

Abstract
An updated meta-analysis incorporating nine randomized trials (n = 816) investigating low-to-moderate dose prolonged glucocorticoid treatment in acute respiratory distress syndrome (ARDS) show moderate-to-high quality evidence that glucocorticoid therapy is safe and reduces (i) time to endotracheal extubation, (ii) duration of hospitalization, and (iii) mortality (number to treat to save one life = 7), and increases the number of days free from (i) mechanical ventilation, (ii) intensive care unit stay, and (iii) hospitalization. Recent guideline suggests administering methylprednisolone in patients with early moderate-to-severe (1 mg/kg/day) and late persistent (2 mg/kg/day) ARDS (conditional recommendation based on moderate quality of evidence).
Keywords: Adult respiratory distress syndrome, Glucocorticoid treatment, Methylprednisolone, Dosage, Duration of treatment, Duration of mechanical ventilation, Tapering, Reconstituted systemic inflammation, Survival
Background
The English version of the clinical practice guidelines for the management of adult patients with ARDS (Japanese version publication July 2016) was recently published in the Journal of Intensive Care [1]. The recommendations are based on only five heterogeneous randomized controlled trials (RCTs) published before 2008. Four RCTs investigated methylprednisolone: one trial (1987) [2] administered 120 mg/kg over 24 h and the other (1998–2007) used 1 mg/kg/day in patients with early ARDS [3] or 2 mg/kg/day in patients with late ARDS [4, 5] over 4 weeks. The other trial investigated hydrocortisone and fludrocortisone over 7 days in patients with ARDS and vasopressor-dependent septic shock. The clinical practice guideline development (CPGD) committee concluded that there was no significant reduction in mortality, no increased risk for infection, and an increase in mechanical ventilation-free days (MVFD). The CPGD committee concluded that the overall quality of evidence across outcomes was “moderate” to suggest (GRADE 2B) the use of methylprednisolone in a dosage of 1 to 2 mg/kg/day. In addition, the CPGD committee referenced a 2014 domestic survey reporting the common practice among Japanese doctors of administering 500–1000 mg/day (pulse dose) of methylprednisolone to patients with ARDS. We wish to present a brief update of the literature and updated guidelines that might be of practical importance to clinicians.
Main body
Recent experimental [6] and clinical research [7, 8] suggest that pulse dose methylprednisolone may not be beneficial in ARDS. In an experimental study, rats with lipopolysaccharide-induced acute lung injury were exposed to graded concentrations of methylprednisolone (3 mg, 30 mg, 180 mg) for up to 14 days [6]. Serial BAL and lung histology demonstrated more significant improvements at 12 h in the higher dose group. However, by day 7, the high-dose group had partial loss of early laboratory improvements and significantly worsen pathological scores, while the lower dose group achieved continued improvement in both pathological and laboratory variables [6]. Similarly, data from two recent retrospective studies suggests that pulse dose steroids may be harmful [7, 8]. For example, in a retrospective comparison with low-dose methylprednisolone (0.5–1 mg/kg/day; n = 165), high-dose methylprednisolone (1000 mg/day for 3 days followed by 2 mg/kg/day) was associated with higher 60-day mortality and a 10-day reduction in ventilator-free days by day 28 [7].
A multi-specialty task force of international experts assembled by the Society of Critical Care Medicine and the European Society of Intensive Care Medicine recently published the updated guidelines for the diagnosis and treatment of Critical Illness Related Corticosteroid Insufficiency (CIRCI) [9]. In a separate document [10], the task force reviewed clinical and experimental evidence on the central role played by CIRCI in the pathobiology of ARDS and how increasing glucocorticoid receptorα (GRα) activation with quantitatively adequate and prolonged glucocorticoid supplementation can reverse CIRCI and accelerate resolution of pulmonary and systemic inflammation. The impact of methylprednisolone treatment on GRα number and function in patients with ARDS was also reviewed [11, 12]. For their recommendations, the task force relied mostly on a recent systematic review of RCTs investigating prolonged (7 days or greater) glucocorticoid treatment in ARDS [13]. This systematic review included a primary individual patient data meta-analysis (IPDMA) of four RCTs investigating methylprednisolone treatment (n = 322) [3–5, 14], and an aggregate data meta-analysis incorporating four additional RCTs [15–18] investigating hydrocortisone treatment in early ARDS (n = 297). There were substantial differences in the treatment protocol design. Data are presented as methylprednisolone vs. hydrocortisone: an initial bolus was used in 4 [3–5, 14] vs. 2 [15, 17]; duration of treatment was 24 to 32 days vs 7 days, and slow tapering of study drug was implemented in 3 [3, 4, 14] vs. none.
