

Abstract
Background
Salary is perceived as a key factor affecting job satisfaction, employment, and the retention or migration of physicians within and across countries. This study aimed to describe physicians’ salary and workload and to examine the factors determining the salary of physicians in China.
Methods
We conducted a self-administered, smartphone-based national survey in 136 tertiary hospitals across 31 provinces. A total of 17,615 physicians self-reported their salaries after tax and their characteristics, practice settings, and work efforts in 2015. Then, 2498 of the physicians were followed up for the second-round survey in 2016. Univariate analysis and general estimate equations were applied to evaluate the factors associated with salary.
Result
In 2015, the average annual salary of the physicians was US$13,764. Physicians in eastern China earned more than those in central (p < 0.001) and western China (p = 0.002) after adjustment for locality expenditure per capita. The salary for men in 2015 was US$14,832, which was more than that for women (US$12,912; p < 0.001). Of the respondents, 76.3% worked more than 40 h per week. The physicians dealt with 40 patients per day on average. Consequently, 67.2% physicians spent no more than 10 min with each outpatient. After adjustments for age and management position, salary was associated with years in practice, education background, and specialty, but not with weekly work hours and gender.
Conclusions
The physicians’ salaries were relatively low, and the majority of the respondents worked more than 40 h per week. Years in practice, education background, specialty, and region were associated with salary, while weekly work hours and gender were not. To better remunerate Chinese physicians, more resources are demanded, and a workload-based salary scheme should be adopted.
Keywords: Physician salary, Workload, Cross-sectional, Follow-up, China
Background
In China, hospitals consist of 3 types: general hospitals, traditional Chinese medicine (TCM) hospitals, and specialty hospitals, and approximately 10% of hospitals are TCM hospitals. There are approximately 383,000 TCM physicians, comprising 15% of registered physicians [1]. The majority of hospitals are public and run by the government. The routine subsidy from the government is mainly used to pay health care workers’ basic salaries in public hospitals, while the private hospitals need to pay physicians themselves, and their salaries are based on contract.
The salaries of physicians in Chinese public hospitals consist of 3 parts: basic salary, benefits, and bonuses [2]. The basic salary subsidized by the government follows a unified standard and is determined by the physician’s educational background, technical title, and years of practice. Benefits mainly refer to mandated benefits and supplemental welfare. Mandated benefits include medical insurance, endowment insurance, unemployment insurance, maternity insurance, injury insurance, and housing funding. Supplemental welfare usually consists of transportation subsidies, management allowance, and malpractice insurance, among other items. Bonuses are regarded as the majority of the salary and have 2 distribution models. One model of bonuses is bound to the profits of the department and is comprehensively adopted by hospitals. The other is the workload count model, which is a reform that was implemented in 2004. However, despite years of trial, this incentive mechanism is not popular and has been slow to be adopted [3, 4].
Salary is a central issue in health care. Salary is perceived as a key factor affecting the job satisfaction, employment, and retention or migration of physicians within and across countries [5, 6]. Lower salary is linked to physicians’ job dissatisfaction, which in turn is linked to shortages of physicians and undesirable patient outcomes [7–9]. Reports indicate that China is suffering a chronic shortage of medical doctors in certain specialties. The proportion of young physicians has decreased by approximately 10% in China in the past 10 years, while the proportion of aged physicians has increased by nearly 10% [10]. Although there is no direct evidence that the decline in numbers of physicians is caused by low job satisfaction, it has been found that job satisfaction is negatively related to the turnover intention of physicians in China; the most frequent complaints among them are the disproportionately low salary and heavy work load [11, 12]. A survey in Zhejiang province showed that the 88% of physicians who would not want their children to be doctors cited poor pay and high pressure from work as the top 2 reasons [13].
Given the challenges of recruiting and retaining of physicians for the health system and the fact that the majority of hospitals are public in China, authorities have begun to focus on physician salaries in public hospitals; however, little national salary data are available. The aims of our research were (1) to describe physicians’ salaries and workloads and (2) to explore the underlying factors that determine physician salary in Chinese public hospitals.
Methods
Cross-sectional samples
The cross-sectional survey was conducted in 136 tertiary hospitals across 31 provinces of China in December 2015. Multistage sampling was used in our study.
Forty-three hospitals associated with the Chinese national health and family commission were included in the sample. In addition, 1 general hospital, 1 traditional medicine hospital, and 1 specialty hospital were selected at random from each province, for a total of 136 tertiary hospitals.
