

Abstract
We evaluated the impact of homework completion on change in PTSD symptoms in the context of two randomized controlled trials of Cognitive Processing Therapy for PTSD (CPT). Female participants (n=140) diagnosed with PTSD attended at least one CPT session and were assigned homework at each session. The frequency of homework completion was assessed at the beginning of each session and PTSD symptoms were assessed every other session. Piecewise growth models were used to examine the relationship between homework completion and symptom change. CPT version (with vs without the written trauma account) did not moderate associations between homework engagement and outcomes. Greater pre-treatment PTSD symptoms predicted more Session 1 homework completion, but PTSD symptoms did not predict homework completion at other timepoints. More homework completion after Sessions 2 and 3 was associated with less change in PTSD from Session 2 to Session 4, but larger pre-to-post treatment changes in PTSD. Homework completion after Sessions 2 and 3 was associated with greater symptom change among patients who had fewer years of education. More homework completion after Sessions 8 and 9 was associated with larger subsequent decreases in PTSD. Average homework completion was not associated with client characteristics. In the second half of treatment, homework engagement was associated with less dropout. The results suggest that efforts to increase engagement in homework may facilitate symptom change.
Keywords: Homework, cognitive behavioral therapy, cognitive processing therapy, posttraumatic stress disorder
Cognitive behavioral therapies (CBT) have received extensive empirical support for a variety of mental health disorders (Beck 2005). Because CBT emphasizes the development of strategies to modify problematic cognitions and behaviors, most CBT protocols emphasize the use of between-session homework as a means of practicing and solidifying new skills. Despite the central role of homework in these treatments, the nature of the relationship between homework completion and symptom change is still not well understood. Theoretically, CBT homework assignments provide clients the opportunity to practice the skills they learn in session so that they can begin to apply CBT skills in their daily lives and experience more rapid and sustained symptom relief (Beck, 1979). Research on the clinical impact of homework completion has demonstrated some support for this theory, though there have been some methodological limitations to consider.
In previous research, studies comparing protocols that included homework with those that did not include homework have demonstrated larger effect sizes for protocols that included homework (Kazantzis, Whittington, & Dattilio, 2010; Neimeyer & Feixas, 1990). Other studies on CBT for depression and anxiety have identified a relationship between homework completion and symptom reduction (Bryant, Simons, & Thase, 1999; Burns & Nolen-Hoeksema, 1991; Busch, Uebelacker, Kalibatseva, & Miller, 2010; Conklin & Strunk, 2015; Kazantzis, Deane, & Ronan, 2000). However, some of the research on homework has been conducted with small samples that may be insufficient to detect moderation (e.g., Bryant, Simons, & Thase, 1999, n=26;. Busch et al., n=12; Olatunji et al., n=27). Additionally, while some larger studies (e.g., Burns & Spangler, 2000; Burns & Nolen-Hoeksema, 1991) have identified a positive association between homework completion and symptom improvement, most previous studies have lacked the precision required to understand the temporal relationship between homework completion and symptom change. Burns and Spangler (2000) employed structural equation modeling to examine whether CBT homework completion increased as a result of symptom change among 399 depressed clients. While this methodology represented an advance in identifying the structure of the correlation that has been observed between homework completion and symptom change, the measure used for homework completion was a single retrospective rating of overall compliance, which was assigned by clinicians towards the end of treatment. Other studies on CBT for cocaine dependence improved upon this methodology by using repeated therapist-rated assessments of the degree of homework completion for 60 patients, which was validated in some studies by observer ratings of their review of the homework in session (Carroll, Nich, & Ball, 2005). However, as with previous studies, homework completion scores were aggregated across sessions, and the potential impact of prior symptom change on homework completion was not assessed. Thus, while the findings of these previous studies suggest that homework completion may precede symptom change, relatively little is known about the temporal relationship between homework completion and symptom change.
Establishing temporal precedence of a process variable is critical to understanding the nature of the relationship between that variable and a clinical outcome (Judd & Kenny, 1981). Few studies to date have examined this relationship using session-to-session measures of homework completion and symptom change. Yovel and Safren (2007) did not detect a statistically significant relationship between session-to-session homework completion and attention deficit hyperactivity disorder symptom change, although their sample size was very small (n=16). However, Olatunji and colleagues (2015) demonstrated that CBT homework completion among 27 youth with obsessive-compulsive disorder predicted symptom change at the next session. Studies with larger samples have reported significant relationships between homework and symptom change. Strunk and colleagues (2010) demonstrated that adherence to behavioral methods and homework predicted session-to-session symptom change among 60 depressed outpatients receiving a combination of medication and cognitive therapy. Subsequently, Conklin and Strunk (2015) found that observer ratings of adherence to behavioral strategies and homework predicted session-to-session depression change (n=53), and Schmidt and Woolaway-Bickel (2000) demonstrated that greater homework completion was associated with panic disorder symptom change in some sessions (n=48). Thus, some evidence indicates that homework completion is associated with subsequent decreases in depression and anxiety.
Even if homework predicts symptom change, understanding the relationship between client factors, homework, and symptom change is necessary to inform treatment planning. If clients with particular characteristics are less likely to complete homework, strategies to address barriers to increase compliance may need to be integrated into treatment to optimize its effectiveness. A systematic review revealed that relatively few studies have examined whether client-level characteristics such as age, education level, or diagnostic factors predict homework completion (Scheel, Hanson, & Razzhavaikina, 2004). Those that have examined potential relationships between demographic variables and homework have studied small samples and found very few associations. For example, Bryant, Simons, and Thase (1999; n=25) did not find a relationship between homework completion during cognitive therapy and demographic variables or symptoms, but they did find that a higher number of prior depressive episodes predicted lower homework completion in CBT for depression. Another study found a positive association between homework completion and both age and unemployment status among individuals with panic disorder (Schmidt & Woolaway-Bickel, 2000). The few other studies that have examined the relationship between symptom profiles and homework completion have generally not found an association (Scheel, Hanson, & Razzhavaikina, 2004).
There has been little research on homework in trauma-focused psychotherapy. Because avoidance is a hallmark symptom of posttraumatic stress disorder (PTSD), engaging clients in CBT homework can represent a considerable challenge (Reger et al., 2013). Whether symptom severity or client factors have an impact on homework completion that requires attention to memories, thoughts and feelings related to the trauma requires exploration. These factors inform clinical decision making about patients' appropriateness for trauma-focused treatments, with clinicians citing severity, chronicity, and perceived client ability to engage in homework as factors in deciding whether to provide trauma-focused treatments (Cook, Dinnen, Simiola, Thompson, & Schnurr, 2014; Osei-Bonsu, 2016). Potential predictors of symptom change or homework engagement that have been examined in previous research (Rizvi et al., 2009; Bryant, Simons, & Thase, 1999; Schmidt & Woolaway-Bickrel) such as education level, employment status, severity, or chronicity may predict homework engagement or moderate relationships between homework completion and symptom change. It is also important to understand whether homework completion is predictive of symptom change, rather than increasing or decreasing as symptoms decrease. If patients are not improving, they may begin to do less homework, or they may begin to work harder. Similarly, symptom improvement may motivate patients to do homework because they perceive treatment to be helping, or they might reduce the amount they do if they believe they have already experienced sufficient benefit. If higher levels of homework engagement precede symptom change, rather than resulting from it, homework completion should be prioritized in treatment, whereas the second scenario would indicate that as clients improve, their compliance with treatment may also increase.
