 | 0.542 |
| Marital status (Ref. no union) | ||||||
| Married | 0.5734 | 0.229 | −0.7406 | 0.329 | 0.5253 | 0.436 |
| Widow | 0.4531 | 0.046 | 0.1523 | 0.703 | 0.3210 | 0.301 |
| Employment (Ref. not working) | −0.0035 | 0.989 | 0.3105 | 0.416 | 0.2283 | 0.458 |
| Household headship (Ref. no head) | 0.1469 | 0.783 | −1.2811 | 0.035 | 1.4739 | 0.011 |
| Home ownership (Ref. no owner) | −0.1457 | 0.491 | −0.2784 | 0.401 | −0.0838 | 0.758 |
| Health coverage (Ref. no coverage) | 0.3845 | 0.245 | −0.2687 | 0.594 | 0.5711 | 0.194 |
| ADL (Ref. no ADLs) | −0.1471 | 0.612 | −0.9852 | 0.101 | −0.2069 | 0.562 |
| IADL (Ref. no IADLs) | 0.5424 | 0.048 | 0.0232 | 0.959 | 0.3987 | 0.224 |
| Self report health (Ref. very good) | −0.0034 | 0.987 | −0.3973 | 0.247 | 0.0228 | 0.931 |
| Chronic diseases (Ref. no disease) | −0.0107 | 0.961 | 0.1798 | 0.618 | −0.1003 | 0.720 |
| Supply of caregivers (Ref. pop 4) | ||||||
| Population 1 | −2.4324 | 0.000 | −0.4087 | 0.619 | −0.2329 | 0.730 |
| Countries (Ref. Uruguay) | ||||||
| Argentina | −0.7851 | 0.020 | −0.6043 | 0.316 | 0.0312 | 0.932 |
| Barbados | −0.5954 | 0.139 | −0.2622 | 0.667 | −0.6497 | 0.189 |
| Brazil | −0.1388 | 0.689 | −0.5413 | 0.345 | −0.0317 | 0.931 |
| Chile | −0.6624 | 0.152 | −0.5042 | 0.555 | −0.6030 | 0.287 |
| Cuba | −0.5125 | 0.133 | 0.0693 | 0.897 | −1.3240 | 0.004 |
| Mexico | −1.4247 | 0.003 | 0.4163 | 0.536 | −1.8422 | 0.022 |
| Constant | 1.8773 | 0.026 | −0.6042 | 0.650 | −3.9825 | 0.000 |
| LR Chi Square | 187 | 0.000 | 29 | 0.169 | 49 | 0.001 |
| d.f | 23 | 23 | 23 | |||
| Pseudo R square | 0.2137 | 0.0811 | 0.0906 | |||
| N | 647 | 647 | 647 | |||
Table 4c.
Estimated effects on the probability of receiving any help, money and goods, and services, Pooled data (AloneSURVchild and SpouseSURVNOCORESchild)
| Independent variables | HelpAny | Money/Goods | Services | |||
|---|---|---|---|---|---|---|
| Coeff. | p | Coeff. | p | Coeff. | p | |
| Gender (Ref. female) | −0.7682 | 0.000 | −0.8381 | 0.000 | 0.4596 | 0.004 |
| Age (ref. 60–69) | ||||||
| 70 – 79 | −0.1501 | 0.304 | 0.1376 | 0.486 | 0.0299 | 0.848 |
| 80 – 84 | 0.3410 | 0.169 | 0.0852 | 0.797 | 0.1078 | 0.657 |
| 85 + | 0.3781 | 0.222 | 0.6564 | 0.087 | 0.2392 | 0.419 |
| Education (Ref. none) | ||||||
| Elementary | 0.3438 | 0.120 | 0.169 | 0.551 | 0.7103 | 0.004 |
| Secondary | 0.0716 | 0.774 | 0.0567 | 0.862 | 0.8225 | 0.004 |
| Marital status (Ref. no union) | ||||||
| Married | −0.1962 | 0.556 | −0.1897 | 0.710 | −0.4545 | 0.347 |
| Widow | 0.0285 | 0.854 | −0.3355 | 0.131 | 0.1954 | 0.320 |
| Employment (Ref. not working) | −0.0488 | 0.741 | −0.2688 | 0.213 | 0.1080 | 0.477 |
| Household headship (Ref. no head) | 0.4413 | 0.083 | −0.4936 | 0.093 | 1.4500 | 0.000 |
| Home ownership (Ref. no owner) | −0.0585 | 0.669 | −0.0536 | 0.770 | 0.4062 | 0.013 |
| Health coverage (Ref. no coverage) | −0.3433 | 0.101 | 0.5651 | 0.042 | 0.3778 | 0.148 |
| ADL (Ref. no ADLs) | 0.1133 | 0.539 | 0.0027 | 0.991 | −0.0325 | 0.855 |
| IADL (Ref. no IADLs) | 0.5428 | 0.006 | −0.5599 | 0.026 | −0.2687 | 0.140 |
| Self-report health (Ref. very good) | 0.5097 | 0.000 | 0.0793 | 0.638 | 0.0757 | 0.568 |
| Chronic diseases (Ref. no disease) | 0.1512 | 0.269 | −0.0598 | 0.756 | −0.0069 | 0.963 |
| Gender, child no home (Ref. fem) | −0.0328 | 0.837 | 0.4760 | 0.053 | −0.2656 | 0.093 |
| Marital, child no home (Ref. other) | ||||||
