

Abstract
Background
Isolated Tricuspid valve infective endocarditis is an infrequent diagnosis, the incidence of Tricuspid valve infective endocarditis accounts for 5% and up to 15% of IE cases.
Aim
To assess the prevalence and the echocardiographic characteristics of tricuspid valve endocarditis among patients presented to the echo lab of Ain Shams hospital from 1-1-2016 to 1-1-2017.
Methods
This is a retrospective study which included all patients presented to the echo lab of Ain Shams university hospital from 1st January 2016 to 1st January 2017, the total number of patients were 8376, patients with infective endocarditis were 278, and patients with tricuspid valve endocarditis were 51 patients respectively. Complete transthoracic echocardiography was done for all patients and data was retrieved from a locally designed electronic database of cardiology department at Ain shams hospitals.
Results
The incidence of TVIE was (17.7%) of all cases of IE, and (0.67%) of all cases attending the echo lab during the study period. The mean age group in our study was (31.1 ± 7.8) and about 84.3% of patient’s age was between 20 and 40 years. Higher incidence of IE was in males (90.2%) than in females (9.8%) with a ratio of 9:1. The vegetations were detected in one leaflet in 33 patients (64.7%), two leaflets in 9 patients (17.6%) and in the three TV leaflets in 7 patients (13.7). The most affected leaflet was the anterior leaflet that was affected in 38 patients constituting about 74.5% of patients. The size of vegetations was large >15 mm in 40 patients (78.4%).
The most encountered echocardiographic complication was severe TR, detected in 40 patients (78.4%) and abscess formation was the least present, detected in only 2 patients (3.9%).
Conclusion
The incidence of TV IE is increasing with male gender predominance, and affects mainly young age groups. TV IE represented 0.6% of all patients, and 17.7% of IE cases. The main echocardiographic feature of TV IE is vegetations which were characterized by being large, highly mobile, and affecting mainly anterior TV leaflet. The main echocardiographic complication is severe TR, but abscess formation was infrequent.
Keywords: Infective endocarditis, TV endocarditis, Echocardiography
1. Introduction
Infective endocarditis (IE) is a disease characterized by high morbidity and mortality. Although first described in the mid-16th century, the Gulstonian lectures by Osler to the Royal College of Physicians in 1885 created the impetus for the systematic study of IE. Beginning in the early 1900s, investigators have frequently reported on the manifestations of this disease.1 However despite advances during the past century in diagnosis, medical therapy,2 and surgical treatment.3 The in-hospital mortality rate for patients with IE is close to 20% with 1-year mortality approaching 40%.4 Several complications may occur during the course of IE, including embolic events, perivalvular extension, and valvular destruction causing heart failure. These main complications are the cause of the persistent high morbidity and mortality of the disease,5 prolonged hospitalization and also the main reasons for surgery, which is performed during the active phase of the disease (early surgery) in about half of patients with acute IE.4, 6 The reasons why TVIE is rare are thought to be the tricuspid and pulmonary valves are not strained because of low pressure; and low oxygen saturation.7 Nevertheless, reports of TVIE are growing because of the increasing frequency of drug-user patients,8 also The recent exponential increase in implantable devices such as pacemakers, defibrillators, and indwelling central venous catheters may lead to an overall increase in the number of TV IE cases.9
2. Aim
To assess the prevalence and the echocardiographic characteristics of tricuspid valve endocarditis among patients presented to the echo lab of Ain Shams hospital from 1-1-2016 to 1-1-2017.
3. Methods
This is a retrospective study which included all patients presented to the echo lab of Ain Shams hospital from 1st January 2016 to 1st January 2017, the total number of patients were 8376, patients with infective endocarditis were 278, and patients with tricuspid valve endocarditis were 51 patients respectively. We studied the prevalence of TV IE patients and their echocardiographic characteristics. Data was retrieved from a locally designed electronic database of cardiology department at Ain shams hospitals.
