

Abstract
A growing number of studies have explored EUS-guided vascular catheterization due to the relative proximity of the gastrointestinal tract to the major blood vessels of the mediastinum and abdomen. In particular, EUS-guided access of the portal vein (PV) may be favorable given the relative difficulty of PV access through standard percutaneous routes. Two major diagnostic applications of EUS-guided vascular access include angiography and assessment of intravascular pressure. This review will outline the different devices and techniques employed to obtain angiographic visualization and/or direct pressure measurements of the portal circulation. Ease of access, safety, and important lessons learned from each approach will be highlighted.
Keywords: EUS, hepatic venous portal gradient, portal vein angiography, portal vein manometry, portal venous pressure
INTRODUCTION
A growing number of studies have explored EUS-guided vascular catheterization due to the relative proximity of the gastrointestinal tract to the major blood vessels of the mediastinum and abdomen and the use of Doppler during EUS to ensure the absence of hemorrhage with needle puncture and withdrawal without additional administration of ionizing radiation. In particular, EUS-guided access to the portal vein (PV) may be favorable given the relative difficulty of PV access through standard percutaneous routes. Two major diagnostic applications of EUS-guided vascular access include angiography and assessment of intravascular pressure. This review will outline the different devices and techniques employed to obtain angiographic visualization and/or direct pressure measurements of the portal circulation. Ease of access, safety, and important lessons learned from each approach will be highlighted.
EUS-GUIDED PORTAL VENOUS ANGIOGRAPHY
The PV is well seen from both the stomach and the duodenum during EUS. The vessel itself is usually in very proximity to the tip of the echoendoscope, making this an ideal target for vascular access. Portal venous angiography is a modality to assess the anatomy of the hepatic vasculature. Initial cases of successful in vivo EUS-guided PV catheterization were performed in porcine models. In 2004, Lai et al. reported an EUS-guided transduodenal approach to access the extrahepatic PV in 21 swine with a 22G FNA needle. A small amount of contrast was injected through the needle for fluoroscopic confirmation of proper placement.[1] This study proved the feasibility on a technical level of EUS-guided PV access.
The first study solely assessing PV angiography was a porcine study reported in 2007 by Magno et al.[2] 19G, 22G, and 25G needles were inserted under EUS guidance into the celiac, splenic, superior mesenteric artery, the thoracic and abdominal aorta, and the splenic, portal, and hepatic veins (HVs). All vessels were successfully identified and punctured in five of five pigs. No signs of intraprocedural hemodynamic instability were observed. Immediate postprocedure necropsy showed no signs of injury with the 25G needle. The 22G needle left puncture marks without bleeding, and the 19G needle caused a vascular hematoma in large-caliber vessels with intra-abdominal bleeding in one of the five pigs. Injection of contrast provided good opacification of smaller vessels – the celiac trunk, splenic artery, and HVs – with only transient opacification in larger caliber vessels. As would be expected, the amount of resistance associated with instilling the iodinated contrast was inversely correlated with needle caliber.
Giday et al. attempted EUS-guided PV access in 2007 using a transgastric, transhepatic approach with a 25G needle and a modified ERCP catheter.[3] This protocol was again performed in 2008 as part of another PV catheterization study.[4] Angiography was achieved using both standard iodinated contrast and medical grade carbon dioxide (CO2). PV catheterization was achieved in six of six swine in 2007 and six of six swine in 2008, and no complications were noted in either study. Necropsy showed no evidence of bleeding, hematoma formation, or liver injury. The transgastric, transhepatic approach is postulated to be safer than the transduodenal approach by allowing for natural tamponade of the needle track by liver parenchyma during withdrawal.[3,5] The use of CO2 as a contrast medium allowed for better visualization of the PV as well as easier intravascular administration through the small-caliber FNA needle when compared to the viscous iodine-based contrast. These studies as a whole suggested that needle puncture of these vessels would not necessarily lead to intra-abdominal hemorrhage or vascular injury.
The safety of CO2 use has been evaluated in both animals and humans. It is highly soluble and easily cleared by the lungs[6] and unlike iodinated contrast is not associated with nephrotoxicity or increased risk for hepatorenal syndrome.[7] The current data suggest that combining CO2 with a 25G needle may allow for easier injection of contrast, adequate visualization of the portal circulation and possibly decreased risk of needle- and contrast-related complications.
