

Abstract
Background: Visit length is an indicator that can be used to assess patients’ satisfaction of the health care services. In recent years, some studies have focused on the mean visit time in Iran. This study aimed at determining the average visit time in Iran by performing a systematic review and meta-analysis.
Methods: In this study, Embase, PubMed/MEDLINE, Scopus, ISI/Web of Science databases, and Google Scholar search engine, as well as Iranian national databases/thesauri, such as MagIran, SID, and Irandoc were used. These databases were searched from their inception until September 2017. The quality of retained studies was assessed using the STROBE checklist. Average visit length was reported using stochastic model with 95% confidence interval (CI). I2 and Q tests were used to assess the heterogeneity of the studies. A sensitivity analysis was conducted to ensure the stability of the results.
Results: After searching the scholarly databases and reviewing the articles based on inclusion and exclusion criteria, 6 studies were finally selected. Based on the random model, the mean visit time was 4.89 minutes in Iran, ranging from 4.66 to 5.12 minutes (p=0.82). The most time visit in specialists belonged to psychiatrists with 9.12 (7.28 to 10.96) minutes (p=0.19) and the lowest belonged to internists with 3.59 (2.24 to 4.95) minutes (p=0.00), respectively.
Conclusion: The average visit time in Iran was estimated to be 4.89 minutes. To increase patients’ satisfaction and provide a better disease treatment and management in Iran, the following suggestions could be helpful: properly distributing physicians across the country, reducing waiting lists, and implementing the use of guidelines to standardize the visit time.
Keywords: Visit length, Physicians, Specialists, Iran, Systematic review, Meta-analysis
↑ What is “already known” in this topic:
Visit time depends on factors such as physicians' behavior, type of treatment, type of insurance, patient-physician relationship, geographical factors, culture, and structure/organization of health care system.
→ What this article adds:
The mean visit time was 4.89 minutes in Iran, ranging from 4.66 to 5.12 minutes. To the best of our knowledge, there are still no overviews addressing this important issue in Iran, whose findings could be of great help to the health sector policymakers to monitor the duration of medical visits in Iran and make plans to increase the visit time if necessary.
Introduction
Organizations providing health care services are seeking high-quality medical care services, which are the basic right of patients and an indicator of a good, efficient organization. The patient has the right to benefit from the best treatments available and from state-of-the-art facilities; furthermore, a proper physician-patient relationship makes the patient talk more comfortably about his/her disease condition, which in turn helps the physician in the diagnosis and selection of appropriate treatment. Adequately organized physician-patient appointments provide the possibility of such interaction (1). Moreover, visit length is considered an indicator that can be used to assess the patient's satisfaction of the provided health care services (2, 3). Visit time can be defined as the time from the moment the patient enters the examination room until he/she leaves the room (4). An ideal visit is recommended to last for about 10 to 15 minutes, respectively, for general practitioners and specialists (5). A range in the average visit length from 7 to 34 minutes has been reported in studies conducted in different contexts worldwide (5-8). Usually, the time dedicated to patients is short in developing countries due to lack of man power and lack of quality monitoring and supervision on the length of physicians' visits (9). Further, in some of these countries, some patients are visited together at the same time, which would violate patients' rights (10).
Visit time depends on factors such as physicians' behavior, type of treatment, type of insurance, patient-physician relationship, geographical factors, culture, and structure/organization of the health care system (11). Appropriate visit length enables a more efficient health care delivery such that the patient will feel less need for next visits. Fewer referrals will lead to a reduction in both direct and indirect costs and to a decrease of additional overhead costs. Many referrals can lengthen, indeed, the waiting queue in healthcare centers. An unusually long waiting time can lead to a reduced patients' satisfaction (12).
Medical visit length is important for physicians to help them understand the precise illness that the patients are suffering from and their causes and to prescribe the best management option (13, 14); moreover, it is important for patients to understand the treatment they should adhere to (13). A review study showed that appropriate visit time has favorable effects on the processes and results of treatment between the physician and the patient (15). Some studies indicate that the duration of the visit affects the quality of the services provided (16, 17).
