

Abstract
We conducted a multicenter retrospective analysis to evaluate the efficacy of systemic chemotherapy for unresectable combined hepatocellular and cholangiocarcinoma. We enrolled 36 patients with pathologically proven, unresectable combined hepatocellular and cholangiocarcinoma treated with systemic chemotherapy. The log‐rank test determined the significance of each prognostic factor. Elevated alpha‐fetoprotein, carcinoembryonic antigen and carbohydrate antigen 19‐9 levels were observed in 58.3%, 16.7% and 38.9% of patients, respectively. First‐line chemotherapy included platinum‐containing regimens consisting of gemcitabine/cisplatin (n = 12) and fluorouracil/cisplatin (n = 11), sorafenib (n = 5) and others (n = 8). The median overall and progression‐free survival times were 8.9 and 2.8 months, respectively, with an overall response rate of 5.6%. Prognostic factors associated with negative outcomes included poor performance status, no prior primary tumor resection, a Child‐Pugh class of B, and elevated carcinoembryonic antigen levels with a hazard ratio of 2.25, 2.48, 3.25 and 2.84 by univariate analysis, respectively. The median overall survival times of the gemcitabine/cisplatin, fluorouracil/cisplatin, sorafenib and other groups were 11.9, 10.2, 3.5 and 8.1 months, respectively. Multivariate analysis revealed that the overall survival of patients within the sorafenib monotherapy group was poor compared with platinum‐containing regimens (HR: 15.83 [95% CI: 2.25‐111.43], P = .006). All 7 patients in the sorafenib group had progressive disease, including 2 patients with second‐line therapy. In conclusion, the platinum‐containing regimens such as gemcitabine/cisplatin were associated with more favorable outcomes than sorafenib monotherapy for unresectable combined hepatocellular and cholangiocarcinoma.
Keywords: Cisplatin, drug therapy, gemcitabine, prognosis, sorafenib
1. INTRODUCTION
Combined hepatocellular and cholangiocarcinoma (CHC) is a primary liver cancer that comprises unequivocal and intimately mixed elements of both hepatocellular carcinoma and cholangiocarcinoma.1 This type of liver cancer accounts for just 0.4%‐14.5% of primary liver cancers,2, 3 with only 46 deaths attributed to CHC in Japan in 2014.4 Regarding the treatment of CHC, surgical resection is the only standard of care,5 and prognostic factors have also been reported in patients who have undergone surgical resection: patients with a tumor diameter of >5.0 cm, a cholangiocarcinoma‐dominant tumor, low‐attenuation lesions, and lymph node metastasis or portal vein invasion have a poorer prognosis.6, 7, 8, 9, 10, 11 In contrast to resectable patients, a standard treatment has not yet been established for unresectable patients. In practice, systemic chemotherapy is frequently used in unresectable CHC patients, according to the treatment strategy of unresectable hepatocellular carcinoma or cholangiocarcinoma, although it is not evidence‐based. Furthermore, there have been few reports on the prognostic factors of unresectable patients. Therefore, we conducted a multicenter retrospective analysis to evaluate the efficacy of systemic chemotherapy and prognostic factors in patients with unresectable CHC.
2. MATERIALS AND METHODS
2.1. Patients
Patients with pathologically proven, unresectable or recurrent, CHC treated with systemic chemotherapy from January 2002 to December 2015 were enrolled from 15 institutions in Japan. The exclusion criteria included those with “double cancer,” which is defined as CHC by Allen's classification but neither by Goodman's classification nor the WHO classification. In addition, it is practical to treat the more malignant tumor rather than the more indolent one in the case of patients with 2 different types of tumors. Those with “type 3 fibrolamellar tumor,” which is defined as CHC by Goodman's classification, but not by Allen's classification, were also excluded. Tumors with high attenuation in >50.0% of the entire tumor in early‐phase dynamic CT were defined as “hypervascular type” and those with high attenuation in <50.0% of the entire tumor were defined as “hypovascular type” (Figure 1). All study participants provided informed consent prior to commencing systemic chemotherapy. The retrospective design of this study was approved by the Institutional Review Board of each participating institution. Research was conducted in accordance with the Declaration of Helsinki (as revised in Fortaleza, Brazil, October 2013).
Figure 1.
