

Abstract
Purpose of Review
The role of retrograde hindfoot nailing in the treatment of acute orthopedic trauma is explored.
Recent Findings
Tibio-talar calcaneal (TTC) nailing is an acceptable treatment alternative for the low-demand geriatric patient with peri-articular ankle trauma permitting immediate weight-bearing with low rates of complication and return to functionality. Hindfoot nailing can be used for limb salvage in the younger active patient; yet, joint-preserving reconstruction is preferred when feasible.
Summary
Retrograde TTC nailing is a reliable option for hindfoot/distal tibia stabilization especially in the elderly frail population. Hindfoot nailing is reserved for a select subset of active patients when severity of bone, joint, and soft tissue injury are not amenable to more conventional reconstruction.
Keywords: Geriatric ankle fracture, Hindfoot nail, Tibio-talar calcaneal nail, Primary ankle fusion, Limb salvage
Introduction
Retrograde tibio-talar calcaneal nailing has a definitive role in the treatment armamentarium for acute trauma involving the distal tibia and hindfoot. Although stringent indications for this technique continue to evolve, tibio-talar calcaneal (TTC) nails have been shown to effectively treat a range of hosts and pathologies from low-energy geriatric injuries to severe high-energy trauma. Yet, hindfoot nailing has traditionally been utilized as a secondary procedure for post-traumatic reconstruction/arthrodesis, and is often performed months to years after the sentinel injury [1].
A nail is ideally suited for the reliable immobilization of the hindfoot/distal third tibia via insertion through a biologically advantageous surgical exposure. Depending on the indications for the procedure and the functional goals of the surgery, TTC nails can be for acute trauma stabilization with or without intent for joint fusion. Outcomes have been largely optimistic in the treatment of unstable geriatric peri-articular ankle trauma [2, 3•, 4•, 5•, 6•, 7•, 8••], and hindfoot nailing of severe high-energy injuries in a younger, active population is a useful limb salvage technique [9–14]. TTC nails have also been used in conjunction with other reconstructive techniques to further improve the likelihood of a successful arthrodesis.
Indications for Acute TTC Nailing
Hindfoot nails are a viable option for arthrodesis of the ankle and/or subtalar joint after severe lower extremity trauma. Primary arthrodesis in the acute management of severe foot and ankle trauma continues to gain in popularity, particularly for patients with injury patterns associated with profound irreversible cartilage injury [15, 16]. Specific examples include AO type 43-C pilon fractures, talus fracture/dislocations, and calcaneal fractures. Purported benefits of TTC nails in this setting include the requirement of only a single reconstructive operation to promote optimal long-term outcomes.
A hindfoot fusion nail effectively renders the hindfoot stiff, mechanically inhibiting motion at both the ankle and subtalar joints. However, acute arthrodesis with a hindfoot nail can be potentially advantageous over more conventional fusion constructs in patients with specific host and injury factors. For instance, the polytrauma patient with a devastating tibial plafond and/or hindfoot injury may benefit from the placement of a TTC nail as a load sharing device, which may permit early mobilization [6•, 7•, 12]. Hosts with co-morbid medical conditions, such as diabetes and peripheral vascular disease, are candidates for this less invasive stabilization technique, thereby limiting the risk of infectious complications from impaired wound healing. Injury patterns with severe concomitant closed or open soft tissue disruption are ideally suited for an intra-osseous device [17]. Fractures with excessive comminution or bone loss benefit from a bridging nail fixation. Finally, complex fracture patterns that render both the ankle and subtalar joints vulnerable to early post-traumatic arthrosis deserve consideration for retrograde hindfoot nailing.
In contrast, TTC nailing is an accepted alternative treatment strategy for the low-demand geriatric patient after peri-articular fragility ankle trauma. Nailing is a powerful technique for reliably stabilizing the hindfoot/distal tibias of this patient cohort, which also commonly presents with co-morbidities including diabetes or vasculopathies in addition to their intrinsic poor bone quality. Nailing in these hosts may be performed with or without formal preparation of the joint for fusion. Nails are typically chosen when more traditional internal or external fixation techniques are deemed unreliable [18], and if early mobilization is a treatment goal.