| Single | 0.1237 | 0.435 | 0.0755 | 0.720 | 0.0423 | 0.810 |
| Union | 0.2175 | 0.217 | −0.0791 | 0.756 | 0.1412 | 0.434 |
| Res. Child Education (Ref. high) | ||||||
| None | 0.0953 | 0.517 | 0.2802 | 0.145 | −0.0719 | 0.641 |
| Elementary | −0.1926 | 0.169 | −0.1055 | 0.554 | −0.1167 | 0.408 |
| Secondary | 0.3916 | 0.012 | 0.0046 | 0.981 | −0.2557 | 0.108 |
| Child works (Ref. no work) | 0.5353 | 0.006 | 0.3935 | 0.219 | 0.1433 | 0.504 |
| Children age | 0.0133 | 0.149 | −0.0075 | 0.556 | 0.0012 | 0.904 |
| Surviving children (number) | 0.0217 | 0.507 | −0.0726 | 0.107 | −0.0464 | 0.221 |
| Supply caregivers (Ref. pop 5) | ||||||
| Population 2 | −2.7690 | 0.000 | 0.8692 | 0.104 | −0.2926 | 0.539 |
| Countries (Ref. Uruguay) | ||||||
| Argentina | 0.5620 | 0.022 | −0.1447 | 0.693 | 0.2397 | 0.340 |
| Barbados | −0.3970 | 0.124 | 0.6099 | 0.090 | −0.7272 | 0.024 |
| Brazil | 0.8350 | 0.001 | −0.3872 | 0.275 | 0.6292 | 0.007 |
| Chile | 0.4966 | 0.039 | 0.1738 | 0.595 | 0.0327 | 0.89 |
| Cuba | 0.6158 | 0.009 | 0.6086 | 0.041 | −0.9054 | 0.001 |
| Mexico | −0.2838 | 0.265 | 1.5284 | 0.000 | −0.7504 | 0.027 |
| Constant | 1.4253 | 0.029 | −3.2121 | 0.001 | −4.1371 | 0.000 |
| LR Chi Square(d.f) | 525(32) | 0.000 | 134(32) | 0.000 | 244(32) | 0.000 |
| Pseudo R-square | 0.2060 | 0.0918 | 0.1118 | |||
c.1. Coresidence.
The effects of age and gender of elderly are as expected as intergenerational coresidence is more likely for females and increases steadily with age (see Table 4a). Widow(er)s or not in a union have a higher probability of living with children. Contrary to conventional expectations in the coresidence literature, education exerts no effects whatsoever (Ruggles and Heggenss, 2008). Those who fair worse in terms of IADL are more likely to coreside but neither the presence of ADL nor of chronic conditions increases the likelihood of coresidence. This finding is consistent, though it does not necessarily confirm, that an important motive for coresidence is assistance to elderly who are in need of assistance either because of basic limitations (ADL), health status (chronic conditions), or more general limitations (IADL).
The finding that elderly who are heads are less likely to coreside with children is consistent with the idea that coresidence is a result of elderly people moving in with their children rather than vice versa. Ownership is a powerful predictor of coresidence, as elderly who own their residence are much more likely to live with their children. This may be a result of children moving in with parents, perhaps as a consequence of housing shortages or unemployment. Finally, as the index of proximity increases (more children live close by), the less likely coresidence is. This suggests that living close by is an arrangement that substitutes for coresidence.
The characteristics of children that are most influential are marital status (higher prevalence of married children diminishes the likelihood of coresidence) and employment. Trivially, and as immediate outcome of demographic constraints, elderly who have more children surviving are more likely to coreside with at least one of them. The older the age distribution of surviving children the less likely is coresidence to occur perhaps as a result of constraints imposed by children’s family life. And, finally and again unexpectedly, children education is not at all associated with coresidence.