In recent years, some studies have focused on the mean visit time in Iran; and awareness of this topic could help health care providers to better organize their practice, make plans to monitor visit time and its impact on patients' level of satisfaction and their treatment status.
Health care policymakers in Iran are working to increase the duration of medical visits in such a way that patients would feel more comfortable to talk to their physicians about their disease and/or symptoms. To the best of our knowledge, there are still no overviews addressing this important issue in Iran. Thus, this study aimed at determining the average visit time in Iran by performing a systematic review and meta-analysis.
Methods
The present study was conducted according to the PRISMA guideline, which is commonly used for assessing, synthesizing, and reporting primary studies in systematic reviews and/or meta-analyses (18).
To find relevant studies, we searched Embase, PubMed/MEDLINE, Scopus, ISI/Web of Science databases, and Google Scholar search engine, as well as Iranian national databases/thesauri, such as MagIran, SID, and Irandoc. These databases were searched from their inception until September 2017. The search strategy used was as follows: a string of keywords such as “visit time”, “length time”, “visit length” “hospital”, “physician” and “Iran” were properly connected by Boolean connectors. When appropriate, wildcard option and medical subject headings (MeSH) were used (The full search strategy used for searching in PubMed/MEDLINE is available in Appendix 1).
Inclusion criteria
Studies that reported visit length or consultation length by the physician were considered potentially eligible for the present study.
Exclusion criteria
On the contrary, studies without appropriate quantitative data or overlapping data were excluded.
Two authors independently assessed the quality of selected studies utilizing the STROBE checklist (19). Any disagreement was resolved through discussion and dialogue until consensus was reached. According to the quality scores, studies were classified into 3 classes: good, average, and weak. More specifically, studies that gained 1 to 9, 10 to 17, and 18 to 22 points were classified as poor, average, and good categories, respectively. After independently selecting the studies, two authors extracted information on articles including first author, year of publication, study setting, sample size, and reported mean visit length. Disagreement between the two authors was resolved by discussion or asking a third person as a judge (The STROBE is available in www.strobe-statement.org).
Average visit length was reported using stochastic model with its computed 95% confidence interval (CI). I2 test was used to assess heterogeneity among studies (14). A sensitivity analysis was conducted to ensure the stability of the obtained results. Subgroup analysis was performed based on quality and publication year of the studies retained in the current meta-analysis and their sample size. The meta-regression analysis was performed according to the year of publication, sample size, and source of heterogeneity between studies. Considering that the number of studies was less than 10, it was impossible to examine the publication bias.
Data analysis was performed using STATA Ver.12 (Stata Corp, College Station, TX, USA) software, and p-values less than 0.05 were considered significant.
Results
After searching the scholarly databases and reviewing articles based on inclusion and exclusion criteria, 6 studies were finally retained (20-25) . Figure 1 displays the details of the search process.
Fig. 1.
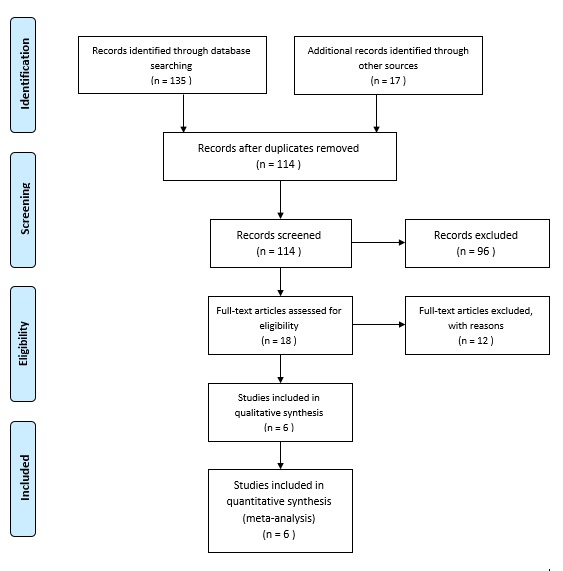
Flow chart of the present meta-analysis
Main characteristics of the studies included in the present meta-analysis can be found in Table 1.