Selected injury patterns amenable to hindfoot nailing in the geriatric host include unstable ankle fracture-dislocations, tibial pilon fractures, and distal quarter tibia fractures [2, 3•]. Further, open peri-articular ankle injuries are suitable for TTC nailing following debridement through the traumatic wound. Rigid stabilization of the skeletal anatomy not only promotes bone healing, but also creates an optimal healing environment for the compromised soft tissue envelope.
Biomechanics of Tibio-talar Calcaneal Nailing
Prior to the commercial availability of hindfoot nails, the utility of retrograde TTC stabilization using an intramedullary nail to bridge the subtalar and tibio-talar joints after selected high- and low-energy trauma was evident to orthopedic trauma surgeons. Curved humeral [4•] and tibial nails [2] were used “off-label” for fracture stabilization and/or joint arthrodesis, inserted retrograde through the anterior process of the calcaneus (Fig. 1). The geometry of the chosen nails accounted for the lateral offset of the calcaneus in relation to the tibial shaft in the coronal plane. Longer nails were initially preferred due to the early belief that failure to bypass the isthmus of the tibia with the chosen stabilization technique would increase the risk of periprosthetic fracture [7•].
Fig. 1.
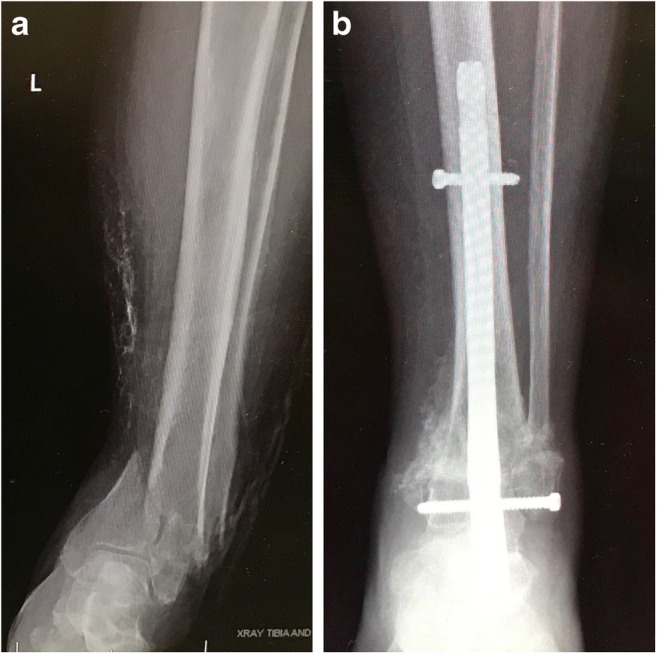
a 89-year-old female with open distal quarter tibia fracture. Patient with co-morbid medical conditions and minimally ambulatory. Patient and family decided to pursue limb salvage yet amputation was offered. Conventional ORIF, antegrade nailing, or external fixation strategies deemed unreliable in this patient with diabetes, peripheral vascular disease, and osteoporotic bone. b Nail inserted retrograde after open fracture care resulting in uneventful fracture healing and ankle joint auto-fusion
Fortunately, nails specific for hindfoot stabilization have been developed and are in widespread use. Modern nail designs permit their intra-osseous passage through the calcaneus and talus into the tibia. Further, cross locking options exist for the calcaneus, talus, and tibia to control both rotation and length. Intra-operative or dynamic compression can be applied when advantageous.
Hindfoot nailing has evolved as a viable treatment strategy because of its numerous biomechanical advantages. TTC nails are durable internal splints for supporting fracture union and/or hindfoot arthrodesis. They are mechanically superior to extra-medullary implants in this application [19]. TTC nails exert maximal leverage in the short distal segment, ensuring a more rigid, reliable fixation. TTC nails are also load sharing constructs, which makes the fracture site more amenable to earlier weight-bearing after injury.