Individual patient data meta-analyses allow for time-to-event analyses and examination of new outcomes not previously reported (e.g., MV-free days and impact of tapering). By study day 28 (Fig. 1), fewer patients in the methylprednisolone group died before extubation (12% vs. 29%; p < 0.001) and more patients achieved extubation (80% vs. 50%; p < 0.001) and were discharged alive from the intensive care unit (75% vs 49%; p < 0.001). In the methylprednisolone group, time to extubation was shorter (hazard ratio 2.59, 95% CI 1.95–3.43, p < 0.001) and hospital mortality was lower (20% vs. 33%; p = 0.006). The results were similar in both the aggregate (eight studies) and individual patient meta-analyses (four studies). In addition, prolonged methylprednisolone treatment was associated with (i) increased MV-free days (13.3 ± 11.8 vs. 7.6 ± 5.7; p < 0.001), ICU-free days (10.8 ± 0.71 vs. 6.4 ± 0.85; p < 0.001), and hospital-free days to day 28 (7.0 ± 0.57 vs. 3.8 ± 0.68; p < 0.001), and a reduction in development of shock (3% vs. 15%; p < 0.001) and infections (32% vs. 41%; p = 0.001) after study entry. In the ARDS network RCT, rapid discontinuation of study drug after extubation was associated with return to mechanical ventilation for 26% of methylprednisolone-treated patients from reconstituted systemic inflammation in the presence of adrenal suppression [19]. Despite the partial loss of early benefits associated with return to mechanical ventilation, patients randomized prior to day 14 had a 25% [18 of 66 (27.3%) vs. 24 of 66 (36.4%); RR 0.75, CI 0.45 to 1.24] and 31% [18 of 66 (27.3%) vs. 26 of 66 (39.4%); RR 0.69, CI 0.42 to 1.13] relative reduction in 60-day and 180-day mortality, respectively [19].
Fig. 1.
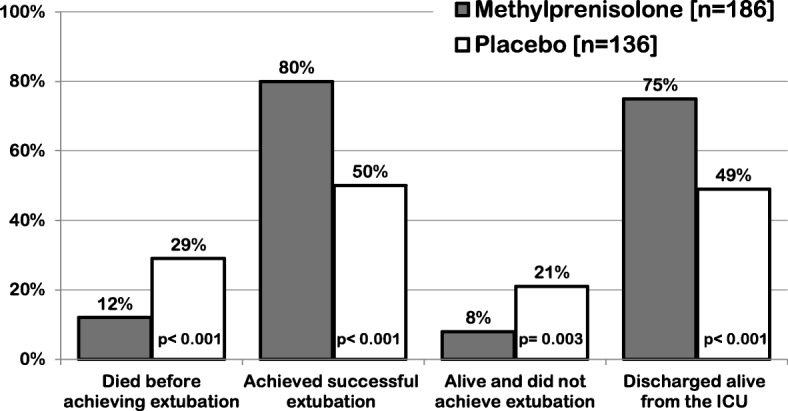
Individual patient data from four randomized trials investigating prolonged methylprednisolone treatment in ARDS [13]: outcome related to achieving extubation and intensive care unit discharge by day 28
During the consensus process, an additional RCT was published by Tongyoo et al. [20] (hydrocortisone 7 days, no bolus, no tapering) and incorporated in the final analysis of the nine trials (n = 816). Overall, glucocorticoid treatment was associated with reduction in MV-free days (mean difference 6.36 days, 95% CI 2.94–9.77; p < 0.001) and decreased hospital mortality for those randomized before day 14 of ARDS (Fig. 2, 28.2% vs. 42.5%, risk ratio 0.68, 95% CI 0.57–0.82, I2 46%, p < 0.0001). The number to treat to save one life was 7. Except for transient hyperglycemia (mostly within the 36 h following an initial bolus), prolonged glucocorticoid treatment was not associated with increased risk for neuromuscular weakness [21], gastrointestinal bleeding, or nosocomial infections [9]. Importantly, the survival benefit observed during hospitalization persisted after hospital discharge with follow-up observations extending up to 1 year (limit of measurement) [3, 4, 16].