Table 1. Characteristics of studies included .
| First author | Year | Type of study | Sample size | Mean (minutes) | City | Score of quality |
| Mosadegh rad | 2004 | Cross-sectional | 1336 | 4.34 | Ghazvin | 14 |
| Khori | 2012 | Cross-sectional | 620 | 6.9 | Gorgan | 15 |
| Mohebbifar | 2014 | Cross-sectional | 160 | NA | Ghazvin | 19 |
| Hasanpoor | 2015 | Cross-sectional | 428 | 4.67 | Ghazvin | 16 |
| Faraji Khiavi | 2016 | Cross-sectional | 550 | NA | Ahvaz | 20 |
| Janati | 2017 | Cross-sectional | 540 | 8.25 | Tabriz | 19 |
Based on the random model, the mean visit time was 4.89 minutes in Iran, ranging from 4.66 to 5.12 minutes (p= 0.829) (Fig. 2).
Fig. 2.
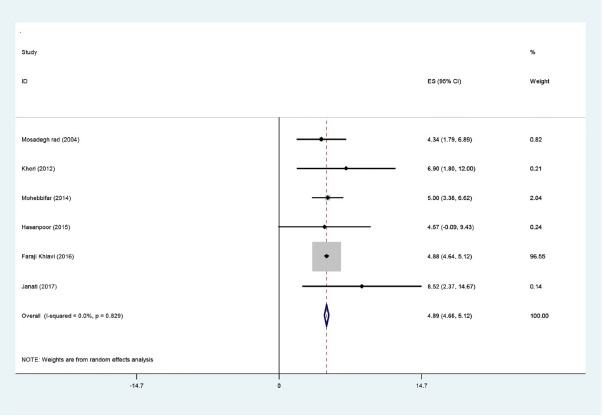
The overall mean visit time in Iran
The average visit time broken down by physicians' specialties is presented in Table 2 and Fig. 3.
Table 2. The average visit time broken down by physicians' specialties .
| Type of specialty | Number of studies | Mean of minutes (95%CI) | I 2 | p |
| Internal medicine | 4 | 3.59 (2.24 to 4.95) | 87.9% | <0.001 |
| Cardiology | 3 | 5.06 (1.08 to 9.05) | 99.5% | <0.001 |
| Infectious diseases | 2 | 5.91 (0.52 to 11.30) | 77.7% | 0.034 |
| Neurology | 3 | 3.8 (3.60 to 4.14) | 37.5% | 0.202 |
| Obstetrics and Gynecology | 4 | 4.21 (2.77 to 5.64) | 93.3% | <0.001 |
| Ophthalmology | 4 | 5.31 (3.69 to 6.94) | 95.6% | <0.001 |
| Orthopedic | 4 | 5.42 (3.93 to 6.92) | 96.4% | <0.001 |
| Pediatrics | 4 | 4.83 (3.13 to 6.53) | 88.3% | <0.001 |
| Psychiatry | 2 | 9.12 (7.28 to 10.960 | 40.5% | 0.195 |
| Surgery | 4 | 4.29 (3.59 to 4.99) | 44.3% | 0.145 |
| Urology | 4 | 4.55 (3.50 to 5.60) | 82.1% | <0.001 |
Fig. 3.
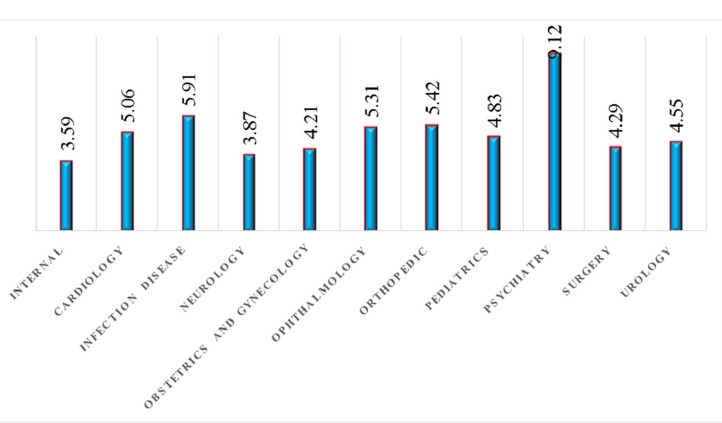
Graph of average visit time by physicians' specialties
Results of subgroups analysis based on year of publication, sample size, and quality of studies are demonstrated in Table 3.
