

Abstract
Objectives: This work follows-up on a systematic review, published in 2017, of acupuncture for the treatment of mono- and polyneuropathy and associated symptoms. Previously reviewed trials of acupuncture for neuropathy primarily used acupuncture points in close proximity to underlying nerves. Further exploration of point selection for the treatment of each neuropathic condition is needed to assess the anatomical relationships between acupuncture points and peripheral nerves with respect to the treatment of neuropathy.
Methods: The 13 randomized controlled trials included in the original review studied acupuncture for neuropathy caused by diabetes, Bell's palsy, carpal tunnel syndrome (CTS), human immunodeficiency virus (HIV), and idiopathic causes. The present review reexamines all acupuncture points used, focusing on specific neuropathic condition treated. Anatomical diagrams are presented to highlight acupuncture points underlying the nerves' anatomical relationships. Each selected acupuncture point is reviewed in detail, including its Traditional Chinese Medicine theory–based function, the point's indications for use, and the peripheral nerve most closely associated with it.
Results: In Bell's palsy, the majority of selected acupuncture points were associated with the ipsilateral facial nerve. In CTS, the majority of the selected acupuncture points were closely associated with the median nerve and its branches. In polyneuropathy caused by diabetes, HIV, or idiopathic causes, most selected acupuncture points were in close proximity to peripheral nerves.
Conclusions: All reviewed trials of acupuncture for neuropathy and neuropathic pain use acupuncture points that are closely associated with the peripheral nerves treated. Local needling is crucial for successful treatment of peripheral neuropathy.
Keywords: : acupuncture, electroacupuncture, mononeuropathy, polyneuropathy, neuropathic pain, point selection
Introduction
In the last few decades there has been a surge in acupuncture research, with multiple evidence-based reviews showing therapeutic benefits of acupuncture for chronic low-back pain,1,2 migraine3 and tension headache,4 chemotherapy-induced nausea and vomiting5 and other conditions.6 The evidence for acupuncture in the treatment of peripheral neuropathy (PN) is emerging rapidly. PN is broadly defined as damage to the peripheral nervous system caused by a primary lesion or dysfunction.7 This includes polyneuropathy involving multiple nerves and mononeuropathy involving a single nerve. The most common causes of polyneuropathy are diabetes, thyroid disorders, vitamin B12 deficiency, alcohol abuse, chemotherapy, and human immunodeficiency virus (HIV) infection.7–9
This work is based on a 2017 summary of the evidence for acupuncture in the treatment of PN and associated symptoms, compared to sham acupuncture or conventional medical therapy.10 That article was the first systematic examination of the effectiveness of acupuncture for various types of neuropathy, including polyneuropathy and mononeuropathy. All successful randomized controlled trials (RCTs) that were selected and reviewed appeared to focus on points in close proximity to an underlying nerve. This prompted further investigation into acupuncture-point selection for the treatment of neuropathy.
For many decades, acupuncture practitioners and anatomists have attempted to correlate the location of acupuncture points to peripheral nerves, spinal segments, and spinal plexuses.11–17 This neuroanatomical theory of acupuncture suggests that acupuncture's effect is mediated via afferent input through the peripheral nervous system, eliciting a reflex at the level of the spinal cord via the sympathetic plexuses and via efferent input to the visceral organs and skeletal muscle.18,19 A closer examination of acupuncture-point selection in successful trials of PN could help explore further the connection between needle placement and effects on the underlying nerve.
Materials and Methods
The following databases were searched from their inceptions to July 2015: Medline,® Cochrane Library, Scopus, Clintrials.gov, AMED [Allied and Complementary Medicine Database], and CINAHL [Cumulative Index to Nursing and Allied Health Literature]. The key search terms used were acupuncture OR acup* OR laser acupuncture OR moxibustion OR electroacupuncture AND neuropathy OR peripheral neuropathy OR neuropathic pain OR neuralgia OR carpal tunnel syndrome OR Bell's palsy. Review articles were used to identify additional references. Language restrictions were set to English and subject restrictions were set to humans. Gray literature in Clintrials.gov was reviewed for unpublished relevant data.