The final set of estimates are country-specific. Note that countries with heavier aging (Uruguay (omitted category)), Argentina and Barbados) experience least coresidence. An important and interesting exception is Cuba where coresidence is highest even though Cuba is among the oldest populations in the LAC region. It is quite possible that this is the exception that proves the rule: in the absence of housing constraints, coresidence tends to be abandoned as societies age but Cuba is a country with severe housing shortage.
c. 2. Transfers
Table 4b displays estimates for the equations for transfers and it does so by types of transfers. We focus on ‘any help’ first and then on the other types of transactions. Note that the effect of coresidence is as expected: the higher the likelihood of coresidence the less likely it is that children living elsewhere will contribute to elderly support. This is particularly the case for the case of services, the good transacted that is most commonly provided by children who live with their parents. The effect of gender is highly significant and in the expected direction: females are much more likely than males to receive support (of any form). This is consistent with other findings and with the idea that females are more dependent when they become older. As altruistic theories would have it, elderly who are in worse health are more likely to receive support whereas those who have access to alternative types of support (employment, unearned income, health coverage) are much less likely to do so. Children who are most educated, and who presumably are the beneficiaries of preceding parental educational investments, are slightly more likely to provide support than those who are not, but only through flows involving money and goods. Instead children who are least educated, and whose opportunity costs are probably lower, are more likely to provide assistance in the form of goods only. Elderly whose children are in the labor force are more likely to receive support but only in the form of money and goods and not through services which, to be delivered, may require time away from work.
Country differences are striking: with one exception, support is more prevalent in countries with less aging (Brazil, Chile and Mexico). Here again, the exception is Cuba, a country in the upper extreme of aging which has levels of kin support equivalent to those countries located at the opposite extreme. But again this may be the exception that proves the rule: although the public sector plays a key role, severe economic hardship may encourage elderly and kin to engage in alternative forms of support.
An important and unexpected feature of our findings is that support through money is much more likely in Mexico and Cuba. This is probably explained by the fact that it is in these two countries where migrant remittances are more likely to play a role due to established migration flows into and out of the US.
It should be noted that in all cases ρ has a very low value (less than .06) but it is still significantly different from 0 thus suggesting the existence of non-trivial residual endogeneity. This may well be a consequence of ignoring elderly labor force participation, a variable that is likely to influence both, coresidence and transfers, but be also a response to them.
d. Summary of results
The most important findings of the foregoing analysis are the following: (a) transfers in money, goods and services are not substitutes for each other but rather complements as they are similarly determined by children and elderly’s characteristics; (b) poor health status of the elderly (as presence of ADL and IADL or chronic diseases) leads to increments on any type of transfers, regardless of currency; (d) employment of children decreases chances of elderly support, perhaps reflecting opportunity costs; (e) elderly females tend to get more support in general (net of marital status) but particularly in terms of money; (f) elderly who have alternative sources of support are much less likely to receive any type of support but particularly help in the form of direct income; (g) although levels of elderly support exhibits considerable intercountry heterogeneity, elderly residing in countries with less advanced aging receive higher levels of support and, in particular, countries with potential for remittances (Mexico and Cuba) are those where elderly have a much higher probability of receiving money as opposed to goods and services.
e. Limitations
The analysis above has several shortcomings. First, by its very nature and as in most cases we know of, the data do not permit to understand elderly support as part of more general intergenerational transfers that occur over a lifetime. The data only reveal patterns that are the result of realized transactions, not the bargaining and negotiations that per force determine the observables. Second, our findings represent what occurs in large urban centers of LAC countries and do not identify patterns of coresidence and transfers that take place in smaller cities and rural areas. Third, the handling of coresidence, labor force participation, and transfers is deficient on several counts. Perhaps as a result of widespread public sector support, labor force participation in LAC is less than in many other low income countries (Clark and Anker, 1990). Yet within LAC there is a fair amount of heterogeneity: labor force participation ranges from about 20% in Uruguay to up to 60% in Guatemala. Thus, estimating models that ignore labor force participation altogether may lead to differentially biased results thus harming comparability across countries. If our conjectures about effects of demographic regimes and institutions prove to be accurate, future support of elderly may require higher rates of labor force participation everywhere and make the contribution of labor force to elderly support much more consequential. Finally, even if labor force participation were negligible the joint handling of coresidence and transfers is not ideal. A better solution is to treat coresidence as a process which ‘selects’ elderly individual into different ‘realms’ of support: those who coreside receive some type of support but are less likely to accede to others and viceversa. If so, coresidence could be thought of as a ‘treatment’ and the transfers as an outcome of interest. The conventional machinery of matched analyses could then be brought to bear to the data. And if one wants to consider labor force participation as well, it is possible to think of it and transfers as two related outcomes conditional on treatment (coresidence).
