

Abstract
Rationale:
As more and more women delay their child bearing age, the prevalence of uterine fibroids during pregnancy is likely to increase.
Patient Concerns & Lessons:
We report a Chinese Tibetan case with spontaneous expulsion of a huge cervical myoma after cesarean. Decreased blood supply of the myoma and the uterine contraction may contribute to the spontaneous expulsion. Vaginal-myomectomy is recommended as the initial treatment.
Keywords: expulsion, myoma, postpartum, pregnancy
1. Introduction
Uterine leiomyoma is the most common benign tumor of the female reproductive system. According to previous reports, the prevalence of uterine leiomyoma among pregnant women ranges from <1% to 10.7%.[1,2] As more and more women delay their child bearing age, the prevalence is likely to increase. It has been reported that uterine leiomyoma may cause malpresentation, puerperal infection, operative vaginal delivery, cesarean delivery, and postpartum hemorrhage, etc.[1,3] Here we report a Chinese puerpera with a spontaneous expulsion of a huge cervical leiomyoma in her postpartum period.
The report complies with the Declaration of Helsinki and it was approved by the institutional ethical committee of Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital. We were given informed consent from the patient to use the medical history and images.
2. Case report
A 22-year-old Chinese Tibetan primipara came to the emergency room with a complaint of fever (up to 39.2 °C), and a mass extrusion in the vaginal orifice with smelly discharge for 2 days. She had delivered a female baby by cesarean in the local hospital in her hometown 2 weeks before. Although she did not have a