

Abstract
Ovarian fibroma/fibrothecoma with elevated serum OC125 antigen (CA125) is rarely encountered in clinical practice, and also easily misdiagnosed as epithelial ovarian carcinoma (EOC). The aim of this study was to investigate the clinicopathological features of ovarian fibroma/fibrothecoma with elevated serum CA125.
In total, 580 patients who underwent primary surgery and pathologically diagnosed as ovarian fibroma/fibrothecoma were retrospectively analyzed. The clinicopathological parameters were collected and compared between the patients with elevated serum CA125 (>35 U/mL) and without. The immunoreactivity for CA125 in ovarian fibroma/fibrothecoma and epithelial cancer tissues was detected and compared by immunohistochemistry. Univariate and multivariate analyses were performed to identify factors associated with elevated serum CA125 level. The correlation between the immunoreactivity of CA125 in tissue and serum CA125 level was examined by Pearson correlation analysis.
Elevated serum CA125 level (range 36.7–1848 u/m) was found in 66 of 580 (11.3%) ovarian fibroma/fibrothecoma patients. Univariate analysis showed that the elevated serum CA125 level was significantly correlated with tumor diameter ≥10 cm (P < .001), ascites (P < .001), and hydrothorax (P < .001). Multivariate analysis revealed that tumor diameter ≥10 cm and ascites were independently associated factors (P < .001 and < .001 respectively). Immunohistochemical staining showed that the expression of CA125 was negative in all fibroma/fibrothecoma tissues, but positive in all EOC tissues, and the immunoreactivity for CA125 was positively correlated with serum CA125 level in the EOC patients (P = .005).
The elevated serum CA125 level in ovarian fibroma/fibrothecoma is nontumor originated and occurs more frequently in those with larger size tumor or Meigs syndrome.
Keywords: clinicopathological characteristics, epithelial ovarian carcinoma (EOC), ovarian fibroma/fibrothecoma, serum CA125
1. Introduction
Since OC125 antigen (CA125) was discovered in 1981,[1] the detection of serum CA125 level by immune-assay has been developed for differential diagnosis between benign and malignant ovarian epithelial tumors and monitoring the outcome of epithelial ovarian carcinoma (EOC), though its sensitivity is suboptimal as an biomarker for screening or early diagnosis for EOC.
Ovarian fibroma/fibrothecoma is classified as sex cord stromal tumors, accounting for approximately 5% to 8% of all ovarian tumors and including 3 pathologic subtypes (fibroma, thecoma, and fibrothecoma) based on the different compositions of fiber and theca ingredients.[2] Most of ovarian fibromas/fibrothecomas occur in adolescents and young women, and show a solid pelvic or adnexal mass with benign biobehavior. About 10% to 15% of ovarian fibromas/fibrothecomas can be combined with ascites, however, less than 1% are combined with both ascites and hydrothorax, known as Meigs syndromes.[3,4] Meigs syndrome, first defined by Meigs and Cassa in 1937, possesses the triad of benign ovarian tumor (fibroma, Brenner tumor, and occasionally granulosa cell tumor) with ascites and hydrothorax, which disappears spontaneously after the tumor be removed.[5] No specific tumor biomarker can be identified in the majority of ovarian fibromas/fibrothecomas, except for serum CA125 elevation occasionally.[5–14] Ovarian fibroma/fibrothecoma with elevated serum CA125 level is rarely encountered in clinical practice, and easily misdiagnosed as EOC, especially in postmenopausal women. Although some case-report literatures have shown that Meigs syndrome caused by fibroma/fibrothecoma can be combined with an elevated serum CA125 level,[5–14] the possible associated factors and origin of serum CA125 are still unknown.
In this study, we retrospectively collected 580 patients with ovarian fibroma/fibrothecoma and compared the clinicpathologic parameters between the patients with and without elevated serum CA125 level. The aim of this study was to explore the clinicopathological characteristics and involved associating factors in ovarian fibroma/fibrothecoma with elevated serum CA125 level, so as to facilitate more exactly preoperative diagnosis of such a tumor.
2. Methods
2.1. Patients and tissue specimens
All patients underwent primary surgery and were pathologically diagnosed as ovarian fibroma, ovarian thecoma, or ovarian fibrothecoma in Women's Hospital, School of Medicine, Zhejiang University, during January 2001 to December 2016. Patients with elevated serum CA125 level caused by uterine leiomyoma, early pregnancy, endometriosis, or other diseases were excluded. Serum CA125 level was examined before definitive surgery and the level of 35 U/mL or above was defined as elevated. The clinical and pathological characteristics were collected and the formalin fixed paraffin embedded (FFPE) tissues were used for CA125 immunohistochemical staining. The study was approved by the Ethics Committee of the Hospital.
