

Neurologists are often accused of being interested in only rare incurable diseases. Although this may have been true in the past, today's neurologists claim to be more concerned with common disorders—but are they really?
Methods and results
We derived a “publication ratio” to measure the amount of research interest in 44 conditions representative of the spectrum of neurological disorders, for which there are population based estimates of frequency.1 We divided the number of Medline papers published in 1998 about each condition (in which their MeSH term was the focus of the paper) by a measure of their frequency (incidence or prevalence) × 100 000. When counting the number of publications, the investigator (RAS) was blinded to the frequency of each disease.
Far more papers investigated rare as opposed to common neurological disorders when the relative frequencies of the diseases were taken into consideration (figure). For example, the publication ratio for variant Creutzfeldt-Jakob disease (incidence 0.02 per 100 000 per year) was more than 100-fold greater than for stroke and transient ischaemic attack (combined incidence 250 per 100 000 per year), and the publication ratio for Wilson's disease (prevalence 0.4 per 100 000) was approximately 6000-fold greater than for migraine (prevalence 10 000 per 100 000).
Although there was a shortfall in research into more common neurological disorders, doctors interested in them might not welcome publication ratios equivalent to those for rarer disorders. Overall, there were 42 papers about variant Creutzfeldt-Jakob disease and 4562 about stroke and transient ischaemic attack. If the publication ratio for stroke and transient ischaemic attack had been equal to that of variant Creutzfeldt-Jakob disease, clinicians and researchers interested in stroke would have had to read 525 000 papers in 1998 (about 10 000 per week)—an insufferable burden!
Comment
The research interest in rare neurological conditions is disproportionately larger than that in common conditions. Our results support a change in the focus of medical research towards the most common conditions that are responsible for the greatest disability, death, economic hardship, and loss of quality of life. It is recognised that funding for research into a disease should be proportional to that disease's burden on society2; however, conditions that account for 90% of the global burden of disease receive less than one tenth of the world's health budget.3
Although our results are striking, the crude publication ratio has limitations. The size of the numerator depends on the proportion of papers indexed in Medline, and Medline's accuracy depends on correct identification of publications that focus on the disease of interest. We made no assessment of the quality of the identified publications. We would have calculated a “controlled trials ratio” were it not for the low specificity of the Cochrane controlled trials register (many studies within it are not controlled trials). We chose the best available data on disease frequency,1 although the quality of such data is often imperfect. 
We could have chosen to compare research interest with measures of disease burden other than the number of people affected.4 For example, mortality, years of life lost, and disability adjusted life years correlate with funding by the National Institutes of Health of research into a selection of diseases in industrialised countries.2 Incidence, prevalence, and hospital inpatient days do not show such a correlation.
Some doctors might justify the lower interest in common conditions on the grounds that their aetiology, prognosis, and treatment are better defined. This is not true for many common neurological illnesses—the greatest good for the greatest number is not being achieved. With consumers becoming increasingly involved in research, the public might expect a more utilitarian approach.5
Some of the differences we have observed might be excused by the political, economic, and scientific interest surrounding some diseases. However, we suspect that part of the explanation is also to do with the fashionable nature of some conditions, the availability of research funding, and the character of neurologists themselves. Are other specialists any different? Perhaps they too should examine their track records.
Figure.
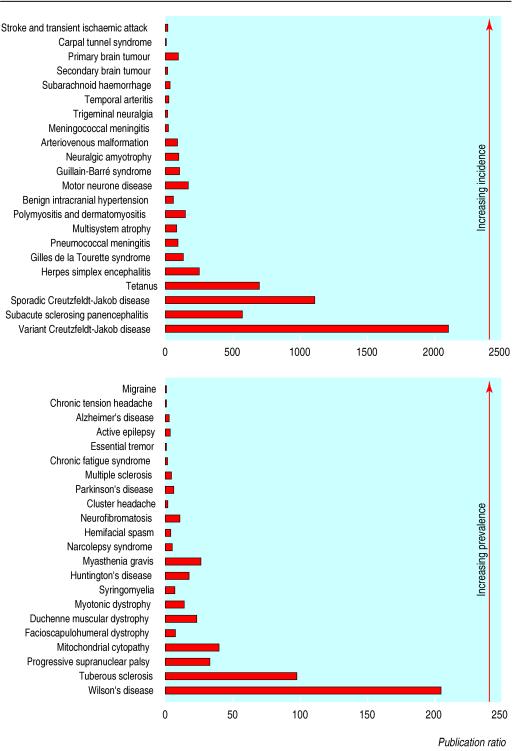
Publication ratios for 44 neurological conditions ordered by their incidence (top) and prevalence (bottom)
Footnotes
Funding: RAS was funded by a Medical Research Council clinical training fellowship.
Competing interests: The research interests of the authors are stroke (RAS and CPW) and Creutzfeldt-Jakob disease (RGW) and, of course, they are all neurologists.
References
- 1.Warlow CP. The frequency of neurological diseases. In: Donaghy M, editor. Brain's diseases of the nervous system. 11th ed. Oxford: Oxford University Press; 2001. [Google Scholar]
- 2.Gross CP, Anderson GF, Powe NR. The relation between funding by the national institutes of health and the burden of disease. N Engl J Med. 1999;340:1881–1887. doi: 10.1056/NEJM199906173402406. [DOI] [PubMed] [Google Scholar]
- 3.The 10/90 report on health research. Geneva: Global Forum for Health Research; 2000. [Google Scholar]
- 4.Frankel MA. The natural history of waiting lists—some wider explanations for an unnecessary problem. Health Trends. 1989;21:56–58. [PubMed] [Google Scholar]
- 5.Tallon D, Chard J, Dieppe P. Relation between agendas of the research community and the research consumer. Lancet. 2000;355:2037–2040. doi: 10.1016/S0140-6736(00)02351-5. [DOI] [PubMed] [Google Scholar]