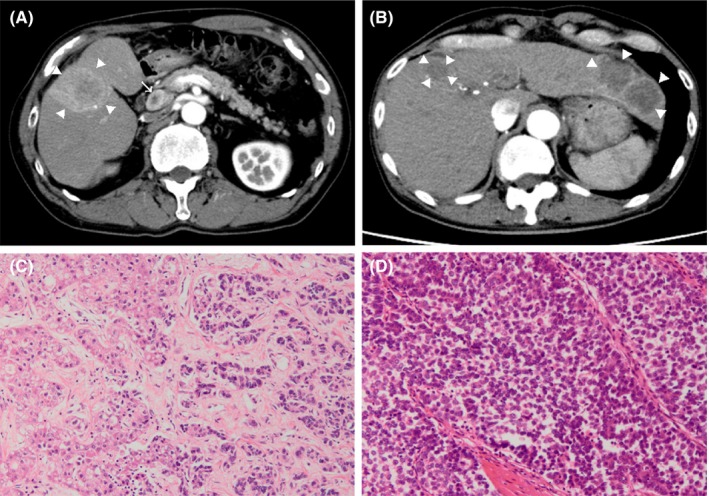
Images of enhanced CT and histopathological specimens. A, Tumors with high attenuation in >50.0% of the entire tumor at early phase were defined as hypervasular type (allow head), and (B) tumors with high attenuation in <50.0% were defined as “hypovascular type” (allow head). C, Collision tumor in Goodman's classification or combined tumor in Allen's classification has distinct epicenters of hepatocellular carcinoma (left side) and cholangiocellular carcinoma (right side) in the same tumor. D, Transitional tumor in Goodman's classification or mixed tumor in Allen's classfication comprise of closely admixing distinguished foci of hepatocellular carcinoma and cholangiocarcinoma
2.2. Systemic chemotherapy regimens
Systemic chemotherapy regimens were determined at the physicians’ discretion, including second‐line or higher‐line treatments after failure with first‐line chemotherapy. All patients continued chemotherapy until clinical or radiological disease progression, intolerable adverse events or patient refusal.
2.3. Clinical outcomes
Data were collected by retrospective review of medical records at each institution. Overall survival (OS) was defined as the time interval between the date of commencing first‐line systemic chemotherapy and the date of death from any cause or last follow‐up. Progression‐free survival (PFS) was defined as the time interval between the date of commencing first‐line systemic chemotherapy and the date of documented disease progression or death. Disease progression was judged by either radiological or clinical progression. OS and PFS times were calculated using the Kaplan‐Meier method. The treatment effects of each systemic chemotherapy were radiologically evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST, version 1.1), although we did not confirm the objective response because of poor prognosis.12 The overall response rate (ORR) was defined as the proportion of patients who achieved a complete or partial response divided by the total number of patients enrolled in the study. The disease control rate was defined as the proportion of patients who achieved a complete or partial response, or stable disease, divided by the total number of patients enrolled in the study.
2.4. Statistical analyses
Univariate analysis and multivariate analysis using a Cox regression hazard model were conducted to evaluate prognostic factors for OS. Multivariate analysis was performed by backward selection using factors that had a P‐value <.10 in the univariate analysis, because there were too few patients to detect statistical differences by using P‐value <.05. Patient characteristics, the ORR and the disease control rates were compared for each regimen using Fisher's exact test. All statistical analyses were conducted using the Statistical Package for the Social Sciences for Windows, software version 22.0 (IBM, Armonk, NY, USA).
3. RESULTS
3.1. Patients
In total, 36 patients were enrolled in this study. The patient characteristics are summarized in Table 1. A pathological diagnosis was obtained by examining archived histology specimens for 21 patients (58.3%) and biopsy specimens for 15 patients (41.7%). Twenty‐four patients (66.6%) had chronic liver disease, mainly due to hepatitis B or hepatitis C viral infections. Approximately half the patients had a history of primary tumor resection, although they had good liver function (Child‐Pugh class of A). Regarding the clinical findings, 25 patients (69.5%) exhibited a “hypovascular type” of tumor when evaluated with dynamic contrast‐enhanced CT. Approximately 70% of the patients had stage 4 disease according to the staging system of hepatocellular carcinoma by the Union for International Cancer Control. Serum alpha‐fetoprotein (AFP), des‐gamma carboxyprothombin (DCP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19‐9 (CA19‐9) levels were elevated in 21 (61.8%) of 34, 12 (36.4%) of 33, 6 (18.8%) of 32, and 14 (43.8%) of 32 patients, respectively.
Table 1.
