

Abstract
Mandibular fracture in younger children is the most common facial fracture among all the facial fracture in the sequence of condyles followed by symphysis/parasymphysis and body of the mandible. Symphysis/Parasymphysis fracture of mandible can be minimally displaced or severely displaced depending upon the severity of the injury. This case report highlights the simple, reliable method of minimally displaced fracture i.e. modified closed cap splint for stability of the fracture segments in pediatric patients.
Keywords: Symphysis fracture, Cap splint, Modified splint, Facial fracture, Parasymphysis
1. Introduction
Mandibular fracture is the most common fracture among the facial fractures. Maxillofacial injuries are less common in children than adults. The incidence of maxillofacial trauma is 3.3% in children age 15 years or younger. In pediatric patients mandibular fracture accounts for the 36% among all the facial fractures. Condylar fracture followed by the symphysis/parasymphysis fractures are the most common type of fractures in the children (Boffano, 2015). Fall from height/stairs, road traffic accidents, child abuse, assault etc. are the major causes of mandibular fracture in pediatric patients (Singh et al., 2014). The management of mandibular fracture differs in children when compared to adults because of the presence of the permanent tooth buds in the mandible. Open reduction with rigid fixation is not commonly used in pediatric cases. Fracture of the mandible may be associated with or without loss of both hard and soft tissues depending on the severity of the injury. The goal of the treatment of these fractures is restore the bone architecture in a stable position as less invasively as possible to restore the function and esthetic impairment (Baby et al., 2010).
2. Case 1
A 4 year old boy reported to the unit of Pedodontics and Preventive Dentistry with the chief complaint of pain and asymmetry of face. Patient had a history of fall from the height 1 week back. There was no history of loss of consciousness or vomiting. Patient went to local hospital but no intervention was done. Intraoral examination revealed asymmetry of the mandibular arch (Fig. 1). Step deformity with tenderness along the lower border of mandible on right side of canine region was observed. Preoperative OPG shows right mandibular parasymphysis fracture with step along the inferior border of the mandible (Fig. 2). A diagnosis of mandibular parasymphysis region was made. The primary impressions were taken with alginate and two sets of casts were subsequently poured. A modified closed acrylic cap splint was fabricated with one anterior and two posterior opening (Fig. 3). Displaced Fractured fragments were reduced under local anaesthesia and modified cap splint was cemented to the reduced fractured jaw with help of luting GIC (GC Fuji I) (Fig. 4). Oral hygiene instructions were given to the patient and analgesics were prescribed. After 6 weeks the splint was removed and the patient was asymptomatic (Fig. 5). An OPG revealed healing of the fracture site after 6 months of follow up (Fig. 6).
Fig. 1.

Intraoral photograph showing space between 82 and 83 region.
Fig. 2.

Preoperative OPG showing right mandibular parasymphysis fracture.
Fig. 3.

Fabrication of Modified closed cap splint for reduction of Parasymphysis fracture.
Fig. 4.

Modified closed cap splint cemented with luting GIC.
Fig. 5.

Reduction of mandibular right parasymphysis fracture and after 6 months follow up.
Fig. 6.

OPG showing reduction of parasymphysis fracture and 6 months follow-up.
3. Case 2
A 4 year old boy reported to the unit of Pedodontics and Preventive Dentistry with the chief complaint of pain in the right mandibular region while chewing food. Patient had a history of road traffic accident (collision with motorcycle) 1 week back. Intraoral examination revealed asymmetry of the arch and gap in the 82 and 83 region (Fig. 7). The primary teeth were carious. Preoperative CT scan showed right mandibular parasymphysis fracture along the inferior border of the mandible (Fig. 8). A diagnosis of mandibular right parasymphysis region was made. A modified closed acrylic cap splint was fabricated with one anterior and two posterior opening (Fig. 9). Fractured fragments were reduced and modified closed cap splint was cemented with help of luting GIC (GC Fuji I). The primary teeth were restored with GIC and stainless steel crowns. Oral hygiene instructions were given to the patient and analgesics were prescribed to the patient. After 6 weeks the splint was removed and the patient was asymptomatic. An OPG revealed healing of the fracture site after 8 months of follow up (Fig. 10).
Fig. 7.

Intraoral photograph showing gap between 82 and 83 region.
Fig. 8.
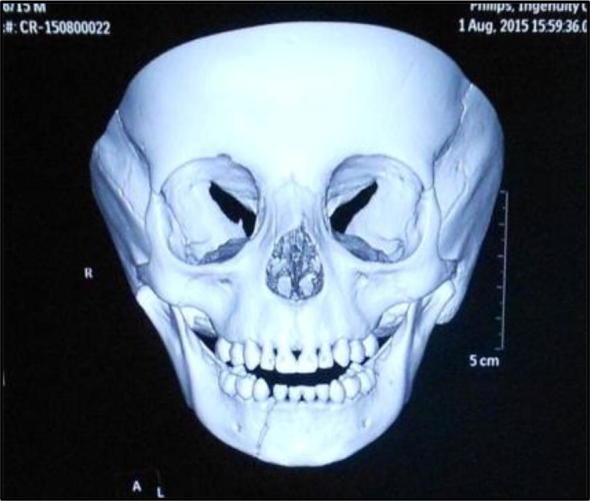
CT Scan revealed fracture line between 82 and 83 region.
Fig. 9.

Modified closed cap splint cemented with Luting GIC.
Fig. 10.