Parallel and crossover RCTs were selected, if their focus was acupuncture as an intervention for the treatment of PN, regardless of blinding. RCTs were selected if they included at least 1 group receiving acupuncture and 1 control group receiving sham acupuncture or another active treatment (e.g., medication).10 All of the selected studies involved adult subjects (older than age 18) who underwent acupuncture, with or without electric stimulation, with or without moxibustion (heating with the mugwort (Artemisia spp. herb). Controls had to be active and included sham acupuncture or relevant medical treatments such as drugs or injections. Included trials had outcome measures such as nerve-conduction studies (NCS), validated questionnaires, or clearly defined study-specific objective criteria distinguishing responders from nonresponders.
Trials were reviewed for inclusion by 2 neurologists with expertise in acupuncture, neuromuscular disorders, neurophysiology, and statistical methodology. RCT methodological quality was assessed using the Scale for Assessing Scientific Quality of Investigations–Complementary and Alternative Medicine (SAS-QI CAM) version, an instrument specifically designed to evaluate RCTs focused on integrative therapies.20 It is used to assess methodological problems and sources of bias commonly encountered in integrative medicine research, such as allocation concealment, investigator- and subject-blinding, blinded outcome assessment, reproducibility of experimental procedures, and sound statistical analysis. The 2 reviewers assigned each article a SAS-QI CAM score independently and in a blinded fashion. As the 2 reviewers were in agreement, there was no need to use a third reviewer as a tiebreaker. Based on a recent study by D'Silva et al.,21 a SAS-QI CAM score of >9 (of 21) served as a cutoff for inclusion based on RCT overall scientific quality.
Results
After abstract reviews, 726 studies were excluded; 46 studies were reviewed in full; and 13 RCTs were included with a focus on acupuncture for the treatment of neuropathy caused by Bell's palsy,22,23 carpal tunnel syndrome (CTS),24–27 diabetes,28–31 HIV,32,33 and a combination of diabetes and idiopathic causes.34 Of the included RCTs, researchers in 9 studied manual acupuncture with or without moxibustion, in 3 studied electroacupuncture (EA), and in 1 studied a combination of manual and EA. Other active interventions included per os medications, intramuscular/intravenous injections, or splinting. As planned, each selected study had an active control arm.
Polyneuropathy Results
The included studies on diabetic PN reported significant improvements in acupuncture groups, compared to controls in neurologic examination,28,29,31 neuropathic symptoms, 28,30,31 composite improvement scales,28–31 NCS28,29 and blood rheology.28 One included study of acupuncture for HIV-related neuropathy32 showed significantly higher pain relief in an acupuncture group (P = 0.03); however, this was not true after adjustment for multiple comparisons. These data were reanalyzed by a different group of investigators,35 who found that amitriptyline alone or acupuncture alone produced significant reductions in Gracely Pain Scale scores at 6 weeks; however, only acupuncture sustained this effect at 14 weeks. The second study on acupuncture for HIV neuropathy33 also showed significant reductions in Gracely Pain Scale scores following a 6-week course of acupuncture/moxibustion, compared to a sham acupuncture/placebo moxibustion control. In addition, the acupuncture group had significant improvement on the Subjective Peripheral Neuropathy Screen, compared to the group's pretreatment baseline.
The 1 included study on idiopathic neuropathy34 included 4 subjects with diabetic neuropathy and 12 subjects with idiopathic neuropathy, in a double-blinded crossover study comparing EA versus sham EA (8 subjects per group). There was no difference between acupuncture and control treatments in any of the outcome measures used. In addition, both groups showed no difference from baseline. The researchers did not perform a separate analysis on subjects with idiopathic neuropathy.