Patient characteristics
| Characteristic | Patients (n = 36) |
|---|---|
| Age (years), median (range) | 62 (24‐83) |
| Sex, n (%) | |
| Male | 26 (72.2) |
| Female | 10 (27.8) |
| CHD, n (%) | 24 (66.6) |
| HBV | 9 (25.0) |
| HCV | 7 (19.4) |
| Other | 8 (22.2) |
| ECOG PS, n (%) | |
| 0 | 25 (69.5) |
| 1 | 8 (22.2) |
| Unknown | 3 (8.3) |
| History of primary tumor resection, n (%) | 19 (52.8) |
| Hypervascular portion (%), n (%) | |
| <50.0 | 25 (69.5) |
| ≥50.0 | 8 (22.2) |
| Unknown | 3 (8.3) |
| Macrovascular invasion, n (%) | 6 (16.7) |
| Extrahepatic metastasis, n (%) | 17 (47.2) |
| UICC stagea | |
| I | 1 (2.8) |
| II | 4 (11.1) |
| III | 6 (16.7) |
| IV | 25 (69.4) |
| Child‐Pugh class, n (%) | |
| A | 24 (66.6) |
| B | 5 (14.0) |
| Unknown | 7 (19.4) |
| AFP levels (ng/mL), n (%) | |
| <14.0 | 13 (36.1) |
| ≥14.0 | 21 (58.3) |
| Unknown | 2 (5.6) |
| Median (range) | 75.4 (0.0‐33 119.0) |
| DCP levels (mAU/mL), n (%) | |
| <40.0 | 21 (58.3) |
| ≥40.0 | 12 (33.4) |
| Unknown | 3 (8.3) |
| Median (range) | 30.0 (0.0‐31 121.0) |
| CEA levels (ng/mL), n (%) | |
| <5.0 | 26 (72.2) |
| ≥5.0 | 6 (16.7) |
| Unknown | 4 (11.1) |
| Median (range) | 2.4 (0.0‐47.0) |
| CA19‐9 levels (U/mL), n (%) | |
| <37.0 | 18 (50.0) |
| ≥37.0 | 14 (38.9) |
| Unknown | 4 (11.1) |
| Median (range) | 22.4 (0.0‐38 111.0) |
| Goodman's classification, n (%) | |
| Collision tumor | 6 (16.7) |
| Transitional tumor | 13 (36.1) |
| Unknown | 17 (47.2) |
| Allen's classification, n (%) | |
| Combined | 8 (22.2) |
| Mixed | 16 (44.4) |
| Unknown | 12 (33.4) |
| WHO classification (2010), n (%) | |
| Classical | 14 (38.9) |
| Stem cell features | |
| Typical | 2 (5.6) |
| Intermediate | 3 (8.3) |
| Cholangiocellular | 4 (11.1) |
| Unknown | 13 (36.1) |
AFP, alpha‐fetoprotein; CA19‐9, carbohydrate antigen 19‐9; CEA, carcinoembryonic antigen; CHD, chronic hepatic disease; DCP, des‐gamma carboxyprothrombin; ECOG, Eastern Cooperative Oncology Group; HBV, hepatitis B virus; HCV, hepatitis C virus; PS, performance status; WHO, World Health Organization.
According to staging system of hepatocellular carcinoma by Union for International Cancer Control.
3.2. Systemic chemotherapy
Patients treated with first‐line systemic chemotherapy were classified into 4 groups according to the treatment regimen (Table 2): (1) gemcitabine plus cisplatin (n = 12); (2) fluorouracil plus cisplatin group (n = 11, comprising tegafur/gimeracil/oteracil [S‐1] plus cisplatin [n = 4], fluorouracil plus cisplatin and mitoxantrone [n = 3], fluorouracil plus cisplatin and epirubicin [n = 2], and fluorouracil plus cisplatin [n = 2]); (3) sorafenib monotherapy (n = 5); and (4) others group (n = 8, comprising S‐1 monotherapy [n = 4], gemcitabine monotherapy [n = 2], fluorouracil plus interferon [n = 1] and gemcitabine plus S‐1 [n = 1]). Second‐line systemic chemotherapy was administered to 11 patients (S‐1 monotherapy [n = 4], gemcitabine plus cisplatin [n = 2], gemcitabine plus S‐1 [n = 2], sorafenib monotherapy [n = 2] and gemcitabine monotherapy [n = 1]). Fluorouracil plus cisplatin‐based regimens were administered more frequently in male patients or patients with a “mixed tumor” status based on Allen's classification (P = .013 and P = .017, respectively). Gemcitabine plus cisplatin regimens were administered more frequently in female patients (P = .045) and sorafenib monotherapy exhibited a trend towards being more frequently administered in patients with elevated serum AFP levels (P = .073).
Table 2.
Four groups of first‐line systemic chemotherapy
| Regimen | Patients (n = 36) |
|---|---|
| 1. Gemcitabine plus cisplatin, n (%) | 12 (33) |
| 2. Fluorouracil plus cisplatin group, n (%) | |
| S‐1 plus cisplatin | 4 (11) |
| Fluorouracil plus cisplatin and mitoxantrone | 3 (8) |
| Fluorouracil plus cisplatin and epirubicin | 2 (6) |
| Fluorouracil plus cisplatin | 2 (6) |
| 3. Sorafenib monotherapy, n (%) | 5 (14) |
| 4. Others group, n (%) | |
| S‐1 monotherapy | 4 (11) |
| Gemcitabine monotherapy | 2 (6) |
| Fluorouracil plus interferon | 1 (3) |
| Gemcitabine plus S‐1 | 1 (3) |
S‐1, tegafur/gimeracil/oteracil.
3.3. Clinical outcomes
For the entire cohort, the median OS and PFS times were 8.9 (95% confidence interval [CI]: 4.6‐13.2) and 2.8 (95% CI: 0.8‐4.7) months, respectively (Figure 2A,B). Objective responses included 1 patient (2.8%) with a complete response, 1 patient (2.8%) with a partial response, 11 patients (30.6%) with stable disease, 20 patients (55.6%) with progressive disease and 3 patients (8.3%) who were not evaluable. This resulted in an ORR and disease control rate of 5.6% and 36.1%, respectively. Univariate analyses showed that patients exhibited a poor prognosis if they had a history of ECOG PS of 1, primary tumor resection, a Child‐Pugh class of B, or elevated serum CEA levels of ≥5.0 ng/mL (hazard ratio: 2.25 [95% CI: 0.90‐5.67], 2.48 [95% CI: 1.04‐5.88], 3.25 [95% CI: 0.99‐10.65] and 2.84 [95% CI: 0.98‐8.26], respectively).