Because homework assignments differ over the course of cognitive behavioral trauma treatments (c.f., Cooper et al., 2017; Resick, Monson, & Chard., 2016), examining associations of homework engagement at different time points can provide more specific information about whether and how certain types of between-session activities are associated with symptom change (Cooper et al., 2017). Previous studies have found an association between assigned or completed homework and symptom change in single (Mueser et al., 2008, n=81) and larger, combined datasets (Ho & Lee, 2012, n=227), but only one PTSD study examined the temporal relationship between homework and symptom change through session-to-session analyses. In a study of Prolonged Exposure for PTSD (n=134), higher self-reported imaginal homework adherence predicted greater symptom improvement between sessions and across treatment (Cooper et al., 2017). Relationships between cognitively-oriented homework and PTSD symptom change have not yet been explored.
The current study therefore aimed to examine the temporal relationship between homework completion and session-to-session PTSD symptom change in a CBT for PTSD. Cognitive Processing Therapy (CPT; Resick et al. 2008) is a 12-session protocol that involves the assignment of homework to promote practice of the skills taught in session. In CPT, clients are taught to challenge their beliefs and assumptions about why the trauma occurred, as well as its implications for the way they view themselves and the world. Standardized homework is assigned at each session. CPT has been shown effective for treating PTSD, with or without the assignment of written trauma accounts, across a variety of populations and demonstrated long-term benefits (Bass et al., 2013; Resick et al., 2015; Resick, Williams, Suvak, Monson, & Gradus, 2012). Combined data from two randomized controlled trials of CPT (Resick et al., 2008; Resick, Nishith, Weaver, Astin, & Feuer, 2002) provides a larger sample than most previous studies, which is necessary to examine moderators of treatment outcome (LeGrange et al., 2012).
The primary goal of this study was to examine whether homework completion predicted subsequent symptom change. We hypothesized that homework completion would predict subsequent symptom change after controlling for PTSD symptoms. We also sought to explore associations between homework engagement and dropout and whether treatment condition (CPT with written trauma narrative or CPT without it) was associated with homework completion and symptom change. The second, exploratory aim was to examine demographic and diagnostic predictors of homework completion. Although important to examine for PTSD treatments, based on null findings in the research literature for other disorders (Scheel, Hanson, & Razzhavaikina, 2004), we did not expect that any specific demographic and diagnostic factors would be associated with overall homework completion. Finally, to inform future research, we examined potential patient-level moderators of the relationship between homework and symptom change, identifying potential moderators from previous studies examining associations between patient factors and homework completion or symptom change (Bryant, Simons & Thase, 1999; Rizvi, Vogt, & Resick, 2009; Scheel, Hanson, & Razzhavaikina, 2004; Schmidt & Woolaway Bickrel, 2000).
Methods
Structure of CPT and Homework
Table 1 lists the homework assigned at each session, which varies in content and purpose across the course of treatment. In CPT, progressive worksheets are introduced in each session to help clients evaluate their thinking with regard to the index trauma, and each worksheet builds on previous skills and material. If homework was not completed, at least one worksheet was completed in session with therapist guidance and patients were asked to complete more for homework in addition to the newly assigned homework. While the original CPT protocol incorporated both a cognitive component and written accounts of the trauma, in a dismantling study, the cognitive-only condition demonstrated comparable improvements to the original protocol at posttreatment and 6-month follow-up, although those who were not assigned written trauma accounts improved more quickly (Resick et al., 2008). Thus, it is important to examine whether differences in the homework assignments between the two treatment versions that may have accounted for differences in the trajectory of symptom change. As Table 1 indicates, in the first third of the treatments, homework centers around the use of ABC sheets to differentiate thoughts and feelings, writing an impact statement, and writing trauma narratives in the version of CPT with a written account (after sessions 3 & 4). If written narratives (e.g., impact statement or trauma accounts) were not completed for homework as assigned, they were completed verbally in session and assigned again for homework along with the appropriate worksheets. In the middle phase of treatment, new worksheets are introduced that are intended to support practice of cognitive restructuring skills; each new worksheet is assigned one session earlier in the version of CPT that does not include the written account. In the final third of treatment, the skills are combined into a single worksheet. Patients used the set of skills covered in previous sessions plus the newly introduced skill to complete each subsequent written homework assignment whether or not they had completed previously assigned homework. During the last phase of treatment (sessions 10-12), clients are also instructed to give and receive compliments and do something nice for oneself. In both studies included in this investigation, twice weekly sessions were scheduled.
Table 1. CPT Homework Assignments by Session and Assessment Period.
| Assessment (PDS/PSS) | Timepoint/ Variable† | Session | Assignment/Purpose | |
|---|---|---|---|---|
| CPT without Trauma Account | CPT with Account (if different) | |||
| 0 (baseline) | ||||
| 1 | HW1 | 1 | Impact Statement/Identify beliefs about the trauma's cause and impact | |
| HW2 | 2 | ABC Sheet/Teach clients to identify and differentiate between thoughts and feelings | ||
| HW2 | 3 | ABC sheets /Identifying thoughts and feelings | Also write trauma account & reread daily/ Facilitate emotional processing and remember the context | |
| 2 | HW3 | 4 | Challenging Questions Worksheet/Begin to challenge unhelpful or inaccurate beliefs related to the trauma | Also rewrite trauma account, reread daily; ABC Sheets |
| HW3 | 5 | Problematic Patterns of Thinking Worksheet/Identify patterns of thinking | Challenging Questions Sheet; Re-read account daily | |
| 3 | HW4 | 6 | Challenging Beliefs Worksheet (CBW) related to safety plus other worksheets on specific stuck points/Challenge trauma-related beliefs and identify more balanced ways of thinking | Problematic Patterns of Thinking Worksheet; Re-read account daily until intensity of self-blame and associated emotions diminish |
| HW4 | 7 | Read Safety Module; CBW related to module plus other CBWs on specific stuck points. | ||
| 4 | HW5 | 8 | Read Trust Module; CBW related to module plus other CBWs on specific stuck points | |
| HW5 | 9 | Read Power/Control Module; CBW related to module plus other CBWs on specific stuck points | ||
| 5 | HW6 | 10 | Read Esteem Module; CBW related to module plus CBWs on specific stuck points; Practice giving and receiving compliments daily; Do at least one nice thing for self each day/Challenge cognitions related to esteem and intimacy | |
| HW6 | 11 | Rewrite Impact Statement/Examine how beliefs about the trauma have changed; Continue to give and receive compliments and do nice things for self, Module/CBW on intimacy. | ||
| 6 | 12 | Final session: Use CBW worksheets as needed | ||
| 7 (Post-tx) | ||||
Note: HW = homework completion; PSS/PDS = PTSD Symptom Scale/Posttraumatic Diagnostic Scale.
An average for homework for the two sessions for each timepoint (between assessment points) was taken to derive variables HW2- HW6.