Beyond mechanics, hindfoot nails preserve fracture biology. The minimally invasive application of TTC nails limits the potential for iatrogenic wound complications. Co-morbid hosts and/or severe injuries associated with soft tissue compromise benefit from the limited operative exposure required for nail insertion. Furthermore, reaming a path for the nail generates cancellous autograft, which is beneficial for fracture and/or arthrodesis union.
Hindfoot Nailing Without an Intent to Fuse
When using a tibio-talar calcaneal nail in the treatment of fractures and/or dislocations of the hindfoot or distal tibia, a decision needs to be made as to whether a formal fusion of the spanned joints is necessary. A fusion is typically required for young and/or active patients, to avoid hardware failure. Further, successful fusion will promote best outcomes in these higher demand patients.
In geriatric and/or low-demand patients, a formal joint preparation may be unnecessary for acceptable results [6•]. Hindfoot nailing without a joint preparation has been performed with a high success and return to function rate in these hosts following malleolar and distal tibial fragility injuries. Hardware failure has not been found to be a significant complication in this minimally ambulatory patient population [7•].
Arthrodesis Using a Tibio-talar Calcaneal Nail
Joint-preserving reconstruction using internal and/or external fixation is the preferred operative care plan for younger patients with fractures and/or dislocations that involve the ankle and/or subtalar joints [20]. A primary arthrodesis, however, does have a significant role in the surgeon’s treatment armamentarium, particularly in the setting of severe profound irreversible cartilage injury. These cases will rapidly progress to arthrosis following conventional management. An acute fusion therefore merits consideration.
The degree of joint damage is typically a marker for the severity of concomitant soft tissue compromise. In an effort to limit surgical dissection while still promoting alignment and immobilization, a hindfoot nail can be used as a primary fusion modality. Joint preparation is recommended in addition to nail insertion. In contrast to the low-demand geriatric patient, a young, active patient will typically have pain and dysfunction if the ankle joint does not fuse. Further, this population will likely go on to hardware failure in the absence of a successful arthrodesis due to cyclic loading on the retained implant (Fig. 2).
Fig. 2.

a Active elderly female s/p open ankle fracture/dislocation with significant irreversible cartilage injury as demonstrated in the clinical photo (a) and presentation radiograph. (b) Hindfoot nail placed with percutaneous method (c) after open fracture care and fracture reduction. Joint preparation performed though traumatic wound. Medial malleolus excised to promote primary healing of traumatic wound (d, e). Patient achieved a pain free extremity and returned to pre-injury function
Adjunctive Techniques Used with a TTC Fusion Strategy
Diverse injury patterns and host characteristics mandate an individualized operative plan for patients who present with a severe trauma to the distal tibia and hindfoot. The goals of hindfoot nail-mediated reconstruction include the avoidance of deformity and the creation of a union across the fracture site and selected joint surfaces. When performing a primary arthrodesis with a hindfoot nail, adjunctive techniques are often useful to supplement the biomechanical milieu.
Limited ORIF in conjunction with the passage of a hindfoot nail after severe tibial pilon fractures is intended to grossly align/compress the major fracture fragments of the distal tibia and/or hindfoot, thereby restoring the patient’s native osseous anatomy and encouraging union. Minimally invasive approaches are typically used for fracture reduction and instrumentation. Lag screws with or without low-profile plates are typically employed for this application. For example, major fragments, including the Chaput, Volkmann, and medial tibial plafond segments, can be grossly aligned and instrumented with a limited form of internal fixation, followed by the removal of the remaining cartilage prior to hindfoot nail passage in an effort to encourage optimal alignment, primary arthrodesis, and fracture healing.