Figure 2.
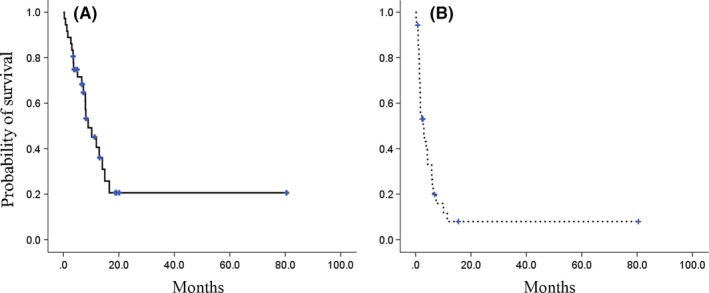
Kaplan‐Meier curves of (A) overall survival and (B) progression‐free survival in the entire study population
According to the treatment groups, the median OS times of the fluorouracil plus cisplatin, gemcitabine plus cisplatin, sorafenib monotherapy, and other groups were 11.9 (95% CI: 4.9‐18.8), 10.2 (95% CI: 3.9‐16.6), 3.5 (95% CI: 0.0‐7.6) and 8.1 (95% CI: 0.9‐15.4) months, respectively (Figure 3A). When a group included a platinum‐containing regimen, such as the fluorouracil plus cisplatin group and gemcitabine plus cisplatin group, the median OS time was 10.2 months (95% CI: 5.7‐14.7). OS times in the sorafenib monotherapy group were inferior to those in the gemcitabine plus cisplatin group (hazard ratio: 5.50 [95% CI: 1.17‐25.84]). Moreover, there were more optimal outcomes in OS among those who received platinum‐containing regimens than those in the sorafenib monotherapy group (hazard ratio: 4.49, 95% CI: 1.07‐18.92; P = .041). Multivariate analysis also demonstrated that first‐line systemic chemotherapy with sorafenib monotherapy was an independent poor prognostic factor compared to gemcitabine plus cisplatin‐based regimens (hazard ratio: 10.7, 95% CI: 1.4‐80.7; P = .022) (Table 3). The prognostic significance of sorafenib monotherapy was similar when compared with platinum‐containing regimen groups (hazard ratio: 15.83, 95% CI: 2.25‐111.43; P = .006). The median PFS times of each treatment group were 3.8 (95% CI: 0.5‐7.2), 3.0 (95% CI: 0.0‐9.1), 1.6 (95% CI: 1.2‐2.0) and 2.8 (95% CI: 0.2‐5.5) months, respectively (Figure 3B). There were no statistical differences in PFS times between the groups. However, none of the patients in the sorafenib monotherapy group achieved disease control, even when patients who received second‐line systemic chemotherapy with sorafenib monotherapy were included.
Figure 3.
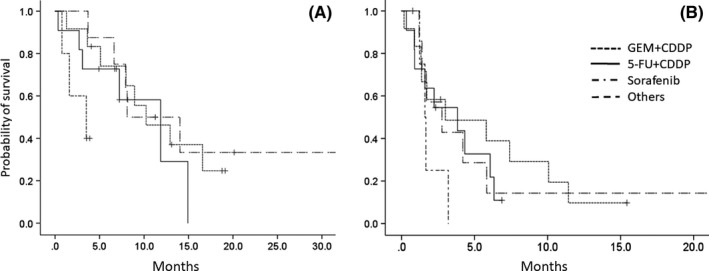
Kaplan‐Meier curves of (A) overall survival and (B) progression‐free survival according to each systemic chemotherapy regimen. The gemcitabine/cisplatin‐based, fluorouracil/cisplatin‐based and sorafenib‐based regimens are represented by the dotted, solid and chain lines, respectively. The other regimens are represented by the broken lines
Table 3.