Participants
Participants were all women who consented to participate in one of two different trials of CPT (Resick et al., 2008; Resick et al., 2002) and were assigned to CPT with or without the written trauma account. Sixty-five (78.3%) out of the 85 participants from Study 1 who were randomized to CPT, and in Study 2, 75 out of the 100 participants assigned to either CPT with (n = 39) or without the written account (n = 36) attended at least one session. Data from these 140 participants were used for the current study. Participants across both studies were female victims of sexual or physical violence who met DSM-IV criteria for PTSD at intake based on the Clinician-Administered PTSD Scale (CAPS, Blake et al., 1995), with initial CAPS scores representing severe levels of PTSD symptoms (M = 73.49, SD = 18.86). At intake, the average time since the index trauma was 12.38 years (SD = 13.38, n = 138). The mean age of participants at intake was 34.63 years old (SD = 11.71, n = 139). The majority of the sample was White (n = 99; 70.7%), while 22.1% identified as African American (n = 31). The majority of the sample was single, separated, divorce, or widowed (n = 108, 70.1%), while a minority (n = 32, 22.9%) were married or cohabitating. The mean years of education endorsed by participants was 14.4 (SD = 2.69, n = 139). Treatment in this study, which was reviewed by the university's Institutional Review board, occurred in a university trauma clinic that served traumatized individuals in the St. Louis community and was delivered by masters or doctoral level clinicians who were trained to deliver CPT for the purpose of the studies (see Resick et al., 2002; 2008 for further details regarding recruitment, inclusion criteria, random assignment, and retention rates).
Measures
Demographic factors
Demographic variables, collected by self-report at intake, included age, years of education, race and ethnicity.
PTSD Symptom Scale (PSS; Foa, Riggs, Dancu, & Rothbaum, 1993)/Postraumatic Diagnostic Scale (PDS; Foa, 1995)
PTSD symptoms were assessed using the PSS (Foa, Riggs, Dancu, & Rothbaum, 1993) from Study 1, and its modified version, the PDS (Foa, 1995) from Study 2. Despite slightly different wording, each measure contains 17 items that correspond to the DSM-IV PTSD symptoms, yielding nearly identical scales. Participants indicate the frequency/severity of 17 symptoms in the past week on a scale from 0 = “not at all/only one time” to 3 = “5 or more times per week/almost always”. A total score is obtained by summing the items. For Study 1, the average total score at pre-treatment was 29.30 (SD = 8.75). For Study 2, the average total score at pre-treatment was 29.01 (SD = 9.53). The PSS and PDS have demonstrated high reliability and validity and high diagnostic agreement with other clinical diagnostic measures of trauma related psychopathology (Foa, Cashman, Jaycox, & Perry, 1997). In the current study, alpha coefficients were .83 and .86, respectively. These measures have been combined in previous secondary analyses (e.g. Lester, Resick, Young-Xu, & Artz, 2010; Stein, Dickstein, Schuster, Litz, & Resick, in press). We followed the same procedure to generate a dataset that combined the symptom scores from the two studies.
Beck Depression Inventory (BDI; (Beck, Ward, Mendelsohn, Mock, & Erbaugh, 1961)/Beck Depression Inventory—II (BDI–II; Beck, Steer, & Brown, 1996)
The BDI (Beck, Ward, Mendelsohn, Mock, & Erbaugh, 1961) was used to assess depression symptoms for Study 1 and the BDI-II (Beck, Steer, & Brown, 1996) for Study 2. Both measures contain 21-items assessing depressive symptoms and have been widely used with good reliability and validity (Beck, Steer, & Brown, 1996). Coefficient alpha for the studies were .92 for the treatment study and .91 for the dismantling study. Scores on these measures were standardized prior to combining.
Assessment of Homework Completion
The homework review form assessed how often clients worked on or reviewed homework materials between sessions. For each homework assignment, clients indicated the frequency of homework completion using a 5-point Likert scale (1 = “not at all”, 2 = “less than 2 times”, 3 = “2-5 times”, 4 = “6-10 times”, 5 = “more than 10 times”). Clients and therapists completed the homework review sheet together before each session, using the number of worksheets and other materials that the client completed to corroborate their assessment of the frequency of their homework completion. Use of homework assignments between each assessment point (every other session) were averaged to generate a homework variable for each time period (“HW”) in the current analyses.
Procedures
Clients completed the PSS/PDS and BDI/BDI-II at baseline, prior to sessions 2, 4, 6, 8, 10, and 12, and post-treatment. The homework completion form was completed by the therapist and client together at the beginning of each session. Observer ratings of fidelity were conducted on a randomly selected subset of sessions and indicated that the homework review procedures and forms were completed in 100% of the sessions that were rated.
Data Analyses
Our primary goal was to examine the association between homework completion during a particular week on subsequent changes in PTSD symptoms from that point in treatment through the post-treatment assessment, and to determine whether this differed based on whether patients received the version of CPT that included the trauma account. To accomplish this goal, we evaluated a series of piecewise growth models conducted using multilevel regression (Singer & Willett, 2003) with the Mplus software package (Version 7; Muthén & Muthén, 1998-2012). A piecewise growth model breaks an overall trajectory into multiple distinct phases. The focus of the current manuscript investigated change over time during treatment following the week during which homework was assessed. We conducted piecewise growth modeling (as opposed to only including data points following homework assessment) because the piecewise regression approach uses all of the information available for each participant (before and after the session of interest) to produce the most accurate and powerful estimates of subsequent change.
The right side of Table 2 depicts the time variables that were used in the piecewise models. With the exception of the first phase, between baseline and session 2, two sessions and homework assignments were completed between PTSD symptom assessment points. Thus, Table 2 shows that time was modeled as session number increasing by two from one assessment to the next, with the exception of an increase in one from session 12 to post-treatment. Two time variables were entered as Level-1 (within participants) predictors of PTSD symptoms in each piecewise model. The first time variable was described above and centered (or zeroed) at the second session of each assessment phase. As shown in Table 2, the remaining time variables were modeled as recommended by Singer & Willet (2003).
Table 2. Time Variables and Estimates of Levels and Subsequent Changes of PTSD for Sessions 2-12.
| Session | Intercept | Subsequent ΔPTSD | Time Variables | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Est. (95% CI) | Est. (95% CI) | S2 | S2_PST | S4 | S4_PST | S6 | S6_PST | S8 | S8_PST | S10 | S10_PST | S12 | S12_PST | |
| 0 | -2 | -2 | -4 | -4 | -6 | -6 | -8 | -8 | -10 | -10 | -12 | -12 | ||
| 2 | 27.65(26.29, 29.02) | -18.57(-20.23, -16.91) | 0 | 0 | -2 | -2 | -4 | -4 | -6 | -6 | -8 | -8 | -10 | -10 |
| 4 | 24.52(23.02, 26.01) | -15.52(-17.12, -13.91) | 2 | 0 | 0 | 0 | -2 | -2 | -4 | -4 | -6 | -6 | -8 | -8 |
| 6 | 20.91(19.29, 22.52) | -11.65(-13.16, -10.14) | 4 | 0 | 2 | 0 | 0 | 0 | -2 | -2 | -4 | -4 | -6 | -6 |
| 8 | 17.43(15.73, 19.13) | -7.91(-9.33, -6.49) | 6 | 0 | 4 | 0 | 2 | 0 | 0 | 0 | -2 | -2 | -4 | -4 |
| 10 | 14.01(12.29, 15.72) | -4.16(-5.38, -2.95) | 8 | 0 | 6 | 0 | 4 | 0 | 2 | 0 | 0 | 0 | -2 | -2 |
| 12 | 10.47(8.76, 12.18) | 0.17(-0.96, 1.30) | 10 | 0 | 8 | 0 | 6 | 0 | 4 | 0 | 2 | 0 | 0 | 0 |
| 13 | 11 | 0 | 9 | 0 | 7 | 0 | 5 | 0 | 3 | 0 | 1 | 0 | ||
Note. Time Variables = the time variables used for the regression analysis at each assessment; S = session number, _PST = the second time coefficient; Est. = estimate; 95% CI = 95% confidence interval; ΔPTSD = change in PTSD. Intercept corresponds to the level of PTSD at that assessment.