We assumed that the CV (coefficient of variation) for the average annual salary was 0.8 based on the results of pilot tests, set the significance level at 0.05, and estimated a minimum sample size of 130 physicians at each hospital. To ensure that the minimum sample size was reached, we planned to select 150 physicians from each hospital. Physicians were eligible for inclusion in this study if they (1) worked full-time and (2) had practised for more than 1 year at the sampled hospital. Physicians were excluded from this study if they (1) had retired but were re-employed or (2) had previously worked as a physician but switched to full-time work as a researcher or administrator. In each sample hospital, the human resources department provided a list of the eligible physicians and categorized them into 3 groups (residents, attendings, and associate chiefs/chiefs). We selected physicians from the 3 groups proportionally according to their representation in each group. Ultimately, 20,400 physicians received invitation to take part in our survey. In total, the actual number of responding physicians was 17,975 (with a response rate of 88.11%), and the number of valid responses was 17,615. Ethics approval was obtained from the Research Ethics Committee of the Chinese Academy of Medical Science & Peking Union Medical College. A statement explaining the purpose of the study and informed consent to participate was included on the opening page of the survey. After accepting the terms of consent, the physicians were able to complete the online questionnaire.
Follow-up samples
In December 2016, we invited the physicians surveyed in December 2015 to participate through short messages, hospital bulletins, and hospital office automation systems. A total of 2498 physicians responded.
Survey instrument design
We implemented a self-administered questionnaire instrument using a smartphone platform (WeChat) to obtain information about the physicians’ salary after taxes, characteristics (including gender, age, education background, technical title, years in practice, and management position), practice settings (including hospital and department), and workload (weekly work hours, the number of visits per day, and consulting time). After all the questions were answered, the questionnaire could be submitted. Trained surveyors were assigned to every sample hospital to help the physicians complete the questionnaire. The same questionnaire was used in both rounds of surveys. The physicians’ salaries were converted to US$ (1 US$ = 6.47 RMB in December 2015 and 1 US$ = 6.95 RMB in December 2016).
Statistical analysis
T-test and ANOVA analyses were used to examine whether salary was linked to region, gender, age, years in practice, education background, technical title, management position, and specialty. Generalized estimating equation analysis was used to determine which factors affected physician salary and whether the salary had changed over time after adjusting for confounders. A p < 0.05 was determined to be statistically significant. SAS version 9.3 (SAS Institute, Inc., NC, USA) was used to perform the statistical analyses.
Results
Cross-sectional study
Demographic characteristics of the cross-sectional study sample
The characteristics of the study sample are shown in Table 1. A total of 17,615 physicians were surveyed in our study in 2015: 7371 from eastern China, 4621 from central China, and 5623 from western China. The mean age was 37.1 years (SD: 8.2), and the average number of years in practice was 10.4 (SD: 8.7). Of the physicians, 7851 (44.6%) were male, and 9764 (55.4%) were female.
Table 1.
Physicians’ characteristics by region in 2015
| Items | Total N = 17,615 | East N (%) | Central N (%) | West N (%) |
|---|---|---|---|---|
| Age, years | ||||
| ≤ 30 | 4434(25.2%) | 1858(25.2%) | 1026(22.2%) | 1550(27.6%) |
| 31–40 | 7970(45.2%) | 3316(45.0%) | 2162(46.8%) | 2492(44.3%) |
| 41–50 | 3753(21.3%) | 1632(22.1%) | 971(21.0%) | 1150(20.5%) |
| ≥ 51 | 1458(8.3%) | 565(7.6%) | 462(10.0%) | 431(7.7%) |
| Years in practice | ||||
| < 10 | 10,076(57.2%) | 4188(56.8%) | 2553(55.2%) | 3335(59.3%) |
| 10–19 | 4300(24.4%) | 1848(25.1%) | 1144(24.8%) | 1308(23.3%) |
| ≥ 20 | 3239(18.4%) | 1335(18.1%) | 924(20.0%) | 1335(18.1%) |
| Education | ||||
| Bachelor’s degree and below | 5145(29.2%) | 1612(21.9%) | 1028(22.2%) | 2505(44.5%) |
| Master’s | 8242(46.8%) | 3337(45.3%) | 2489(53.9%) | 2416(43.0%) |
| Doctorate | 4228(24.0%) | 2422(32.9%) | 1104(23.9%) | 702(12.5%) |
| Technical title | ||||
| Resident | 5589(31.7%) | 2241(30.4%) | 1344(29.1%) | 2004(35.6%) |