Table 3. Result of subgroup analysis of average visit time in Iran .
| Variable | Number of studies | Mean in minutes (95%CI) | I 2 | p |
| Year of publication | ||||
| <2013 | 2 | 4.85 ( 2.57 to 7.13 ) | 0% | 0.378 |
| >2013 | 4 | 4.89 ( 4.65 to 5.12 ) | 0% | 0.713 |
| Sample size | ||||
| <500 | 2 | 4.97 ( 3.43 to 6.50 ) | 0% | 0.898 |
| >500 | 4 | 4.88 ( 4.65 to 5.12 ) | 0% | 0.548 |
| Quality of studies | ||||
| Good | 3 | 4.89 ( 4.66 to 5.12 ) | 0% | 0.506 |
| Medium | 3 | 4.82 ( 2.76 to 6.87 ) | 0% | 0.677 |
Results of meta-regression analysis based on publication year and sample size are presented in Table 4 and Fig. 4.
Table 4. Result of meta-regression of average visit time in Iran .
| Variable | Coef | SE | T | p |
| Year | -0.000 | 0.001 | -0.39 | 0.719 |
| Sample size | 0.030 | 0.1041 | 0.29 | 0.788 |
Fig. 4.

Meta-regression based on sample size and year of publication
Sensitivity analysis revealed that obtained results were robust and consistent, as no change could be detected before and after analysis (Fig. 5).
Fig. 5.
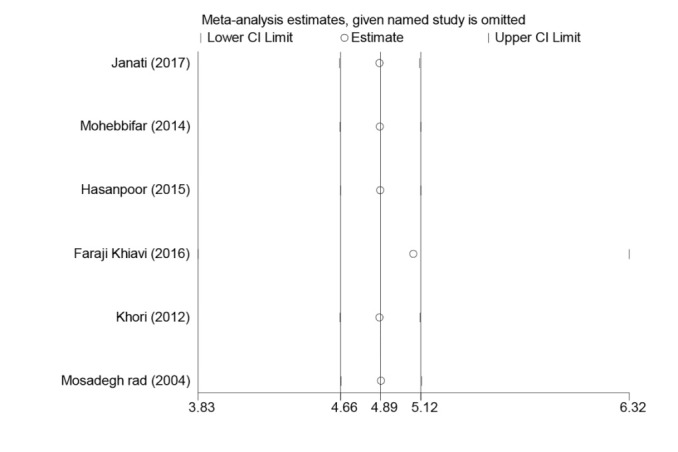
Sensitivity analysis
Discussion
Patients' satisfaction is an important part of a dynamic process that can result from a good and effective patient-physician relationship (26). The extant literature indicates that a good relationship between physicians and patients leads to a more effective treatment (27). For many diseases, behavioral changes and patient adherence to treatment regimen can be induced by an appropriate physician visit.
The finding of this study indicated that the average visit time was 4.89 minutes in Iran, which is comparable with that of other studies conducted in other countries (Table 5) (5-8, 28).