Supplemental internal fixation should also be considered across prepared joint surfaces to encourage an uneventful fusion. Large fragment, partially threaded cannulated screws are often used to compress the joint surface. Screws are strategically placed to avoid the path of the hindfoot nail. Trans-articular low-profile plates can also be used to impart rigidity and bone/joint healing across the fusion mass [21].
Biologic supplementation may also be used as part of the patient’s individualized care plan. Autogenous cancellous bone graft should be considered in the setting of fractures and/or joint surfaces with bone defects. Structural autograft may also be utilized to this end [22], which may involve the decortication and transfer of the distal fibula to the lateral distal tibia/talus (Fig. 3) [23]. This biologic plate will also impart early stability to the fusion construct as it incorporates into the fusion mass.
Fig. 3.

Hindfoot nail combined with limited ORIF and distal fibula transfer utilized for obtaining fracture union and ankle arthrodesis for severe open pilon fracture
Outcomes Using the TTC Nail for Acute Trauma
Hindfoot nailing is an acceptable treatment alternative for the infirm, low-demand geriatric patient with unstable periarticular ankle fracture/dislocations. TTC nailing may also be chosen when conventional methods of internal and/or external fixation are deemed unreliable. Multiple outcome studies have validated the safety and efficacy of acute TTC nailing of fragility fractures in low-demand hosts.
Jonas et al. [6•] selectively treated 31 primarily geriatric unstable ankle fractures with a hindfoot nail and early mobilization. Encouraging results were reported, as 94% of patients returned to their pre-injury level of function. However, complications included three periprosthetic fractures and two broken nails, prompting others to hypothesize that longer nails that bypassed the isthmus of the tibia were necessary to prevent periprosthetic complications [4•, 7•].
Al-Nammari [7•] described a case series of 48 infirm elderly patients with a mean age of 82 treated for unstable ankle fractures with a long talocalcaneal nail applied through the calcaneus, bridging the subtalar and ankle joints without formal joint preparation. Early weight-bearing was encouraged. Ninety percent of patients returned to their pre-injury functionality. No nail breakages or periprosthetic fractures were reported, which the authors attributed to the use of a long TTC nail.
Georgiannos et al. [8••] performed a prospective randomized study comparing TTC nailing and traditional open reduction internal fixation (ORIF) in the management of malleolar, unstable ankle trauma in geriatric patients. Postoperative complications were four-fold higher in the ORIF group. While the functional outcomes of both groups were equivalent, as measured by the Olerud Molander Ankle Score.
TTC nailing must be used more cautiously in the younger, active patient, as a joint-preserving reconstruction is more advantageous in these hosts. Hindfoot nailing, however, has been successfully employed after the most severe bone, joint, and soft tissue injuries and in the sickest hosts to promote limb salvage (Fig. 4). Unfortunately, the body of literature that supports using TTC nails in the treatment high-energy trauma is more limited, consisting of a small case series and case reports, highlighting the very selective nature of this technique in the active patient population [10–14].
Fig. 4.
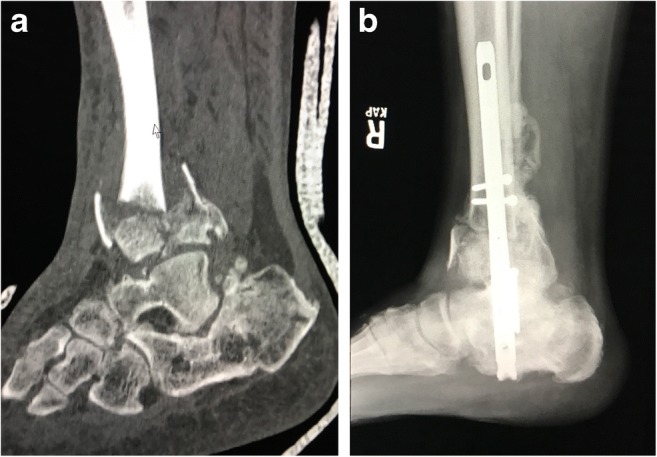
a 55-year-old polytrauma patient with history of smoking with new type C3 pilon fracture. His past history is significant for symptomatic arthrosis of ankle and subtalar joints from previous calcaneous malunion as seen on sagittal CT scan. b Arthrodesis of both tibio-talar and subtalar joints and fracture fixation with TTC nail resulting in best outcomes for this complex hindfoot injury
Al-Ashhab [10] reported on hindfoot nailing with formal joint preparation for 20 consecutive severe high-energy tibial pilon fractures deemed unreconstructable by the author in a relatively young patient cohort, with an average age of 33. The author in all cases performed a distal fibulectomy, which was used as autograft to facilitate joint preparation and serve as an adjunct for fusion. Unions were observed in all cases, with 90% of fractures deemed to be in an acceptable alignment. Good outcome scores (average 85) according to the AOFAS were reported despite unnecessary immobilization of the subtalar joint.