Three time coefficients were produced from these piecewise models. The intercept term estimated PTSD symptoms assessed prior to the second session of the phase in which homework was assessed (the assessment for which both time variables were equal to zero in Table 2), the coefficient for the first time variable produced an estimate in change in PTSD from that session to post-treatment, and the coefficient for the second time variable represented the difference in rate of change prior to and after the session. The intercept and coefficient for the first time variable were of most interest to the current analyses. To evaluate the impact of homework on subsequent change in PTSD symptoms, homework completion was entered as a Level-2 predictor of each change coefficient, and the primary coefficient of interest was the Homework × time variable interaction, which assessed the impact of homework during that phase (the two sessions between assessment points) on subsequent changes in PTSD symptoms through post-treatment. To evaluate the impact of treatment condition (CPT with or without the trauma account) on the homework effect on subsequent change in PTSD, we added a treatment condition variable and a treatment condition × homework interaction (product) term as Level-2 predictors of each time coefficient. We then conducted a logistic regression analyses with treatment dropout status (0,1) regressed on homework scores to evaluate the relationship between homework and dropout.
For our exploratory analyses, we examined zero-order correlations between patient characteristics and homework completion to determine whether certain characteristics predicted the amount of homework that patients complete. We next conducted exploratory analyses that included patient characteristics that might moderate the relationship between homework completion and symptom change as Level-2 predictors in the piecewise models described above.
Results
Homework and Treatment Outcome
The left side of Table 2 reports the model-derived estimates for PTSD levels and subsequent change in PTSD for each time point. Table 3 reports the coefficients for estimates of the impact of homework completion on the level of PTSD at each assessment point (i.e., impact on the intercept of the piecewise models) and impact of HW on subsequent change on PTSD. Significant effects of homework emerged at two sessions, as described below. The extent to which patients completed the homework assigned in Sessions 2 and 3 (HW2; when ABC worksheets are assigned to help the patient identify and differentiate between thoughts and feelings and at session 3 when first written account or focusing all of the ABC worksheets on the worst traumatic event is assigned) was related to both PTSD levels at Session 4 and subsequent changes from Session 4 to post-treatment. Participants who scored a zero (lowest score) on homework completion during these sessions on average exhibited a 7.24 (d = -.82) decrease in PTSD symptoms from Session 4 to post treatment, while people who scored a five (highest score) exhibited a 22.49 (d = -2.55) decrease in PTSD symptoms during this time period.
Table 3. Homework Use as a Predictor of PTSD Levels and Subsequent Changes in PTSD.
| Homework by Time Interactions (Combined Sample) | Written Account by Homework Interaction (Moderator Analysis) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Relationship | n | b | CR | p | d | b | CR | p | d |
| bHW1→S2 | 139 | 1.38 | 1.51 | .132 | 0.26 | 0.36 | 0.20 | .842 | 0.03 |
| HW1→ΔS2-PST | 0.03 | 0.31 | .758 | 0.05 | -0.27 | -1.33 | .183 | -0.23 | |
| HW2→S4 | 136 | 2.65 | 2.83 | .005 | 0.48 | -2.48 | -1.15 | .251 | -0.20 |
| HW2→ΔS4-PST | -0.34 | -2.82 | .005 | -0.48 | -0.18 | -0.65 | .517 | -0.11 | |
| HW3→S6 | 128 | 1.95 | 1.83 | .068 | 0.32 | -3.99 | -1.63 | .104 | -0.29 |
| HW3→ΔS6-PST | -0.27 | -1.79 | .074 | -0.32 | 0.49 | 1.56 | .120 | 0.27 | |
| HW4→S8 | 119 | 1.26 | 0.68 | .496 | 0.12 | -5.31 | -1.37 | .170 | -0.25 |
| HW4→ΔS8-PST | 0.07 | 0.23 | .820 | 0.04 | -0.43 | -0.74 | .457 | -0.14 | |
| HW5→S10 | 119 | 1.26 | 1.32 | .187 | 0.24 | -0.17 | -0.07 | .946 | -0.01 |
| HW5→ΔS10-PST | -0.66 | -2.49 | .013 | -0.46 | 0.18 | 0.29 | .774 | 0.05 | |
| HW6→S12 | 89 | -0.59 | -0.33 | .739 | -0.07 | -3.76 | -1.01 | .313 | -0.21 |
| HW6→ΔS12-PST | -0.37 | -0.37 | .712 | -0.08 | -0.59 | -0.26 | .795 | -0.06 | |
Note. Results on the left side indicate findings for the entire sample, homework by time interaction. Analyses represented on the right side included an interaction between time and a variable indicating whether or not the trauma account was assigned. HW = homework completion, S = session, n = sample size for that analysis, CR = critical ratio (b/standard error of b, which follows a z-distribution), p = p -value, d = effect size estimate calculated using , with .20, .50, and .80 indicating the cutoffs for small, medium, and large effect sizes. The Level-1 regression equation for the analysis was Yij = bo + b1Time1 + b2Time2 + rij, where Yij = PTSD symptoms for participant at assessment i for participant j, bo = the regression intercept (PTSD levels at that session); b1Time1 = Change in PTSD from that session to the posttreatment assessment; PTSD Time2 = the difference in rate of change in PTSD before and after the session, and rij = the level-1 residual. All of these terms as well as homework use × time parameters interactions were included in the model. However, to facilitate interpretation of the results, only the parameters representing the impact of HW on PTSD levels and subsequent change are presented on the left, and the main effects of Time, HW, and the moderator, as well as all two way and three way interactions were included in the model reported on the right. Coefficients for the entire model can be obtained from the authors.
Figure 1 shows that participants who completed more homework during the HW2 phase, comprising Sessions 2 and 3 of treatment, initially exhibited higher PTSD levels at Session 4 and experienced larger subsequent decreases in PTSD relative to participants who completed less homework that was assigned in Sessions 2 and 3. Mplus allows intercepts and slopes to be modeled as predictors or outcomes at Level-2. Because homework completion during the phase comprising Sessions 2 and 3 was associated with higher Session 4 PTSD symptom levels, but larger decreases in PTSD symptoms, we evaluated a model with the two time coefficients regressed on the Level-1 intercept (which represented PTSD levels at Session 4) to evaluate change over time when controlling for Session 4 PTSD levels. In this model, the impact of homework after Sessions 2 and 3 on subsequent PTSD approached statistical significance (b = -0.21, CR = -1.86, p = 0.063, d = -0.32). Thus, the larger decrease in PTSD symptoms exhibited from Session 4 to post-treatment by participants who completed more homework at Sessions 2 and 3 relative to those who completed less homework was largely accounted for by differences in PTSD symptoms prior to Session 4. Participants who completed more homework during this phase had exhibited more PTSD symptoms prior to Session 4 than participants who completed less homework assigned in Sessions 2 and 3. Participants who completed more homework during this phase also exhibited larger decreases from Session 4 to post-treatment. While completion of homework assigned in Sessions 2 and 3 was not associated with post-treatment PTSD scores, patients who were scoring higher in symptoms prior to Session 4 and did more homework at Sessions 2 and 3 were able to catch up to their counterparts who were experiencing lower symptoms during this earlier phase of treatment.