Complete transthoracic echocardiography was done for all patients. All echocardiographic studies were performed with commercially available echocardiography systems equipped with a 2.5-MHz multi frequency phased array transducer (Vivid 5, GE-Vingmed, Morton, Norway). Routine digital grayscale 2-D was obtained, including mid-LV short axis views at the level of the papillary muscle and standard apical views (4-chamber, 2-chamber, and long axis). Sector width was optimized to allow for complete myocardial visualization while maximizing the frame rate. LV end-diastolic volume, end-systolic volume (ESV), and ejection fraction were obtained with the modified biplane Simpson's method from the apical 2- and 4-chamber images using the biplane Simpson's technique. Right ventricular size and function were qualitatively graded in the apical four-chamber and subcostal views. Enlargement of the RV was considered mild if the RV was greater than two-thirds of the LV but less than the LV size; moderate if the RV equaled the LV; and severe if the RV was greater than the LV.10 Right ventricular systolic function was estimated by the attending echocardiographer as normal or reduced, using the following criteria as a sign of RV dysfunction: (a) any RV wall motion abnormalities; (b) descent of base 2.0 cm.11 Right atrial pressure was estimated by visualizing the inferior vena cava (IVC) and its response to respiration. Right atrial pressure was estimated as 5 mm Hg if the IVC was 2.0 cm in diameter at the junction of the right atrium, 15 mm Hg if the IVC was dilated and collapsed with respiration, and 20 mm Hg if the IVC was dilated and did not collapse with respiration. Estimated PASP was calculated as the sum of tricuspid jet gradient and estimated right atrial pressure.12 Tricuspid regurgitation was graded qualitatively using Framingham Heart Study criteria: mild if the regurgitant jet area/right atrial area was <20%; moderate if 20–40%; or severe if >40%.13 Vegetation was defined as a, fixed or oscillating mass adherent to a leaflet or other cardiac structure with a distinct echogenic structure and independent motion.14 The lesion had to be visible in multiple views and detectable during the complete cycle. The measurements of vegetations were obtained in various planes, and the maximal length was used. In the presence of multiple vegetations, the largest value was used for analysis.
4. Statistical analysis
The collected data was revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (SPSS 15.0.1 for windows; SPSS Inc, Chicago, IL, 2001). Data was presented and suitable analysis was done according to the type of data obtained for each parameter. Parametric numerical data were expressed as Mean and Standard deviation (±SD), while non-numerical data were expressed as Frequency and Percentage.
5. Results
5.1. The prevalence of TVIE and basic demographic characters (Table 1)
Table 1.
Prevalence of TV endocarditis and demographic data.
| Variable | N | % |
|---|---|---|
| TVIE | 51 | 0.6 (of all) and 17.7 (of IE) |
| IE | 287 | 3.4 |
| All patients | 8376 | |
| Mean ± SD |
Range |
|
| Age (years) | 31.1 ± 7.8 | 17.0–55.0 |
| Categories (years) | N | % |
| 17–20.0 | 2 | 3.9 |
| 20.0–30.0 | 17 | 33.3 |
| 30.0–40.0 | 26 | 51.0 |
| 40.0–50.5 | 4 | 7.8 |
| 50.0–55.0 | 2 | 3.9 |
| Sex | N | % |
| Male | 46 | 90.2 |
| Female | 5 | 9.8 |
Patients with TV IE were 51 patients that constitute 0.6% of all patients and 17.7% of patients with infective endocarditis. Patients with IE were 287, which constitute 3.4% of all patients. The total number of patients underwent echocardiography during the study period were 8376. The mean age of patients with TVIE was (31.1 ± 7.8) years. Patients between 17 and 20 years were 2 (3.9%), patients between 20 and 30 years were 17 (33.3%), patients between 30 and 40 years were 26 (51%), patients between 40 and 50 years were 4 (7.8%), and patients between 50 and 55 years were 2 (3.9%). Males were 46 (90.2%), and females were 5 (9.8%).
5.2. Echocardiographic measurements and cardiac chambers dilatation (Table 2)
Table 2.