2.2. Immunohistochemical staining for CA125
Immunohistochemical staining for CA125 in formalin fixed paraffin embedded tissue samples (n = 28) was accessed, including ovarian fibroma/fibrothecoma with >250 U/mL of serum CA125 level (n = 10), ovarian fibroma/fibrothecoma with <35 U/mL of serum CA125 (n = 10), and epithelial ovarian cancer with >250 U/mL of serum CA125 (n = 8) as controls, including 2 serous, 2 mucinous, 2 endometrioid, and 2 clear cell ovarian cancers.
The primary antibodies used for immunohistochemistry analysis were anti-CA125 antibody (1:1000) from Santa Cruz Biotechnology (Santa Cruz, Heidelberg, Germany). The percentage of positive cells was scored as: 0 (0%); + (<10%); ++ (11%–50%); +++ (51%–80%); and ++++ (>80%). The staining intensity was defined as: 0∗ (negative), 1∗ (weak), 2∗ (moderate), and 3∗ (strong). Detailed protocols, antibody dilutions, image acquisition, and immunohistochemistry analysis were described previously.
2.3. Statistical analysis
Categorical data were compared between groups by using univariate chi square test or Fisher exact test and expressed as the relative risk. Multivariate logistic regression analysis was used to evaluate the correlation between the continuous variables. P value < .05 was considered statistically significant.
3. Results
3.1. Clinical characteristics of patients with elevated CA125 level
During the 15-year study period, a total of 580 patients were surgically managed and pathologically diagnosed as ovarian fibroma/fibrothecoma in our hospital. The clinical features of those patients are summarized and illustrated in Table 1.
Table 1.
The relationship between the serum CA125 and clinicopathological parameters.
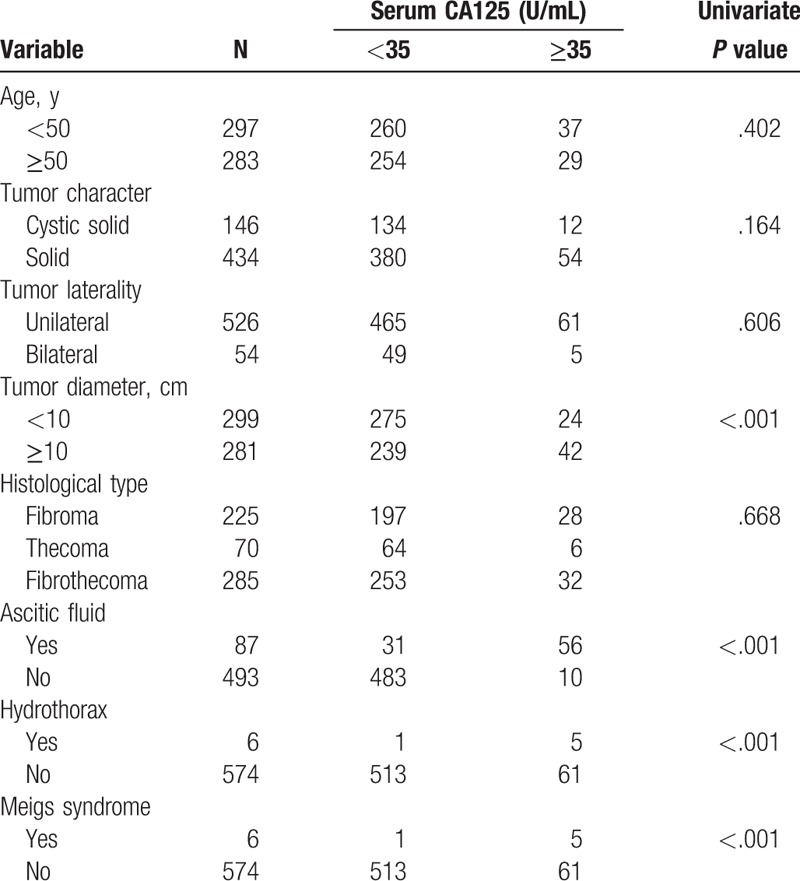
Among 580 patients, 66 (11.3%) were preoperatively found to be elevated serum CA125 level, range from 36.7 to 1848 U/mL. The mean age of 66 patients was 49.37 (range 22–75) years. The main indication of surgery was pelvic mass detected by ultrasonography, including 61 unilateral and 5 bilateral lesions. The final histological diagnoses were ovarian fibroma in 28 (42.4%), ovarian thecoma in 6 (9.1%), and ovarian fibrothecoma in 32 (48.5%) patients. Among 66 patients, 56 (84.8%) presented ascites, with the amount of fluid ranging from 50 to 3500 mL, and 5 (7.58%) presented ascites combined with hydrothorax and were diagnosed as Meig syndrome, 2 of them presented above 1000 U/mL of serum CA125 level. After surgery, 64 patients were followed up in out-patient interview for an average 45 months (range 7–240 months). No recurrence was observed by clinical and sonographic examination. Ascites and hydrothorax disappeared spontaneously at the fourth month after operation.