Figure 1.
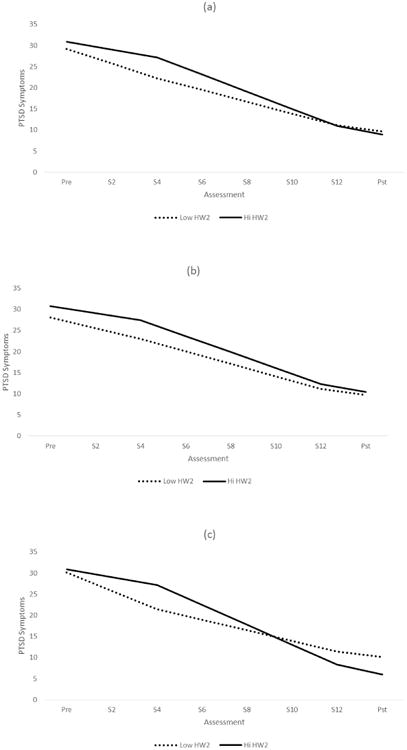
The impact of sessions 2 and 3 homework: a) overall, b) at high levels of years of education, and c) at low levels of years of education. HW2 = Homework completion for sessions 2 and 3
The amount of homework completed during the phase comprising Sessions 8 and 9 (when Challenging Beliefs worksheets, which guide the patient in challenging their beliefs and identifying more adaptive beliefs, and modules on Trust and Power and Control are assigned) also predicted subsequent changes in PTSD symptoms. Participants who scored a zero (lowest score) on homework use during this time period on average exhibited a .01 (d < -.01) decrease in PTSD symptoms from Session 10 to post treatment, while people who scored a 3.75 (highest score) exhibited a 5.93 (d = -.49) decrease in PTSD symptoms during this time period. However, as indicated in Table 4, the amount of homework completed after Sessions 8 and 9 was not associated with Session 12 PTSD symptoms, and when controlling for Session 10 PTSD symptoms, the impact of homework completion on symptom change over the remainder of the protocol remained significant (b = -0.56, CR = -2.134, p = 0.033, d = -0.39). While on average, participants who completed more homework assigned in Sessions 8 and 9 reported fewer PTSD symptoms at post-treatment, the effect was small, and this difference did not approach statistical significance (b = -0.74, CR = -1.027, p = 0.471, d = -0.13).
Table 4. Descriptive Statistics and Bivariate Associations.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | n | M(SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | --- | 139 | 34.63 (11.71) | |||||||||||
| 2 Years of Education | .08 | --- | 139 | 14.4 (2.69) | ||||||||||
| 3 Months Since Rape | .57** | .11 | --- | 138 | 148.63 (160.52) | |||||||||
| 4 Minority Status | .08 | -.01 | .21* | --- | 140 | 0.29 (0.46) | ||||||||
| 5 Pre-Treatment PTSD symptoms | -.11 | -.02 | -.15 | -.07 | --- | 139 | 29.58 (8.93) | |||||||
| 6 Pre-Treatment Depression symptoms | .09 | -.09 | .01 | -.09 | .50** | --- | 138 | 26.04 (10.97) | ||||||
| 7 HW1 (session 1) | .01 | -.06 | .05 | .03 | .20* | .22* | --- | 139 | 3.16 (0.86) | |||||
| 8 HW2 (sessions 2 and 3) | -.12 | .21* | -.11 | -.06 | .15 | -.04 | .13 | --- | 136 | 2.69 (0.94) | ||||
| 9 HW3 (sessions 4 and 5) | -.04 | .03 | -.02 | -.06 | .05 | -.01 | .03 | .53** | --- | 128 | 2.03 (0.86) | |||
| 10 HW4 (sessions 6 and 7) | .15 | -.03 | .14 | .04 | .03 | .04 | .22* | .03 | .14 | --- | 119 | 2.34 (0.49) | ||
| 11 HW5 (sessions 8 and 9) | -.08 | .05 | -.13 | -.14 | -.10 | -.13 | -.12 | .64** | .65** | -.08 | --- | 119 | 1.91 (0.92) | |
| 12 HW6 (session 10 and 11) | -.04 | .28** | -.22* | -.09 | .12 | -.06 | -.12 | .65** | .66** | .18 | .65** | --- | 89 | 2.15 (0.81) |
| 13 Average HW Use | -.11 | .03 | -.14 | -.04 | .16 | .04 | .39** | .77** | .80** | .30** | .77** | .81** | 140 | 2.47 (0.64) |
Note:
p < .05,
p < .01.
PSS/PDS = PTSD Symptom Scale/Posttraumatic Diagnostic Scale; HW = homework completion; n = sample size; M = mean; SD = standard deviation. Because some data were missing in the original data set, sample sizes are noted with descriptive statistics.
The righthand side of Table 3 presents results of a moderator analysis to determine whether treatment version (CPT with or without the account) was associated with symptom change. Treatment version did not moderate the relationship between homework and symptom change. This held true even during the time periods when the trauma account would have been assigned, completed, and reviewed (HW2 and HW3) or at the subsequent assessment period, when worksheet assignments between the two versions of the treatment (as described in Table 1).
We next conducted a series of logistic regression analyses examining HW as a predictor of whether or not participants dropped out of treatment. Twenty-five (18.0%) of the 139 participants with data for Session 1 (HW1) dropped out of treatment. HW1 did not significantly predict dropout status (b = .35, CR = 1.39, p = .165, OR1 = 1.41, OR/SD = 1.65). HW2 (Session 2 and 3, b = -.20, CR = -.78, p = .438, OR = .82, OR/SD = .88) and HW3 (Session 4 and 5, b = .23, CR = .67, p = .501, OR = 1.25, OR/SD = 1.46) scores also did not significantly predict treatment dropout. Five (4.2%) of the 119 participants who had HW4 scores available dropped out of treatment. HW4 (Session 6 and 7) homework scores predicted dropout (b = -2.96, CR = -2.43, p = .015, OR = .05, OR/SD = .10) such that a one SD increase in homework completion was associated with a 9.55 times decrease in the likelihood of dropping out. Similarly, six (5%) of the 119 participants who had HW5 scores available dropped out of treatment with HW5 (sessions 8 and 9) scores inversely related to dropout (b = -1.43, CR = -2.69, p = .007, OR = .24, OR/SD = .26) such that a one SD increase in homework completion was associated with a 3.82 times decrease in the likelihood of dropping out. Only four (4.5%) of 89 participants with HW6 (session 10-11) scores available dropped out of treatment. The association between HW6 and dropout approached statistical significance (b = -4.47, CR = -1.69, p = .090, OR = .01, OR/SD = .01). However the odds ratios were quite small and indicated a one SD increase in homework completion was associated with at 72.89 times decrease in the likelihood of dropping out, suggesting the failure to reach statistical significance may have been due having such a small number of dropouts during this phase.