regular antenatal care there was nothing special about the gestational procedure. When she felt regular uterine contractions at about 9 months’ gestation, she went to the local hospital. And the ultrasonic test showed a transverse lie of the fetus, so the doctor proposed her a cesarean. Her baby weighted 2850 g and was healthy. The postoperative course was uneventful and she was discharged 3 days after the cesarean. On postpartum day 12, she had a fever of 38 °C to 39.2 °C , and, she felt uncomfortable about the vagina. When she squatted, a big mass extruded from the vagina with a lot of foul-smelling discharge. Her doctor was not sure about the mass and referred her to our hospital.
At the time of admission, general physical examination was unremarkable except a temperature of 38.3 °C. She appeared calm without severe pain. Cardiopulmonary examination was nothing special. There was no abdominal tenderness, and the incision healed well. An irregular, long, thin, and broad sarcoid mass hung down through the vaginal orifice with foul-smelling serosanguinous discharge on the surface (Fig. 1). Speculum examination showed that the mass seemed to come from the internal uterine cavity. The cervix was dilated (Fig. 2A). The uterus was firm and tenderness on bimanual examination. The tips of the doctor's fingers in the vagina could not reach the root of the mass.
Figure 1.
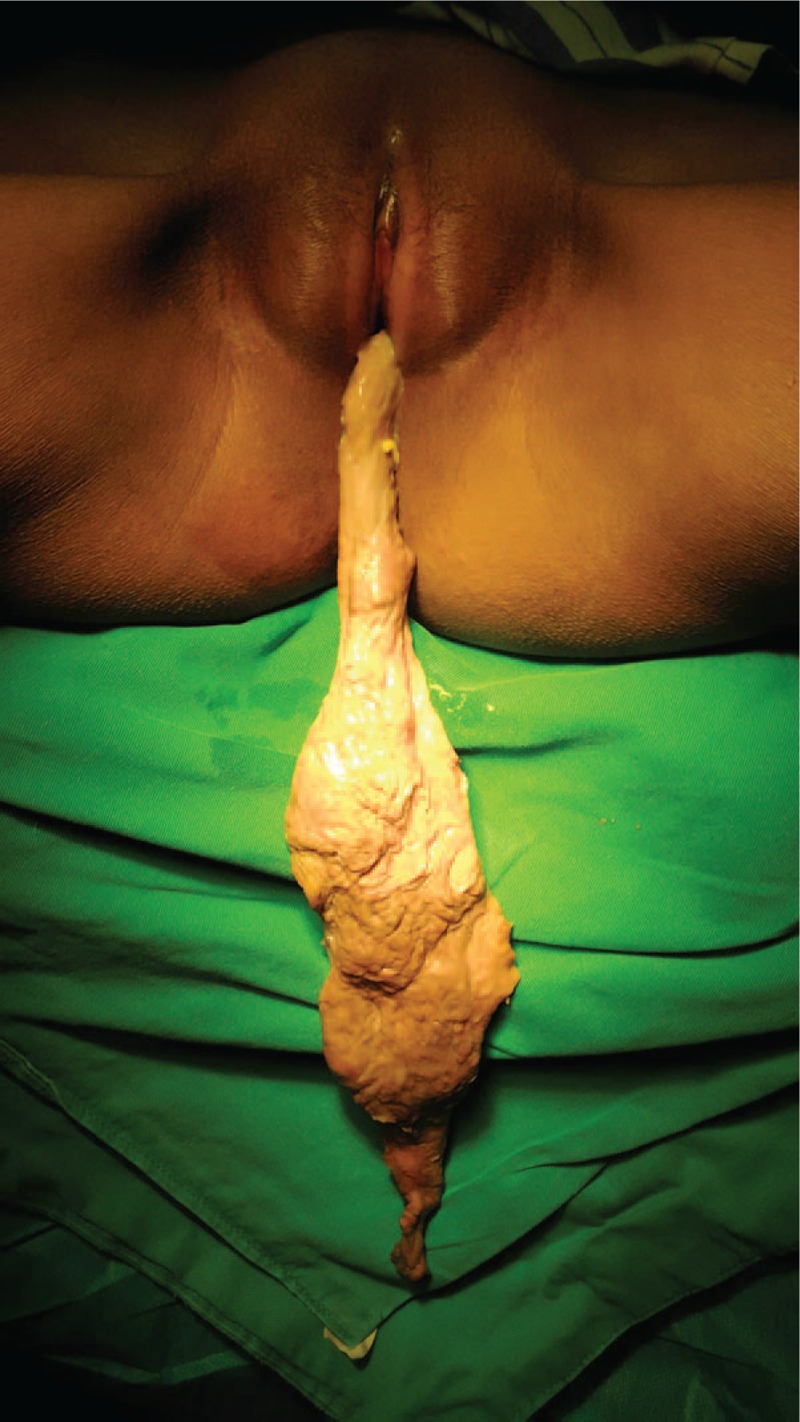
An irregular, long, thin, and broad sarcoid mass hung down through the vaginal orifice with foul-smelling serosanguinous discharge on the surface.
Figure 2.
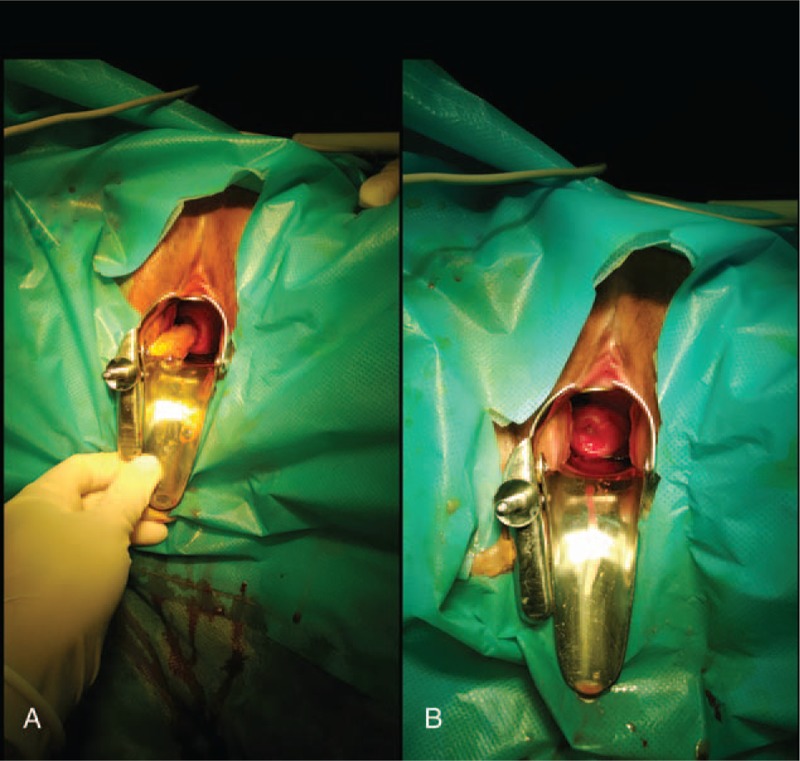
Speculum examination. (A) Before dissection. (B) After dissection.