OPG after 8 month of follow up showing complete healing.
4. Discussion
Facial fractures in the pediatric age group generally account for about 5% of all facial fractures (Aizenbud et al., 2009). The most common causes of facial injuries are fall from height, road traffic accident, sports injuries, etc. Pediatric patients presents a unique challenge to oral surgeons because of anatomic variation and changes in the mandibular growth. The management of pediatric mandibular fractures also depends upon the patient cooperation during the treatment. Healing period is also faster in children aided by the well vascularized tissue and blood supply of the face (Kaban, 1990, Mohan et al., 2012). Therefore, the treatment required in pediatric patients depends on the patient’s age, patient cooperation and stage of tooth development. Haug and Foss classified the mandibular fracture into condylar, alveolus, body, symphysis, parasymphysis, angle, ramus, and coronoid (Haug and Foss, 2000). Interdental wiring is difficult to achieve in pediatric patients because of insufficient number of teeth/root resorption of the teeth and presence of the permanent tooth buds, etc.
There are various techniques which were utilized in management of pediatric fractures like Tape Muzzles, Circumferential wiring, acrylic Splint, percutaneous skeletal fixation, open reduction, resorbable plates, orthodontic resin, modified orthodontic brackets, rubber elastics in combination with orthodontics brackets, nickel titanium staples depending upon the minimally/severely displaced fractures (Madan and Bajaj, 2010).
In severely displaced fracture, intermaxillary fixation, cap splints, mini plates or resorbable plates can be used. Miniplates should be cautiously used to prevent injuries to the permanent tooth buds and require second surgery for removal in growing patients. A resorbable plate eliminates the need for the second surgical procedure but the risk of damage to tooth buds does exist (Eppley, 2005). Minimally displaced fractures can be treated conservatively by means of soft diet, analgesic and antibiotic prophylaxis. However, healing might be delayed because of insufficient cooperation of the young patients in following postoperative instructions. To overcome this, a modified closed cap splint can be fabricated and cemented with luting cement to maintain the stability. In both the present cases, modified closed cap splint was fabricated and cemented with GIC luting cement.
Modified Closed cap splint is a simple, easy to fabricate and more reliable method than circum-mandibular wiring with cap splint, open reduction or intermaxillary fixation. It has other advantages like ease of application and removal, less time consumption, cost-effectiveness, good stability during healing period and minimal trauma to surrounding tissues. Therefore, the modified closed cap splint should be a reliable method in minimally displaced mandibular fractures in pediatric patients.
Most of the pediatric fractures are greenstick type of fractures, so conservative approach is preferred compared to more invasive ones. During the early years of age, growth of the mandible and development of dentition are the main concerns while treating mandibular fractures. Majority of mandibular body and parasymphysis fracture in pediatric are undisplaced because of elasticity of bone and tooth buds. Exact method employed for immobilization depends upon child’s age and stage of dental development. Under two years of age, no anchorage can be taken from teeth as they are unerupted.
5. Conclusion
Mandibular fractures in children most commonly occur in the condylar region followed by parasymphysis and angle region. Minimally displaced fractures can be managed conservatively by the modified closed cap splint compared to the severely displaced fracture which may require open reduction and rigid internal fixation. In pediatric patients cap splint can be recommended in mandibular symphysis/ parasymphysis fractures.
Conflict of interest
The authors declared that there is no conflict of interest.
Footnotes
Peer review under responsibility of King Saud University.
References
- Aizenbud D., Hazan-Molina H., Emodi O., Rachmiel A. The management of mandibular body fractures in young children. Dental Traumatol. 2009;25:565–570. doi: 10.1111/j.1600-9657.2009.00815.x. [DOI] [PubMed] [Google Scholar]
- Baby J., Reena J.R., Stalin A., Indumathi E. Management of mandibular body fracture in pediatric patients: a case report with review of literature. Contemp. Clin. Dent. 2010;3(4):291–296. doi: 10.4103/0976-237X.76406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boffano P. European Maxillofacial Trauma (EURMAT) in children: A multicenter and prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015;119(5):499–504. doi: 10.1016/j.oooo.2014.12.012. [DOI] [PubMed] [Google Scholar]
- Eppley B.L. Use of resorbable plates and screws in Pediatric Facial Fractures. J. Oral Maxillofac. Surg. 2005;63(3):385–391. doi: 10.1016/j.joms.2004.11.011. [DOI] [PubMed] [Google Scholar]
- Haug R.H., Foss J. Maxillofacial injuries in the pediatric patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000;90(2):126–134. doi: 10.1067/moe.2000.107974. [DOI] [PubMed] [Google Scholar]
- Kaban L.B. W.B. Saunders; Philadelphia: 1990. Facial Trauma I: Pediatric Oral and Maxillofacial Surgery; pp. 209–232. [Google Scholar]
- Madan N., Bajaj N. Conservative treatment of pediatric mandibular fracture with removable acrylic splint. Indian J. Dent. Sci. 2010;2(4):22–24. [Google Scholar]
- Mohan M.C., Bhat S., Karaikal A., Gupta N. Reinforced open cap splint: a novel therapeutic technique in paediatric mandibular fracture. Heal Talk. 2012;5(1):32–33. [Google Scholar]
- Singh A.K., Sharma N.K., Verma V., Pandey A. Open Cap Splint Fixation with Circum-mandibular wiring still best method in Management of Pediatric Mandibular Fracture. J. Dentofacial. Sci. 2014;3(4):55–58. [Google Scholar]