Prognostic factors for overall survival
| Factor | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | P‐value | HR (95% CI) | P‐value | |
| ECOG PS | ||||
| 0 | 1 | 1 | ||
| 1 | 2.25 (0.90‐5.67) | .085 | 7.62 (1.84‐31.59) | .005a |
| Initially unresectable | ||||
| Yes | 1 | – | ||
| No | 2.48 (1.04‐5.88) | .034a | – | |
| Extrahepatic metastasis | ||||
| Yes | 1 | |||
| No | 1.15 (0.85‐1.55) | .38 | ||
| Tumor vascularity | ||||
| Hypervascular | 1 | |||
| Hypovascular | 1.19 (0.45‐3.12) | .72 | ||
| Child‐Pugh class | ||||
| A | 1 | – | ||
| B | 3.25 (0.99‐10.65) | .052 | – | |
| AFP levels (ng/mL) | ||||
| <14.0 | 1 | |||
| ≥14.0 | 0.76 (0.32‐1.79) | .53 | ||
| DCP levels (mAU/mL) | ||||
| <40.0 | 1 | |||
| ≥40.0 | 0.61 (0.24‐1.51) | .28 | ||
| CEA levels (ng/mL) | ||||
| <5.0 | 1 | – | ||
| ≥5.0 | 2.84 (0.98‐8.26) | .055 | – | |
| CA19‐9 levels (U/mL) | ||||
| <37.0 | 1 | |||
| ≥37.0 | 0.51 (0.20‐1.32) | .17 | ||
| Goodman's classification | ||||
| Collision tumor | 1 | |||
| Transitional tumor | 0.69 (0.31‐1.54) | .36 | ||
| Allen's classification | ||||
| Combined | 1 | |||
| Mixed | 0.61 (0.31‐1.18) | .14 | ||
| WHO classification (2010) | ||||
| Classical | 1 | |||
| Stem cell features | 0.52 (0.18‐1.51) | .23 | ||
| First‐line chemotherapy | ||||
| GEM+CDDP | 1 | 1 | ||
| 5‐FU+CDDP | 1.53 (0.51‐4.55) | .45 | 0.40 (0.078‐2.05) | .340 |
| Sorafenib | 5.50 (1.17‐25.84) | .031a | 10.65 (1.41‐80.74) | .022a |
| Other | 0.89 (0.29‐2.71) | .83 | 0.19 (0.024‐1.49) | .11 |
5‐FU, 5‐fluorouracil; AFP, alpha‐fetoprotein; CA19‐9, carbohydrate antigen 19‐9; CDDP, cisplatin; CEA, carcinoembryonic antigen; CI, confidence interval; CPS, Child‐Pugh score; DCP, des‐gamma carboxyprothrombin; ECOG, Eastern Cooperative Oncology Group; GEM, gemcitabine; HR, hazard ratio; PS, Performance status; WHO, World Health Organization.
P < .05.
We also compared the efficacies of each treatment type in patients with hypervascular tumors, high levels of AFP and low levels of CEA to confirm the superiority of platinum‐containing regimens over sorafenib, even in hepatocellular carcinoma‐like tumors (Table 4). The median OS times of the sorafenib monotherapy group were shorter than those in the group with a platinum‐containing regimen, even in patients with “hypervascular type” tumors (1.6 vs 11.9 months; P = .008). There were similar trends of high AFP levels and low CEA levels for hypervascular tumors, although these trends were not statistically significant. There was no influence of historical trend on the OS times in patients before and after the approval of sorafenib for hepatocellular carcinoma or cisplatin for biliary tract cancer, with P‐values of .23 and .93, respectively.
Table 4.
Comparison of the overall survival time between the platinum‐containing regimens and sorafenib group for hepatocellular carcinoma‐like tumors
| Platinum‐containing regimens | Sorafenib monotherapy | P‐value | |
|---|---|---|---|
| Hypervascular portion ≥50% | 11.9 (8.6‐15.1) | 1.6 (NA) | .008 |
| AFP levels ≥14.0 ng/mL | 12.9 (5.3‐20.6) | 3.5 (0‐7.6) | .093 |
| CEA levels <5.0 ng/mL | 10.2 (5.3‐15.1) | 3.5 (NA) | .26 |
NA, not applicable.
Hepatocellular carcinoma‐like tumors were hypervascular and had high AFP and low CEA levels. The data represent the median overall survival time with 95% confidence intervals.
4. DISCUSSION
Combined hepatocellular and cholangiocarcinoma is a rare type of primary liver cancer, which is more common in men and individuals with chronic liver disease caused by hepatitis B or hepatitis C viral infections, and these etiologies are more commonly associated with hepatocellular carcinoma rather than cholangiocarcinoma.6, 7, 13, 14, 15 With respect to histopathological findings, 2 classical classification systems (Goodman's and Allen's) have been used.2, 3 A new classification system was proposed by the World Health Organization in 2010.1 Contrast‐enhanced CT and MRI may be useful for determining CHC subtypes according to Goodman's or Allen's classification, although this remains experimental.16, 17, 18, 19 In unresectable patients, neither a standard of care nor prognostic factors have been established. Therefore, we conducted a multicenter retrospective analysis to evaluate the efficacy of systemic chemotherapy and prognostic factors in patients with pathologically‐proven unresectable CHC treated with systemic chemotherapies. Platinum‐containing regimens proved more promising than sorafenib monotherapy. Furthermore, poor liver function, no prior history of primary tumor resection and elevated serum CEA levels were identified as potential poor prognostic factors, although the statistical difference was small.