| Attending | 6122(34.8%) | 2665(36.2%) | 1627(35.2%) | 1830(32.5%) |
| Associate chief | 3572(20.3%) | 1488(20.2% | 995(21.5%) | 1089(19.4%) |
| Chief | 2332(13.2%) | 977(13.3%) | 655(14.2%) | 700(12.4%) |
| Management position | ||||
| Yes | 2422(13.9%) | 982(13.3%) | 702(15.2%) | 758(13.5%) |
| No | 15,173(86.1%) | 6389(86.7%) | 3919(84.8%) | 4865(86.5%) |
| Specialty | ||||
| Internal medicine | 4905(27.8%) | 2098(28.5%) | 1427(30.9%) | 1380(24.5%) |
| Surgery | 3303(18.8%) | 1431(19.4%) | 952(20.6%) | 920(16.4%) |
| Obstetrics | 2661(15.1%) | 1156(15.7%) | 717(15.5%) | 788(14.0%) |
| Paediatrics | 1407(8.0%) | 442(6.0%) | 332(7.2%) | 633(11.3%) |
| Emergency medicine | 744(8.0%) | 327(4.4%) | 145(3.1%) | 272(4.8%) |
| Traditional Chinese medicine | 812(4.6%) | 334(4.5%) | 182(3.9%) | 296(5.3%) |
| Otolaryngology | 935(5.3%) | 371(5.0%) | 228(4.9%) | 336(6.0%) |
| Anaesthesiology | 778(4.4%) | 312(4.2%) | 180(3.9%) | 286(5.1%) |
| Ophthalmology | 536(3.0%) | 298(4.0%) | 107(2.3%) | 131(2.3%) |
| Stomatology | 693(3.9%) | 300(4.1%) | 169(3.7%) | 224(4.0%) |
| Other | 841(4.8%) | 302(4.1%) | 182(3.9%) | 357(6.3%) |
Average annual salary
The average annual physician salary was US$13,764 in 2015. Physicians in eastern China, including some developed areas, such as Beijing, Shanghai, and Guangdong, earned more than those in central and western China (p < 0.001). The average annual salaries were US$18,984, US$12,840 and US$13,872 in eastern, central, and western China, respectively. After adjustment for locality expenditure per capita, the average adjusted annual salary was US$14,505 in eastern China, which is still higher than those in central China (US$12,816, p < 0.001) and western China (US$13,643, p = 0.002). The average annual salary of the male physicians was US$14,832, which was higher than that of the female physicians (US$12,912; p < 0.001). The top 3 highest paid specialties were ophthalmology (US$18,156), otolaryngology (US$17,664), and stomatology (US$15,852). Traditional Chinese medicine (US$ 11,748) was the specialty with the lowest annual salary, followed by paediatrics (US$12,240) and internal medicine (US$12,372; Table 2).
Table 2.
Average annual salary by physicians’ characteristics in 2015
| Item | Average annual salary (US$) | 95% CI | p value |
|---|---|---|---|
| Region | < 0.001 | ||
| East | 18,984 | 18,768-19,200 | |
| Central | 12,840 | 12,636-13,056 | |
| West | 13,872 | 13,656-14,076 | |
| Gender | < 0.001 | ||
| Male | 14,832 | 14,544-15,120 | |
| Female | 12,912 | 12,696-13,128 | |
| Age, years | < 0.001 | ||
| ≤ 30 | 9108 | 8928-9288 | |
| 31–40 | 13,200 | 12,984-13,416 | |
| 41–50 | 18,132 | 17,652-18,612 | |
| ≥ 51 | 19,848 | 18,936-20,760 | |
| Years in practice | < 0.001 | ||
| < 10 | 11,016 | 10,848-11,172 | |
| 10–19 | 16,380 | 15,984-16,776 | |
| ≥ 20 | 18,852 | 15,996-19,416 | |
| Education | < 0.001 | ||
| Bachelor’s degree and below | 11,676 | 11,412-11,940 | |
| Master’s | 12,060 | 11,844-12,276 | |
| Doctorate | 19,644 | 19,188-20,100 | |
| Technical title | < 0.001 | ||
| Resident | 8940 | 8784-9096 | |
| Attending | 13,356 | 13,116-13,596 | |
| Associate chief | 17,400 | 16,944-17,856 | |
| Chief | 20,880 | 20,148-21,612 | |
| Management position | < 0.001 | ||
| Yes | 20,544 | 19,872-21,216 | |
| No | 12,684 | 12,516-12,852 | |
| Specialty | < 0.001 | ||
| Internal medicine | 12,372 | 12,084-12,648 | |
| Surgery | 14,916 | 14,448-15,384 | |
| Obstetrics | 13,968 | 13,536-14,400 | |
| Paediatrics | 12,240 | 11,736-12,744 | |
| Emergency medicine | 13,680 | 12,864-14,496 | |
| Traditional Chinese medicine | 11,748 | 11,004-12,492 | |
| Otolaryngology | 17,664 | 16,752-18,576 | |
| Anaesthesiology | 15,600 | 14,808-16,392 | |
| Ophthalmology | 18,156 | 16,644-19,668 | |
| Stomatology | 15,852 | 14,784-16,920 | |
| Other | 10,788 | 10,236-11,340 | |
Workload
The average time per week spent seeing patients was 50.5 h (SD: 10.8). Most of the physicians (76.3%) worked more than 40 h per week; of these, 62.1% worked 41–60 h per week, and 37.9% spent more than 60 h per week with patients. The average numbers of weekly hours worked were 50.6 for male physicians and 50.3 for female physician, with no significant difference between them (p = 0.515). The physician saw an average of 40 patients per day in clinics; 38.0% saw fewer than 20 patients per day, 39.4% saw 21 to 50 patients per day, and 22.6% saw more than 50 patients. The average consultation time was 12 min, and 67.2% physicians spent no more than 10 min with each outpatient.