Table 5. Visit time in other countries in comparison with Iran .
| Author | Country | Average of visit |
| Chen | China | 34.3 |
| Bener | Qatar | From 7 to 17.4 |
| Tahepold | Estonia | 9 |
| Migongo | USA | 14.5 |
| Aomatsu | Japan | 17 |
In a study conducted in 6 European countries, it was found that average visit time was 7.6, 7.8, 9.4, 10.2, 15, 15.6 and 10.7 minutes in Germany, Spain, England, the Netherlands, Belgium, and Switzerland, respectively (29). However, visit length in Iran is significantly shorter. Physician shortage, high workload of physicians, long waiting lists, lack of proper guidelines, cultural-social conditions, disease type, personality characteristics of patients, and features of the health care system are among the factors which contribute to reduced visit time in Iran (29, 30). On the contrary, women and elderly patients are more likely to be visited for longer time (5). Another important factor is the place of residence (urban versus rural areas) (31). Also, physician characteristics, such as gender, age, and attitude towards patients, play a major role (29). Older and female physicians tend to have a positive attitude towards patients' problems, so they are more inclined to increase the visit length (32-34). Changes in the health care system can affect the visit time as well (11).
Furthermore, besides visiting patients, some Iranian physicians have managerial duties and administrative responsibilities (35).
The findings of our study showed that psychiatrists tended to visit their patients for longer time. The physician's visit length specifically depends on the type of disease. In the case of patients with mental health problems, physicians need more time to better diagnose the disease to talk to the patient and listen to his/her problems for longer time. Studies show that psychiatrists spend more time with their patients (36).
The findings of the current meta-regressions showed that visit time in Iran increased and decreased based on publication year and sample size, respectively, even though this trend was not statistically significant. Recently, the Iranian Ministry of Health and Medical Education (MOHME) delivered a national guideline for standardizing visit time and indicated that an appropriate visit should last 15, 25, and 30 minutes for general practitioners, specialist physicians, and psychiatrists, respectively. Iran’s health system underwent a major change in its health system. The plan of the 2014 health reformation has many goals, one of which is standardization of the visit time (16). This study found that there is still a gap between the current visit time and the announced standards.
However, this study had several limitations: first, the number of studies included in this meta-analysis was small; therefore, there is a need for further studies to better comment on the visit length in Iran. Also, the conducted studies were limited to few Iranian provinces, and considering the size and distribution of population in Iran, future studies should be performed in all provinces of Iran.
Conclusion
The average visit time in Iran was estimated to be 4.89 minutes. Thus, to increase patients’ satisfaction and provide a better disease treatment and management, the following actions may be useful: properly distributing physicians across the country, reducing waiting lists, and implementing the use of guidelines to standardize the visit time.
Conflict of Interests
The authors declare that they have no competing interests.
Appendix 1
Search strategy in Pub med:
#1 visit time
#2 length time
#3 visit length
#4 #1 OR #2 OR #3
#5 hospital
#6 physician
#7 specialist
#8 #5 OR #6 OR #7
#9 Iran
#10 #4 AND #8 AND #9
Cite this article as: Heydarvand S, Behzadifar M, Abolghasem Gorji H, Behzadifar M, Darvishnia M, Luigi Bragazzi N. Average medical visit time in Iran: A systematic review and meta-analysis. Med J Islam Repub Iran. 2018 (8 Jul);32:58. https://doi.org/10.14196/mjiri.32.58
References