3.2. Factors associated with elevated serum CA125 level
To examine clinicopathologic factors associated with elevated serum CA125 level, the age of patients, tumor size, histological type, ascites, hydrothorax, tumor characters, and Meigs syndrome were compared between 66 patients with elevated serum CA125 level and 514 without. As shown in Table 1, univariate analysis revealed that 10 cm or more tumor size, ascites, hydrothorax, and Meigs syndrome were significantly more frequent in patients with elevated CA125 than that in those without (P < .001, < .001, and < .001, respectively). Furthermore, multivariate logistic regression analysis revealed that tumor diameter ≥10 cm and ascites were independently associated factors (P < .001 and < .001 respectively), as shown in Table 2.
Table 2.
Odds for elevated serum CA125 analyzed by multivariate logistic regression.

3.3. Immunohistochemical staining for CA125
To clarify the origin of elevated serum CA125, immunohistochemical staining for CA125 was performed in 10 ovarian fibroma/fibrothecoma tissues with elevated CA125 level and 10 tissues without, and 8 tissue samples from epithelial ovarian cancer with >250 U/mL of serum CA125 were selected as controls. As shown in Fig. 1, CA125 staining was mainly localized in the cytomembrane. Interestingly, all of 20 ovarian fibromas/fibrothecomas, including with elevated and normal serum CA125 level, presented negative CA125 staining. Contrarily, the immunoreactivity for CA125 was positive in all epithelial ovarian carcinoma tissues and correlated positively with serum CA125 level (P = .005).
Figure 1.
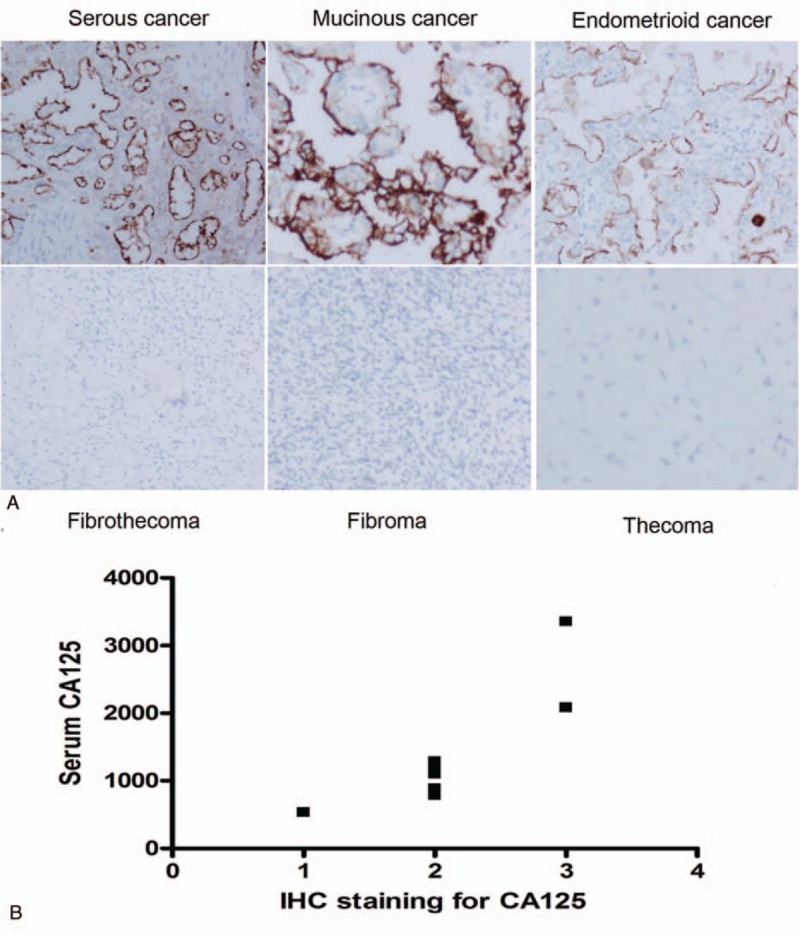
Immunohistochemical staining for CA125 on formalin fixed paraffin embedded (FFPE) ovarian tumor tissues and the correlation with serum CA125 level. A, Immunohistochemical staining for CA125 was accessed in 28 formalin fixed paraffin embedded (FFPE) tissues. All of 20 ovarian fibromas/fibrothecomas including elevated and normal serum CA125 level presented negative CA125 staining, all of 8 epithelial carcinoma tissues presented positive CA125 staining. B, Immunohistochemical staining for CA125 in epithelial carcinoma tissues was positively correlated to serum CA125 level (P = .005).