Follow-up study
Demographic characteristics of the follow-up study sample
To analyse the association between salary and time, 2498 physicians were followed up in December 2016. Of these, 43.3% (n = 1082) were male physicians, and 56.7% (n = 1416) were female physicians; 36.4% (n = 909) were from eastern China, 22.7% (n = 566) were from central China, and 41.0% (n = 1023) from western China. The average age of the physicians in the follow-up sample was 37.5 years (SD: 7.4), the average number of years in practice was 10.6 (SD: 8.2), and the average hours worked per week was 49.6 (SD: 11.1; Table 3).
Table 3.
Characteristics of the physicians followed up in 2016
| Item | Number | Percent |
|---|---|---|
| Gender | ||
| Male | 1080 | 43.2 |
| Female | 1418 | 56.8 |
| Region | ||
| East | 909 | 36.4 |
| Central | 566 | 22.7 |
| West | 1023 | 41.0 |
| Age, years | ||
| ≤ 30 | 448 | 17.9 |
| 31–40 | 1300 | 52.0 |
| 41–50 | 566 | 22.7 |
| ≥ 51 | 184 | 7.4 |
| Years in practice | ||
| < 10 | 1398 | 56.0 |
| 10–19 | 674 | 27.0 |
| ≥ 20 | 426 | 17.1 |
| Education | ||
| Bachelor’s degree and below | 806 | 32.3 |
| Master’s | 1267 | 50.7 |
| Doctorate | 425 | 17.0 |
| Technical title | ||
| Resident | 644 | 25.8 |
| Attending | 998 | 40.0 |
| Associate chief | 538 | 21.5 |
| Chief | 318 | 12.7 |
| Management position | ||
| Yes | 420 | 16.8 |
| No | 2078 | 83.2 |
| Specialty | ||
| Internal medicine | 568 | 22.7 |
| Surgery | 408 | 16.3 |
| Obstetrics | 425 | 17.0 |
| Paediatrics | 110 | 4.4 |
| Emergency medicine | 80 | 3.2 |
| Traditional Chinese medicine | 263 | 10.5 |
| Otolaryngology | 125 | 5.0 |
| Anaesthesiology | 109 | 4.4 |
| Ophthalmology | 63 | 2.5 |
| Stomatology | 54 | 2.2 |
| Other | 293 | 11.7 |
Factors influencing physician salary
The results of an analysis comparing physicians’ salaries among subgroups, adjusted for age and management position, are presented in Table 4.
Table 4.
Results of 2498 physicians’ longitudinal analysis of factors associated with salary, 2015–2016
| Items | Estimate (SE) | p value |
|---|---|---|
| Gender | ||
| Male | Ref. | |
| Female | −48.6 | 0.1655 |
| Age | 14.0 | 0.0051 |
| Years in practice | 13.0 | 0.0014 |
| Education | ||
| Doctorate | Ref. | |
| Bachelor’s and below | − 538.0 | <.0001 |
| Master’s | −383.0 | <.0001 |
| Technical Title | ||
| Chief | Ref. | |
| Resident | − 345.0 | 0.0008 |
| Attending | −230.1 | 0.0121 |
| Associate chief | − 142.7 | 0.0981 |
| Management position | ||
| Yes | Ref. | |
| No | −274.3 | <.0001 |
| Workload | −1.8 | 0.7399 |
| Specialty | ||
| Paediatrics | Ref. | |
| Internal medicine | − 160.1 | 0.0011 |
| Surgery | 11.61 | 0.8489 |
| Obstetrics | 33.8 | 0.5340 |
| Traditional Chinese medicine | − 166.8 | 0.0113 |
| Emergency medicine | −87.0 | 0.2086 |
| Otolaryngology | 218.5 | 0.0182 |
| Anaesthesiology | 191.7 | 0.0137 |
| Ophthalmology | 73.2 | 0.6268 |
| Stomatology | 38.0 | 0.7160 |
| Other | −60.7 | 0.3862 |
| Region | ||
| West | Ref. | |
| Central | 262.8 | <.0001 |
| Middle | −176.3 | <.0001 |
| Time (2015y = 1, 2016y = 2) | 394.4 | <.0001 |
Those with more years in practice (p = 0.001) and a higher education level (p < 0.001) earned more. Chief physicians had a higher salary than residents (p < 0.001) and attending physicians (p = 0.012). Compared with paediatrics, otolaryngology (p = 0.018) and anaesthesiology (p = 0.014) had relatively higher salaries, while traditional Chinese medicine (p = 0.011) had lower salaries. Physicians in the western part of the country earned less than those in the eastern region (p < 0.001) but more than those in central China (p < 0.001). However, there was no gender difference in salary (p = 0.165). The weekly number of hours worked had no effect on salary (p = 0.740, Table 4).