- 1.Mattke S, Epstein AM, Leatherman S. The OECD Health Care Quality Indicators Project: history and background. Int J Qual Health Care. 2006;18:1–4. doi: 10.1093/intqhc/mzl019. [DOI] [PubMed] [Google Scholar]
- 2.Hutchinson PL, Do MAS. Measuring client satisfaction and the quality of family planning services: a comparative analysis of public and private health facilities in Tanzania, Kenya and Ghana. BMC Health Serv Res. 2011;11:203. doi: 10.1186/1472-6963-11-203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Behzadifar M, Mirzaei M, Behzadifar M, Keshavarzi A, Behzadifar M, Saran M. Patients’ Experience of Tuberculosis Treatment Using Directly Observed Treatment, Short-Course (DOTS): A Qualitative Study. Iran Red Crescent Med J. 2015;17:e20277. doi: 10.5812/ircmj.17(4)2015.20277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Aeenparast A, Tabibi SJ, Shahanaghi K, Aryanejhad M. Estimating outpatient waiting time: a simulation approach. Payesh. 2009;8:327–33. doi: 10.5812/ircmj.7908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chen BL, Li ED, Yamawuchi K, Kato K, Naganawa S, Miao WJ. Impact of adjustment measures on reducing outpatient waiting time in a community hospital: application of a computer simulation. Chin Med J (Engl) 2010;123:574–80. [PubMed] [Google Scholar]
- 6.Bener A, Al-Marri S, Abdulaziz A, Ali BS, Al-Jaber K, Mohammed H. Do Minutes Count for Health Care? Consultation Length in a Tertiary Care Teaching Hospital and in General Practice. Middle East J Fam Med. 2007;5:3–8. [Google Scholar]
- 7.Tähepold H, Maaroos HI, Kalda R, van den Brink-Muinen A. Structure and duration of consultations in Estonian family practice. Scand J Prim Health Care. 2003;21:167–70. doi: 10.1080/02813430310000708. [DOI] [PubMed] [Google Scholar]
- 8.Migongo AW, Charnigo R, Love MM, Kryscio R, Fleming ST, Pearce KA. Factors relating to patient visit time with a physician. Med Decis Making. 2012;32:93–104. doi: 10.1177/0272989X10394462. [DOI] [PubMed] [Google Scholar]
- 9.Dansky KH, Miles J. Patient satisfaction with ambulatory healthcare services: waiting time and filling time. Hosp Health Serv Adm. 1997;42:165–77. [PubMed] [Google Scholar]
- 10.Eldabi T, Irani Z, Paul RJ. A proposed approach for modelling health‐care systems for understanding. J Manag Med. 2002;16:170–87. doi: 10.1108/02689230210434916. [DOI] [PubMed] [Google Scholar]
- 11.Petek Šter M, Švab I, Živčec Kalan G. Factors related to consultation time: Experience in Slovenia. Scand J Prim Health Care. 2008;26:29–34. doi: 10.1080/02813430701760789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Solomon J. How strategies for managing patient visit time affect physician job satisfaction: a qualitative analysis. J Gen Intern Med. 2008;23:775–80. doi: 10.1007/s11606-008-0596-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kaplan SH, Greenfield S, Gandek B, Rogers WH, Ware JE. Characteristics of physicians with participatory decision-making styles. Ann Intern Med. 1996;124:497–504. doi: 10.7326/0003-4819-124-5-199603010-00007. [DOI] [PubMed] [Google Scholar]
- 14.Mechanic D, McAlpine DD, Rosenthal M. Are patients’ office visits with physicians getting shorter? N Engl J Med. 2001;344:198–204. doi: 10.1056/NEJM200101183440307. [DOI] [PubMed] [Google Scholar]
- 15.Wilson MA, Childs S. The relationship between consultation length, process and outcomes in general practice: a systematic review. Br J Gen Pract. 2002;?:521012–20. [PMC free article] [PubMed] [Google Scholar]
- 16.Heany D, Howie J, Porter A. Factors influencing waiting times and consultation times in general practice. Br J Gen Pract. 1991;41:315–9. [PMC free article] [PubMed] [Google Scholar]
- 17.Howie J, Porter A, Heany D, Hopton J. Long to short consultation ratio: a proxy measure of quality of care in general practice. Br J Gen Pract. 1991;41:48–54. [PMC free article] [PubMed] [Google Scholar]
- 18.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151:W65–94. doi: 10.7326/0003-4819-151-4-200908180-00136. [DOI] [PubMed] [Google Scholar]