Mononeuropathy Results
All four RCTs focused on CTS24–27 reported significant improvement with acupuncture, compared to baseline, in Global Symptom Score,24,27 Boston Carpal Tunnel Score,25 Carpal Tunnel Self-assessment Questionnaire,26 and a visual analogue scale.25 Three of the 4 RCTs included showed significantly greater effectiveness of acupuncture, compared to night splinting,25 sham acupuncture,24 oral vitamins B1 and B6,24 and oral prednisolone.27 In contrast, Yao et al.26 revealed no difference in CTS symptoms between acupuncture + night splinting, and sham acupuncture + night splinting, with both groups improved from baseline. Most long-term follow-ups favored acupuncture at 4 weeks,24,27 5 weeks,25 and 7 and 13 months,36 with only a single study showing no difference between acupuncture and control at 3 months.26
One of the RCTs on Bell's palsy22 showed significant improvement in the House–Brackmann Scale and Facial Disability Index in acupuncture and in the acupuncture + medical therapy groups, compared to a medical therapy group. In contrast, the second included RCT23 found no significant difference on the House–Brackmann Scale between an acupuncture group, compared to oral steroids and home exercise groups, as all 3 groups had high improvement rates.
Various methodological concerns were encountered and discussed as part of a critical appraisal of the evidence. These included problems with standardization of acupuncture regimens (points used, number of sessions, and follow-up periods), problems with control-treatment selection, problems with sample-size calculations, problems with subject and investigator blinding, problems involving the placebo effect and subject expectancy, and problems with outcome measures.
Adverse Events
Critical review of acupuncture safety and adverse events across trials led to the conclusion that acupuncture in the treatment of neuropathy was safe overall, without serious adverse events, except in the early study on HIV-related neuropathy,32 in which both groups experienced significant morbidity that was unrelated to acupuncture.
Acupuncture Point Selection
Only one of the 13 reviewed trials justified point selections.30 The reviewed RCTs used various acupuncture treatment courses in terms or number of sessions per week, session durations, total numbers of sessions, and the use of modalities such as EA and moxibustion (Table 1). While there were a wide variety of acupuncture points used across the trials, most acupuncture regimens included needling of local points, which have close anatomical associations with underlying nerves (Table 1).
Table 1.
Acupuncture Point Selection and Treatment Course
 |
 |
CTS, carpal tunnel syndrome: DPN, diabetic peripheral neuropathy; HIV, human immunodeficiency virus; IPN, idiopathic peripheral neuropathy; EA, electroacupuncture; IM, intramuscular; IV, intravenous; min, minutes
Discussion
For many decades, acupuncture practitioners and anatomists have attempted to correlate the location of acupuncture points to peripheral nerves, spinal segments, and spinal plexuses.11–17 This neuroanatomical theory of acupuncture suggests that acupuncture's effect is mediated via afferent input through the peripheral nervous system, eliciting a reflex at the level of the spinal cord via the sympathetic plexuses and via efferent input to the visceral organs and skeletal muscle.18,19 In the case of local needling in close proximity to a nerve, acupuncture's likely mechanism of action is direct mechanical stimulation, such as pressure on the perineural tissues by the needle in manual acupuncture or electrical current stimulation of the nerve with EA.
The neurophysiologic testing to support these theories is lacking so far, and further study on the local effects of acupuncture on the peripheral nervous system is needed. There is a consensus, however, that the nervous system is vital in processing the effects of acupuncture.
More so than polyneuropathy trials, the trials focused on Bell's palsy and CTS used local points that are closely associated with the facial nerve and the median nerve, respectively (Table 2). All included CTS trials involved points on the ipsilateral Pericardium meridian—PC 6,24,26,27 PC 7,24– 27 and PC 8.25 Pericardium meridian points are commonly used in CTS treatment due to their close association with the median nerve, which is affected in CTS (Fig. 1). The anatomical correlation between the acupuncture point PC 6 and the median nerve has been well-established, both in cadavers37 and in live subjects by using ultrasound,38,39 most strikingly with a documented case of the acupuncture needle piercing through the median nerve sheath, with absence of any symptoms in the subject.39
Table 2.