Discussion
In this study, we conducted a national survey to analyse the average physician salary, determine physicians’ workloads, and examine the potential factors that influence physician salary in China. The average annual physicians’ salary was US$13,764, and the average number of hours worked per week was 50.5.
The average annual salary (US$13,764) uncovered for Chinese physicians in our study is close to the finding reported by Dingxiangyuan ($12,360), an online forum for health care workers, although the characteristics of the participants in that survey were largely unknown [14]. However, the annual salary found in our study is far less than those reported for the United States, Canada, and Taiwan. In 2005, it has been reported that physicians earned approximately US$230,000 and US$130,000 in the United States and Canada, respectively [15]. Physicians in Taiwan, with an average annual salary of US$57,370 [16], also earned more than physicians in our survey. The gross domestic product (GDP) per capita in each country reflects the average earnings of all citizens. Figure 1 shows that the ratio of physician salaried income to GDP per capita in China is lower than those of Canada, the United States, and Taiwan. The physicians surveyed by us earned only approximately 1.5 times the Chinese GDP per capita. Canadian, US, and Taiwan physicians earned more than 4 times their local GDP per capita. The actual value in China may be lower than what we found because our data were from tertiary hospitals, which tend to have a high salary level.
Fig. 1.
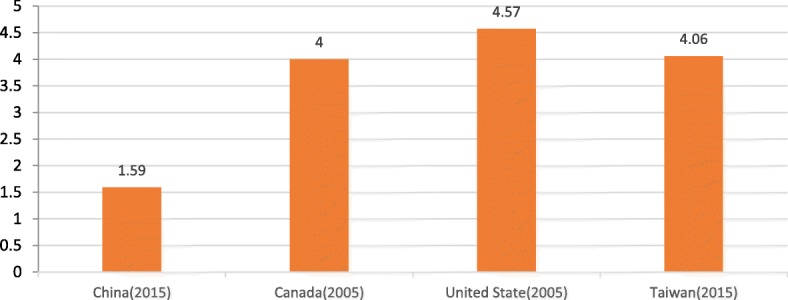
The ratio of physician salaried income to GDP per capita
Source: For Canadian and US physician income, see reference [15]. For Taiwan physician salaried income, see reference [16]. For gross gemestic product per capita in those countries and regions from IMF, see reference [40]
More resources are demanded to better remunerate physicians, but the subsidies from the government are not sufficient. The average subsidies from the government are less than 10% of the total income of each public hospital in China [17–19]. Medicine was a main source of hospital profit in the past, but a zero-profit medicine policy has been enacted in recent years, meaning that the hospitals are faced with fewer resources to remunerate their physicians. Given that the price of health care services (such as surgery) is still far lower than medicine and material, these costs could be increased to match the value of physicians’ work and could be compensated by the social health insurance fund without increasing the patients’ out-of-pocket expenditures.
Weekly work hours were not a significant contributor to salary. However, 76.3% of the physicians in our study worked more than 40 h per week. This finding is in line with the White Paper of the Chinese Physicians’ Medical Practice Environment, in which 76.6% of physicians complained about heavy work pressure and intense workloads [20]. In China, 40 h per week is the legal work week. The average weekly worked hours was 45.5 for Chinese urban employees in 2015 [21], while the average weekly worked hours was 50.5 for physicians in our study, and 28.9% of them worked more than 60 h per week. In recent years, the number of patients treated at hospitals has increased by 59%, from 2060 million in 2009 [22] to 3270 million in 2016 [23]; this increase is attributed to universal health insurance coverage [24, 25]. The huge volume of patients has made it difficult for physicians to spend sufficient time with patients: 67.2% of the physicians in our study said they spent no more than 10 min with each outpatient, while 59% of physicians in the United States spend 13 to 24 min with each patient [26]. More time on consultation leads to better treatment decisions [27], and tense physician-patient relationships may originate from less communication [28]. Physicians are entitled to high income because of their many years of study and training, heavy responsibility, and long hours of work. Physicians have always been well paid in Canada and the United States, with their earnings reaching more than 4 times their countries’ GDP per capita [15], while those in our survey earned only 1.59 times the Chinese GDP per capita. It has been demonstrated in our study that the heavy workload and low salary of physicians are disproportionate. Given that overwork may be associated with physician burnout [29, 30] and physicians’ salaries do not compensate for the extra hours worked in China, an increased salary is a feasible way to attract and retain physicians, which would reduce workloads and provide better health care services for patients.