The laboratory studies were uneventful with a slightly elevated white blood cell (WBC) of 9.52 × 109/L (normal 3.69–9.16 × 109/L). The ultrasound showed that the echo of the anterior uterine wall was heterogeneous. No occupation was detected in the uterine cavity.
The patient was first treated with broad-spectrum intravenous antibiotics. Then she was sent to the operation room. After anesthesia, we made bimanual examination again, and this time the doctor's finger tips could reach the root of the mass which grew up from the upper right side of the cervical canal, near the internal ostium. Then the mass was removed with blunt and sharp dissection. After the dissection, the cervix looked normal (Fig. 2B). The resected surface showed a pink, sarcoid, tenacious texture (Fig. 3). The pathology report confirmed a 38.0 × 6.0 (the widest) ×2 cm degenerating leiomyoma with infarction and no atypical features. The patient's postoperative course was uncomplicated and she was discharged home 3 days after the operation. As following-up, she had given birth to another baby 2 years after the operation with nothing special.
Figure 3.
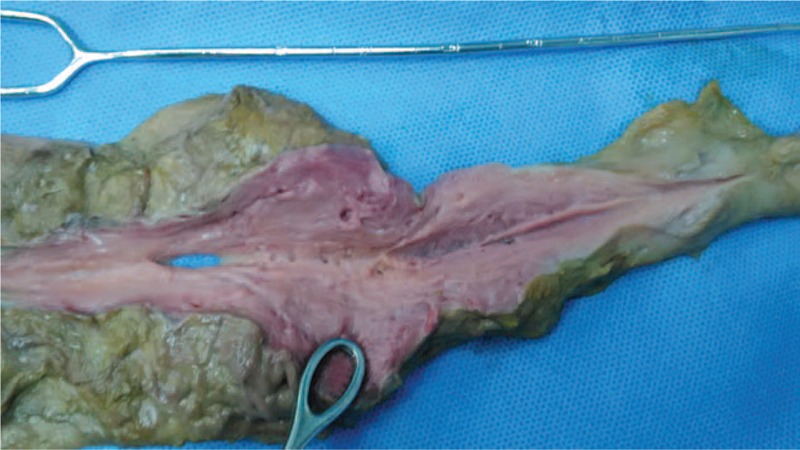
The resected mass.
3. Discussion
Recently, Zhao et al[4] reported that 2.68% of Chinese pregnant women were identified with at least 1 fibroid. And 64.7% of them were subserosal, 33.2% submucosal, and 2.1% intramural. In their research, all fibroids were identified during routine prenatal care, while all of the ultrasound data came from the second trimester (18–22 weeks).[4] The patient in our case was a Tibetan woman who lived in the remote and economically depressed mountainous area of China. The health care there was poor and the patient did not get either a preconception examination or antenatal care routinely. Fortunately, her gestational course was uneventful without vaginal bleeding, infection, or threatened preterm labor, etc. But the malpresentation of the fetus may be related with the cervical myoma as reported by others.[2,4,5]
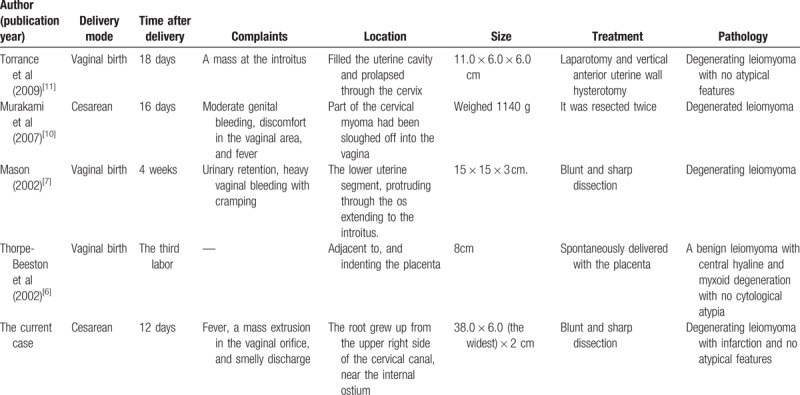
We summarized the cases with spontaneous expulsion of the submucosal or cervical myoma reported since the year 2000 (Table 1). Most of them were very big and located in the lower segment of the uterus or the cervix. The most common complaints included fever, vaginal bleeding, smelly discharge, and the feel of an extrusion through the vagina. Postpartum expulsion of submucosal myoma has invariably resulted from infarction, hyalinization, or necrosis histologically.[6–11] During pregnancy, red degeneration of the myoma could be induced when the growth rate outstripped its blood supply. After delivery, the blood flow of the uterus decreased dramatically which could also result in myoma degeneration. The uterine contraction and the softening of the cervix in puerperium might also cause spontaneous expulsion of the cervical myoma. However, it should be distinguished with placental residual, uterine inversion, placenta-site tumor, etc. If the patient had a high fever, pyomyoma should be seriously considered.[12] When the myoma was expelled into the vagina, blunt and sharp dissection through the vagina would usually work.[7] If the root of the myoma was too broad or if there was a severe bleeding during the dissection, laparotomy or laparoscopy could be considered.[11]
Table 1.