Relationship between baseline characteristics, homework completion, and symptom change
Table 4 displays zero-order correlations among demographic variables, initial PTSD symptom levels, and the HW variables between each PTSD assessment point, as well as descriptive statistics for these variables. The scores indicate that on average, clients endorsed doing homework either less than two times or two to five times between sessions, which were scheduled twice per week. As indicated in Table 4, the initial PTSD scores were positively correlated with HW1 (Session 1; r = .20, p = .016), such that those endorsing higher initial PTSD symptoms reported completing the first homework assignment more frequently. Initial depression scores were positively correlated with HW1 (Session 1) in the same manner; r = .20, p = .011. Number of years of education was significantly, positively associated with completion of homework assigned in Sessions 3 and 4 (HW2; r = .21, p = .015) and Sessions 10 and 11 (HW6; r = .28, p = .008). Number of years since the index trauma was negatively associated with HW6 (r = -.22, p = .044). Average homework completion did not correlate with any other demographic or baseline variable. The supplemental table summarizes the findings of the exploratory analyses examining moderators of the impact of homework on changes in PTSD. Only one significant moderator by homework interaction emerged, that of years of education and completion of homework assigned after Sessions 2 and 3 (HW2). Figure 1b and 1c shows that completion of the homework assigned in Sessions 2 and 3 was associated with better outcomes for patients with fewer years of formal education compared to those who endorsed more years of education.
Discussion
With data from two clinical trials of CPT, this study examined the association between homework completion and symptom change in a cognitive behavioral therapy. We employed a session-to-session measure of homework completion to investigate the relationship between specific homework activities and subsequent symptom change. We found some support for the hypothesis that homework completion is associated with greater overall symptom change, with homework engagement at certain timepoints associated with subsequent symptom change. Whether patients received the version of CPT that included a written trauma account or the version that did not include the account, did not appear to moderate the association between homework completion and symptom change at any timepoint in the treatment. Our results regarding the relationship between homework completion and subsequent dropout also suggested that homework completion in the latter half of treatment may be a good indicator of treatment engagement as patients who completed more homework were less likely to drop out. Finally, we found evidence that while certain client characteristics were associated with early homework completion, they do not predict overall engagement in homework. For the most part, they did not moderate the relationship between homework completion and treatment outcomes, with one exception (years of education).
More frequent completion of homework assigned in Sessions 2 and 3 was associated with smaller short-term decreases in PTSD symptoms at Session 4 regardless of whether the trauma account was assigned in Session 3. However, homework completion during this time period predicted greater symptom change over the course of treatment. While this may have been because in part there was more room for improvement among those who completed more homework, it suggests that those with higher symptoms in Sessions 2 and 3 may be able to “catch up” to those with lower symptoms by completing more homework. In both forms of the treatment (with and without the trauma account), homework assignments in these early sessions require attention to the index trauma and identification of associated thoughts and feelings. While the decreases in avoidance required to do this work may initially reduce the amount of symptom change that patients experience, or even occasionally result in a transient increase in symptoms (Larsen, Stirman, Smith, & Resick, 2016), working on the traumatic event between sessions ultimately appears to be beneficial. These findings suggest that clients, especially those who are experiencing less improvement in early sessions, should be encouraged to complete more homework during these sessions, and reassured that doing so, even if challenging in the short-term, is associated with better longer-term results.
Because patients with higher levels of education completed more homework assigned in Sessions 2 and 3, but those with lower levels of education appeared to benefit more from these assignments, it may be important for clinicians to encourage those with lower levels of education to complete assignments early in treatment. Education has not consistently been identified as a prognostic variable in previous CBT research, but it was found to predict dropout in a previous study that examined treatment outcome in CPT and Prolonged Exposure (Rizvi, Vogt, & Resick, 2009). Findings related to education should be replicated, particularly because they were not significant at every timepoint, but is possible that individuals with lower levels of education may struggle more with some concepts of CPT and that additional practice is required early on in order to maximize treatment effectiveness and engagement. Additional practice at identifying thoughts and differentiating them from feelings may benefit individuals with lower levels of education by promoting a sense of mastery and providing a solid foundation on which new skills are introduced.
The frequency of homework completion decreased somewhat during the middle weeks of therapy before increasing over the last two assignments. Particularly in Sessions 6 and 7, the restricted range may have made it difficult to discern whether increased engagement was related to symptom change, and completion of the assignments in these two sessions was not correlated with completion of earlier assignments. It is possible that during the middle period of treatment, cognitive work completed during sessions impacted symptom change in addition to (or instead of) homework completed outside of session, which is designed to reinforce the work done within sessions. The nature of the homework may also play a role in this pattern of change. A worksheet (Challenging Beliefs Worksheet) that combines all other cognitive restructuring elements and takes longer to complete, especially in the beginning, was introduced during this time period. Participants may have had some difficulty completing this assignment without additional practice and guidance, which may have limited the assignment's impact on symptom change when it was first introduced. In contrast, homework completion for Sessions 8 and 9, which occur after that worksheet was introduced and practiced in earlier sessions, predicted a decrease in PTSD symptoms. Thus, even towards the end of treatment, completion of homework is associated with additional improvement, with those who completed more assignments during this phase experiencing an additional benefit of nearly a 6-point difference, which can be considered clinically meaningful (Larsen et al., 2016).
The participants in this study represented a diverse population of multiply traumatized, low income women who, for the most part, had not completed college and endorsed significant symptoms of depression. Our findings indicated that they were able to practice and benefit from a standardized set of homework activities, and that the relationship between homework completion and symptom change was not due to an association with number of years of education. These findings have implications for the implementation of CPT outside the context of research settings. Considered in conjunction with other studies of CPT conducted with diverse populations (Schulz, Huber, & Resick, 2006), our results support a growing body of literature suggesting that CPT homework can be assigned to clients of diverse cultural and educational backgrounds. Homework completion was associated with PTSD symptom change, at least for participants with lower levels of education and those with higher symptoms in early sessions. However, because this sample comprised only women who experienced interpersonal violence index traumas, future research should examine the impact of homework completion in other populations of clients who experience PTSD. Of course, it is also possible that individuals with certain characteristics such as motivation that were not measured in this study are more likely to complete homework, and that homework is a proxy for a particular trait or psychological process that impacts treatment, such as willingness to learn new skills (Burns & Nolen-Hoeksema, 1991) or motivation (Huppert et al., 2006). While previous research on client characteristics, including factors such as resourcefulness were not related to homework completion (Bryant, Simons, & Thase, 1999), factors such as motivation, self-efficacy, or expectancies have not been examined in relation to homework. Other factors such as the therapeutic alliance, fidelity to the treatment, and patient receptivity/resistance were not measured in session, but may impact treatment outcome (DeRubeis, Brotman, & Strunk, 2005).
There is a relative dearth of studies examining the impact of homework completion on treatment outcome in CBTs for PTSD, and the current analyses used data from two RCTs that were not specifically designed to assess the impact of homework completion on symptom change. Therefore, rather than a conservative or strict test of a well-developed theoretical model about the relative importance of different homework assignments, the current study was conducted in the spirit of providing research findings that can facilitate the generation of hypotheses for future studies designed specifically to assess the impact of homework completion on symptom change. Although our investigation of homework was one of the largest to date, we did not have a sufficient sample size to examine homework and their interactions with time simultaneously and instead evaluated the impact of homework between each PTSD assessment in separate models. Because we conducted multiple analyses, particularly for our exploratory moderator analyses, these findings should therefore be interpreted with caution and replicated in future research. However, the effect sizes for our findings regarding Sessions 2 and 3, including that of education as a potential moderator, suggest that they should be investigated further. Replication of our findings with a very large sample and a more conservative, confirmatory analytic approach is necessary.