In our study, years of practice, educational background, technical title, management position, and specialty had effects on salary. Except for weekly work hours, as discussed above, the other factors were similar to the findings of Weeks and Wallace, who suggested that provider characteristics (including age, years in practice, and role at the hospital) and practice characteristics (including region and insurance status) were likely to affect salaries [31–34]. In terms of basic salary scheme, our study found that educational background, technical title, and years of practice were associated with physician salary; physicians with a higher level of education, a higher technical title, and more years of practice earned more. Due to the bonus payment scheme, physicians’ salaries relied heavily on departmental profits; specialty was also associated with salary because the numbers of patients seen and health care expenditures varied among specialties.
We also found that salary was unequal across regions. Physicians in eastern China earned more than those in western and central China. Although the cost of living is relatively higher in eastern China, after adjustment for locality expenditure per capita, the physician annual salary in eastern China is still higher than those in western and central China. Eastern China, which includes Beijing, Shanghai, and Guangdong, is a developed region and attracts excellent physicians for work [35, 36]. As a result, the capacity of the health care service is better in eastern China, and more severe and complex patient cases are likely to be transported there from the western and central regions to receive better treatment. As mentioned in the Introduction, the physician salary relies heavily on their departmental profit. Consequently, physicians in eastern China had the highest salaries because of the region’s high socioeconomic level and abundant patient load. These factors seem to form a circle: higher salaries attract more excellent physicians, patients flock to excellent physicians, and abundant patients lead to higher salaries. To narrow the salary difference among regions, senior specialists outreach service in poor regions for priority promotion, and ‘deals’ to pay for medical education may feasible approaches.
A gender difference has been reported in other countries, such as the United States and Japan, even after adjustment for work effort, physician characteristics, and practice characteristics [37–39]. We found that Chinese male physicians earned more than their female counterparts, but after adjustments, the salary difference became nonsignificant. In our cross-sectional sample, 31.0% and 10.7% of the female physicians worked in internal medicine and paediatrics, the lower-salary specialties, compared with 23.9% and 4.6% of their male counterparts, respectively. The proportion of male physicians (16.8%) in management positions was higher than the proportion of female physicians (11.5%). The unadjusted gender difference can be attributed to the facts that more female physicians worked in lower income specialties and that the male physicians were more likely to be in management. However, there was no difference in physician-hospital contact between genders. As a result, no adjusted gender difference was found in our study.
There are several limitations in our research. First, work hours were used to represent the work load without considering the intensity of the work. In the future, researchers hope to distinguish between academic and clinical work hours and to adjust clinical work hours using the case mix index. Second, the physicians were selected from tertiary public hospitals. We plan to survey physicians in secondary public hospitals, community health centres, village hospitals, and private hospitals in the future to form a complete picture. Third, after data from pilot tests in 3 provinces were examined, we found that the average reported salaries by specialty and technical title were near to the real levels remunerated by the hospital. Although the reported salaries were reliable, we failed to collect the grey income, such as pharmaceutical kickbacks and thanks money from patients, which are important sources of physicians’ income but are illegal in China. Compared with physicians in the west, physicians do not need to pay malpractice insurance and the annual cost of licence accreditations themselves. As a result, the income of physicians may be under estimated. Finally, there is gender difference in salary, but we do not have sufficient evidence to explain it. We plan to perform more research to determine why the difference exists.
Conclusion
In conclusion, we found that physicians’ salaries were relatively low and that the majority of the sample worked more than 40 h per week. In addition to weekly work hours, the number of years in practice, education background, and specialty were associated with salary as a result of the salary scheme. Regional differences were found even after adjustment for locality expenditure per capita. To better remunerate Chinese physicians, more resources are demanded, and a workload-based salary scheme should be adopted.
Acknowledgements
We would like to thank all physicians who decided to respond to the questionnaire. In addition, we gratefully acknowledge the health authorities and experts from the 31 provinces who helped coordinate with the sample hospitals.
Funding
This work was supported by a grant from the National Health & Family Planning Commission, PR China.
Availability of data and materials
The distribution of the data files is restricted by the written consent of the participating investigators. Researchers who want access to the data may contact the corresponding author, who will determine whether the requested data may be made available in a form that does not violate the written consent.
Abbreviations
- CV
Coefficient of Variation
- GDP
Gross domestic product
- SD
Standard Deviation
- TCM
Traditional Chinese medicine
Authors’ contributions
CZ and YL conceived and designed the study. CZ conducted the data analysis and wrote the first draft of the manuscript. YL contributed to critical appraisal and finalizing of the manuscript. All the authors critically read and approved the final manuscript.
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of the Chinese Academy of Medical Science & Peking Union Medical College. A statement explaining the informed consent to participate was included on the opening page of the survey. The participants were only able to complete the online questionnaire after accepting the terms of consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Chunyu Zhang, Email: zcy_fish@sina.com.
Yuanli Liu, Phone: (+86)010-62026607, Email: yuanliliu_pumc@163.com.