EUS-GUIDED PORTAL PRESSURE GRADIENT MEASUREMENT
Portal hypertension (PH), resulting from increased resistance of hepatic sinusoids to blood flow, is most commonly a complication of liver cirrhosis. The pathogenesis involves alteration of the liver vasculature due to fibrosis as well as increased production of vasoconstrictive mediators relative to endogenous vasodilators. Complications of PH include esophageal varices, portal hypertensive gastropathy, ascites, and hepatorenal syndrome. Measurement of PH has been useful in determining the stage, progression, and prognosis of cirrhosis in individual patients. Portal pressure gradient (PPG) measurement of ≥10 mmHg is associated with development of esophageal varices[8] and PPG of ≥12 mmHg with variceal hemorrhage.[9] Reduction of PPG by 20% or to below 12 mmHg with pharmacotherapy has been found to decrease risk of future bleeding or rebleeding episodes.[10,11]
Previously, PPG values were obtained directly through either a percutaneous approach or using a transjugular intrahepatic portosystemic shunt. The current standard for evaluation of PH is indirect measurement of the hepatic venous pressure gradient (HVPG). In this technique, a catheter is inserted into the HV percutaneously through either the jugular or femoral vein. The free hepatic venous pressure is recorded and subtracted from the wedged hepatic venous pressure to determine the HVPG. Both percutaneous PV catheterization and HVPG measurement are invasive procedures and require a high level of technical expertise. Direct PV catheterization has been associated with a high complication rate[12,13] and is not commonly performed. Despite the overall safety profile of HVPG measurement, it is only routinely performed at tertiary medical centers.[14,15] Furthermore, HVPG has been shown to correlate poorly with directly measured portal pressure in cases of presinusoidal PH, which may be seen in cases of noncirrhotic portal fibrosis and presinusoidal PH, including PV thrombosis and schistosomiasis.[4,16,17]
Animal studies
Lai et al. were the first to report EUS-guided PV pressure (PVP) measurement in a porcine model.[1] In a cohort of 21 pigs, a PH model was generated in 14 animals using polyvinyl alcohol injection and a coagulopathy model generated in 7 animals with heparin administration. A transduodenal EUS approach was used to access the PV in 21 pigs with a 22G FNA needle and a transabdominal ultrasound-guided transhepatic approach in 14 of 21 pigs through a 22G needle. PVP measurements were obtained in 18 of 21 swine. Minor complications found at necropsy included small subserosal hematomas at the EUS puncture site in all 21 pigs and a 25 mL blood collection between the liver and duodenum in 1 of 7 anticoagulated pigs. Failure to measure pressures in three subjects may have occurred due to thrombosis within the FNA needle. There was a strong correlation between EUS- and transhepatic-measured PVP (r = 0.91). The development of hematomas in this study suggests that a transduodenal approach that does not traverse the liver may increase risk of bleeding, and therefore, an approach traversing through liver parenchyma may be favorable.
In 2007, Giday et al. used the transgastric approach with a 19G needle and modified ERCP catheter to obtain continuous PVP measurement without an echoendoscope in place.[3] Five of five pigs were successfully catheterized, and no hemorrhage or liver injury was noted on necropsy in all subjects despite the use of a significantly larger caliber needle. Two of five pigs were survived for 2 weeks and exhibited no signs of adverse events before and after necropsy. In a later study, the same group used the same methods to measure fluctuations in PVP and inferior vena cava (IVC) pressures in pigs that underwent common endoscopic procedures: esophagogastroduodenoscopy (EGD), colonoscopy, and ERCP.[18] PV and IVC were accessed using a 19G needle and modified ERCP catheter. Access and pressure measurements of both vessels were achieved in five of five pigs. Necropsy showed no evidence of injury in all subjects. A threefold increase in PVP was noted between baseline and during ERCP. Values of IVC pressure, as well as of PVP for EGD and colonoscopy, were similar between baseline and procedure time.