In a clinical setting, unresectable CHC patients are frequently administered treatments according to the treatment guidelines of either hepatocellular carcinoma or cholangiocarcinoma, which may be reasonable given that this type of tumor is comprised of hepatocellular carcinoma and cholangiocarcinoma. When considered as an unresectable hepatocellular carcinoma, patients are administered radiofrequency ablation, percutaneous transhepatic ethanol injections, transcatheter arterial chemoembolization or systemic chemotherapy. In systemic chemotherapies for advanced hepatocellular carcinoma, sorafenib has been a standard of care, and lenvatinib recently became another option.20 When considered to have an unresectable cholangiocarcinoma, patients are administered systemic chemotherapy such as gemcitabine plus cisplatin. We were unable to determine the best treatment strategy because biopsy specimens are representative of only part of the tumor, and it is difficult to know the precise composition of hepatocellular carcinoma and cholangiocarcinoma in each patient. In addition, recurrent lesions may not always have the same composition as previously resected lesions. Radiological findings of dynamic CT or MRI were reported to be useful in diagnosing whether the tumor is “cholangiocarcinoma‐dominant”.16, 17, 19 According to these findings, 69.0% of patients in the present study may have cholangiocarcinoma‐dominant tumors. Gemcitabine plus cisplatin showed antitumor activity in biliary tract cancer,21 and it seems reasonable that gemcitabine plus cisplatin exhibited a better outcome in our study. Another finding that supports the benefit of gemcitabine plus cisplatin is the identification of prognostic factors. Univariate analysis revealed elevated serum CEA levels (not AFP levels) to be a significant poor prognostic factor. This may suggest that we should treat the cholangiocarcinoma component, even in patients with “hepatocellular carcinoma‐dominant type” tumors. In addition, it was notable that sorafenib monotherapy did not exhibit better trends compared to platinum‐containing regimens, even in patients with “hypervascular type” tumors or elevated serum AFP levels, suggesting that platinum‐containing regimens may be more promising than sorafenib, even in unresectable patients with “hepatocellular carcinoma‐dominant type” CHC.
There are some reports of systemic chemotherapy for CHC, although these are reports of single cases or case series without detailed descriptions of the chemotherapy regimens (Table 5).22, 23, 24, 25, 26, 27, 28, 29 Therefore, we conducted a multicenter retrospective study to evaluate the efficacy of different regimens, although a future prospective randomized controlled study is needed to establish the standard of care for unresectable CHC. However, CHC is so rare that a prospective study may be difficult to conduct. In rare cancers, such as CHC, the development of biomarker‐targeted agents in basket trials may be favorable. A previous report30 demonstrated that TP53, FGFR4, FLT3 and EGFR were more frequently expressed in CHC than in hepatocellular carcinoma or cholangiocarcinoma, and other reports31, 32 documented that TP53, AR1D1A/2, PBRM1 and PTEN were expressed in CHC. We hope that more basic research of genetic mutations and subsequent basket trials will advance the treatment of unresectable CHC.
Table 5.
Literature review of systemic chemotherapy regimens for combined hepatocellular cholangiocarcinoma
| Author(s) | Patient(s) (n) | Regimen | Response | Survival |
|---|---|---|---|---|
| Lee et al22 | 7 | N/A | N/A | 1‐year and 3‐year survival rate: 42.9% and 14.3% |
| Chi et al23 | 1 | GEM+CDDP | PR | 31 months |
| FOLFOX | PD | |||
| Hatano et al24 | 1 | S‐1 | PR | N/A |
| Kitamura et al25 | 1 | 5‐FU+CDDP | PD | 6 months |
| GEM | SD | |||
| Shimizu et al26 | 1 | UFT | SD | 14 months |
| Kim et al27 | 1 | DOX+CDDP | PR | 18 months |
| 5‐FU | SD | |||
| Tani et al28 | 1 | GEM+CBDCA+5‐FU/LV | PR | 18 months |
| Hayashi et al29 | 1 | 5‐FU+CDDP+irradiation | N/A | 42 months |
5‐FU, 5‐fluorouracil; CBDCA, carboplatin; CDDP, cisplatin; DOX, doxorubicin; FOLFOX, 5‐fluorouracil/leucovorin/oxaliplatin; GEM, gemcitabine; LV, leucovorin; N/A, not available; PD, progressive disease; PR, partial response; S‐1, tegafur/gimeracil/oteracil; SD, stable disease; UFT, tegafur/uracil.
Our study has several limitations. First, is its retrospective design, which could lead to potential selection bias, and second is the small sample size, which could result in type I and type II statistical errors as well as multiplicity problems. Third, the population in this study may have been inaccurately categorized as having unresectable CHC because of the inclusion criteria of histopathologically proven CHC. Physicians will not take specimens from patients who have early enhancement of a tumor or a high level of AFP/DCP, or those who are diagnosed with hepatocellular carcinoma. In addition, patients who have tumors with a low attenuation indicated on imaging and a high level of CEA/CA19‐9 will be diagnosed with cholangiocellular carcinoma without a histopathological analysis. As a result, patients in this study might not represent those with unresectable CHC.
Despite these limitations, we concluded that, to the best of our knowledge, this is the first report to investigate the efficacy and prognostic factors of several chemotherapy regimens for unresectable CHC. Patients with poor liver function, no prior history of primary tumor resection and elevated serum CEA levels had a poor prognosis. These factors should be used to stratify patients in future clinical trials. In addition, platinum‐containing regimens, such as gemcitabine plus cisplatin, which is a current standard of care for unresectable cholangiocarcinoma, represent the most promising among several systemic chemotherapy regimens that are currently being adopted to treat unresectable CHC in a clinical setting. Further investigation is warranted to establish a standard therapy for unresectable CHC.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
ACKNOWLEDGMENTS
We would especially like to thank Takuji Okusaka of the National Cancer Center Hospital (Tokyo, Japan) for organizing the research group.