Cardiac measurements and chamber enlargement.
| Variable | Mean ± SD | Range |
|---|---|---|
| LVEDD (cm) | 4.9 ± 0.6 | 3.6–6.3 |
| LVESD (cm) | 3.8 ± 3.8 | 2.2–30.0 |
| IVSD (cm) | 0.8 ± 0.2 | 0.6–1.3 |
| IVSS (cm) | 1.2 ± 0.2 | 0.8–1.6 |
| EF% | 61.7 ± 8.6 | 25.0–77.0 |
| RVSP (mmHg) | 44.6 ± 16.0 | 19.0–85.0 |
| Chamber | N | % |
| Left atrium | 4 | 7.8 |
| Right atrium | 16 | 31.4 |
| Left ventricle | 2 | 3.9 |
| Righ ventricle | 15 | 29.4 |
The mean LVEDD (cm) was 4.9 ± 0.6, the mean LVESD (cm) was 3.8 ± 3.8, the mean IVSD (cm) was 0.8 ± 0.2, IVSS (cm) was 1.2 ± 0.2, the mean EF% was 61.7 ± 8.6, and the mean RVSP (mmHg) was 44.6 ± 16.0. Patients with right atrial dilatation were 16 (31.4%), patients with right ventricular dilatation were 15 (29.4%), patients with left atrial dilatation were 4 (7.8%), and those with left ventricular dilatation were 2 (3.9%).
5.3. Degree of tricuspid incompetence among the studied cases (Fig. 1)
Fig. 1.
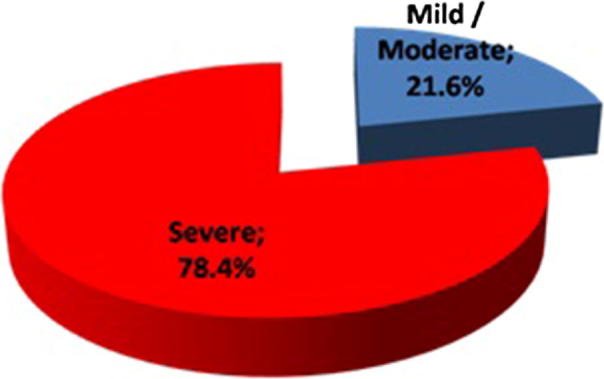
Degree of tricuspid incompetence among the studied cases.
It was found that tricuspid incompetence was presented in all our patients with TVIE. Mild to moderate tricuspid incompetence was presented in 11 patients (21.6%) and severe tricuspid incompetence was presented in 40 patients (78.4%).
5.4. Number of vegetations and vegetation mobility among the studied cases (Table 3)
Table 3.
Number of vegetations and vegetation mobility.
| Vegetation | N | % |
|---|---|---|
| Absent | 2 (presented with TV abscess) | 3.9 |
| Present | 49 | 96.1 |
| One vegetation | 33 | 64.7 |
| Two vegetations | 9 | 17.6 |
| Three vegetations | 7 | 13.7 |
| Mobile | 38 | 74.5 |
| Fixed | 13 | 25.5 |
Total TVIE patients = 51.
Tricuspid vegetations were absent in 2 patients (3.9%) and presented in 49 patients (96.1%). single vegetation was present in 33 patients (64.7%), two vegetations in 9 patients (17.6), and three in 7 patients (13.7%). Mobile tricuspid valve vegetations were found in 38 patients (74.5%) and fixed vegetations were found in 13 patients (25.5%).
5.5. Vegetation site and size among the studied cases (Table 4)
Table 4.
Vegetations site and size.
| Site | N | % |
|---|---|---|
| Anterior | 38 | 74.5 |
| Posterior | 16 | 31.4 |
| Septal | 14 | 27.5 |
| Prothetic | 3 | 5.9 |
| Native | 46 | 94.1 |
| Size | N | % |
| Small (<1.5 cm) | 9 | 17.6 |
| Large (>1.5 cm) | 40 | 78.4 |
| Not found | 2 | 3.9 |
Total TVIE patients = 51.
The most common site for tricuspid valve vegetations was the anterior leaflet of tricuspid valve where it was found in 38 patients (74.5%), then the posterior leaflet of tricuspid valve in 16 patients (31.4%), and finally the septal leaflet of tricuspid valve where it was found in 14 patients (27.5%), prosthetic valve vegetations was presented in 3 patients (5.9%). Vegetations were small (<1.5 cm2) in 9 patients (21.6%), and large (>1.5 cm2) in 40 patients (78.4%).
5.6. Other valve lesions and vegetations among the studied cases (Table 5)
Table 5.