Schulman et al. demonstrated a novel method of measuring PVP in 2016 using an EUS-guided 22G needle through which a wire with a digital pressure sensor was passed.[19] Conventional transjugular catheterization was performed as a control. Successful device placement and PVP measurement were achieved in five of five pigs with no hemorrhage or thrombosis noted on both EUS and postprocedural necropsy. Comparison of EUS-measured PVP with transjugular HVPG measurements showed a difference of within 1 mmHg for all pigs. The study endoscopists rated the procedure as having overall low subjective workload. The authors used the same device to perform PVP measurement in five other pigs that were then survived for 14 days before necropsy.[20] PVP was again measured on day 14. No signs of complications were observed during the 2-week survival period, and necropsy again showed no abnormalities. PVP values on days 0 and 14 were similar for all five pigs.
Our group developed a method of EUS-guided portal pressure measurement using a 25G needle and simple transducer setup. The apparatus for PPG measurement included a linear echoendoscope, a 25G FNA needle, and a compact manometer [Figure 1] with noncompressible tubing.[21] Before echoendoscope insertion, the manometer was zeroed at the midaxillary line. Measurements were conducted in the PV, HV, and IVC. When the PV was targeted, manometry was performed through a transgastric and less often a transduodenal, transhepatic approach and only the intrahepatic portion near the PV bifurcation was accessed [Figure 1]. When evaluating the HV, the needle tip was placed 2 cm distal to the ostia where possible. Needle placement was meticulous to ensure consistency. One milliliter of heparinized saline was flushed through the needle before pressure measurement to clear the needle lumen and confirm intravascular placement. We also measured pressures in a swine model of PH induced by dextran-40 administration. Percutaneous measurements in the same vessels were obtained for comparison. All vessels were successfully accessed and pressures measured through EUS in all three pigs. Necropsy was not performed, but intraprocedural monitoring showed no signs of cardiorespiratory instability. Correlations between EUS-guided and percutaneous pressure measurements were very strong, with R values in all vessels ≥0.985.
Figure 1.
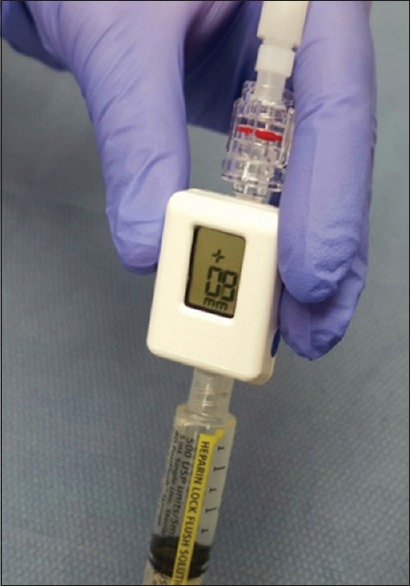
Compact manometer used for EUS-guided portal pressure measurement (Cook Medical, Bloomington, IN)
Human studies
The first human single case of EUS-guided PVP measurement was reported by Fujii-Lau et al. in 2014, in which a 22G FNA needle connected to an arterial pressure catheter was used to rule out PH in a 27-year-old man with arteriovenous malformations secondary to Noonan syndrome. The measured PPG was 1 mmHg and correlated with the gradient obtained by interventional radiology at a prior procedure. There was no evidence of bleeding or hemodynamic instability after this procedure.[22]
Our group performed the first prospective pilot study of PPG measurement in human patients with suspected or confirmed cirrhosis.[23] The setup employed the simple transducer setup discussed above with our animal study. The compact manometer was zeroed at the midaxillary line of each patient, and care was taken to consistently place the needle 2 cm distal to the HV ostia. Pressure readings were taken of the PV and either the HV or the IVC if anatomy was unfavorable for HV access. Needle placement was achieved and PPG measurement obtained in 28 of 28 patients, and no adverse events including bleeding, perforation, or infection were noted. The time required to obtain pressure measurements was short, under 30 min per patient. PPG measurements correlated well with clinical and endoscopic parameters with significant differences in PPG noted in patients that were high-risk vs. low-risk for cirrhosis and in patients with esophageal varices, portal hypertensive gastropathy, and thrombocytopenia relative to patients without these conditions. There were no complications in any of the 28 patients. In addition, the majority of the patients in this study had EUS-guided liver biopsies performed at the same procedure, suggesting that combining a PPG measurement and liver biopsy in the same session should be safe.