Summary of the cases with spontaneous expulsion of submucosal or cervical myoma after delivery since the year 2000, including the current case.
In conclusion, gestational myoma, especially submucosal or cervical myoma, may have an unusual appearance in puerperium period that may be misinterpreted. Some of them could be expelled spontaneously after delivery. Vaginal-myomectomy is recommended as the initial treatment of choice for prolapsed submucosal or cervical myoma.[10]
Acknowledgments
We are thankful to the patient for her consent to the report. In addition, we would like to extend special thanks to Lucas Green (medical student, Sichuan University, with his permission) for his help in revising the manuscript.
Author contributions
Conceptualization: Jian Zhang, Bingyu Zou.
Data curation: Jian Zhang.
Formal analysis: Jian Zhang.
Investigation: Jian Zhang.
Supervision: Jian Zhang, Bingyu Zou.
Writing – original draft: Jian Zhang, Kana Wang.
Writing – review & editing: Jian Zhang, Bingyu Zou, Kana Wang.
Footnotes
Abbreviation: WBC = white blood cell.
The authors have no conflicts of interest to disclose.
References
- [1].Coronado GD, Marshall LM, Schwartz SM. Complications in pregnancy, labor, and delivery with uterine leiomyomas: a population-based study. Obstet Gynecol 2000;95:764–9. [DOI] [PubMed] [Google Scholar]
- [2].Laughlin SK, Baird DD, Savitz DA, et al. Prevalence of uterine leiomyomas in the first trimester of pregnancy: an ultrasound-screening study. Obstet Gynecol 2009;113:630–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Vergani P, Locatelli A, Ghidini A, et al. Large uterine leiomyomata and risk of cesarean delivery. Obstet Gynecol 2007;109(2 pt 1):410–4. [DOI] [PubMed] [Google Scholar]
- [4].Zhao R, Wang X, Zou L, et al. Adverse obstetric outcomes in pregnant women with uterine fibroids in China: A multicenter survey involving 112,403 deliveries. PLoS One 2017;12:e187821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Oruc S, Karaer O, Kurtul O. Coexistence of a prolapsed, pedunculated cervical myoma and pregnancy complications: a case report. J Reprod Med 2004;49:575–7. [PubMed] [Google Scholar]
- [6].Thorpe-Beeston JG, Sebire NJ. Spontaneous expulsion of submucous fibroid after preterm labour. BJOG 2002;109:726–7. [DOI] [PubMed] [Google Scholar]
- [7].Mason TC. Red degeneration of a leiomyoma masquerading as retained products of conception. J Natl Med Assoc 2002;94:124–6. [PMC free article] [PubMed] [Google Scholar]
- [8].Honore LH, Reid DW. Uncomplicated, spontaneous expulsion of a uterine leiomyoma postpartum. A case report. J Reprod Med 1985;30:358–9. [PubMed] [Google Scholar]
- [9].Gainey HL, Keeler JE. Submucous myoma in term pregnancy. Am J Obstet Gynecol 1949;58:727–37. [DOI] [PubMed] [Google Scholar]
- [10].Murakami T, Niikura H, Shima Y, et al. Sloughing off of a cervical myoma after cesarean section: a case report. J Reprod Med 2007;52:962–4. [PubMed] [Google Scholar]
- [11].Torrance SM, Muhn N, Ellis S, et al. Role of dynamic MRI in surgical decision-making for a postpartum woman with a prolapsed degenerating uterine leiomyoma. J Obstet Gynaecol Can 2009;31:446–51. [DOI] [PubMed] [Google Scholar]
- [12].DeMaio A, Doyle M. Pyomyoma as a rare source of postpartum sepsis. Case Rep Obstet Gynecol 2015;2015:263518. [DOI] [PMC free article] [PubMed] [Google Scholar]