Other valve lesions and other valve vegetations among the studied cases.
| Valve lesion | N | % |
|---|---|---|
| Pulmonary | 7 | 13.7 |
| Aortic | 4 | 7.8 |
| Mitral | 16 | 31.4 |
| Valve vegetation | N | % |
| Pulmonary | 0 | 0.0 |
| Aortic | 4 | 7.8 |
| Mitral | 7 | 13.7 |
| Concomitant mitral and aortic | 8 | 15.7 |
Total TVIE patients = 51.
Associated pulmonary valve lesion was found in 7 patients (13.7%). associated aortic valve lesion was found in 4 patients (7.8%) while associated mitral valve lesion was found in 7 patients (31.4%). Concomitant aortic valve vegetations were found in 4 patients (7.8%) and concomitant mitral valve vegetations were found in 7 patients (13.7%).
5.7. Cardiac complications among the studied cases (Fig. 2)
Fig. 2.
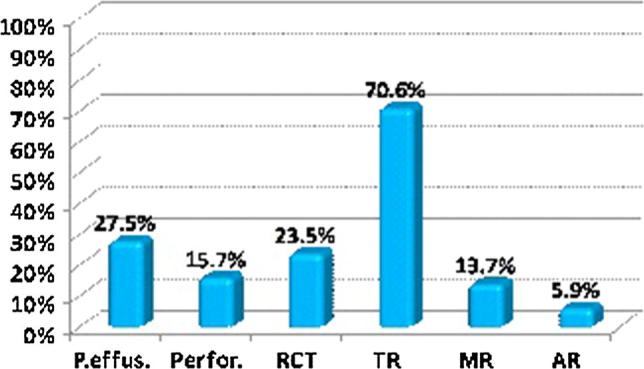
Cardiac complications among the studied cases. *P.effus. = Pericardial effusion. *RCT = Rupture chordae tendinae.
The most encountered complication in patients with TVIE was severe TR which was presented in 40 patients (78.4%), then Pericardial effusion in 14 patients (27.5%), Perforation of cusps in 18 patients (15.7%), Rupture chordae tendineae (RCT) in 12 patients (23.5%), MR in 7 patients (13.7%), and AR in 3 patients (5.9%).
6. Discussion
Isolated native non-rheumatic TVE is rarely diagnosed in the absence of intravenous drug use, intracardiac catheters or cardiac anomalies. The incidence of TVIE in developed countries varies from 5% in some studies up to 15% in others of all cases of IE.15 The rarity of tricuspid valve endocarditis (TVE) as compared to left sided endocarditis are attributed to infrequent occurrence of right-sided congenital and rheumatic heart diseases as well as the low pressure, and low oxygen saturation in the right side, which protects the tricuspid and pulmonary valves from being subjected to being excessively strained.16 The main finding of our study was that the prevalence of TVIE is about (17.7%) of all cases of IE, and is about (0.6%) of all cases attending the echo lab of Ain shams hospitals during the study period. The incidence of TVIE in a similar study of infective endocarditis done in Alexandria main university hospitals for one year, and was about 32% of all cases of IE (16 of 50 patients).17 but in a previous study extended for 3 years, done in the Cairo University cardiology department by Al-Mogheer et al., the incidence of TVIE was about 9.7% of all IE cases (15 of 155 patients).18 Multiple factors could have led to variability in this TVIE incidence, including referral and case ascertainment biases, disease misclassification, differences in populations at risk, study designs, and use of different case definitions.19
The mean age group in our study was (31.1 ± 7.8) and about 84.3% of patients age was between (20–40) these results are very close to the results in Kaser-Elaini study by Al-Mogheer et al. in which the mean age was (32 ± 13 years),18 and the study in Alexandria main university hospitals by Mohamed Sadaka et al. where the mean age group was (33.42 ± 11.37).17 Majority of the researchers from developing countries report a similar age group affected, including Tariq M et al., who found that the overall median age of his patients with IE was 24 years20 and Koegelenberg et al., who found that Patients with definite endocarditis in his study had a mean age of 37.7 years.21
Also the present study showed a higher incidence of IE in males (90.2%) than in females (9.8%) with a ratio of 9:1. This very big variation in ratio may be explained by the specific nature of TVIE which occurs predominantly in IVDAs, which is a problem related mainly to male gender in our society, as most females are grown up in a conservative way in accordance with our religious and culture in our society. Miró JM et al. estimated that the incidence of IE in IVDAs to be about 2–5% per year and is documented that it is responsible for 5% to 10% of the overall death rate.8 Baddour et al. documented that The majority of TVIE were young, between 20 and 40 years of age, and predominantly men (male:female ratio, 4 to 6:1.22 His results are concordant with our results here.