References
- 1.National Health and Family Planning Commission PRC . China health and family planning yearbook. Beijing: China Health and Family Planning Yearbook Press; 2016. [Google Scholar]
- 2.Ran LM, Luo KJ, Wu YC, Yao L, Feng YM. An analysis of China's physician salary payment system. J Huazhong Univ Sci Technolog Med Sci. 2013;33:309–314. doi: 10.1007/s11596-013-1116-9. [DOI] [PubMed] [Google Scholar]
- 3.Yip WC, Hsiao W, Meng Q, Chen W, Sun X. Realignment of incentives for health-care providers in China. Lancet. 2010;375:1120–1130. doi: 10.1016/S0140-6736(10)60063-3. [DOI] [PubMed] [Google Scholar]
- 4.Xia M, Pei L. Research on doctor payment system of public hospitals in China. Chin Hosp. 2016;20:40–43. [Google Scholar]
- 5.Ferrinho P, Van Lerberghe W, Julien MR, Fresta E, Gomes A, Dias F, et al. How and why public sector doctors engage in private practice in Portuguese-speaking African countries. Health Policy Plan. 1998;13:332–338. doi: 10.1093/heapol/13.3.332. [DOI] [PubMed] [Google Scholar]
- 6.Morgan P, Everett CM, Humeniuk KM, Valentin VL. Physician assistant specialty choice: distribution, salaries, and comparison with physicians. JAAPA JAAPA. 2016;29:46–52. doi: 10.1097/01.JAA.0000484301.35696.16. [DOI] [PubMed] [Google Scholar]
- 7.Abelsen B, Olsen JA. Does an activity based remuneration system attract young doctors to general practice? BMC Health Serv Res. 2012;12:68. doi: 10.1186/1472-6963-12-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sarma S, Devlin RA, Belhadji B, Thind A. Does the way physicians are paid influence the way they practice? The case of Canadian family physicians’ work activity. Health Policy. 2010;98:203–217. doi: 10.1016/j.healthpol.2010.06.019. [DOI] [PubMed] [Google Scholar]
- 9.Kahn D, Pillay S, Veller MG, Panieri E, Westcott MJ. General surgery in crisis--comparatively low levels of remuneration. S Afr J Surg. 2006;44(96):98–99. [PubMed] [Google Scholar]
- 10.Lien SS, Kosik RO, Fan AP, Huang L, Zhao X, Chang X, et al. 10-year trends in the production and attrition of Chinese medical graduates: an analysis of nationwide data. Lancet. 2016;388:S11. doi: 10.1016/S0140-6736(16)31938-9. [DOI] [Google Scholar]
- 11.Wang Z, Xie Z, Dai J, Zhang L, Huang Y, Chen B. Physician burnout and its associated factors: a cross-sectional study in shanghai. J Occupat Health. 2014;56:73–83. doi: 10.1539/joh.13-0108-OA. [DOI] [PubMed] [Google Scholar]
- 12.Zhang Y, Feng X. The relationship between job satisfaction, burnout, and turnover intention among physicians from urban state-owned medical institutions in Hubei. China: a cross-sectional study BMC Health Serv Res. 2011;11:235. doi: 10.1186/1472-6963-11-235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wu D, Wang Y, Lam KF, Hesketh T. Health system reforms, violence against doctors and job satisfaction in the medical profession: a cross-sectional survey in Zhejiang Province. Eastern China BMJ Open. 2014;4:e006431. doi: 10.1136/bmjopen-2014-006431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ding XY. Report on Chinese doctors’ salaries in 2015. 2016. [Google Scholar]
- 15.Duffin J. The impact of single-payer health care on physician income in Canada, 1850-2005. Am J Public Health. 2011;101:1198–1208. doi: 10.2105/AJPH.2010.300093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bureau of Statistics of Taiwan. Taiwan statistics year-book 2016. http://www.dgbas.gov.tw/lp.asp?CtNode=3120&CtUnit=1049&BaseDSD=34 &mp=1. Accessed 29 Nov 2017.
- 17.Xu Y. Problems and countermeasures of public hospital fiscal input in China. Med Soc. 2016;29:50–52. [Google Scholar]
- 18.Tan H, Yan W, Liu X, Zhu X, Zheng W, et al. Analysis on the economic operation and development status of urban public hospitals in Chongqing. Chin Health Econ. 2016;35:71–74. [Google Scholar]
- 19.National of Health and Family Planning Commission of the People’s Republic of China . Health and family planning statistic year book of China. Beijing: Chinese Union Medical College Press; 2015. p. 100. [Google Scholar]
- 20.Association CMD. The white paper of Chinese medical doctors’ practice environment. http://www.cmda.net/xiehuixiangmu/falvshiwubu/tongzhigonggao/2015-05-28/14587.html. Accessed 11 Sept 2017.