Additional reports describe the successful salvage of high-energy traumatic injuries using a retrograde hindfoot nail [11–14]. Co-morbid hosts can achieve a viable limb reconstruction using this method, as conventional strategies can be fraught with unacceptable iatrogenic complications. Patients with talus fracture/dislocations or frank extrusions are also potential candidates for TTC nail reconstruction (Fig. 5). Mangled extremities with injuries to the tibial plafond, talus, and/or calcaneous can also be considered for this method. Lastly, fracture/dislocations associated with a severe soft tissue injury may benefit from rigid hindfoot stabilization to stop the cycle of injury, permitting soft tissue recovery in the setting of a concomitant reconstruction.
Fig. 5.
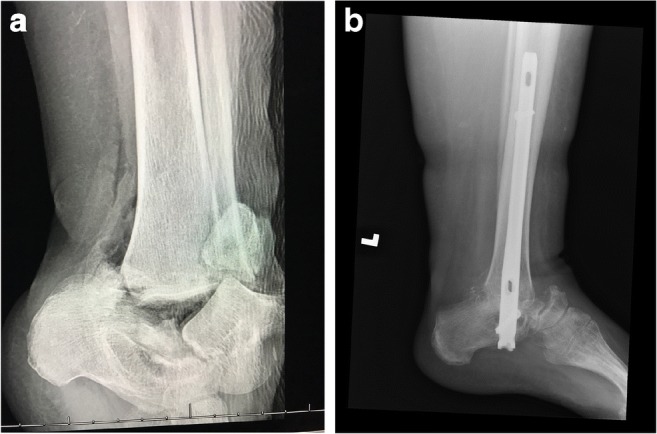
a Supermorbid elderly obese female polytrauma patient with diabetes and peripheral vascular disease with open grossly contaminated talus extrusion. Talus without meaningful vascular attachment. b Talectomy and fusion performed for limb salvage with hindfoot nail. Shortening of the hindfoot allowed for primary wound closure of the transverse wound and uneventful soft tissue healing
Conclusion
Tibio-talar calcaneal nailing is a minimally invasive strategy for effectively stabilizing the hindfoot and distal tibia. It should be utilized in selected patients based on clinical judgment, which should include the consideration of both host and injury pattern. Hindfoot nailing is optimally indicated for the minimal demand, elderly patient with unstable peri-articular ankle trauma, as it permits early weight-bearing in these patients. Indications for this technique in the younger, active patient population should be made on a case-by-case basis, and should be reserved as a salvage tool for only the most complex injuries.