Echocardiography plays an important role in diagnosis of TVIE, Habib et al. documented that the two most important diagnostic features of TVE in patients with IVDA are echocardiographic evidence of vegetation, and the presence of septic embolic phenomena.23 The key echocardiographic finding in tricuspid valve endocarditis is that of vegetation(s).24 Nabeel Buhari et al. strongly emphasized the importance of blood cultures and echo-cardiography in postpartum patients with persistent fever and in those patients with multiple IV lines and intravenous injections who continue to have persistent fever despite ruling out all the usual causes of fever.25
In this study vegetation was present in 49 patients that constitute about 96.1% of patients. Vegetation was absent in two patients, but their echocardiographic reports documented them as TV IE cases; this may be due to embolization of vegetation or very small vegetation. The vegetation were detected more commonly in one leaflet in 33 patients (64.7%) and the anterior leaflet that was the most commonly affected in 38 patients constituting about 74.5% of patients. Moss R et al., found that the anterior leaflet, the largest one is the most frequent site for vegetations to attach, finding similar to our findings her.24 The size of vegetations in this study was large >15 mm in 40 patients (78.4%). This mean that tricuspid vegetations tends to be mainly large, finding similar to Moss R et al., study that reveal that Tricuspid vegetations are usually large due to the low pressure in right heart chambers, allowing them to grow and may be in excess of 2 cm.24 Our finding is also consistent with Panduranga P et al. He reported that Tricuspid vegetations are often large and may be in excess of 2 cm.26 Increasing vegetation size is major indications for surgery as reported by Habib G et al., Mohamed Sadaka et al. and Al-Mogheer et al.17, 18, 23 The size of vegetation is also an important indicator for mortality and In one study the main predictors of death in right-sided IE in IVDAs are vegetation size (>20 mm) and fungal etiology.27 Also we found that the majority of vegetations were mobile (38 patients 74.5%) this may explain the high rate of embolizations in TVIE. Robbins et al. also documented that Septic pulmonary embolism in patients with TVE occur in 75% to 100% of patients.27 Native TVIE was present in 46 patients (94.1%), and tricuspid prosthetic valve affection was in 3 patients (5.9%), this percentage of prosthetic valve affection is less that was reported by Mohamed Sadaka et al.17 where it was about 22%. However, this difference can be explained by the fact that prosthesis is much frequent in mitral and aortic valves than tricuspid valve, and his study included right and left sided endocarditis.
Right ventricular dilatation was present in 15 patients (29.4%). Lewis JF et al. documented that right ventricular dilatation and enlargement is associated with increased mortality.28
Concomitant aortic valve vegetations was present in 4 patients (7.8%) and Concomitant mitral valve vegetations was present in 7 patients (13.7%), these results are much higher than the results of Mohamed Sadaka et al.,17 where Concomitant aortic and tricuspid valves vegetation were (4%) and Concomitant mitral and tricuspid valves vegetation were presented in (2%) of his patients. Also vegetations were present in both aortic and mitral valve in 8 patients (15.7%). The later result is similar to Al-Mogheer et al.,18 where concurrent mitral and aortic vegetations was about (15.5%) of his patients.