Fig. 2.

Forest plot of mortality in randomized trials of patients with ARDS, by glucocorticoid molecule. Hospital mortality for patients (n = 766) randomized before day 14 of ARDS onset in nine randomized trials investigating prolonged glucocorticoid treatment in ARDS. Comparison between randomized trials which investigated methylprednisolone (n = 272) vs. hydrocortisone (n = 494) treatment. M–H Mantel–Haenszel statistics, df degrees of freedom
The task force suggests administering (Table 1) methylprednisolone in patients with early (up to day 7 of onset; PaO2/FiO2 of ≤ 200) moderate-to-severe ARDS in a dose of 1 mg/kg/day (ideal body weight) and late (after day 6 of onset) persistent ARDS in a dose of 2 mg/kg/day followed by slow tapering over 13 days (conditional recommendation based on moderate quality of evidence). Furthermore, the task force suggested that methylprednisolone should be weaned slowly (6–14 days) and not stopped rapidly (2–4 days) or abruptly as deterioration may occur from the development of a reconstituted inflammatory response [9]. Since glucocorticoid treatment blunts the febrile response, infection surveillance was recommended to promptly identify and treat hospital-acquired infections [9].
Table 1.
Methylprednisolone treatment of early moderate-to-severe ARDS and late unresolving ARDS
| Early moderate-to-severe ARDS (PaO2:FiO2 ≤ 200 on PEEP 5 cmH20) | ||
| Time | Intravenous administration form | Dosage |
| Loading | Bolus over 30 min | 1 mg/kg |
| Days 1 to 14*,†,‡ | Infusion at 10 cc/hour | 1 mg/kg/day |
| Days 15 to 21*,‡ | Infusion at 10 cc/hour | 0.5 mg/kg/day |
| Days 22 to 25*,‡ | Infusion at 10 cc/hour | 0.25 mg/kg/day |
| Days 26 to 28*,‡ | Infusion at 10 cc/hour | 0.125 mg/kg/day |
| Unresolving ARDS = less than (a) one-point reduction in lung injury score or (b) or 100 improvement of in PaO2:FiO2 • By day 7 of ARDS in patients not receiving methylprednisolone for early ARDS • By days 5–7 of ARDS in patients receiving methylprednisolone (above) for early ARDS | ||
| Time | Intravenous administration form | Dosage |
| Loading | Bolus over 30 min | 2 mg/kg |
| Days 1 to 14*,†,‡ | Infusion at 10 cc/hour | 2 mg/kg/day |
| Days 15 to 21*,‡ | Infusion at 10 cc/hour | 1 mg/kg/day |
| Days 22 to 25*,‡ | Infusion at 10 cc/hour | 0.5 mg/kg/day |
| Days 26 to 28*,‡ | Infusion at 10 cc/hour | 0.25 mg/kg/day |
| Days 29 to 28*,‡ | Bolus over 30 min | 0.125 mg/kg/day |
IV = intravenous. The dosage is adjusted to ideal body weight and round up to the nearest 10 mg (i.e., 77 mg round up to 80 mg). The bolus is given over 30 min. The infusion is obtained by adding the daily dosage to 240 cc of normal saline and run at 10 cc/hour
*Five days after the patient can ingest medications, methylprednisolone is administered per os in one single daily equivalent dose. Enteral absorption of methylprednisolone is compromised for days after extubation. Prednisone (available in 1-mg, 5-mg, 10-mg, and 20-mg strengths) can be used in place of methylprednisolone
†If between days 1 to 14 the patient is extubated, the patient is advanced to day 15 of drug therapy and tapered according to schedule
‡When patients leave the intensive care unit, if they are still not tolerating enteral intake for at least 5 days, they should be given the dosage specified but divided into two doses and given every 12 h IV push until tolerating ingestion of medications by mouth
Methylprednisolone may have several advantages over hydrocortisone for the treatment of ARDS. Methylprednisolone has (i) greater affinity for the glucocorticoid receptor (GR) [22], (ii) high penetration in lung tissue with longer residence time [23], and high potency for both (iii) genomic (inhibitory activity of transcription factor nuclear factor-kB) [24] and (iv) non-genomic activity [25]. Bolus administration prior to infusion achieves prompt elevation in plasma levels to assure higher GR saturation in the (i) cytoplasm and on the (ii) cell membrane for genomic and non-genomic actions, respectively. Cytoplasmic GR reach maximal saturation with approximately 100 mg methylprednisolone equivalent [26]. Bolus-associated increase in plasma methylprednisolone level causes transient hyperglycemia that does not affect the outcome. The methylprednisolone dose of 1 mg/kg/day in early ARDS is similar to the one commonly used in other forms of interstitial lung diseases [27] and in the IPDMA was associated—in comparison to placebo—with a threefold increase in the rate extubation by day 28 (HR 3.48, 95% CI 2.07–5.85; p < 0.0001) [13]. In critically ill patients, reduction in duration of mechanical ventilation is associated with a significant improvement in long-term outcomes including mortality, functional status, and quality of life [28, 29].