Acupuncture Point Summary by Neuropathic Condition
 |
 |
 |
HIV, human immunodeficiency virus; IV, intravenous.
Bold indicates neurological conditions.
FIG. 1.
Carpal tunnel syndrome points. Color images available online at www.liebertpub.com/acu
Similarly, both included Bell's palsy trials used ipsilateral points on the Stomach meridian—ST 2,23 ST 422,23 ST 6,22,23 and ST 7,22 as well as GB 14,22,23 which are in close proximity to branches of the facial nerve (Fig. 2). Both trials also included needling of bilateral LI 4, which is one of the most commonly used points for addressing headache and facial pain. The anatomical correlations between acupuncture points and the cranial nerves (facial nerve in particular) have been well-established.11,40 The local points used on the Stomach and Gall Bladder meridians are traditionally used for addressing facial pain and weakness (Table 2) and are closely related to various branches of the facial nerve (Fig. 2). These points are commonly used in acupuncture trials on Bell's palsy.18
FIG. 2.

Bell's palsy points. Color images available online at www.liebertpub.com/acu
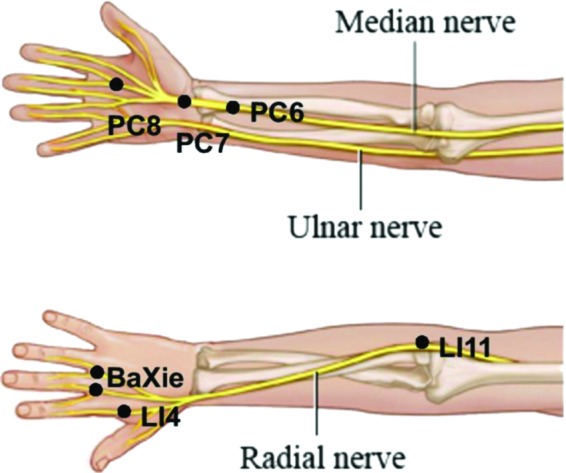
With respect to reviewed trials of polyneuropathy, the RCTs on acupuncture for diabetic, HIV-related, and idiopathic neuropathy used a greater variety of acupuncture points; however there were some underlying themes (Table 2). Points used were on the Large Intestine, Triple Energizer, Gall Bladder, Stomach, Bladder, Spleen, Kidney, and Liver channels, as well as the accessory points BaFeng (EX-LE 10) and BaXie (EX-UE 9). The points used in multiple trials of polyneuropathy were SP 6, SP 9, KI 3, BaFeng (EX-LE 10), and ST 36.
The majority of the used acupuncture points are in close anatomical correlation with distal nerves in the arm and leg (Figs. 3, 4, and 5) and each used point could be correlated to a large peripheral nerve or its branch. These correlations are known and have been explored before.13–16,40
FIG. 3.
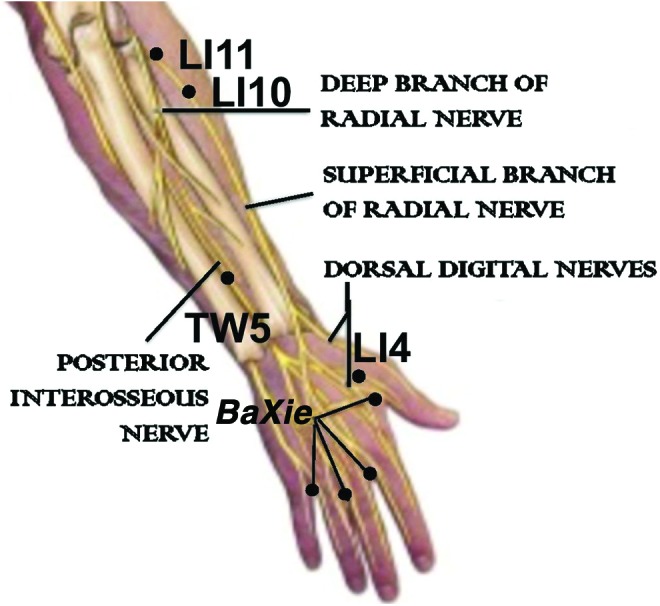
Polyneuropathy points in the arm. Color images available online at www.liebertpub.com/acu
FIG. 4.