EUS-GUIDED PORTAL PRESSURE GRADIENT MEASUREMENT TECHNIQUE
The EUS manometry apparatus used in our human study is a simple setup that includes a 25G FNA needle, noncompressible tubing, a compact digital manometer, and heparinized saline [Videos 1 and 2]. The tubing is connected by a luer lock to the distal port of the manometer, while the heparinized saline is connected the proximal port. The end of the tubing is connected through a luer lock to the inlet of the 25G needle. The patient is positioned supine, and during EUS guided pressure measurement reading, the manometer is placed at the patient's midaxillary line [Figure 2]. We prefer monitored anesthesia care or general anesthesia for this procedure.
Figure 2.

EUS-guided portal pressure measurement apparatus showing noncompressible tubing attached to the FNA needle inlet (right pane) and compact manometer being placed at the midaxillary line of the patient (left pane)
The HV measurement is conducted first. Of the HVs, the middle HV is targeted most commonly due to its larger caliber and better alignment with the needle trajectory on linear EUS [Figure 3]. Doppler flow is used to confirm the typical multiphasic waveform of hepatic venous flow [Figure 4]. Using the 25G FNA needle, a transgastric transhepatic approach is used to puncture the HV. Approximately 1 cc of heparinized saline is used to flush the needle which is visible on EUS confirming good position within the vessel. Following the flush, the pressure reading on the manometer will immediately rise and then fall and equilibrate at a steady pressure which is recorded. This measurement should be repeated second and third time to minimize any error or fluctuation and to give a range of pressures from which to derive a mean pressure. The mean of the three pressures is then considered the HV pressure. The FNA needle is slowly withdrawn from the vein into the liver parenchyma and then back into the needle sheath. The needle tract within the liver parenchyma is then observed with Doppler flow on to ensure there is no flow within the needle tract.
Figure 3.
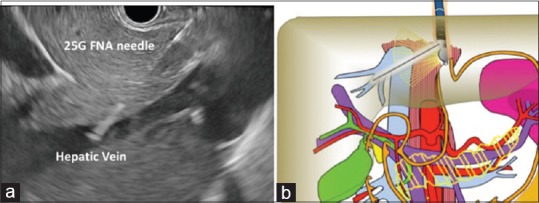
EUS image of needle puncture of middle hepatic vein with 25G FNA needle (a – ultrasound image; b – diagram)
Figure 4.
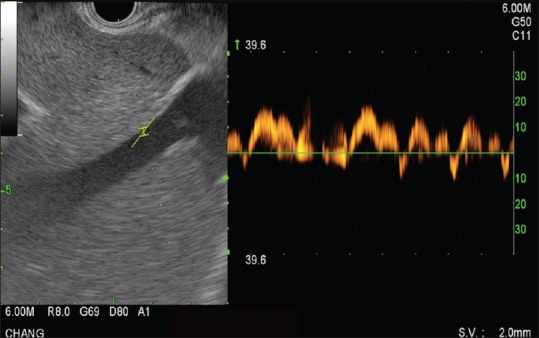
EUS Doppler flow image of middle hepatic vein demonstrating multiphasic waveform
The PV measurement is conducted next, and the umbilical portion of the left PV is targeted [Figure 5]. Doppler flow is used to confirm the typical venous hum of portal venous flow [Figure 6]. Using the 25G FNA needle, a transgastric transhepatic approach is used to puncture the PV. The procedure that follows is the same as what was performed for the HV. Approximately 1 cc of heparinized saline is used to flush the needle which is visible on EUS confirming good position within the vessel. Following the flush, the pressure reading on the manometer will immediately rise and then fall and equilibrate at a steady pressure which is recorded. This measurement should be repeated second and third time. The mean of the three pressures is then considered the PV pressure. The FNA needle is slowly withdrawn from the vein into the liver parenchyma and then back into the needle sheath. The needle tract within the liver parenchyma is then observed with Doppler flow on to ensure there is no flow within the needle tract.
Figure 5.
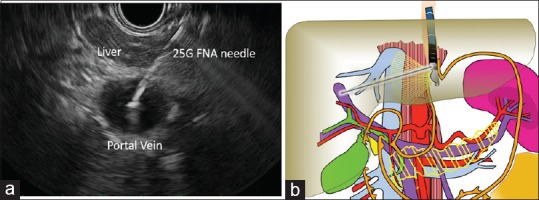
EUS image of needle puncture of left portal vein with 25G FNA needle (a – ultrasound image; b – diagram)
Figure 6.