Observational studies and controlled trials have investigated the impact of early initiation of glucocorticoid treatment on preventing progression of the temporal continuum of systemic inflammation in patients with, or at risk for, ARDS. In a large retrospective observation study, among patients admitted to the ICU with sepsis, preadmission oral glucocorticoid treatment was independently associated with a lower incidence of ARDS (35% vs. 42%; p = 0.008) [30]. Two prospective controlled studies found that the intra-operative intravenous administration of methylprednisolone (125 or 250 mg) reduced the incidence of post-surgical ALI ARDS in patients undergoing pneumonectomy (N = 72; 0% vs. 13.5%, p < 0.05) [31] and esophagectomy (N = 234; 1.3% vs. 9.3%; p = 0.04) [32]. In aggregate data from four RCTs in patients (n = 945) hospitalized with community-acquired pneumonia, early prolonged glucocorticoid treatment prevented progression to ARDS (N = 945; 0.4% vs. 3.0%; RR 0.24, 95% CI 0.24, 0.10–0.56) [33]. In patients with early ARDS, prolonged methylprednisolone treatment prevented progression to respiratory failure requiring mechanical ventilation (42% vs. 100%; p = 0.02) [34] or progression to unresolving ARDS (8% vs. 36%; p = 0.002) [3].
Finally, the ARDS network RCT “Efficacy of Corticosteroids as Rescue Therapy for the Late Phase of Acute Respiratory Distress Syndrome (LaSRS)” [5] is frequently quoted—in isolation of the updated literature—to negate a therapeutic benefit for prolonged glucocorticoid treatment in ARDS [35]. Contrary to the misinformation associated with this publication, a recent re-analysis of the data demonstrates that methylprednisolone treatment was safe and highly effective in achieving disease resolution with sizable and significant improvements in all pre-specified secondary outcomes [19].
Conclusions
In summary, there is moderate-to-high quality evidence that prolonged glucocorticoid therapy is safe and reduces (i) time to endotracheal extubation, (ii) duration of hospitalization, and (iii) mortality (number to treat to save one life = 7), and increases the number of days free from (i) mechanical ventilation, (ii) intensive care unit stay, and (iii) hospitalization. The mortality benefits—in comparison to placebo—persist after hospitalization. The adverse effects from glucocorticoids appear to be minimal and not important to patients (e.g., hyperglycemia). We believe that based on this evidence, all or almost all fully informed patients with ARDS would choose to use glucocorticoid therapy following the protocol outlined in Table 1.
Funding
This material is the result of work supported with the resources and use of facilities at the Memphis VA Medical Center. The contents of this review do not represent the views of the US Department of Veterans Affairs or the US Government.