Polyneuropathy points in the anterior leg. Color images available online at www.liebertpub.com/acu
FIG. 5.

Polyneuropathy points in the posterior leg. Color images available online at www.liebertpub.com/acu
Clinical Implications
The awareness that local needling is effective for addressing neuropathic conditions could guide point selection for points that are in close proximity with affected nerves in cases of mononeuropathy or for multiple points that allow needle proximity to large peripheral nerves in cases of polyneuropathy. This structural approach has led to the development of a standardized protocol for the treatment of PN, regardless of its etiology.41 While this approach is somewhat reductionist, it is well-suited for use by medical acupuncturists because of its neuroanatomical basis.
Conclusions
Much has been written about the anatomical correlations among acupuncture points, cranial nerves, and peripheral nerves. Close examination of acupuncture points used in trials of mono- and polyneuropathy confirms that the majority of selected acupuncture points overlie the pathways of the nerves implicated in the specific neuropathic conditions addressed. Future studies should explore the functional aspect of acupuncture point–nerve correlations, such as electrophysiologic measurements of changes in nerve function as direct result of needling.
Acknowledgments
This study was funded by the following grants: NIH K23 AT008405 (principal investigator: Dr. Dimitrova), NIH 5T32 AT002688 (principal investigator: Dr. Oken).
Author Disclosure Statement
No competing financial interests exist.
CME Quiz Questions
Article learning objectives:
After studying this article, participants should be able to identify some of the important research questions about acupuncture point use in treating neuropathic conditions and summarize some of the research on anatomical relationships of acupuncture points and peripheral nerves in the treatment of neuropathy.
Publication date: August 20, 2018
Expiration date: August 31, 2019
Disclosure Information:
Authors have nothing to disclose.
Richard C. Niemtzow, MD, PhD, MPH, Editor‐in‐Chief, has nothing to disclose.
Questions:
-
1.
Identify the incorrect statement
-
a.
The authors in this paper have conducted a multicenter trial evaluating the anatomical relationships of acupuncture points and peripheral nerves in the treatment of diabetic neuropathy.
-
b.
The method utilized in this paper is that of a systematic review of randomized controlled trials of acupuncture treatment for neuropathy.
-
c.
The RCTs in this review included neuropathies categorized as diabetic, Bell's Palsy, HIV, carpal tunnel, and idiopathic type.
-
d.
The authors emphasize acupuncture point and their anatomical relationship to underlying nerves rather than Traditional Chinese Medical theory.
-
e.
This paper includes RCTs for mono‐ and polyneuropathies.
-
a.
-
2. Identify the incorrect statement
-
a.
Neuroanatomical theory of acupuncture suggests that acupuncture's effect is mediated via afferent input through the peripheral nervous system, eliciting a reflex at the level of the spinal cord via the sympathetic plexuses and via efferent nerve fibers to the visceral organs and skeletal muscle.
-
b.
Peripheral neuropathy is generally defined as damage to the peripheral nervous system caused by a primary lesion or dysfunction of the nerve itself.
-
c.
The authors rely upon Traditional Chinese Medicine theory of channels and collaterals to explain acupuncture's use in the treatment of neuropathy.
-
d.
The most common causes of polyneuropathy are diabetes, thyroid disorders, Vitamin B 12 deficiency, alcohol abuse, chemotherapy, and HIV induced.
-
e.
Signs and symptoms of peripheral neuropathy may include gradual onset of numbness or tingling in the hands or feet, freezing or burning pain, extreme sensitivity to touch, lack of coordination and falling, and muscle weakness.
-
a.
-
3. Identify the incorrect statement
-
a.