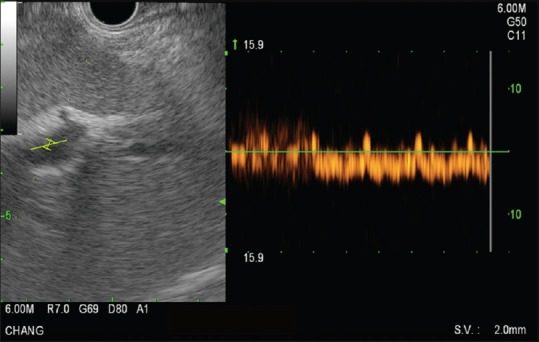
EUS Doppler flow image of left portal vein demonstrating typical waveform
The PPG is calculated by subtracting the mean PV pressure from the mean HV pressure. The patient is recovered in a similar manner to a routine diagnostic EUS with FNA. Postprocedural antibiotics are usually given for 5 days postprocedure.
CONCLUSION
Given the wide availability of EUS, an EUS-guided approach for the measurement of the PPG would be a great advance in the field of endo-hepatology. As we have just covered, the current literature suggests that EUS-guided measurement of the PPG is becoming safe and feasible. We look forward to the results of an international multicenter human trial using our recently designed manometry apparatus to further evaluate the safety and clinical utility of this approach for patients with liver disease.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initial will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos Available on: www.eusjournal.com
REFERENCES
- 1.Lai L, Poneros J, Santilli J, et al. EUS-guided portal vein catheterization and pressure measurement in an animal model: A pilot study of feasibility. Gastrointest Endosc. 2004;59:280–3. doi: 10.1016/s0016-5107(03)02544-6. [DOI] [PubMed] [Google Scholar]
- 2.Magno P, Ko CW, Buscaglia JM, et al. EUS-guided angiography: A novel approach to diagnostic and therapeutic interventions in the vascular system. Gastrointest Endosc. 2007;66:587–91. doi: 10.1016/j.gie.2007.01.011. [DOI] [PubMed] [Google Scholar]
- 3.Giday SA, Ko CW, Clarke JO, et al. EUS-guided portal vein carbon dioxide angiography: A pilot study in a porcine model. Gastrointest Endosc. 2007;66:814–9. doi: 10.1016/j.gie.2007.05.056. [DOI] [PubMed] [Google Scholar]
- 4.Giday SA, Clarke JO, Buscaglia JM, et al. EUS-guided portal vein catheterization: A promising novel approach for portal angiography and portal vein pressure measurements. Gastrointest Endosc. 2008;67:338–42. doi: 10.1016/j.gie.2007.08.037. [DOI] [PubMed] [Google Scholar]
- 5.Brugge WR. EUS is an important new tool for accessing the portal vein. Gastrointest Endosc. 2008;67:343–4. doi: 10.1016/j.gie.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 6.Hawkins IF, Caridi JG. Carbon dioxide (CO2) digital subtraction angiography: 26-year experience at the University of Florida. Eur Radiol. 1998;8:391–402. doi: 10.1007/s003300050400. [DOI] [PubMed] [Google Scholar]
- 7.Liss P, Eklöf H, Hellberg O, et al. Renal effects of CO2 and iodinated contrast media in patients undergoing renovascular intervention: A prospective, randomized study. J Vasc Interv Radiol. 2005;16:57–65. doi: 10.1097/01.RVI.0000144807.81633.79. [DOI] [PubMed] [Google Scholar]
- 8.Bosch J, Garcia-Pagán JC, Berzigotti A, et al. Measurement of portal pressure and its role in the management of chronic liver disease. Semin Liver Dis. 2006;26:348–62. doi: 10.1055/s-2006-951603. [DOI] [PubMed] [Google Scholar]
- 9.Groszmann RJ, Bosch J, Grace ND, et al. Hemodynamic events in a prospective randomized trial of propranolol versus placebo in the prevention of a first variceal hemorrhage. Gastroenterology. 1990;99:1401–7. doi: 10.1016/0016-5085(90)91168-6. [DOI] [PubMed] [Google Scholar]
- 10.Albillos A, Bañares R, González M, et al. Value of the hepatic venous pressure gradient to monitor drug therapy for portal hypertension: A meta-analysis. Am J Gastroenterol. 2007;102:1116–26. doi: 10.1111/j.1572-0241.2007.01191.x. [DOI] [PubMed] [Google Scholar]