Kobayashi S, Terashima T, Shiba S, et al. Multicenter retrospective analysis of systemic chemotherapy for unresectable combined hepatocellular and cholangiocarcinoma. Cancer Sci. 2018;109:2549–2557. 10.1111/cas.13656
Funding information
This study was supported by a National Cancer Center Research and Development Fund (26‐A‐5) from the Ministry of Health, Labour, and Welfare of Japan. M.M. has received research funding from Kyowa Hakko Kirin and Merck Sharp & Dohme. Y.K has received research funding from Kyowa Hakko Kirin, NanoCarrier, Ono Pharmaceutical and Takeda Pharmaceutical. J.F. is a consultant/advisor to and has received honoraria and research funding from Astellas Pharma, Bayer AG, Chugai Pharmaceutical, Eisai, Eli Lilly Japan K.K., Merck Sharp & Dohme, Novartis, Ono Pharmaceutical, Shionogi & Taiho Pharmaceutical and Yakult Honsha. J.F. is a consultant/advisor to AstraZeneca, Boehringer Ingelheim GmbH, Bristol‐Myers Squibb, Fujifilm, J‐Pharma, Kyowa Hakko Kirin, Otsuka Pharmaceutical, Sandoz, Sanofi and Zeria Pharmaceutical; is part of the Speaker's Bureau for Taiho Pharmaceutical and Yakult Honsha; and has received honoraria and research funding from Daiichi Sankyo, Merck Serono, Mochida Pharmaceutical, Sumitomo Dainippon Pharma and Takeda Pharmaceutical. J.F. has also received honoraria from AstraZeneca, EA Pharma, Mitsubishi Tanabe Pharma, Pfizer and Sawai Pharmaceutical and research funding from Bristol‐Myers Squibb, Janssen Pharmaceuticals, J‐Pharma, Kyowa Hakko Kirin, NanoCarrier, OncoTherapy Science and Zeria Pharmaceutical.
REFERENCES
- 1. Bosman FT, Carneiro F, Hruban RH, Theise ND, ed. WHO Classification of Tumours of the Digestive System (4th edn). Lyon: International Agency for Research on Cancer; 2010. [Google Scholar]
- 2. Goodman ZD, Ishak KG, Langloss JM, Sesterhenn IA, Rabin L. Combined hepatocellular‐cholangiocarcinoma. A histologic and immunohistochemical study. Cancer. 1985;55:124‐135. [DOI] [PubMed] [Google Scholar]
- 3. Allen RA, Lisa JR. Combined liver cell and bile duct carcinoma. Am J Pathol. 1949;25:647‐655. [PMC free article] [PubMed] [Google Scholar]
- 4. Vital statistics of Japan, Ministry of Health, Labour and Welfare . http://www.mhlw.go.jp/english/database/db-hw/vs01.html. Accessed January 17, 2017.
- 5. Kassahun WT, Hauss J. Management of combined hepatocellular and cholangiocarcinoma. Int J Clin Pract. 2008;62:1271‐1218. [DOI] [PubMed] [Google Scholar]
- 6. Okuda K. Natural history of hepatocellular carcinoma including fibrolamellar and hepato‐cholangiocarcinoma variants. J Gastroenterol Hepatol. 2002;17:401‐405. [DOI] [PubMed] [Google Scholar]
- 7. Yano Y, Yamamoto J, Kosuge T, et al. Combined hepatocellular and cholangiocarcinoma: a clinicopathologic study of 26 resected cases. Jpn J Clin Oncol. 2003;33:283‐287. [DOI] [PubMed] [Google Scholar]
- 8. Koh KC, Lee H, Choi MS, et al. Clinicopathologic features and prognosis of combined hepatocellular cholangiocarcinoma. Am J Surg. 2005;189:120‐125. [DOI] [PubMed] [Google Scholar]
- 9. Yin X, Zhang BH, Qiu SJ, et al. Combined hepatocellular carcinoma and cholangiocarcinoma: clinical features, treatment modalities, and prognosis. Ann Surg Oncol. 2012;19:2869‐2876. [DOI] [PubMed] [Google Scholar]
- 10. Aishima S, Kuroda Y, Asayama Y, et al. Prognostic impact of cholangiocellular and sarcomatous components in combined hepatocellular and cholangiocarcinoma. Hum Pathol. 2006;37:283‐291. [DOI] [PubMed] [Google Scholar]
- 11. Lin G, Toh CH, Wu RC, et al. Combined hepatocellular cholangiocarcinoma: prognostic factors investigated by computed tomography/magnetic resonance imaging. Int J Clin Pract. 2008;62:1199‐1205. [DOI] [PubMed] [Google Scholar]
- 12. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228‐247. [DOI] [PubMed] [Google Scholar]
- 13. Liu CL, Fan ST, Lo CM, et al. Hepatic resection for combined hepatocellular and cholangiocarcinoma. Arch Surg. 2003;138:86‐90. [PubMed] [Google Scholar]
- 14. Chantajitr S, Wilasrusmee C, Lertsitichai P, Phromsopha N. Combined hepatocellular and cholangiocarcinoma: clinical features and prognostic study in a Thai population. J Hepatobiliary Pancreat Surg. 2006;13:537‐542. [DOI] [PubMed] [Google Scholar]