Conflict of Interest
Both authors declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Foot and Ankle Trauma
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Rammelt S, Pyrc J, Agren PH, Hartsock LA, Cronier P, Friscia DA, Hansen ST, Schaser K, Ljungqvist J, Sands AK. Tibiotalocalcaneal fusion using the hindfoot arthrodesis nail: a multicenter study. Foot Ankle Int. 2013;34(9):1245–1255. doi: 10.1177/1071100713487526. [DOI] [PubMed] [Google Scholar]
- 2.Loosen S, Preuss S, Zelle BA, Pape HC, Tarkin IS. Multimorbid patients with poor soft tissue conditions: treatment of distal tibia fractures with retrograde intramedullary nailing. Unfallchirurg. 2013;116(6):553–558. doi: 10.1007/s00113-012-2244-6. [DOI] [PubMed] [Google Scholar]
- 3.•.Lemon M, Somayaji HS, Khaleel A, Elliott DS. Fragility fractures of the ankle: stabilisation with an expandable calcaneotalotibial nail. J Bone Joint Surg Br. 2005;87(6):809–813. doi: 10.1302/0301-620X.87B6.16146. [DOI] [PubMed] [Google Scholar]
- 4.•.Amirfeyz R, Bacon A, Ling J, Blom A, Hepple S, Winson I, et al. Fixation of ankle fragility fractures by tibiotalocalcaneal nail. Arch Orthop Trauma Surg. 2008;128(4):423–8. Thirteen patients were treated with either a long humeral nail or a short TTC fusion nail through the same approach. All patients returned to their baseline function regardless of the hardware used, and radiographic analysis showed fracture union in all cases. Findings reinforced that the benefits of TTC nailing, early weight-bearing, and fewer complications outweighed the stiffness that resulted from the joint immobilization in the geriatric population. [DOI] [PubMed]
- 5.•.Fourman MS, Tarkin IS. Retrograde tibiotalocalcaneal hindfoot nail without joint preparation is a viable salvage technique for geriatrics with extensive comorbidities and minimal ambulatory status following major trauma Proceedings of the American Academy of Orthopaedic Surgery Annual Meeting; Orlando, FL; March 2017. Here, we describe our institutional experience with acute TTC nailing following orthopedic trauma, which included a total of 18 patients treated after high- and low-energy injuries. Joint preparation was only performed in those patients whose traumatic wounds permitted access. Despite a significantly co-morbid population (mean Charlson Index 3.9) and a high percentage (22.2%) of high-energy trauma, limb preservation was possible in 88.9% of patients, and 83.3% were able to return to weight-bearing as tolerated.
- 6.•.Jonas SC, Young AF, Curwen CH, McCann PA. Functional outcome following tibio-talar-calcaneal nailing for unstable osteoporotic ankle fractures. Injury. 2013;44(7):994–997. doi: 10.1016/j.injury.2012.11.008. [DOI] [PubMed] [Google Scholar]
- 7.•.Al-Nammari SS, Amin A, Nielsen D. Fragility fractures of the ankle in the frail elderly patient: treatment with a long calcaneotalotibial nail. Bone Joint J. 2014;96-B(6):817–822. doi: 10.1302/0301-620X.96B6.32721. [DOI] [PubMed] [Google Scholar]
- 8.Georgiannos D, Lampridis V, Bisbinas I. Fragility fractures of the ankle in the elderly: open reduction and internal fixation versus tibio-talo-calcaneal nailing: short-term results of a prospective randomized-controlled study. Injury. 2017;48(2):519–524. doi: 10.1016/j.injury.2016.11.017. [DOI] [PubMed] [Google Scholar]
- 9.Ho B, Ketz J. Primary arthrodesis for tibial pilon fractures. Foot Ankle Clin. 2017;22(1):147–161. doi: 10.1016/j.fcl.2016.09.010. [DOI] [PubMed] [Google Scholar]