- 11.D’Amico G, Garcia-Pagan JC, Luca A, et al. Hepatic vein pressure gradient reduction and prevention of variceal bleeding in cirrhosis: A systematic review. Gastroenterology. 2006;131:1611–24. doi: 10.1053/j.gastro.2006.09.013. [DOI] [PubMed] [Google Scholar]
- 12.Perelló A, Escorsell A, Bru C, et al. Wedged hepatic venous pressure adequately reflects portal pressure in hepatitis C virus-related cirrhosis. Hepatology. 1999;30:1393–7. doi: 10.1002/hep.510300628. [DOI] [PubMed] [Google Scholar]
- 13.Tsushima Y, Koizumi J, Yokoyama H, et al. Evaluation of portal pressure by splenic perfusion measurement using dynamic CT. AJR Am J Roentgenol. 1998;170:153–5. doi: 10.2214/ajr.170.1.9423623. [DOI] [PubMed] [Google Scholar]
- 14.Suk KT. Hepatic venous pressure gradient: Clinical use in chronic liver disease. Clin Mol Hepatol. 2014;20:6–14. doi: 10.3350/cmh.2014.20.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thalheimer U, Bellis L, Puoti C, et al. Should we routinely measure portal pressure in patients with cirrhosis, using hepatic venous pressure gradient (HVPG) as a guide for prophylaxis and therapy of bleeding and rebleeding?. No. Eur J Intern Med. 2011;22:5–7. doi: 10.1016/j.ejim.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 16.Sarin SK, Khanna R. Non-cirrhotic portal hypertension. Clin Liver Dis. 2014;18:451–76. doi: 10.1016/j.cld.2014.01.009. [DOI] [PubMed] [Google Scholar]
- 17.Pomier-Layrargues G, Kusielewicz D, Willems B, et al. Presinusoidal portal hypertension in non-alcoholic cirrhosis. Hepatology. 1985;5:415–8. doi: 10.1002/hep.1840050312. [DOI] [PubMed] [Google Scholar]
- 18.Buscaglia JM, Shin EJ, Clarke JO, et al. Endoscopic retrograde cholangiopancreatography, but not esophagogastroduodenoscopy or colonoscopy, significantly increases portal venous pressure: Direct portal pressure measurements through endoscopic ultrasound-guided cannulation. Endoscopy. 2008;40:670–4. doi: 10.1055/s-2008-1077341. [DOI] [PubMed] [Google Scholar]
- 19.Schulman AR, Thompson CC, Ryou M. EUS-guided portal pressure measurement using a digital pressure wire with real-time remote display: A novel, minimally invasive technique for direct measurement in an animal model. Gastrointest Endosc. 2016;83:817–20. doi: 10.1016/j.gie.2015.11.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schulman AR, Thompson CC, Ryou M. Endoscopic ultrasound-guided direct portal pressure measurement using a digital pressure wire with real-time remote display: A survival study. J Laparoendosc Adv Surg Tech A. 2017;27:1051–4. doi: 10.1089/lap.2017.0032. [DOI] [PubMed] [Google Scholar]
- 21.Huang JY, Samarasena JB, Tsujino T, et al. EUS-guided portal pressure gradient measurement with a novel 25-gauge needle device versus standard transjugular approach: A comparison animal study. Gastrointest Endosc. 2016;84:358–62. doi: 10.1016/j.gie.2016.02.032. [DOI] [PubMed] [Google Scholar]
- 22.Fujii-Lau LL, Leise MD, Kamath PS, et al. Endoscopic ultrasound-guided portal-systemic pressure gradient measurement. Endoscopy. 2014;46(Suppl 1):E654–6. doi: 10.1055/s-0034-1390845. [DOI] [PubMed] [Google Scholar]
- 23.Huang JY, Samarasena JB, Tsujino T, et al. EUS-guided portal pressure gradient measurement with a simple novel device: A human pilot study. Gastrointest Endosc. 2017;85:996–1001. doi: 10.1016/j.gie.2016.09.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.