The RCTs included on diabetic peripheral neuropathy reported significant improvement in acupuncture groups compared to control in neurologic exam, neuropathic symptoms, composite improvement scores, and blood rheology.
-
b.
The RCTs included in this review utilized various methods of acupuncture point stimulation including manual acupuncture, acupuncture with and without moxabustion, and electroacupuncture.
-
c.
Polyneuropathy studies included those of diabetic and HIV related type.
-
d.
RCTs on treatment of diabetic neuropathy with acupuncture did not demonstrate any benefit to neuropathic symptoms.
-
e.
The polyneuropathy trials analyzed commonly used the extra points Baxie (EX‐UE‐9) and Bafeng (EX‐LE‐10) in addition to points on the principal acupuncture channels.
-
a.
-
4. Identify the incorrect statement
-
a.
Review of these trials reports on safety and adverse effects suggest that acupuncture is safe in the treatment of neuropathies.
-
b.
Trials of the treatment of mono‐neuropathic conditions demonstrated an emphasis on local points related to the effected nerve.
-
c.
The authors analyzed RCTs of trials for Bell's Palsy and Carpal Tunnel Syndrome.
-
d.
The trials for Bell's Palsy most commonly used ipsilateral hand Yangming Stomach points such as ST4, ST6, ST7 and bilateral LI 4 Hegu.
-
e.
The acupuncture points used in the trial for Bell's Palsy are commonly known to be near the branches of the Occipital nerve.
-
a.
-
5. Identify the incorrect statement
-
a.
The acupuncture points commonly used for Bell's Palsy are closely related to the facial nerve.
-
b.
Trials for Carpal Tunnel Syndrome (CTS) routinely employed acupuncture points that have close association with the median nerve.
-
c.
Commonly employed points for CTS were ipsilateral hand Jueyin Pericardium channel points PC6, PC 7, and PC 8.
-
d.
The authors propose that for mono‐neuropathies, a structural approach of use of acupuncture points can be used to create simple but effective standardized treatment protocols.
-
e.
The authors propose that based on their systematic review Traditional Chinese Medicine theory is the suggested evidence‐based approach to treatment of neuropathies.
-
a.
Continuing Medical Education – Journal Based CME Objectives:
Articles in Medical Acupuncture will focus on acupuncture research through controlled studies (comparative effectiveness or randomized trials); provide systematic reviews and meta‐analysis of existing systematic reviews of acupuncture research and provide basic education on how to perform various types and styles of acupuncture. Participants in this journal‐based CME activity should be able to demonstrate increased understanding of the material specific to the article featured and be able to apply relevant information to clinical practice.
CME Credit
You may earn CME credit by reading the CME‐designated article in this issue of Medical Acupuncture and taking the quiz online. A score of 75% is required to receive CME credit. To complete the CME quiz online, go to http://www.medicalacupuncture.org/cme – AAMA members will need to login to their member account. Non‐members have the opportunity to participate for a small fee.