The current study did not assess the quality of the homework completed or the amount of time spent on the assignments, which are limitations. While our results suggest that irrespective of quality, the frequency of engagement with homework assignments is associated with clinical improvement, it is possible that an assessment of quality or quantity would allow for a greater understanding of the relationship between homework completion and symptom change, as prior research suggests that quality may be more predictive of outcomes than quantity (Schmidt & Woolaway-Bickel, 2000). The current study also did not examine whether specific assignments or elements of homework led to symptom change. Although the homework assignments built on one another, it is possible that clients who did not complete an assignment and had it re-assigned in addition to current homework may have experienced different levels of session-to-session symptom change than those who completed homework on time. Furthermore, if clients were engaged in the form of CPT that does not include a trauma account, they began using some cognitive worksheets sooner and more Socratic questioning than their counterparts who completed the written account. Relationships between specific homework activities and symptom change warrants exploration in a dataset in which symptoms were assessed at every session. Because samples for later analyses were smaller due to treatment dropout, results for these sessions in particular require replication.
While observer ratings of homework completion may also enhance our understanding of the role of homework in CBT, previous research has suggested that self-reports of homework completion, when collected in each session, can be reliable sources of data (Burns & Spangler, 2000; Kassler & Neimeyer, 1997). A recent meta-analysis suggested that in studies of homework and clinical outcomes, combined therapist and client ratings are associated with greater effect sizes than observer ratings (Mausbach et al., 2010). The fact that the questionnaire used in this study was completed by therapists and clients together, using the completed homework worksheets to corroborate clients' reports of homework activities, strengthened our confidence in these assessments as reliable estimates of homework completion. In future research, session-to-session (rather than every other session) assessments will allow greater precision in identifying relationships between specific assignments and subsequent symptom change.
Despite these limitations, this study provides additional support for the theory that practicing skills between sessions through completion of homework may be associated with greater symptom improvement (Beck, 1979). It adds to a small literature suggesting that patients in trauma-focused treatment who complete more homework (which focuses on extending key aspects of treatment between sessions) experience decreases in PTSD that are greater than those who are less engaged in homework (Cooper et al., 2017; Mueser et al., 2008). Similar to other recent findings (Cooper et al., 2017), our results suggest that either certain assignments, or homework at specific timepoints, may be particularly important. Furthermore, this study suggests that later in treatment, homework completion may indicate greater engagement in treatment and a lower likelihood of dropout. Collectively, these studies point to compelling directions for future experimental and naturalistic investigations of associations between homework and symptom change.
Homework is sometimes perceived as a burden on clients, and both clinicians who are learning CBT and clients who are beginning treatment may struggle to integrate it into treatment (Waltman, Hall, McFarr, Beck, & Creed, 2016). Further research on homework will be useful when conducted in routine care settings, because there have been very few empirical studies on compliance with and impact of homework during routine clinical practice. However, our findings suggest that completion of homework is associated with clinical improvements, and that encouraging early and frequent homework activities may enhance treatment outcome.
Supplementary Material
Highlights.
Examined associations between patient factors, CPT homework, and symptom change.
Homework completion after certain sessions predicted subsequent symptom change.
Few patient characteristics predicted CPT homework completion.
Education moderated associations between Session 2 and 3 homework and symptom change.
Acknowledgments
The datasets used for this research was collected through studies funded by the National Institute of Mental Health (NIH-1 R01-MH51509 and NIH-2 R01-MH51509), awarded to Dr. Resick while she was at University of Missouri, St. Louis. Dr. Gutner's work was supported by a career development award from the National Institute of Mental Health (1K23MH103396)
Footnotes
OR = Odds Ratio. With continuous predictors it is difficult to interpret the strength (i.e., effect size) of odds ratios because the unit of continuous measures is usually arbitrary. Therefore, we also calculated the odds ratio per standard deviations of the predictor variable (OR/SD). The OR/SD values can be interpreted as the increase in the likelihood of dropping out of treatment associated with a one standard deviation increase in HW scores.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Bass JK, Annan J, McIvor Murray S, Kaysen D, Griffiths S, Cetinoglu T, et al. Bolton PA. Controlled trial of psychotherapy for Congolese survivors of sexual violence. New England Journal of Medicine. 2013;368(23):2182–2191. doi: 10.1056/NEJMoa1211853. [DOI] [PubMed] [Google Scholar]
- Beck AT. Cognitive therapy and the emotional disorders. New York: Penguin Books USA; 1979. [Google Scholar]
- Beck AT. The Current State of Cognitive Therapy: A 40-Year Retrospective. Archives of General Psychiatry. 2005;62(9):953–959. doi: 10.1001/archpsyc.62.9.953. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK. Beck depression inventory-II [Measurement instrument] San Antonio, TX: The Psychology Corporation; 1996. [Google Scholar]
- Bryant M, Simons AD, Thase ME. Therapist skill and patient variables in homework compliance: controlling an uncontrolled variable in cognitive therapy outcome research. Cognitive Therapy and Research. 1999;23(4):381–399. doi: 10.1023/a:1018703901116. [DOI] [Google Scholar]
- Burns D, Nolen-Hoeksema S. Coping styles, homework compliance, and the effectiveness of cognitive-behavioral therapy. Journal of Consulting & Clinical Psychology. 1991;59(2):305–311. doi: 10.1037/0022-006X.59.2.305. [DOI] [PubMed] [Google Scholar]
- Burns D, Spangler D. Does psychotherapy homework lead to improvements in depression in cognitive-behavioral therapy or does improvement lead to increased homework compliance? Journal of Consulting & Clinical Psychology. 2000;68(1):46–56. doi: 10.1037/0022-006X.68.1.46. [DOI] [PubMed] [Google Scholar]