4. Discussion
CA125 antigen is a glycoprotein with a high molecular weight and can be recognized by a monoclonal antibody. Various data have shown the association of an elevated serum CA125 level with ovarian epithelial carcinoma. However, it has been observed that the elevation of CA125 level also occurs in 29% of patients with nongynecological cancers and some benign gynecological conditions, such as pelvic inflammatory disease, endometriosis, uterine leiomyoma, and early pregnancy, even in peritoneal, pleural and pericardial inflammation or irritation.[1]
Ovarian fibroma/fibrothecoma derives from sex cord stromal and often presents benign biobehavior with a good prognosis. The most common sign is unilaterally asymptomatic pelvic mass. Ovarian fibroma/fibrothecoma with elevated serum CA125 level is rarely encountered in clinical practice, and can be indexed in only 2 studies with small samples.[2,3] Chechia et al[3] measured serum CA125 level in 21 fibroma/fibrothecoma patients and found that 3 (14.2%) had values ≥ 35 U/mL. Chen et al[2] found that 12 (20.6%) had serum CA125 value ≥ 35 U/mL in 58 ovarian fibroma/fibrothecoma patients. In this study with the largest samples so far, to our knowledge, we found that in total 66 (11.4%) presented elevated serum CA125 level in 580 ovarian fibroma/fibrothecoma patients, which is little lower than that reported in above-mentioned 2 studies. When ovarian fibroma/fibrothecoma combines an elevated serum CA125 level, it may be confused with epithelial ovarian carcinoma. The differential diagnosis between ovarian fibroma/fibrothecoma and epithelial carcinoma is needed in such a condition, especially for a postmenopausal woman. Meigs syndrome caused by ovarian fibroma/fibrothecoma can be combined with an elevated serum CA125 level, but only 32 cases have been reported in the published literatures, up to now.[5–14] Liou et al[11] reviewed Meigs syndrome with elevated serum CA125 level and found that ascitic volume was positively correlated with CA125 level. In our series, univariate analysis showed that the elevated serum CA125 level was significantly correlated tumor with 10 cm or more diameter (P < .001), ascites (P < .001), hydrothorax (P < .001), and Meigs syndrome (P < .001), but multivariate analysis revealed that tumor diameter ≥10 cm and ascites were independent associated factors (P < .001 and < .001, respectively). Although the ultimate diagnosis of ovarian fibroma/fibrothecoma always depends on the intraoperative findings and should be confirmed by histological examination, our results might provide some clues, to some extent, to differentiate ovarian fibroma/fibrothecoma from epithelial ovarian carcinoma.
The source of serum CA125 in ovarian fibroma/fibrothecoma remains unclear. Some previous studies have considered that elevated serum CA125 is originated from nontumor cells, and some biochemical factors may be involved in this condition, such as a mechanical irritation of peritoneum or an increase in intraperitoneal pressure from a large volume of tumor and ascites.[1] In this study, we accessed the immunohistochemical staining for CA125 in 20 ovarian fibroma/ fibrothecoma tissues with or without elevated serum CA125 as well as 8 epithelial carcinoma tissues with >250 U/mL of elevated serum CA125 as controls, and found that all fibromas/fibrothecoma tissues were negative and epithelial carcinoma tissues were strongly positive for anti-CA125 antibody. Moreover, the immunoreactivity for CA125 was positively correlated with serum CA125 level in epithelial ovarian carcinoma. Our data suggest that elevated serum CA125 originate, at least partially, from tumor cells in epithelial ovarian carcinoma, but not from tumor cells in ovarian fibroma/fibrothecoma. Our results supported previous Timmerman findings that the peritoneal mesothelium cells might be the source of elevated serum CA125 in fibromas/fibrothecoma.[15]
In summary, ovarian fibromas/fibrothecoma is occasionally combined with elevated serum CA125 level, and such a condition is easily misdiagnosed as ovarian epithelial carcinoma. Large size tumor and ascites were independent associated factors, but tumor cells are not the origin of elevated serum CA125. Gynecologists should be aware of the clinical features of this unusual ovarian tumor, and conservative surgery and intraoperative frozen section are an option, especially for the patients with the reproductive age.