- 15. Tang D, Nagano H, Nakamura M, et al. Clinical and pathological features of Allen's type C classification of resected combined hepatocellular and cholangiocarcinoma: a comparative study with hepatocellular carcinoma and cholangiocellular carcinoma. J Gastrointest Surg. 2006;10:987‐998. [DOI] [PubMed] [Google Scholar]
- 16. Aoki K, Takayasu K, Kawano T, et al. Combined hepatocellular carcinoma and cholangiocarcinoma: clinical features and computed tomographic findings. Hepatology. 1993;18:1090‐1095. [PubMed] [Google Scholar]
- 17. Fukukura Y, Taguchi J, Nakashima O, Wada Y, Kojiro M. Combined hepatocellular and cholangiocarcinoma: correlation between CT findings and clinicopathological features. J Comput Assist Tomogr. 1997;21:52‐58. [DOI] [PubMed] [Google Scholar]
- 18. Sanada Y, Shiozaki S, Aoki H, Takakura N, Yoshida K, Yamaguchi Y. A clinical study of 11 cases of combined hepatocellular‐cholangiocarcinoma assessment of enhancement patterns on dynamics computed tomography before resection. Hepatol Res. 2005;32:185‐195. [DOI] [PubMed] [Google Scholar]
- 19. Nishie A, Yoshimitsu K, Asayama Y, et al. Detection of combined hepatocellular and cholangiocarcinomas on enhanced CT: comparison with histologic findings. AJR Am J Roentgenol. 2005;184:1157‐1162. [DOI] [PubMed] [Google Scholar]
- 20. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first‐line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non‐inferiority trial. Lancet. 2018;391:1163‐1173. [DOI] [PubMed] [Google Scholar]
- 21. Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. New Engl J Med. 2010;362:1273‐1281. [DOI] [PubMed] [Google Scholar]
- 22. Lee CH, Hsieh SY, Chang CJ, Lin YJ. Comparison of clinical characteristics of combined hepatocellular‐cholangiocarcinoma and other primary liver cancers. J Gastroenterol Hepatol. 2013;28:122‐127. [DOI] [PubMed] [Google Scholar]
- 23. Chi M, Mikhitarian K, Shi C, Goff LW. Management of combined hepatocellular‐cholangiocarcinoma: a case report and literature review. Gastrointest Cancer Res. 2012;5:199‐202. [PMC free article] [PubMed] [Google Scholar]
- 24. Hatano H, Kobayashi S, Nagano H, et al. A case of successful multimodal treatment for combined hepatocellular and cholangiocarcinoma with portal venous tumor thrombus]. Gan To Kagaku Ryoho. 2009;36:2374‐2376. [PubMed] [Google Scholar]
- 25. Kitamura T, Okada S, Yamamoto T, et al. A case of combined hepatocellular and cholangiocarcinoma developed 6 years after sustained virological response of interferon for hepatitis C and beneficial effect of gemcitabine for lymph node metastases. Liver Cancer. 2008;14:172‐177. [Google Scholar]
- 26. Shimizu J, Hayashi S, Dono K, et al. A case report of combined hepatocellular‐cholangiocarcinoma whose lymph node recurrence effectively treated with UFT. Gan To Kagaku Ryoho. 2009;36:2380‐2382. [PubMed] [Google Scholar]
- 27. Kim GM, Jeung HC, Kim D, et al. A case of combined hepatocellular‐cholangiocarcinoma with favorable response to systemic chemotherapy. Cancer Res Treat. 2010;42:235‐238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Tani S, Murata S, Tamura M, et al. Effectiveness of systemic chemotherapy of GEM+CBDCA+5‐FU/LV and hepatic arterial infusion of CDDP in a case of advanced, combined hepatocellular‐cholangiocarcinoma with multiple lung metastases. Nihon Shokakibyo Gakkai Zasshi. 2011;108:1892‐1901. [PubMed] [Google Scholar]
- 29. Hayashi H, Beppu T, Ishiko T, et al. A 42‐month disease free survival case of combined hepatocellular‐cholangiocarcinoma with lymph node metastases treated with multimodal therapy. Gan To Kagaku Ryoho. 2006;33:1941‐1943. [PubMed] [Google Scholar]
- 30. Keller JW, Doyle MM, Wang‐Gillam A, et al. Analysis of the genomic profile of biphenotypic tumors compared to cholangiocarcinoma and hepatocellular carcinoma. J Clin Oncol. 2014;32:226. [Google Scholar]
- 31. Fujimoto A, Furuta M, Shiraishi Y, et al. Whole‐genome mutational landscape of liver cancers displaying biliary phenotype reveals hepatitis impact and molecular diversity. Nat Commun. 2015;6:6120. [DOI] [PubMed] [Google Scholar]
- 32. Fujimoto A, Furuta M, Totoki Y, et al. Whole‐genome mutational landscape and characterization of noncoding and structural mutations in liver cancer. Nat Genet. 2016;48:500‐509. [DOI] [PubMed] [Google Scholar]