V. Conclusion
This review of elderly support in LAC countries and the empirical analyses suggest a number of problems worth investigating. First, that the speed of aging is unparalleled in LAC (and other low income countries) is uncontroversial. The question is whether this accelerated aging will come along with some undesirable features. In particular, is it the case that health status and disability among elderly will be worst than it was in high income countries at similar stages of the aging process?
Second, the transformation of the institutional context generates conditions that pump up the demand for elderly support. Will the resulting gap be filled by families and kin? Third, coresidence is not only a currency transacted across generations but it also oils the machinery for other types of transactions. We have seen that despite demographic constraints, patterns of coresidence in LAC have not changed much and, if anything, they have enhanced intergenerational cohabitation perhaps as a response to the younger generations’ lack of fortune in labor and housing markets. To the extent that patterns of coresidence do not crumble, levels of supports are unlikely to change much without a simultaneous decrease in younger generations’ propensities to provide support. This may be oppose resistance to the erosion of elderly support that originates in the overhaul of familial ideologies. However, it should be noted that coresidence appears to substitute for other forms of support suggesting that if levels of intergenerational coresidence decline, we should expect an increase in transfers form children to parents. Fourth, patterns of support and association with individual characteristics suggest that much of what is known in developed countries is replicated in LAC. In particular, younger children are more likely to support elderly parents when their cost of opportunity is lower and when the elderly are either more infirm or have less access to alternative sources. Fifth, we do not know much about the nature or time trajectory of informal support through private institutions, charities, NGO’s. The evidence we gathered (results not shown) suggests that this type of source of support is neither trivial nor unsystematic. It tends to be more frequent in countries with more advanced aging, where both availability and propensities could have turned against traditional support, and is more common among elderly who have less options available. Informal support deserves special attention for it may become a last line of defense when all other means of support (public sector, intrafamily transfers, coresidence, labor force participation) weaken or vanish altogether.
| Source of stress | Outcome | Dimension affected |
|---|---|---|
| Speed of aging | Rapid growth of elderly population (generational imbalance) |
Availability of kin |
| Sources of elderly growth | Increase of disability and ill-health | Demand for elderly care |
| Ideological changes | Weakening of moral obligation | Propensity to support |
| Institutional changes | Dismantling of pension systems Reduction of public health care (safety nets) |
Demand for elderly care |
Contributor Information
Alberto Palloni, Center for Demography and Health of Aging, University of Wisconsin-Madison.
Guido Pinto, Center for Demography and Health of Aging, University of Wisconsin-Madison.
References
- Altimir O 1984. “Poverty, Income Distribution and Child Welfare in Latin America: A Comparison of Pre- and Post-Recession Data.” World Development 12(3):261–82. [Google Scholar]
- Barker DJP 1998. Mothers, Babies and Health in Later Life London: Churchill-Livingston. [Google Scholar]
- Barrientos Armando. 1997. “The Changing Face of Pensions in Latin America: Design and Prospects of Individual Capitalization Pension Plans.” Social Policy & Administration 31(4):336–53. [Google Scholar]
- Barrientos Armando and Firinguetti L. 1995. “Individual Capitalisation Pension Plans and Old-Age Pension Benefits for Low-Paid Workers in Chile.” International Contributions to Labour Studies 5:27–43. [Google Scholar]
- Bianchi Suzanne, Joseph Hotz V, McGarry Katheleen, and Seltzer Judith A.. 2008. “Intergenerational Ties: Theories, Trends, and Challenges” in Intergenerational Caregiving,” edited by Booth A, Crouter AC, Bianchi SM, and Seltzer JA. The Urban Institute; Washington: DC, pp. 3–44. [Google Scholar]
- Billari Francesco, and Liefbroer Aart C. . 2008. “Intergenerational Ties: What Can Be Gained from an International Perspective” in Intergenerational Caregiving,” edited by Booth A, Crouter AC, Bianchi SM, and Seltzer JA. The Urban Institute; Washington DC, pp. 53–66. [Google Scholar]
- Caldwell JC 1976. “Toward a restatement of demographic transition theory.” Population and Development Review
- Caldwell J 1982. Theory of Fertility Decline New York: Academic Press. [Google Scholar]
- Clark R and Anker R. 1990. “Labour Force Participation Rates of Older Persons: An International Comparison.” International Labour Review 129(2):255–71. [Google Scholar]
- Cleland J and and Wilson C. 1987. “Demand theories of fertility transition: an iconoclastic view.” Population Studies 41(1): 5–30. [Google Scholar]
- Fries JF 1980. “Aging, Natural Death and the Compression of Morbidity.” New England Journal of Medicine 303:130–35. [DOI] [PubMed] [Google Scholar]
- Grushka Carlos O. and Preston Samuel H.. 1995. “Latin America Adult Mortality with Special Attention to Advanced Ages.” Univ of Pennsylvania/Population Studies Center. [Google Scholar]
- Horiuchi Shiro and Preston Samuel H.. 1988. “Age-Specific Growth Rates: The Legacy of Past Population Dynamics.” Demography 25(3):429–41. [PubMed] [Google Scholar]
- Kliksberg B 2000. “America Latina: Una Region en Riesgo, Pobreza, Inequidad e Institucionalidad Social. Unpublisehd Draft.