- 21.Ministry of Human Resources and Social Security of the People’s Republic of China. Weekly working hours in urban area by sector and sex http://www.mohrss.gov.cn/SYrlzyhshbzb/zwgk/szrs/tongjinianjian/201803/t20180302_289122.html. Accessed 24 July 2018.
- 22.National Health and Family Planning Commission of the People's Republic of China. Health statistics yearbook. 2010. http://www.nhfpc.gov.cn/htmlfiles/zwgkzt/ptjnj/year2010/index2010.html. Accessed 11 Sept 2017.
- 23.National Health and Family Planning Commission of the People's Republic of China. China health and family planning development bulletin. 2017. http://www.moh.gov.cn/guihuaxxs/s10748/201708/d82fa7141696407abb4ef764f3edf095.shtml?winzoom=1. Accessed 11 Sept 2017.
- 24.Meng Q, Xu L, Zhang Y, Qian J, Cai M, Xin Y, et al. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. Lancet. 2012;379:805–814. doi: 10.1016/S0140-6736(12)60278-5. [DOI] [PubMed] [Google Scholar]
- 25.Chen J, Yu H, Dong H. Effect of the new rural cooperative medical system on farmers’ medical service needs and utilization in Ningbo. China BMC Health Serv Res. 2016;16:593. doi: 10.1186/s12913-016-1842-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Medscape. Medscape physician compensation report 2017. http://www.medscape.com/slideshow/compensation-2017-overview-6008547. Accessed 11 Sept 2017.
- 27.de Wit NJ. A “time out consultation” in primary care for elderly patients with cancer: better treatment decisions by structural involvement of the general practitioner. Eur J Cancer Care (Engl). 2017; 10.1111/ecc.12711. [DOI] [PubMed]
- 28.Jalil A, Zakar R, Zakar MZ, Fischer F. Patient satisfaction with doctor-patient interactions: a mixed methods study among diabetes mellitus patients in Pakistan. BMC Health Serv Res. 2017;17:155. doi: 10.1186/s12913-017-2094-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dyrbye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88:1358–1367. doi: 10.1016/j.mayocp.2013.07.016. [DOI] [PubMed] [Google Scholar]
- 30.Hoff T, Carabetta S, Collinson GE. Satisfaction, burnout, and turnover among nurse practitioners and physician assistants: a review of the empirical literature. Med Care Res Rev. 2017;1077558717730157 10.1177/1077558717730157. [DOI] [PubMed]
- 31.Weeks WB, Wallace AE. The influence of race and gender on family physician’s annual incomes. J Am Board Fam Med. 2006;19:548–556. doi: 10.3122/jabfm.19.6.548. [DOI] [PubMed] [Google Scholar]
- 32.Weeks WB, Wallace AE. Race and gender differences in general internists’ annual incomes. J Gen Intern Med. 2006;21:1167–1171. doi: 10.1111/j.1525-1497.2006.00592.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Weeks WB, Wallace AE. Differences in the annual incomes of emergency physicians related to gender. Acad Emerg Med. 2007;14:434–440. doi: 10.1197/j.aem.2006.12.013. [DOI] [PubMed] [Google Scholar]
- 34.Weeks WB, Wallace AE. Gender differences in ophthalmologists’ annual incomes. Ophthalmology. 2007;114:1696–1701. doi: 10.1016/j.ophtha.2006.12.020. [DOI] [PubMed] [Google Scholar]
- 35.An Y. Characters and improvement strategies of distribution of high - quality medical resources. Chin Heal Qual Manag. 2011;18:110–113. [Google Scholar]
- 36.Zhang N, Sun XJ, Li C. Analyzing the equity of health resources allocation in China based on Theil index. Chinese health management. 2014;31:88–91. [Google Scholar]
- 37.Nguyen Le TA, Lo Sasso AT, Vujicic M. Trends in the earnings gender gap among dentists, physicians, and lawyers. J Am Dent Assoc. 2017;148:257–262.e2. doi: 10.1016/j.adaj.2017.01.005. [DOI] [PubMed] [Google Scholar]
- 38.Jena AB, Olenski AR, Blumenthal DM. Sex differences in physician salary in US public medical schools. JAMA Intern Med. 2016;176:1294–1304. doi: 10.1001/jamainternmed.2016.3284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Okoshi K, Nomura K, Taka F, Fukami K, Tomizawa Y, Kinoshita K, et al. Suturing the gender gap: income, marriage, and parenthood among Japanese surgeons. Surgery. 2016;159:1249–1259. doi: 10.1016/j.surg.2015.12.020. [DOI] [PubMed] [Google Scholar]
- 40.International Monetary Fund. IMF financial data by country. http://www.imf.org/en/data#imffinancial. Accessed 24 July 2017.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The distribution of the data files is restricted by the written consent of the participating investigators. Researchers who want access to the data may contact the corresponding author, who will determine whether the requested data may be made available in a form that does not violate the written consent.