Accreditation: The American Academy of Medical Acupuncture is accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Designation: The AAMA designates this journal‐based CME activity for a maximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
References
- 1.Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: Acupuncture for low back pain. Ann Intern Med. 2005;142(8):651–663 [DOI] [PubMed] [Google Scholar]
- 2.Furlan AD, van Tulder M, Cherkin D, et al. . Acupuncture and dry-needling for low back pain: An updated systematic review within the framework of the Cochrane Collaboration. Spine (Phila Pa 1976). 2005;30(8):944–963 [DOI] [PubMed] [Google Scholar]
- 3.Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis. Cochrane Database Syst Rev. 2009;1:CD001218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for tension-type headache. Cochrane Database Syst Rev. 2009;1:CD007587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ezzo JM, Richardson MA, Vickers A, et al. . Acupuncture-point stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst Rev. 2006;2:CD002285. [DOI] [PubMed] [Google Scholar]
- 6.Vickers AJ, Cronin AM, Maschino AC, et al. . Acupuncture for chronic pain: Individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444–1453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Amato AA, Russell JA. Neuromuscular Disorders. New York: McGraw–Hill Medical; 2008 [Google Scholar]
- 8.Herskovitz S, Scelsa SN, Schaumburg HH. Peripheral Neuropathies in Clinical Practice. New York: Oxford University Press; 2010 [Google Scholar]
- 9.Martyn CN, Hughes RA. Epidemiology of peripheral neuropathy. J Neurol Neurosurg Psychiatry. 1997;62(4):310–318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dimitrova A, Murchison C, Oken B. Acupuncture for the treatment of peripheral neuropathy: A systematic review and meta-analysis. J Altern Complement Med. 2017;23(3):164–179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dung HC. Acupuncture points of the cranial nerves. Am J Chin Med. 1984;12(1–4):80–92 [DOI] [PubMed] [Google Scholar]
- 12.Dung HC. Acupuncture points of the cervical plexus. Am J Chin Med. 1984;12(1–4):94–105 [DOI] [PubMed] [Google Scholar]
- 13.Dung HC. Acupuncture points of the brachial plexus. Am J Chin Med. 1985;13(1–4):49–64 [DOI] [PubMed] [Google Scholar]
- 14.Dung HC. Acupuncture points of the lumbar plexus. Am J Chin Med. 1985;13(1–4):133–143 [DOI] [PubMed] [Google Scholar]
- 15.Dung HC. Acupuncture points of the sacral plexus. Am J Chin Med. 1985;13(1–4):145–156 [DOI] [PubMed] [Google Scholar]
- 16.Dung HC. Acupuncture points of the typical spinal nerves. Am J Chin Med. 1985;13(1–4):39–47 [DOI] [PubMed] [Google Scholar]
- 17.Bossy J. Morphological data concerning the acupuncture points and channel network. Acupunct Electrother Res. 1984;9(2):79–106 [DOI] [PubMed] [Google Scholar]
- 18.Cheng K. Neuroanatomical basis of acupuncture treatment for some common illnesses. Acupunct Med. 2009;27(2):61–64 [DOI] [PubMed] [Google Scholar]
- 19.Cheng K. Neuroanatomical characteristics of acupuncture points: Relationship between their anatomical locations and traditional clinical indications. Acupunct Med. 2011;29(4):289–294 [DOI] [PubMed] [Google Scholar]
- 20.Jeste D, Dunn L, Folsom D, et al. . Multimedia educational aids for improving consumer knowledge about illness management and treatment decisions: A review of randomized controlled trials. J Psychiatr Res. 2008;42(1):1–21 [DOI] [PubMed] [Google Scholar]
- 21.D'Silva S, Poscablo C, Habousha R, Kogan M, Kligler B. Mind–body medicine therapies for a range of depression severity [sic]: A systematic review. Psychosomatics. 2012;53(5):407–423 [DOI] [PubMed] [Google Scholar]
- 22.Li Y, Liang FR, Yu SG, et al. . Efficacy of acupuncture and moxibustion in treating Bell's palsy: A multicenter randomized controlled trial in China. Chin Med J (Engl). 2004;117(10):1502–1506 [PubMed] [Google Scholar]