Complications of the TVIE are much less common than left sided endocarditis. In this study the most encountered echocardiographic complication is severe TR which was in 40 patients (78.4%). It was reported that all our patients were complaining of TR ranging from mild TR to severe regurgitations. Lewis JF et al. had documented that moderate to severe TR have worse survival than patients with mild or less TR, regardless of pulmonary artery pressure and LVEF.28 The reason for higher mortality with significant TR remains to be determined. It is possible that TR is a more sensitive marker of RV dysfunction than is visual interpretation of systolic performance. Also, the presence of TR may mask the decreased contractility of the RV, analogous to the effect of mitral regurgitation on the ability to estimate LV contractility from LVEF. Severe TR is a leading cause of right sided heart failure and associated with poor prognosis. Based on these findings, significant (moderate or greater) TR should be considered an additional risk factor for mortality. Nath J et al. proved that increasing TR severity is associated with worse survival in men regardless of LVEF or pulmonary artery pressure.29
Perforations of cusps in 8 patients (15.7), AR in 3 patients (5.9%), MR in 7 patients (13.7%) and Paravalvar abscess in 2 patients (3.9%), this results is discordant with Mohamed Sadaka et al.,17 where abscess was recorded in 18% of the patients.
7. Conclusion and recommendations
The incidence of TV IE is increasing with male gender predominance, and affects mainly young age groups. TV IE represented 0.6% of all patients, and 17.7% of IE cases. The main echocardiographic feature of TV IE is vegetations which were characterized by being large, highly mobile, and affecting mainly anterior TV leaflet. The main echocardiographic complication is severe TR, but abscess formation was infrequent. A multi-center prospective study is warranted.
8. Limitations
It was a single center study with relatively small number of patients as well as it was retrospective lacking the follow up data.
Conflicts of interest
The authors have no conflicts of interest.
Funds
None.
Footnotes
Peer review under responsibility of Egyptian Society of Cardiology.
References
- 1.Osler W. The Gulstonian lectures, on malignant endocarditis. Br Med J. 1885;1:467–470. doi: 10.1136/bmj.1.1262.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bayer A.S., Bolger A.F., Taubert K.A. Diagnosis and management of infective endocarditis and its complications. Circulat – J Am Heart Assoc. 1998:2936–2948. doi: 10.1161/01.cir.98.25.2936. [DOI] [PubMed] [Google Scholar]
- 3.Mullany C.J., Chua Y.L., Schaff H.V. Early and late survival after surgical treatment of culture-positive active endocarditis. Mayo Clin Proc. 1995;70:517–525. doi: 10.4065/70.6.517. [DOI] [PubMed] [Google Scholar]
- 4.Aref A. Bin Abdulhak, Larry M. Baddoury, et al., 2012. Global and Regional Burden of Infective Endocarditis, 1990:2010 GLOBAL HEART, Vol. 9, pp. 131–143. [DOI] [PubMed]
- 5.Hasbun R., Vikram H.R., Barakat L.A. Complicatedleft-sided native valve endocarditis in adults: risk classification for mortality. J Am Med Assoc. 2003;289:1933–1940. doi: 10.1001/jama.289.15.1933. [DOI] [PubMed] [Google Scholar]
- 6.Tornos P., Iung B., Baron G. Infective endocarditis in Europe: lessons from the Euro heart survey. Heart. 2005;91:571–575. doi: 10.1136/hrt.2003.032128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Heydari A.A., Safari H. Isolated tricuspid valve endocarditis. Int J Infect Dis. 2009;13:e109–e111. doi: 10.1016/j.ijid.2008.07.018. [DOI] [PubMed] [Google Scholar]
- 8.Miro J.M., del Rio A. Infective endocarditis inintravenous drug abusers and HIV-1 infected patients. Infect Dis Clin North Am. 2002;16:273–295. doi: 10.1016/s0891-5520(01)00008-3. [DOI] [PubMed] [Google Scholar]
- 9.Cabell C.H., Heidenreich P.A., Chu V.H., Moore C.M. Increasing rates of cardiac device infections among Medicarebeneficiaries: 1990–1999. Am Heart J. 2004;147:582–586. doi: 10.1016/j.ahj.2003.06.005. [DOI] [PubMed] [Google Scholar]