- Busch A, Uebelacker L, Kalibatseva Z, Miller I. Measuring homework completion in behavioral activation. Behavior Modification. 2010;34(4):310–329. doi: 10.1177/0145445510373384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carroll KM, Nich C, Ball SA. Practice makes progress? Homework assignments and outcome in treatment of cocaine dependence. Journal of Consulting & Clinical Psychology. 2005;73(4):749–755. doi: 10.1037/0022-006X.73.4.749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conklin LR, Strunk DR. A session-to-session examination of homework engagement in cognitive therapy for depression: Do patients experience immediate benefits? Behaviour Research and Therapy. 2015;72:56–62. doi: 10.1016/j.brat.2015.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook JM, Dinnen S, Simiola V, Thompson R, Schnurr PP. VA residential provider perceptions of dissuading factors to the use of two evidence-based PTSD treatments. Professional Psychology: Research and Practice. 2014;45(2):136–142. doi: 10.1037/a0036183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper AA, Kline AC, Graham B, Bedard-Gilligan M, Mello PG, Feeny NC, Zoellner LA. Homework “dose,” type, and helpfulness as predictors of clinical outcomes in prolonged exposure for PTSD. Behavior Therapy. 2017;48(2):182–194. doi: 10.1016/j.beth.2016.02.013. [DOI] [PubMed] [Google Scholar]
- DeRubeis RJ, Brotman MA, Gibbons CJ. A conceptual and methodological analysis of the nonspecifics argument. Clinical Psychology: Ccience and Practice. 2005;12(2):174–183. doi: 10.1093/clipsy.bpi022. [DOI] [Google Scholar]
- Foa EB. The Posttraumatic Diagnostic Scale (PDS) manual. Minneapolis, MN: National Computer Systems; 1995. [Google Scholar]
- Foa EB, Cashman L, Jaycox L, Perry K. The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Diagnostic Scale. Psychological Assessment. 1997;9(4):445–451. doi:1040-3590/97/S3.00. [Google Scholar]
- Foa EB, Riggs DS, Dancu CV, Rothbaum B. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress. 1993;6(4):459–474. doi: 10.1002/jts.2490060405. [DOI] [Google Scholar]
- Ho MSK, Lee C. Cognitive behaviour therapy versus eye movement desensitization and reprocessing for post-traumatic disorder–is it all in the homework then? Revue Européenne de Psychologie Appliquée/European Review of Applied Psychology. 2012;62(4):253–260. doi: 10.1016/j.erap.2012.08.001. [DOI] [Google Scholar]
- Huppert JD, Barlow DH, Gorman JM, Shear MK, Woods SW. The interaction of motivation and therapist adherence predicts outcome in cognitive behavioral therapy for panic disorder: Preliminary findings. Cognitive and Behavioral Practice. 2006;13(3):198–204. doi: 10.1016/j.cbpra.2005.10.001. [DOI] [Google Scholar]
- Judd CM, Kenny DA. Estimating the effect of social interventions. New York: Cambridge University Press; 1981. [Google Scholar]
- Kassler DM, Neimeyer DM. Homework compliance and skill acquisition as predictors of outcome in cognitive-behavioral group therapy for depression. 1997 doi: 10.1080/16506070801981240. Unpublished manuscript. [DOI] [PubMed] [Google Scholar]
- Kazantzis N, Deane F, Ronan K. Homework assignments in cognitive and behavioral therapy: A meta-analysis. Clinical Psychology: Science & Practice. 2000;7(2):188–202. doi: 10.1093/clipsy.7.2.189. [DOI] [Google Scholar]
- Kazantzis N, Whittington C, Dattilio F. Meta-analysis of homework effects in cognitive and behavioral therapy: A replication and extension. Clinical Psychology: Science & Practice. 2010;17(2):144–156. doi: 10.1111/j.1468-2850.2010.01204. [DOI] [Google Scholar]
- Lester KM, Resick PA, Young-Xu Y, Artz CE. Impact of ethnicity on early treatment termination and outcomes in PTSD treatment. Journal of Consulting and Clinical Psychology. 2010;78(4):480–489. doi: 10.1037/a0019551. [DOI] [PubMed] [Google Scholar]
- Le Grange D, Lock J, Agras WS, Moye A, Bryson SW, Jo B, Kraemer HC. Moderators and mediators of remission in family-based treatment and adolescent focused therapy for anorexia nervosa. Behaviour research and therapy. 2012;50(2):85–92. doi: 10.1016/j.brat.2011.11.003. doi:doi:10.1016/j.brat.2011.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueser KT, Rosenberg SD, Xie H, Jankowski MK, Bolton EE, Lu W, et al. Wolfe R. A randomized controlled trial of cognitive-behavioral treatment for posttraumatic stress disorder in severe mental illness. Journal of Consulting and Clinical Psychology. 2008;76(2):259–271. doi: 10.1037/0022-006X.76.2.259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neimeyer RA, Feixas G. The role of homework and skill acquisition in the outcome of cognitive therapy for depression. Behavior Therapy. 1990;21(3):281–292. doi: 10.1016/S0005-7894(05)80331-4. [DOI] [PubMed] [Google Scholar]
- Osei-Bonsu PE, Bolton RE, Stirman SW, Eisen SV, Herz L, Pellowe ME. Mental health providers' decision-making around the implementation of evidence-based treatment for PTSD. The Journal of Behavioral Health Services & Research. 2017;44(2):213–223. doi: 10.1007/s11414-015-9489-0. [DOI] [PubMed] [Google Scholar]
- Reger GM, Hoffman J, Riggs D, Rothbaum BO, Ruzek J, Holloway KM, Kuhn E. The “PE coach” smartphone application: An innovative approach to improving implementation, fidelity, and homework adherence during prolonged exposure. Psychological Services. 2013;10(3):342. doi: 10.1037/a0032774. [DOI] [PubMed] [Google Scholar]
- Rizvi SL, Vogt DS, Resick PA. Cognitive and affective predictors of treatment outcome in cognitive processing therapy and prolonged exposure for posttraumatic stress disorder. Behaviour Research and Therapy. 2009;47(9):737–743. doi: 10.1016/j.brat.2009.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resick PA, Galovski TE, Uhlmansiek MOB, Scher CD, Clum GA, Young-Xu Y. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. Journal of Consulting and Clinical Psychology. 2008;76(2):243. doi: 10.1037/0022-006X.76.2.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resick PA, Nishith P, Weaver TL, Astin MC, Feuer CA. A comparison of cognitive-processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. Journal of Consulting and Clinical Psychology. 2002;70(4):867. doi: 10.1037/0022-006X.70.4.867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resick PA, Wachen JS, Mintz J, Young-McCaughan S, Roache JD, Borah AM, et al. Litz BT. A randomized clinical trial of group cognitive processing therapy compared with group present-centered therapy for PTSD among active duty military personnel. Journal of Consulting and Clinical Psycholog. 2015;83(6):1058. doi: 10.1037/ccp0000016. [DOI] [PubMed] [Google Scholar]
- Resick PA, Williams LF, Suvak M, Monson CM, Gradus J. Long-term outcomes of cognitive-behavioral treatments for posttraumatic stress disorder among female rape survivors. Journal of Consulting & Clinical Psychology. 2012;80(2):201–210. doi: 10.1037/a0026602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt N, Woolaway-Bickel K. The effects of treatment compliance on outcome in cognitive-behavioral therapy for panic disorder: Quality versus quantity. Journal of Consulting & Clinical Psychology. 2000;68(1):13–18. doi: 10.1037//0022-006X.68.1.13. [DOI] [PubMed] [Google Scholar]
- Schulz PM, Huber LC, Resick PA. Practical adaptations of cognitive processing therapy with Bosnian refugees: Implications for adapting practice to a multicultural clientele. Cognitive and Behavioral Practice. 2006;13(4):310. doi: 10.1016/j.cbpra.2006.04.019. [DOI] [Google Scholar]
- Stein NR, Dickstein BD, Schuster J, Litz BT, Resick PA. Trajectories of response to treatment for posttraumatic stress disorder. Behavior Therapy. 2012;43(4):790–800. doi: 10.1016/j.beth.2012.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strunk DR, Brotman MA, DeRubeis RJ, Hollon SD. Therapist competence in cognitive therapy for depression: predicting subsequent symptom change. Journal of Consulting and Clinical Psychology. 2010;78(3):429–437. doi: 10.1037/a0019631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waltman S, Hall BC, McFarr LM, Beck AT, Creed TA. In-Session Stuck Points and Pitfalls of Community Clinicians Learning CBT: Qualitative Investigation. Cognitive and Behavioral Practice. 2017;24(2):256–267. doi: 10.1016/j.cbpra.2016.04.002. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.