- 23.Tong FM, Chow SK, Chan PY, et al. . A prospective randomised controlled study on efficacies of acupuncture and steroid in treatment of idiopathic peripheral facial paralysis. Acupunct Med. 2009;27(4):169–173 [DOI] [PubMed] [Google Scholar]
- 24.Khosrawi S, Moghtaderi A, Haghighat S. Acupuncture in treatment of carpal tunnel syndrome: A randomized controlled trial study. J Res Med Sci. Jan 2012;17(1):1–7 [PMC free article] [PubMed] [Google Scholar]
- 25.Kumnerddee W, Kaewtong A. Efficacy of acupuncture versus night splinting for carpal tunnel syndrome: A randomized clinical trial. J Med Assoc Thai. 2010;93(12):1463–1469 [PubMed] [Google Scholar]
- 26.Yao E, Gerritz PK, Henricson E, et al. . Randomized controlled trial comparing acupuncture with placebo acupuncture for the treatment of carpal tunnel syndrome. PM R. 2012;4(5):367–373 [DOI] [PubMed] [Google Scholar]
- 27.Yang CP, Hsieh CL, Wang NH, et al. . Acupuncture in patients with carpal tunnel syndrome: A randomized controlled trial. Clin J Pain. May 2009;25(4):327–333 [DOI] [PubMed] [Google Scholar]
- 28.Yu J, Cui Z. Clinical study of diabetic peripheral neuropathy treated by acupuncture. Int J Clin Acupunct. 2002;12(4):315–318 [Google Scholar]
- 29.Zuo L, Zhang L. Study on the effect of acupuncture plus methylcobalamin in treating diabetic peripheral neuropathy. J Acu Tuina Sci 2010;8(4):249–252 [Google Scholar]
- 30.Zhang C, Ma YX, Yan Y. Clinical effects of acupuncture for diabetic peripheral neuropathy. J Tradit Chin Med. 2010;30(1):13–14 [DOI] [PubMed] [Google Scholar]
- 31.Zheng HT, Li YF, Yuan SX. Observations on 52 patients with diabetic peripheral neuropathy treated by needling combined with [sic] drug. J Acu Tuina Sci. 2004;2(6):24–26 [Google Scholar]
- 32.Shlay JC, Chaloner K, Max MB, et al. . Acupuncture and amitriptyline for pain due to HIV-related peripheral neuropathy: A randomized controlled trial. Terry Beirn Community Programs for Clinical Research on AIDS. JAMA. 1998;280(18):1590–1595 [DOI] [PubMed] [Google Scholar]
- 33.Anastasi JK, Capili B, McMahon DJ, Scully C. Acu/moxa for distal sensory peripheral neuropathy in HIV: A randomized control pilot study. J Assoc Nurses AIDS Care. 2013;24(3):268–275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Penza P, Bricchi, Bricchi M, Scola A, Campanella A, Lauria G. Electroacupuncture is not effective in chronic painful neuropathies. Pain Med. 2011;12(12):1819–1823 [DOI] [PubMed] [Google Scholar]
- 35.Shiflett SC, Schwartz GE. Effects of acupuncture in reducing attrition and mortality in HIV-infected men with peripheral neuropathy. Explore (NY). 2011;7(3):148–154 [DOI] [PubMed] [Google Scholar]
- 36.Yang CP, Wang NH, Li TC, et al. . A randomized clinical trial of acupuncture versus oral steroids for carpal tunnel syndrome: A long-term follow-up. J Pain. 2011;12(2):272–279 [DOI] [PubMed] [Google Scholar]
- 37.Joo OH, Ko Y, Cho S, Yoon S. A cadaveric study of needle insertion at PC6 in eight wrists of four subjects and an understanding of the anatomy. Acupunct Med. 2012;30(1):44–46 [DOI] [PubMed] [Google Scholar]
- 38.Streitberger K, Eichenberger U, Schneider A, Witte S, Greher M. Ultrasound measurements of the distance between acupuncture needle tip at P6 and the median nerve. J Altern Complement Med. 2007;13(5):585–591 [DOI] [PubMed] [Google Scholar]
- 39.Kessler J, Streitberger K. Perforation of the median nerve with an acupuncture needle guided by ultrasound. Acupunct Med. 2008;26(4):231–233 [DOI] [PubMed] [Google Scholar]
- 40.Dung H. Acupuncture: An Anatomical Approach, 2nd ed. New York: Routledge; 2013 [Google Scholar]
- 41.Dimitrova A. Introducing a standardized acupuncture protocol for peripheral neuropathy: A case series. Med Acupunct. 2017;29(6):352–365 [DOI] [PMC free article] [PubMed] [Google Scholar]
References
To receive CME credit, you must complete the quiz online at: www.medicalacupuncture.org/cme