Abbreviations
- ARDS
Acute respiratory distress syndrome
- CIRCI
Critical Illness Related Corticosteroid Insufficiency
- CPGD
Clinical practice guideline development
- IPDMA
Individual patient data meta-analysis
- IV
Intravenous
- RCT
Randomized controlled trial
Authors’ contributions
GUM developed the original draft, and all authors (GUM, RACS, RAN, and SJS) contributed equally to the final version. All authors reviewed and approved the final report.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Gianfranco Umberto Meduri, Phone: 901-577-7520, Email: gmeduri@uthsc.edu.
Reed A. C. Siemieniuk, Email: reed.siemieniuk@medportal.ca
Rachel A. Ness, Email: Rachel.Ness2@va.gov
Samuel J. Seyler, Email: samseyler@gmail.com
References
- 1.Hashimoto S, Sanui M, Egi M, Ohshimo S, Shiotsuka J, Seo R, Tanaka R, Tanaka Y, Norisue Y, Hayashi Y, et al. The clinical practice guideline for the management of ARDS in Japan. J Intensive Care. 2017;5(1):50. doi: 10.1186/s40560-017-0222-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bernard GR, Luce JM, Sprung CL, Rinaldo JE, Tate RM, Sibbald WJ, Kariman K, Higgins S, Bradley R, Metz CA, et al. High-dose corticosteroids in patients with the adult respiratory distress syndrome. N Engl J Med. 1987;317(25):1565–1570. doi: 10.1056/NEJM198712173172504. [DOI] [PubMed] [Google Scholar]
- 3.Meduri GU, Golden E, Freire AX, Taylor E, Zaman M, Carson SJ, Gibson M, Umberger R. Methylprednisolone infusion in early severe ARDS: results of a randomized controlled trial. Chest. 2007;131(4):954–963. doi: 10.1378/chest.06-2100. [DOI] [PubMed] [Google Scholar]
- 4.Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, Tolley EA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1998;280(2):159–165. doi: 10.1001/jama.280.2.159. [DOI] [PubMed] [Google Scholar]
- 5.Steinberg KP, Hudson LD, Goodman RB, Hough CL, Lanken PN, Hyzy R, Thompson BT, Ancukiewicz M. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006;354(16):1671–1684. doi: 10.1056/NEJMoa051693. [DOI] [PubMed] [Google Scholar]
- 6.Teng D, Pang QF, Yan WJ, Zhao Xin W, Xu CY. The harmful effect of prolonged high-dose methylprednisolone in acute lung injury. Int Immunopharmacol. 2013;15(2):223–226. doi: 10.1016/j.intimp.2012.12.004. [DOI] [PubMed] [Google Scholar]
- 7.Takaki M, Ichikado K, Kawamura K, Gushima Y, Suga M. The negative effect of initial high-dose methylprednisolone and tapering regimen for acute respiratory distress syndrome: a retrospective propensity matched cohort study. Crit Care. 2017;21(1):135. doi: 10.1186/s13054-017-1723-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kido T, Muramatsu K, Asakawa T, Otsubo H, Ogoshi T, Oda K, Kubo T, Fujino Y, Matsuda S, Mayumi T. The relationship between high-dose corticosteroid treatment and mortality in acute respiratory distress syndrome: a retrospective and observational study using a nationwide administrative database in Japan. BMC Pulm Med. 2018;18(1):28. doi: 10.1186/s12890-018-0597-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Annane D, Pastores S, Rochwerg B, Arlt W, Balk R, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper M. Guidelines for the diagnosis and management of Critical Illness-Related Corticosteroid Insufficiency (CIRCI) in critically ill patients (part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Crit Care Med. 2017;45(12):2078–2088. doi: 10.1097/CCM.0000000000002737. [DOI] [PubMed] [Google Scholar]
- 10.Annane D, Pastores S, Arlt W, Balk R, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper M, Marik P. Critical Illness-Related Corticosteroid Insufficiency (CIRCI): a narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM) Crit Care Med. 2017;45(12):2089–2099. doi: 10.1097/CCM.0000000000002724. [DOI] [PubMed] [Google Scholar]