Author contributions
Data curation: Yun Liang.
Formal analysis: Weiguo Lu.
Funding acquisition: Yuanming Shen.
Investigation: Yuanming Shen, Weiguo Lu.
Project administration: Xiaoyun Wan.
Writing – original draft: Yuanming Shen.
Writing – review & editing: Xiaodong Cheng, Xing Xie, Xiaoyun Wan.
Footnotes
Abbreviations: CA125 = OC125 antigen, EOC = epithelial ovarian carcinoma, FFPE = formalin fixed paraffin embedded.
This research was supported by National Natural Science Foundation of China NO. 81501233, Health and Medicine of Zhejiang province China NO. 2016KYB164.
This work has not been previously presented in any form.
The authors have no conflicts of interest to disclose.
References
- [1].Bottoni P, Scatena R. The role of CA 125 as tumor marker: biochemical and clinical aspects. Adv Exp Med Biol 2015;867:229–44. [DOI] [PubMed] [Google Scholar]
- [2].Chen H, Liu Y, Shen LF, et al. Ovarian thecoma-fibroma groups: clinical and sonographic features with pathological comparison. J Ovarian Res 2016;9:81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Chechia A, Attia L, Temime RB, et al. Incidence, clinical analysis, and management of ovarian fibromas and fibrothecomas. Am J Obstet Gynecol 2008;199:473.e1–4.e1. [DOI] [PubMed] [Google Scholar]
- [4].Cho YJ, Lee HS, Kim JM, et al. Clinical characteristics and surgical management options for ovarian fibroma/fibrothecoma: a study of 97 cases. Gynecol Obstet Invest 2013;76:182–7. [DOI] [PubMed] [Google Scholar]
- [5].Cha MY, Roh HJ, You SK, et al. Meigs’ syndrome with elevated serum CA 125 level in a case of ovarian fibrothecoma. Eur J Gynaecol Oncol 2014;35:734–7. [PubMed] [Google Scholar]
- [6].Sofoudis C, Kouiroukidou P, Louis K, et al. Enormous ovarian fibroma with elevated Ca-125 associated with Meigs’ syndrome. Presentation of a rare case. Eur J Gynaecol Oncol 2016;37:142–3. [PubMed] [Google Scholar]
- [7].Chan WY, Chang CY, Yuan CC, et al. Correlation of ovarian fibroma with elevated serum CA-125. Taiwan J Obstet Gynecol 2014;53:95–6. [DOI] [PubMed] [Google Scholar]
- [8].Yazdani S, Alijanpoor A, Sharbatdaran M, et al. Meigs’ syndrome with elevated serum CA125 in a case of ovarian fibroma /thecoma. Caspian J Intern Med 2014;5:43–5. [PMC free article] [PubMed] [Google Scholar]
- [9].Morán-Mendoza A, Alvarado-Luna G, Calderillo-Ruiz G, et al. Elevated CA125 level associated with Meigs’ syndrome: case report and review of the literature. Int J Gynecol Cancer 2006;16(suppl 1):315–8. [DOI] [PubMed] [Google Scholar]
- [10].Park JW, Bae JW. Postmenopausal Meigs’ syndrome in elevated CA-125: a case report. J Menopausal Med 2015;21:56–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Liou JH, Su TC, Hsu JC. Meigs’ syndrome with elevated serum cancer antigen 125 levels in a case of ovarian sclerosing stromal tumor. Taiwan J Obstet Gynecol 2011;50:196–200. [DOI] [PubMed] [Google Scholar]
- [12].Amorim-Costa C, Costa A, Baptista P, et al. Sclerosing stromal tumour of the ovary associated with Meigs’ syndrome and elevated CA125. J Obstet Gynaecol 2010;30:747–8. [DOI] [PubMed] [Google Scholar]
- [13].Benjapibal M, Sangkarat S, Laiwejpithaya S, et al. Meigs’ syndrome with elevated serum CA125: case report and review of the literature. Case Rep Oncol 2009;2:61–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Jung NH, Kim T, Kim HJ, et al. Ovarian sclerosing stromal tumor presenting as Meigs’ syndrome with elevated CA-125. J Obstet Gynaecol Res 2006;32:619–22. [DOI] [PubMed] [Google Scholar]
- [15].Timmerman D, Moerman P, Vergote I. Meigs’ syndrome with elevated serum CA 125 levels: two case reports and review of the literature. Gynecol Oncol 1995;59:405–8. [DOI] [PubMed] [Google Scholar]