- Knodel John, Amornsirisomboon Pattama, and Khiewyoo Jiraporn. 1997. “Living Arrangements, Family Support and the Welfare of the Elderly: Findings and Implications of the 1994 Survey of Elderly in Thailand.” Population Studies Research Report 97_43 University of Michigan, Ann Arbor, Michigan. [Google Scholar]
- Lesthaeghe Ron J. 1980. “On the social control of human reproduction” Population and Development Review 6(4): 527–548 [Google Scholar]
- Lesthaeghe Ron J. 1983. “A Century of Demographic and Cultural Change in Western Europe: An Exploration of Underlying Dimensions” Population and Development Review, Vol. 9, No. 3 (Sep., 1983), pp. 411–435 [Google Scholar]
- Lee R 1994. “The Formal Demography of Population Aging, Transfers, and the Economic Life Cycle.” Pp. 8–49 in Demography of Aging, edited by Martin L and Preston S. Washington D.C.: National Academy Press. [Google Scholar]
- Lee R 1997. “Intergenerational Relations and the Elderly” in Between Zeus and the Salmon,” edited by Watcher Kenneth W. and Finch Caleb. Committee on Population. National Research Council; Washington DC, pp. 212–233. [Google Scholar]
- Manton K 1982. “Changing Concepts of Morbidity and Mortality in the Elderly Population.” Milbank Memorial Fund Quarterly 60:183–244. [PubMed] [Google Scholar]
- Marichal Carlos. 1989. A Century of Debt Crises in Latin America: From Independence to the Great Depression, 1820–1930. Princeton, NJ: Princeton University Press. [Google Scholar]
- Palloni A, Pinto G, et al. (2002). “Demographic and health conditions of ageing in Latin America.” International Journal of Epidemiology 31: 762–771. [DOI] [PubMed] [Google Scholar]
- Preston Samuel H. and Lahiri S. 1991. “A Short-Cut Method for Estimating Death Registration Completeness in Destabilized Population.” Mathematical Population Studies 3(1):39–52. [DOI] [PubMed] [Google Scholar]
- Ruggles Steven and Heggenss Misty. 2008. “Intergenerational Coresidence in Developing Countries” Population and Development Review 34(2): 253–281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruggles Steven. 2009. “Reconsidering Northwest European Family System: Living Arrangements of the Aged in Comparative Historical Perspective” Population and Development Review 35(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singer BS and Manton K. 1994. “What’s the Fuss About the Compression Morbidity?” Chance, Fall. [Google Scholar]
- United Nations 1997. World Population Prospects: The 1996 Revision. Anex I, II and III New York: United Nations Department of Economic and Social Affairs, Population Division. [Google Scholar]
- Van de Kaa Dirk J. 2002. The idea of a Second Demographic Transition in Industrialized Countries. Paper presented at the Sixth Welfare Policy Seminar of the National Institute of Population and Social Security. Tokyo, Japan. [Google Scholar]
- Wolf DA 1994. The elderly and their kin: patterns of availability and access. Demography of Aging Martin LG and Preston SH Washington D. C., National Academy Press: 146–194. [Google Scholar]
- Wong Rebeca. 2008. “Are We Asking the Right Questions on Intergenerational ties?” in Intergenerational Caregiving,” edited by Booth A, Crouter AC, Bianchi SM, and Seltzer JA. The Urban Institute; Washington DC, pp. 45–52. [Google Scholar]