- 11.Annane D, Pastores SM, Arlt W, Balk RA, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper MS, Marik PE, et al. Critical illness-related corticosteroid insufficiency (CIRCI): a narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM) Intensive Care Med. 2017;43(12):1781–1792. doi: 10.1007/s00134-017-4914-x. [DOI] [PubMed] [Google Scholar]
- 12.Meduri GU, Tolley EA, Chrousos GP, Stentz F. Prolonged methylprednisolone treatment suppresses systemic inflammation in patients with unresolving acute respiratory distress syndrome. Evidence for inadequate endogenous glucocorticoid secretion and inflammation-induced immune cell resistance to glucocorticoids. Am J Respir Crit Care Med. 2002;165(7):983–991. doi: 10.1164/ajrccm.165.7.2106014. [DOI] [PubMed] [Google Scholar]
- 13.Meduri GU, Bridges L, Shih MC, Marik PE, Siemieniuk RAC, Kocak M. Prolonged glucocorticoid treatment is associated with improved ARDS outcomes: analysis of individual patients’ data from four randomized trials and trial-level meta-analysis of the updated literature. Intensive Care Med. 2016;42(5):829–840. doi: 10.1007/s00134-015-4095-4. [DOI] [PubMed] [Google Scholar]
- 14.Rezk N, Ibrahim A. Effects of methylprednisolone in early ARDS. Egypt J Chest Dis Tuberc. 2013;62(1):167–172. doi: 10.1016/j.ejcdt.2013.02.013. [DOI] [Google Scholar]
- 15.Confalonieri M, Urbino R, Potena A, Piattella M, Parigi P, Puccio G, Della Porta R, Giorgio C, Blasi F, Umberger R, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med. 2005;171(3):242–248. doi: 10.1164/rccm.200406-808OC. [DOI] [PubMed] [Google Scholar]
- 16.Annane D, Sebille V, Bellissant E, Ger-Inf-05 Study G Effect of low doses of corticosteroids in septic shock patients with or without early acute respiratory distress syndrome. Crit Care Med. 2006;34(1):22–30. doi: 10.1097/01.CCM.0000194723.78632.62. [DOI] [PubMed] [Google Scholar]
- 17.Sabry NA, Omar EE-D. Corticosteroids and ICU course of community acquired pneumonia in Egyptian settings. Pharmacol Pharm. 2011;2:73–81. doi: 10.4236/pp.2011.22009. [DOI] [Google Scholar]
- 18.Liu L, Li J, Huang YZ, Liu SQ, Yang CS, Guo FM, Qiu HB, Yang Y. The effect of stress dose glucocorticoid on patients with acute respiratory distress syndrome combined with critical illness-related corticosteroid insufficiency. Zhonghua Nei Ke Za Zhi. 2012;51(8):599–603. [PubMed] [Google Scholar]
- 19.Meduri GU, Bridges L, Siemieniuk RAC, Kocak M. An exploratory reanalysis of the randomized trial on efficacy of corticosteroids as rescue therapy for the late phase of acute respiratory distress syndrome. Crit Care Med. 2018; 10.1097/CCM.0000000000003021). Published ahead of print [DOI] [PubMed]
- 20.Tongyoo S, Permpikul C, Mongkolpun W, Vattanavanit V, Udompanturak S, Kocak M, Meduri GU. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: results of a randomized controlled trial. Crit Care. 2016;20(1):329. doi: 10.1186/s13054-016-1511-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Meduri GU, Schwingshackl A, Hermans G. Prolonged glucocorticoid treatment in ARDS: impact on intensive care unit-acquired weakness. Front Pediatr. 2016;4:69. doi: 10.3389/fped.2016.00069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mager DE, Moledina N, Jusko WJ. Relative immunosuppressive potency of therapeutic corticosteroids measured by whole blood lymphocyte proliferation. J Pharm Sci. 2003;92(7):1521–1525. doi: 10.1002/jps.10402. [DOI] [PubMed] [Google Scholar]
- 23.Greos LS, Vichyanond P, Bloedow DC, Irvin CG, Larsen GL, Szefler SJ, Hill MR. Methylprednisolone achieves greater concentrations in the lung than prednisolone. A pharmacokinetic analysis. Am Rev Respir Dis. 1991;144(3 Pt 1):586–592. doi: 10.1164/ajrccm/144.3_Pt_1.586. [DOI] [PubMed] [Google Scholar]