- 19.Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ. et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med. 2007;147:W163–94. doi: 10.7326/0003-4819-147-8-200710160-00010-w1. [DOI] [PubMed] [Google Scholar]
- 20.Mosadegh Rad AM. The role of participative management in outpatients' waiting time, visit time and satisfaction at Razi Hospital. Hakim Health Sys Res. 2004;7:14–23. [Google Scholar]
- 21.Khori V, Changizi S, Biuckians E, Keshtkar A, Alizadeh AM, Mohaghgheghi AM. et al. Relationship between consultation length and rational prescribing of drugs in Gorgan City, Islamic Republic of Iran. East Mediterr Health J. 2012;1:480–6. doi: 10.26719/2012.18.5.480. [DOI] [PubMed] [Google Scholar]
- 22.Mohebbifar R, Hasanpoor E, Mohseni M, Sokhanvar M, Khosravizadeh O, Isfahani HM. Outpatient Waiting Time in Health Services and Teaching Hospitals: A Case Study in Iran. Glob J Health Sci. 2014;6:172–80. doi: 10.5539/gjhs.v6n1p172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hasanpoor E, Delgoshie B, Gorji H, khogam M, Sokhanvar M. Surveying The Standard of Outpatient Visit Time among General Hospitals: A case study in Qazvin. J Hosp. 2015;14:75–81. [Google Scholar]
- 24.Faraji Khiavi F, Qolipour M, Afshar Farouji D, Mirr I. Relationship between Outpatients’ Visit Time and Physicians’ Prescription Quality in Teaching Hospitals of Ahvaz: 2015. Glob J Health Sci. 2016;8:83–91. [Google Scholar]
- 25.Janati A, Hasanpoor E, Aslani F, HaghGoshayie E, Hassanzadeh E. Evaluating visit quality in plan of health sector evolution in Iran: A local survey from Tabriz. Int J Epidemiol Res. 2017;4:69–77. [Google Scholar]
- 26.Donabedian A. Evaluating the quality of medical care. Milbank Mem Fund Q. 1996;44:166–206. [PubMed] [Google Scholar]
- 27.Golin CE, DiMatteo MR, Gelberg L. The role of patient participation in the doctor visit Implications for adherence to diabetes care. Diabetes Care. 1996;19:1153–64. doi: 10.2337/diacare.19.10.1153. [DOI] [PubMed] [Google Scholar]
- 28.Aomatsu M, Abe H, Abe K, Yasui H, Suzuki T, Sato J. et al. Validity and reliability of the Japanese version of the CARE measure in a general medicine outpatient setting. Fam Pract. 2014;31:118–26. doi: 10.1093/fampra/cmt053. [DOI] [PubMed] [Google Scholar]
- 29.Deveugele M, Derese A, van den Brink-Muinen A, Bensing J, De Maeseneer J. Consultation length in general practice: cross sectional study in six European countries. BMJ. 2002;325:472. doi: 10.1136/bmj.325.7362.472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Behzadifar M, Behzadifar M, Saroukhani M, Sayehmiri K, Delpisheh A. Evaluation of Effective Indexes on Quality of Life Related to Health in Western Iran in 2013. Iran Red Crescent Med J. 2016;18:e23781. doi: 10.5812/ircmj.23781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Landström B, Rudebeck CE, Mattsson B. Working behaviour of competent general practitioners: Personal styles and deliberate strategies. Scand J Prim Helth Care. 2006;24:122–8. doi: 10.1080/02813430500508355. [DOI] [PubMed] [Google Scholar]
- 32.Gray J. The effect of the doctor's sex on the doctor patient relationship. J R Coll Gen Pract. 1982;32:167–9. [PMC free article] [PubMed] [Google Scholar]
- 33.Whitehouse CR. A survey of the management of psychosocial illness in general practice in Manchester. J R Coll Gen Pract. 1987;37:112–5. [PMC free article] [PubMed] [Google Scholar]
- 34.Howie JG, Porter AM, Forbes JF. Quality and the use of time in general practice: widening the discussion. BMJ. 1989;298:1008–10. doi: 10.1136/bmj.298.6679.1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Knight R. The importance of list size and consultation length as factors in general practice. J R Coll Gen Pract. 1987;37:19–22. [PMC free article] [PubMed] [Google Scholar]
- 36.Zantinge EM, Verhaak PF, Kerssens JJ, Bensing JM. The workload of GPs: consultations of patients with psychological and somatic problems compared. Br J Gen Pract. 2005;55:609–14. [PMC free article] [PubMed] [Google Scholar]