- 10.Haddad François, Hunt Sharon A., Rosenthal David N. Right ventricular function in cardiovascular disease, Part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117:1436–1448. doi: 10.1161/CIRCULATIONAHA.107.653576. [DOI] [PubMed] [Google Scholar]
- 11.Per L., Avin C., Michael H. Echocardiography in the assessment of right heart function. Eur J Echocardiogr. 2008;9:225–234. doi: 10.1016/j.euje.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 12.Yock P.G., Popp R.L. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation. 1984;70:657–662. doi: 10.1161/01.cir.70.4.657. [DOI] [PubMed] [Google Scholar]
- 13.Singh J.P., Evans J.C., Levy D. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study) Am J Cardiol. 1999;83:897–902. doi: 10.1016/s0002-9149(98)01064-9. [DOI] [PubMed] [Google Scholar]
- 14.Habib G., Badano Luigi, Tribouilloy Christophe. Recommendations for the practice of echocardiography in infective endocarditis. Eur J. 2010;2010:202–219. doi: 10.1093/ejechocard/jeq004. [DOI] [PubMed] [Google Scholar]
- 15.Ruotsalainen E., Sammalkorpi K. Clinical manifestations and outcome in Staphylococcus aureus endocarditis among injection drug users and nonaddicts: a prospective study of 74 patients. BMC Infect Dis. 2006;6:137. doi: 10.1186/1471-2334-6-137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Morokuma H., Minato N., Kamohara K. Three surgical cases of isolated tricuspid valve infective endocarditis. Ann Thoracic Car-diovascular Surg. 2010;16:134–138. [PubMed] [Google Scholar]
- 17.Sadaka Mohamed, ElSharkawy Eman, Soliman Manal. Study of infective endocarditis in Alexandria main university hospitals. Egyptian Heart J. 2013;2013:307–317. [Google Scholar]
- 18.Al-Mogheer B., Waleed A., Sameh B. Predictors of inhospital mortality in patients with infective endocarditis. Egyptian Heart J. 2013;65:159–162. [Google Scholar]
- 19.Tleyjeh I.M., Abdel-Latif A., Rahbi H. A systematic review of population-based studies of infective endocarditis. Chest. 2007;132:1025–1035. doi: 10.1378/chest.06-2048. [DOI] [PubMed] [Google Scholar]
- 20.Tariq M., Alam M., Munir G. Infective endocarditis a five year experience at a tertiary care hospital in Pakistan. Int J Infect Dis. 2004;2004:163–170. doi: 10.1016/j.ijid.2004.02.001. [DOI] [PubMed] [Google Scholar]
- 21.Koegelenbergl C.F., Doubell A.F. Infective endocarditis in the Western Cape Province of South Africa: a three-year prospective study. Q J Med. 2003;96:217–225. doi: 10.1093/qjmed/hcg028. [DOI] [PubMed] [Google Scholar]
- 22.Baddour L.M., Wilson W.R., Bayer A.S. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications. Circulation. 2005;111:3167–3184. doi: 10.1161/CIRCULATIONAHA.105.165564. [DOI] [PubMed] [Google Scholar]
- 23.Habib G., Hoen B., Tornos P., Thuny F. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC. Eur Heart J. 2009;30:2369–2413. doi: 10.1093/eurheartj/ehp285. [DOI] [PubMed] [Google Scholar]
- 24.Moss R., Munt B. Injection drug use and right sided endocarditis. Heart. 2003;89:577–581. doi: 10.1136/heart.89.5.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Buhari Nabeel., Balasubramanian A., Ravi Cherian M. Tricuspid valve endocarditis: not just in IV drug abusers. Int J Med Sci Public Health. 2013;2013:468–471. [Google Scholar]
- 26.Panduranga P., Al-Mukhaini Mohammed., Sulaiman Kadhim. Tricuspid valve endocarditis in an intravenous drug abuser masquerading as pulmonary tuberculosis. Heart Views. 2010;2010:121–124. doi: 10.4103/1995-705X.76805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Robbins J.M., Frater M.W.R. Influence of vegetation size on clinical outcome of right-sided infective endocarditis. AM J Med. 1986;80:165. doi: 10.1016/0002-9343(86)90004-5. [DOI] [PubMed] [Google Scholar]
- 28.Lewis J.F., Webber J.D. Discordance in degree of right and left ventricular dilation in patients with dilated cardiomyopathy: recognition and clinical implications. J Am Coll Cardiol. 1993;21:649–654. doi: 10.1016/0735-1097(93)90097-k. [DOI] [PubMed] [Google Scholar]
- 29.Nath J., Foster E., Heidenreich P.A. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004;43:405–409. doi: 10.1016/j.jacc.2003.09.036. [DOI] [PubMed] [Google Scholar]