- 24.Li SMG, Miller DD, Yates CR. Evaluation of AP-1 and NF-kB inhibitory potency for oral glucocorticoids. PharmSci. 2003;5(S1):Abstract R6173. [Google Scholar]
- 25.Croxtall JD, Van Hal PTW, Choudhury Q, Gilroy DW, Flower RJ. Different glucocorticoids vary in their genomic and non-genomic mechanism of action in A549 cells. Br J Pharmacol. 2002;135(2):511–519. doi: 10.1038/sj.bjp.0704474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Buttgereit F, da Silva JA, Boers M, Burmester GR, Cutolo M, Jacobs J, Kirwan J, Kohler L, Van Riel P, Vischer T, et al. Standardised nomenclature for glucocorticoid dosages and glucocorticoid treatment regimens: current questions and tentative answers in rheumatology. Ann Rheum Dis. 2002;61(8):718–722. doi: 10.1136/ard.61.8.718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jantz MA, Sahn SA. Corticosteroids in acute respiratory failure. Am J Respir Crit Care Med. 1999;160(4):1079–1100. doi: 10.1164/ajrccm.160.4.9901075. [DOI] [PubMed] [Google Scholar]
- 28.Wilson ME, Barwise A, Heise KJ, Loftsgard TO. Dziadzko M, Cheville A, Majzoub A, Novotny PJ, Gajic O, Biehl M. Long-term return to functional baseline after mechanical ventilation in the ICU. Crit Care Med. 2018;46(4):562–569. doi: 10.1097/CCM.0000000000002927. [DOI] [PubMed] [Google Scholar]
- 29.Combes A, Costa MA, Trouillet JL, Baudot J, Mokhtari M, Gibert C, Chastre J. Morbidity, mortality, and quality-of-life outcomes of patients requiring >= 14 days of mechanical ventilation. Crit Care Med. 2003;31(5):1373–1381. doi: 10.1097/01.CCM.0000065188.87029.C3. [DOI] [PubMed] [Google Scholar]
- 30.McKown AC, McGuinn EM, Ware LB, Wang L, Janz DR, Rice DA, Semler MW. Pre-admission oral corticosteroids are associated with reduced risk of acute respiratory distress syndrome in critically Ill adults with sepsis. Crit Care Med. 2017;45:774. doi: 10.1097/CCM.0000000000002286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cerfolio RJ, Bryant AS, Thurber JS, Bass CS, Lell WA, Bartolucci AA. Intraoperative solumedrol helps prevent postpneumonectomy pulmonary edema. Ann Thorac Surg. 2003;76(4):1029–1033. doi: 10.1016/S0003-4975(03)00879-8. [DOI] [PubMed] [Google Scholar]
- 32.Park SY, Lee HS, Jang HJ, Joo J, Zo JI. Efficacy of intraoperative, single-bolus corticosteroid administration to prevent postoperative acute respiratory failure after oesophageal cancer surgery. Interact Cardiovasc Thorac Surg. 2012;15(4):639–643. doi: 10.1093/icvts/ivs167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Siemieniuk RA, Meade MO, Alonso-Coello P, Briel M, Evaniew N, Prasad M, Alexander PE, Fei Y, Vandvik PO, Loeb M, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(7):519–528. doi: 10.7326/M15-0715. [DOI] [PubMed] [Google Scholar]
- 34.Lee HS, Lee JM, Kim MS, Kim HY, Hwangbo B, Zo JI. Low-dose steroid therapy at an early phase of postoperative acute respiratory distress syndrome. Ann Thorac Surg. 2005;79(2):405–410. doi: 10.1016/j.athoracsur.2004.07.079. [DOI] [PubMed] [Google Scholar]
- 35.Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med. 2017;377(6):562–572. doi: 10.1056/NEJMra1608077. [DOI] [PubMed] [Google Scholar]
- 36.Venkatesh B, Finfer S, Cohen J, Rajbhandari D, Arabi Y, Bellomo R, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378(9):797–808. doi: 10.1056/NEJMoa1705835. [DOI] [PubMed] [Google Scholar]
- 37.Tasaka S, Tatsumi K, Assembly of Pulmonary C, Lung Injury tJRS. Clinical practice of acute respiratory distress syndrome in Japan: a nationwide survey and scientific evidences. Respir Investig. 2017;55(4):257-263 [DOI] [PubMed]