- 10.Al-Ashhab M. Primary ankle arthrodesis for severely comminuted tibial pilon fractures. Orthopedics. 2017;40(2):e378–e381. doi: 10.3928/01477447-20161202-04. [DOI] [PubMed] [Google Scholar]
- 11.Ochman S, Evers J, Raschke MJ, Vordemvenne T. Retrograde nail for tibiotalocalcaneal arthrodesis as a limb salvage procedure for open distal tibia and talus fractures with severe bone loss. J Foot Ankle Surg. 2012;51(5):675–679. doi: 10.1053/j.jfas.2012.04.015. [DOI] [PubMed] [Google Scholar]
- 12.Hsu AR, Szatkowski JP. Early tibiotalocalcaneal arthrodesis intramedullary nail for treatment of a complex tibial pilon fracture (AO/OTA 43-C) Foot Ankle Spec. 2015;8(3):220–225. doi: 10.1177/1938640014548322. [DOI] [PubMed] [Google Scholar]
- 13.Mohammad HR, A’Court J, Pillai A. Extruded talus treated with reimplantation and primary tibiotalocalcaneal arthrodesis. Ann R Coll Surg Engl. 2017;99(4):e115–e117. doi: 10.1308/rcsann.2017.0042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jain NS, Lopez GD, Bederman SS, Wirth GA, Scolaro JA. Surgical management of complex lower-extremity trauma with a long hindfoot fusion nail: a case report. Foot Ankle Spec. 2016;9(4):354–360. doi: 10.1177/1938640015609982. [DOI] [PubMed] [Google Scholar]
- 15.Zelle BA, Gruen GS, McMillen RL, Dahl JD. Primary arthrodesis of the tibiotalar joint in severely comminuted high-energy pilon fractures. J Bone Joint Surg Am. 2014;96(11):e91. doi: 10.2106/JBJS.M.00544. [DOI] [PubMed] [Google Scholar]
- 16.Buckley R, Leighton R, Sanders D, Poon J, Coles CP, Stephen D, et al. Open reduction and internal fixation compared with ORIF and primary subtalar arthrodesis for treatment of Sanders type IV calcaneal fractures: a randomized multicenter trial. J Orthop Trauma. 2014;28(10):577–83. [DOI] [PubMed]
- 17.de Cesar Netto C, Johannesmeyer D, Cone B, Araoye I, Hudson PW, Sahranavard B, et al. Neurovascular structures at risk with curved retrograde TTC fusion nails. Foot Ankle Int. 2017;38(10):1139–45. [DOI] [PubMed]
- 18.Aigner R, Salomia C, Lechler P, Pahl R, Frink M. Relationship of prolonged operative time and comorbidities with complications after geriatric ankle fractures. Foot Ankle Int. 2017;38(1):41–48. doi: 10.1177/1071100716667315. [DOI] [PubMed] [Google Scholar]
- 19.Lee AT, Sundberg EB, Lindsey DP, Harris AH, Chou LB. Biomechanical comparison of blade plate and intramedullary nail fixation for tibiocalcaneal arthrodesis. Foot Ankle Int. 2010;31(2):164–171. doi: 10.3113/FAI.2010.0163. [DOI] [PubMed] [Google Scholar]
- 20.Tarkin IS, Clare MP, Marcantonio A, Pape HC. An update on the management of high-energy pilon fractures. Injury. 2008;39(2):142–154. doi: 10.1016/j.injury.2007.07.024. [DOI] [PubMed] [Google Scholar]
- 21.Tarkin IS, Mormino MA, Clare MP, Haider H, Walling AK, Sanders RW. Anterior plate supplementation increases ankle arthrodesis construct rigidity. Foot Ankle Int. 2007;28(2):219–223. doi: 10.3113/FAI.2007.0219. [DOI] [PubMed] [Google Scholar]
- 22.Popelka V, Zamborský R. Tibio-calcaneal arthrodesis with vertically placed tricortical bone graft after traumatic talar extrusion—a case report. Acta Chir Orthop Traumatol Cechoslov. 2017;84(6):462–465. [PubMed] [Google Scholar]
- 23.Watanabe K, Teramoto A, Kobayashi T, Ogon I, Sakakibara Y, Kamiya T, et al. Tibiotalocalcaneal arthrodesis using a soft tissue-preserved fibular graft for treatment of large bone defects in the ankle. Foot Ankle Int. 2017;38(6):671–6. [DOI] [PubMed]